
Abstract
We aimed to investigate the sex differences in associations of diabetes mellitus (DM) with echocardiographic phenotypes and clinical outcomes of heart failure (HF). We studied 4,180 patients admitted for acute HF between 2009 and 2016 (median follow-up, 31.7 months) whose left ventricular global longitudinal strain (LV-GLS) data were available. Patients were compared by sex and DM. Structural equation model (SEM) analysis was performed to evaluate the moderating effects of two causal paths, via ischemic heart disease (IHD) and LV-GLS, linking DM with mortality. Compared to non-diabetic women, diabetic women had significantly lower LV-GLS (11.3% versus 10.1%, p < 0.001), but the difference was attenuated within men (9.7% versus 9.2%, p = 0.014) (p-for-interaction by sex = 0.018). In Cox analyses, DM was an independent predictor for higher mortality in both sexes (women: adjusted hazard ratio [HR] 1.35, 95% confidence interval [CI] 1.15–1.59 versus men: HR 1.24, 95% CI 1.07–1.44, p-for-interaction by sex = 0.699). Restricted cubic spline curves showed that LV-GLS consistently declined, and mortality increased in women with worsening hyperglycemia, but these trends were not evident in men. In SEM analysis, the main driver from DM to mortality differed by sex; men had a stronger effect via IHD than LV-GLS, whereas LV-GLS was the only predominant path in women.
Similar content being viewed by others
Introduction
Despite the advances in the management of heart failure (HF), re-hospitalization and mortality rates remain distressingly high1. The need for further understanding of the pathophysiology of HF is thus imperative, and efforts to improve the risk stratification of HF patients based on underlying pathophysiology are ongoing. Although the pathophysiology of HF includes diverse mechanisms, neurohormonal disturbances and oxidative stress have been recognized as major contributing factors2. Intriguingly, these mechanisms are also important for the development of diabetes mellitus (DM)3. Indeed, DM is highly prevalent in HF, accounting for up to 40% of HF patients4, and also associated with a worse prognosis5. These findings suggest the importance of detection and management of DM in individuals at risk for or with HF.
On the other hand, accumulating evidence proposes that there are significant sex differences in the cardiovascular consequences of DM, including the development of HF6. A recent meta-analysis demonstrated that the excess risk of HF associated with DM was significantly higher in women than in men7. Considering that HF in women occurred with less ischemic etiology than in men8, and ischemic heart disease (IHD) in diabetic patients had an especially deleterious impact on mortality9, it can be assumed that the prognosis of women with HF and DM might differ from men. However, there is a relative paucity of data on sex differences in the association of DM with clinical outcomes of HF, although most registries suggest that women with HF survive better than men with HF10.
We hypothesized that the impact of DM on clinical and echocardiographic characteristics of patients with HF and their prognosis differs by sex. This study aimed to investigate the association of DM with left ventricular (LV) systolic function, measured as LV global longitudinal strain (LV-GLS), and mortality according to sex in HF patients, from the cohort of patients with acute HF.
Results
The main findings is summarized in Fig. 1.

Sex-related differences in the impact of DM on phenotypes, LV-GLS, and causal associations in HF. The main findings of the study are summarized. (Left) Diabetic men and women with HF had different clinical and echocardiographic phenotypes. (Middle) The associations of presentation blood glucose level with the LV-GLS impairment were more pronounced in women. In the RCS curves, LV-GLS continually declined as hyperglycemia became severe in women, while it reached a plateau in men, resulting in the gradual convergence of the two curves. (Right) The main driver from DM to mortality differed; men had a larger effect via IHD than LV-GLS impairment, whereas effect mediating LV-GLS was the only predominant path in women. Dominant pathways are indicated by bold arrows; those with dashes arrows are statistically insignificant. DM = diabetes mellitus; HF = heart failure; IHD = ischemic heart disease; LV-GLS = left ventricular global longitudinal strain; RCS = restricted cubic spline.
Clinical and echocardiographic features by DM
Among 4,180 patients with HF (mean 70.7 years), 1,431 (34.2%) had DM, with more prevalence in men than women (792 [35.7%] versus 639 [32.6%], p = 0.036) (Supplementary Table S1). Baseline characteristics according to sex and DM are summarized in Table 1. In both men and women, diabetic patients had higher body mass index, and more prevalent hypertension and IHD compared to non-diabetic patients (Table 1). DM was also significantly associated with anemia, lower sodium level, and impaired renal function in both sex. Regarding the echocardiographic parameters, women had higher LV ejection fraction (LV-EF) and LV-GLS, smaller LV dimensions, and more frequent concentric LV hypertrophy (LVH) than men (Supplementary Table S1). When comparing echocardiography parameters according to sex and DM, diabetic men and women had a higher E/e’ ratio and more concentric LVH compared to non-diabetic counterparts (Table 2).
Sex difference in the association of DM with clinical and echocardiographic features
DM severity assessed by glycosylated hemoglobin (HbA1c) and presentation glucose levels was similar between men and women (Supplementary Table S1); however, clinical and echocardiographic features significantly differed when stratified by sex and DM. Compared to diabetic men, diabetic women were older and had lower hemoglobin level and glomerular filtration rate, whereas diabetic men more often had IHD with elevated troponin I level (Table 1). DM was associated with more frequent LVH in women, but the difference was not identified among men. Diabetic women had the highest proportion of concentric LVH among the four groups (44.3% of LVH), as well as the highest E/e’ ratio (18.8 [IQR, 14.5–25.9]) (Table 2). Of note, diabetic women had significantly lower LV-EF than non-diabetic women (42.1% [IQR, 30.0–57.0%] vs. 45.0% [IQR, 32.0–58.0%], p = 0.003), whereas no significant difference was observed between diabetic and non-diabetic men (34.0% [IQR, 25.0–48.4%] vs. 34.7% [IQR, 25.0–49.0%], p = 0.554) (p-for-interaction by sex = 0.019). In both sex, however, LV-GLS was significantly lower in diabetic patients than non-diabetics, with a more prominent difference in women (10.1% [IQR, 7.0–14.1%] vs. 11.3% [IQR, 8.1–15.4%], p < 0.001 for women; 9.2% [IQR, 6.3–12.6%] vs. 9.7% [IQR, 6.5–13.8%], p = 0.014 for men) (p-for-interaction by sex = 0.018).
Mortality risk according to sex and DM
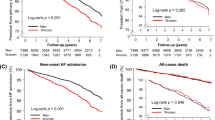
During a median of 31.7 months (IQR, 11.6–54.3 months), 1,765 deaths occurred. 5-year mortality according to sex and DM is shown (Fig. 2). Among the four groups, non-diabetic women had the lowest mortality during the early follow-up period, which was non-significantly lower than that of non-diabetic men. The difference in mortality rates between non-diabetic women and non-diabetic men gradually decreased and became similar at a longer follow-up of 5 years (p = 0.773). The mortality rates between diabetic women and diabetic men were consistently similar throughout the entire follow-up.

Kaplan–Meier curves for 5-year all-cause mortality according to sex and DM.
Cox analysis showed that DM was significantly associated with increased unadjusted and adjusted risks of death in both sex (Table 3). The magnitude of hazard ratio for mortality between DM and non-DM was greater in women than men, although not significant (adjusted hazard ratio = 1.35 [95% confidence interval: 1.15–1.59] versus 1.24 [1.07–1.44], p-for-interaction = 0.699) (Table 3).
When patients were stratified according to the tertile values of HbA1c (< 5.7%, 5.7–7.0%, > 7.0%), there was a stepwise increase in mortality with worsening HbA1c levels in women (p = 0.026), but it was not significant among men (p = 0.133) (Supplementary Figure S1). While men with mid-range HbA1c levels (5.7–7.0%) had a long-term outcome similar to those with lower HbA1c levels (< 5.7%), the survival of women with mid-range HbA1c levels was approaching that of women with the highest HbA1c levels (> 7%) (Supplementary Figure S1).
Sex-specific associations of presentation glucose level with mortality
The restricted cubic spline (RCS) curves showed the associations of presentation blood glucose level with 5-year mortality risk according to sex (Fig. 3a). Data on presentation glucose level was available in 4125 (98.7%), consisting of 2183 men and 1942 women, and all these patients were included in the RCS analysis irrespective of DM status. The patterns of RCS curves differed by sex. At the 5-year follow-up, the risk of mortality continually increased as glucose level rise in women, while the linear increase pattern was less pronounced in men, particularly if glucose level exceeds 200 mg/dL (Fig. 3a). Density plots showed that the distribution of patients according to glucose level was similar between sex.

Sex-specific association of presentation glucose level with mortality risk and LV-GLS. (a) The graph shows the adjusted hazard ratios (solid lines) and 95% confidence intervals (dashed lines and shaded area) for the association between presentation glucose level and 5-year mortality in men (blue) and women (red). The glucose level was modeled with RCS in Cox models. The reference of glucose level was set at 125 mg/dL for hazard ratios estimation. Density plots show the distribution of patients according to the glucose level. (b) RCS curves were plotted between presentation glucose level and LV-GLS. Each dot indicates an individual patient’s data. LV-GLS = left ventricular global longitudinal strain, RCS = restricted cubic spline.
Sex-specific associations of presentation glucose level with LV-GLS
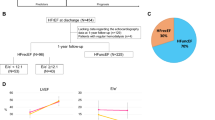
The associations between presentation glucose level and LV-GLS in men and women are examined. In the simple linear regression model, there was a negative correlation between presentation glucose level and LV-GLS, with a stronger association in women (r = − 0.10 in men, p < 0.001, r = − 0.14 in women, p < 0.001, p-for-interaction by sex = 0.058). The RCS curves demonstrated a marked nonlinear relationship between presentation glucose level and LV-GLS by sex (Fig. 3b). Overall, the gradual decrease in LV-GLS was observed with an increase in the glucose level, approximately until 200 mg/dL in both sex (Fig. 3b). When the glucose level exceeded 200 mg/dL, LV-GLS further declined approximately from 12 to 10% in a dose-dependent manner in women. In men, however, LV-GLS decreased to around 10% at the glucose level of 200 mg/dL and reached a plateau thereafter, resulting in the gradual convergence of the two curves (Fig. 3b).
Regarding the effect of hyperglycemia on diastolic function, E/e’ ratio increased as the presentation blood glucose level increased up to approximately 200 mg/dL and reached a plateau thereafter in both sexes. Women had a higher E/e’ ratio than men for the same degree of hyperglycemia (Supplementary Figure S2).
Sex differences in regression paths between DM and mortality
The structural equation model (SEM) diagrams with standardized path coefficients are presented for each sex (Fig. 4). This model included a direct path from DM to mortality, with two indirect paths from DM to mortality via IHD and LV-GLS as intermediate mediators, and it had an adequate statistical fit (Supplementary Table S2). The direct path from DM to mortality was significant in both men and women. Regarding the indirect paths, the path from DM to LV-GLS was significant in both sex, with a larger coefficient for women (coefficient = − 0.10, p < 0.001) than men (coefficient = − 0.06, p = 0.004). The path from DM to IHD was also significant in both sex. However, the path from IHD to mortality was significant in men (coefficient = 0.07, p = 0.001), but not in women (coefficient = − 0.003, p = 0.890), while the path from LV-GLS to mortality was significant in both sex.

Path diagrams of relationship between DM, LV-GLS or IHD, and mortality by sex. Diagrams of the structural equation model in men (a) and women (b). Standardized path coefficients are shown on each path as effect estimates. Solid lines denote significant paths and dashed lines, non-significant paths. 5-year mortality data was used. DM = diabetes mellitus; IHD = ischemic heart disease; LV-GLS = left ventricular global longitudinal strain. *p < 0.05, **p < 0.001.
Table 4 summarizes the standardized coefficients of direct and indirect effects. In men, the indirect effect mediated through IHD was greater (DM–IHD–mortality path: coefficient = 0.015, p = 0.001) than that mediated through LV-GLS (DM–LV-GLS–mortality path: coefficient = 0.008, p = 0.009). In women, however, the indirect effect via IHD was markedly smaller than that in men, and not significant (DM–IHD–mortality path: coefficient = − 0.001, p = 0.890). The indirect effect mediated through LV-GLS was significant and more pronounced in women (DM–LV-GLS–mortality path: coefficient = 0.015, p < 0.001) compared to men. Similar findings were observed in the sensitivity analysis using the presentation glucose or HbA1c level instead of DM (Supplementary Figure S3 and Supplementary Table S3).
When we repeated analyses after incorporating the E/e’ ratio as a third intermediate mediator, the results were materially unchanged. Specifically, in men, IHD had the largest mediating effect, but the mediating effect via E/e’ ratio or LV-GLS was not statistically significant. In women, the E/e’ ratio and LV-GLS had the largest and similar mediating effects, but the mediating effect via IHD was not statistically significant (Supplementary Figure S4 and Supplementary Table S4).
Discussion
The main findings of our study can be summarized as follows: (1) clinical and echocardiographic features of patients with acute HF significantly differed by sex and DM, (2) DM was a significant and independent predictor for increased mortality in both men and women, (3) although the effect of DM on mortality was similarly significant in both sexes, the predominant mediating factor between DM and mortality was different, namely, LV-GLS for women and IHD for men, and 4) the associations of presentation blood glucose level with LV-GLS impairment were more pronounced in women than men (Fig. 1).
Multiple evidence support that there are significant sex differences in the characteristics and prognosis of HF patients. It has been reported that women with HF are more likely to be older, obese, have reduced renal function, and higher LV-EF, whereas men with HF more commonly have IHD11. Sex-related differences in DM have also gained intense attention. For instance, women are over-represented as diabetic cardiomyopathy, in contrast to ischemic cardiomyopathy, which is more prevalent in men12. However, these sex differences have been evaluated separately for HF and DM. Considering up to 40% of HF patients have DM and 12% of diabetic patients have HF4, it is important to consider the integrated effects of HF and DM on sex differences. Our study demonstrated that the association between presentation glucose level and LV-GLS was more prominent in women than men with HF, suggesting a more deleterious impact of hyperglycemia on prognosis in women with HF.
It is worth mentioning that there were significant sex differences in the LV remodeling patterns related to DM in HF patients. When stratifying HF patients into four groups by sex and diabetes status, diabetic women with HF more frequently had LVH compared to the non-diabetic counterpart (p = 0.017), which was not observed among men (p = 0.990) (Table 2). In addition, concentric LVH was most prevalent (44.3%), and E/e’ ratio was highest (18.8 [IQR, 14.5–25.9]) in diabetic women (Table 2), suggesting a female preponderance in the prevalence of HF with preserved EF coexisting with DM. These findings also corroborate with the previous studies highlighting the sex-specific pattern of cardiac remodeling and diastolic function in DM13,14. Of note, these cardiac structural and functional abnormalities had a more deleterious impact on prognosis in women than men14. Therefore, our study adds support to the concept that a sex-specific approach is key for investigating the pattern of cardiac remodeling and its association with outcomes in HF patients. Furthermore, given recent promising results of the clinical trial showing that dapagliflozin treatment reduced LV mass in diabetic patients with LVH15, optimized drug therapy can induce reverse cardiac remodeling, which may lead to improved cardiovascular outcomes in patients with HF and DM, particularly in women.
Mechanisms underlying sex differences in HF are poorly understood. One possible mechanism is the cardio-protective role of sex-hormone in women. Several studies suggest that estrogen protects the heart from various types of stress, including hypertrophic, ischemic, and cytotoxic stimuli16,17. On the other hand, menopause, a physiological estrogen withdrawal, was significantly associated with impaired LV systolic performance and concentric LV geometry18. Regarding DM, estrogen also exerts various positive effects including insulin sensitivity, protection of pancreatic beta-cell, reduction in hepatic gluconeogenesis, and increase in muscle glucose transporter19. These findings imply that estrogen withdrawal from menopause may negatively impact the myocardial function and structure. Our study showed that the detrimental association between glucose level and LV-GLS was more remarkable in women than men, which raises the speculation that adverse effects of DM are possibly accentuated by estrogen withdrawal in women. However, since the data on estrogen levels or menopausal status were unavailable in our study, further studies are needed to test this hypothesis.
Sex-differences in cardiac steatosis can be another possible mechanism for the finding that LV systolic function is more vulnerable to hyperglycemia in women. Cardiac steatosis is characterized by the accumulation of triglyceride into the myocardium in patients with metabolic abnormalities, especially type 2 diabetes20. A major consequence of cardiac steatosis is the structural and functional change of heart, including impaired LV myocardial strain21. Notably, cardiac steatosis has been reported to be more pronounced in women than men22. In our study, LV systolic dysfunction by hyperglycemia was more prominent and consistent in women, which implies that such mechanism may play a role. However, since our study did not have data on cardiac steatosis, this explanation needs further research.
Worse prognosis in diabetic women with HF has been repeatedly reported13,23. This finding might stem from the fact that diabetic women have more prevalent comorbidities compared to diabetic men13, or that women with HF receive less optimal management23. Our findings suggest another possibility that a more pronounced impairment of LV systolic function under hyperglycemia in women could be one biological basis for the female vulnerability. This theory is further supported by our SEM analysis, which showed that LV-GLS was a major moderator between DM and mortality in women, while IHD was a dominant one in men. Hence, our study highlights the importance of sex-specific strategies to improve the prognosis of patients with both HF and DM; more intensive monitoring of the change in LV systolic function is recommended for women while timely detection of concomitant IHD is crucial for men.
Strengths and limitations
The most compelling advantage of our study is a well-constructed, large imaging database containing LV-GLS from all participants. Additionally, considering the relatively low body mass index in this study population, our findings might be less confounded by overweight or obesity, which is an important confounding factor in the studies investigating the effect of DM.
However, several limitations should be considered when interpreting the results. First, we could not find that these sex differences are translated into significant differences in hard outcomes, probably due to the lack of long-term survival data. Future studies with a larger population and longer follow-up are warranted to validate the long-term consequences of sex-specific association of DM with LV systolic function. Second, analyses based on the other metrics of DM severity, such as fasting glucose level, would have provided additional information. We used blood glucose level at the time of HF presentation for analyses, an index known to have a linear association with adverse outcomes both in diabetic and non-diabetic HF24,25. As HbA1c measurements were not routinely performed, it was only available in (42.3%) in our study, which had a moderate correlation with the presentation glucose level in both sex (men: r = 0.55, p < 0.001, women: r = 0.45, p < 0.001) (p-for-interaction by sex = 0.509) (Supplementary Figure S5). Lastly, as Korean patients were exclusively enrolled, it is uncertain whether these results may be generalized to other ethnicities.
Conclusions
Although diabetic patients with HF had higher mortality than non-diabetic counterparts in both men and women, sex differences were found in clinical and echocardiographic features, and notably, the effect of hyperglycemia on LV-GLS and mortality, with more pronounced associations in women. Furthermore, the major factor intermediating between DM and mortality differed by sex, namely, LV-GLS for women and IHD for men. Our study provides support for the importance of sex-specific strategies for HF management.
Methods
Study population
This study utilized data from The STrain for Risk Assessment and Therapeutic Strategies in patients with Acute Heart Failure registry, whose protocol has been previously described26. Briefly, 4312 patients admitted to the hospital from HF were prospectively enrolled from 3 tertiary university hospitals between January 2009 and December 2016. Eligible criteria were symptoms and signs compatible with HF, and one of the following: (1) evidence of pulmonary edema on physical examination or chest radiography or (2) objective findings of LV dysfunction or structural heart disease. The lack of LV-GLS data was the main exclusion criterion; echocardiography was performed in 4237 (98.2%), and LV-GLS was measured in 4180 (96.9%), which was the final study sample.
All study protocols were approved by the ethics committees at each center (Seoul National University Hospital, Seoul National University Bundang Hospital, Chungnam National University Hospital), and conformed with the Declaration of Helsinki. As anonymized and unidentified information was used for the analysis, the need for written informed consent was waived by the same ethics committees at each center.
Variables and definitions
Data on demographics, medical history, and laboratory tests were collected by each center. We defined DM as a chart-documented diagnosis of DM and/or treatment with glucose-lowering medications. Presentation glucose level, which was defined as the initial serum glucose level measured at the time of HF admission24,25, was collected irrespective of DM status, and the HbA1c level was obtained within a 1-month period. We defined IHD as one of the following: a history of myocardial infarction or coronary revascularization, or significant coronary stenosis (> 50% epicardial artery stenosis on coronary angiography or computed tomography angiography) or ischemia (perfusion defect on myocardial single photon emission computed tomography).
Patients were categorized into 4 groups by sex and DM: diabetic men, non-diabetic men, diabetic women, and non-diabetic women. The primary outcome was 5-year all-cause mortality. Patients’ vital statuses were obtained from the national insurance data or national death records.
Echocardiography and strain analysis
Echocardiography was performed following contemporary guidelines27, and the details are described in Supplementary Methods. The median time interval between HF admission and echocardiography was 1 day (IQR, 0–2 days).
Echocardiography images were subsequently analyzed for strain measurement at the strain core laboratory. Briefly, images qualified for the strain analysis were uploaded to TomTec software (Image Arena 4.6, Munich, Germany) for deformation analysis. Speckles were automatically tracked frame by frame, aligning to the endocardial border of the myocardium, and LV-GLS was calculated as the averaged values from 3 apical views of the entire LV. All strain measurements were performed by independent observers blinded to participants’ clinical information. We used the absolute value of LV-GLS for a straightforward interpretation.
Statistical analysis
Categorical variables are presented as frequencies (percentages), and continuous variables as median (interquartile range). The difference between groups was compared using the χ2 test or Fisher’s exact test for categorical variables, and Student’s t-test or Wilcoxon’s rank-sum test for continuous variables. Analyses investigating the interactions between sex and each continuous variable were also performed using two-way analysis of variance. The cumulative survival was plotted and compared using Kaplan–Meier curves and log-rank test. Cox proportional hazard analyses were performed to evaluate the association between DM and mortality, expressed as hazard ratios with 95% confidence intervals. Multivariate Cox analyses were adjusted for the variables with p < 0.05 in univariable analysis and known risk factors in HF28, of which the data is available with missing values < 10%, without multicollinearity: age, body mass index, hypertension, IHD, sodium level, glomerular filtration rate, LV-GLS, and use of beta-blocker and renin-angiotensin system blocker.
The RCS curves were plotted to evaluate the relationship between presentation glucose levels and adjusted hazard ratios of mortality, with 3 knots at the 10th, 50th, 90th percentiles of glucose levels (men: 90, 127, and 243 mg/dL, women: 91, 129, and 246 mg/dL). We also used RCS curves for displaying the relationship between presentation glucose levels and LV-GLS.
To further elucidate which intermediate variables lie on a causal path from exposure (i.e., DM) to outcome (i.e., mortality), we performed the SEM analysis, which is a powerful statistical method to assess complex and multivariate relationships by using several regression equations simultaneously, enabling measurement of both direct and indirect effects between variables29. In this study, we examined the contribution of two intermediate variables (LV-GLS and IHD) between DM and mortality, where the magnitude of each path was calculated as path coefficients29. LV-GLS and IHD were selected as intermediate variables since myocardial contractile dysfunction and ischemia are known to be the major contributors to cardiovascular mortality in HF patients, especially those with DM9,30. Separate SEM analyses were performed for each sex based on our hypothesis that there would be sex-difference in the paths connecting DM and mortality. The final models were depicted as diagrams, with standardized path coefficients and P-values. The lavaan and sem package in R was used31. For a more detailed description of the SEM model, see Supplementary methods.
A two-tailed P-value < 0.05 was considered statistically significant. All analyses were performed using R (version 3.6.0, Vienna, Austria).
Data availability
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- DM:
-
Diabetes mellitus
- HF:
-
Heart failure
- IHD:
-
Ischemic heart disease
- LV-EF:
-
Left ventricular ejection fraction
- LV-GLS:
-
Left ventricular global longitudinal strain
- LVH:
-
Left ventricular hypertrophy
- RCS:
-
Restricted cubic splines
- SEM:
-
Structural equation model
References
Cleland, J. G. F., Lyon, A. R., McDonagh, T. & McMurray, J. J. V. The year in cardiology: heart failure. Eur Heart J. 41, 1232–1248 (2020).
Munzel, T. et al. Impact of oxidative stress on the heart and vasculature: part 2 of a 3-part series. J. Am. Coll. Cardiol. 70, 212–229 (2017).
Muoio, D. M. & Newgard, C. B. Mechanisms of disease: molecular and metabolic mechanisms of insulin resistance and beta-cell failure in type 2 diabetes. Nat. Rev. Mol. Cell Biol. 9, 193–205 (2008).
MacDonald, M. R. et al. Diabetes, left ventricular systolic dysfunction, and chronic heart failure. Eur. Heart J. 29, 1224–1240 (2008).
Ponikowski, P. et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 37, 2129–2200 (2016).
Norhammar, A. Diabetes and cardiovascular mortality: the impact of sex. Lancet Diabetes Endocrinol. 6, 517–519 (2018).
Ohkuma, T., Komorita, Y., Peters, S. A. E. & Woodward, M. Diabetes as a risk factor for heart failure in women and men: a systematic review and meta-analysis of 47 cohorts including 12 million individuals. Diabetologia 62, 1550–1560 (2019).
Shaw, L. J., Bugiardini, R. & Merz, C. N. Women and ischemic heart disease: evolving knowledge. J. Am. Coll. Cardiol. 54, 1561–1575 (2009).
Johansson, I. et al. Prognostic implications of Type 2 diabetes mellitus in ischemic and nonischemic heart failure. J. Am. Coll. Cardiol. 68, 1404–1416 (2016).
Levy, D. et al. Long-term trends in the incidence of and survival with heart failure. N. Engl. J. Med. 347, 1397–1402 (2002).
Lam, C. S. P. et al. Sex differences in heart failure. Eur. Heart J. 40, 3859–3868c (2019).
Murphy, E., Amanakis, G., Fillmore, N., Parks, R. J. & Sun, J. Sex differences in metabolic cardiomyopathy. Cardiovasc. Res. 113, 370–377 (2017).
Chandramouli, C. et al. Impact of diabetes and sex in heart failure with reduced ejection fraction patients from the ASIAN-HF registry. Eur. J. Heart Fail. 21, 297–307 (2019).
Wu, M. Z. et al. Sex-specific pattern of left ventricular hypertrophy and diastolic function in patients with type 2 diabetes mellitus. Eur. Heart J. Cardiovasc. Imaging. 5, jeaa079 (2020).
Brown, A. et al. A randomized controlled trial of dapagliflozin on left ventricular hypertrophy in people with type two diabetes: the DAPA-LVH trial. Eur. Heart J. 41, 3421–3432 (2020).
Babiker, F. A. et al. Estrogenic hormone action in the heart: regulatory network and function. Cardiovasc. Res. 53, 709–719 (2002).
de Jager, T. et al. Mechanisms of estrogen receptor action in the myocardium. Rapid gene activation via the ERK1/2 pathway and serum response elements. J. Biol. Chem. 276, 27873–27880 (2001).
Schillaci, G., Verdecchia, P., Borgioni, C., Ciucci, A. & Porcellati, C. Early cardiac changes after menopause. Hypertension 32, 764–769 (1998).
Moran, A. et al. Changes in insulin resistance and cardiovascular risk during adolescence: establishment of differential risk in males and females. Circulation 117, 2361–2368 (2008).
McGavock, J. M. et al. Cardiac steatosis in diabetes mellitus: a 1H-magnetic resonance spectroscopy study. Circulation 116, 1170–1175 (2007).
Levelt, E. et al. Relationship between left ventricular structural and metabolic remodeling in Type 2 diabetes. Diabetes 65, 44–52 (2016).
Iozzo, P. et al. Contribution of glucose tolerance and gender to cardiac adiposity. J. Clin. Endocrinol. Metab. 94, 4472–4482 (2009).
Johansson, I. et al. Risk factors, treatment and prognosis in men and women with heart failure with and without diabetes. Heart 101, 1139–1148 (2015).
Sud, M. et al. Presentation blood glucose and death, hospitalization, and future diabetes risk in patients with acute heart failure syndromes. Eur. Heart J. 36, 924–931 (2015).
ItzhakiBenZadok, O. et al. Admission blood glucose and 10-year mortality among patients with or without pre-existing diabetes mellitus hospitalized with heart failure. Cardiovasc. Diabetol. 16, 102 (2017).
Park, J. J., Park, J. B., Park, J. H. & Cho, G. Y. Global longitudinal strain to predict mortality in patients with acute heart failure. J. Am. Coll. Cardiol. 71, 1947–1957 (2018).
Lang, R. M. et al. Recommendations for cardiac chamber quantification by echocardiography in adults: an update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 28, 1–39 (2015).
Pocock, S. J. et al. Meta-Analysis Global Group in Chronic Heart F. Predicting survival in heart failure: a risk score based on 39,372 patients from 30 studies. Eur. Heart J. 34, 1404–1413 (2013).
Bojan, M. et al. Structural equation modelling exploration of the key pathophysiological processes involved in cardiac surgery-related acute kidney injury in infants. Crit. Care. 20, 171 (2016).
Jia, G., Hill, M. A. & Sowers, J. R. Diabetic cardiomyopathy: an update of mechanisms contributing to this clinical entity. Circ. Res. 122, 624–638 (2018).
Rosseel, Y. lavaan: an R package for structural equation modeling. J Stat Softw. 48, 36 (2012).
Acknowledgements
None.
Funding
This work was supported by the National Research Foundation of Korea of the Ministry of Science and ICT (2020R1C1C1010890).
Author information
Authors and Affiliations
Contributions
S.K. and J.B.P. planned and designed the current study, performed the statistical analysis, and drafted the manuscript. I.C.H., J.J.P., and J.H.P. reviewed/edited the manuscript and contributed to the discussion. G.Y.C. supervised all aspects of the study and revised the manuscript critically. G.Y.C. is the guarantor of this work and, as such, had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Kwak, S., Hwang, IC., Park, J.J. et al. Sex-specific impact of diabetes mellitus on left ventricular systolic function and prognosis in heart failure. Sci Rep 11, 11664 (2021). https://doi.org/10.1038/s41598-021-91170-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-021-91170-x
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
