
Abstract
Shear wave elastography (SWE) is a technique to non-invasively and quantitatively evaluate tissue stiffness. We aimed to investigate whether we can differentiate pancreatic cancer (PC) from normal pancreatic parenchyma (NPP) by SWE using transabdominal ultrasound. We investigated a total of 106 patients (84 with NPP and 22 with PC) whose pancreatic elastic modulus was measured by two-dimensional SWE (2D-SWE). Intra-rater reliability in this study was examined, and three measurements were sufficiently reliable. There were no differences between the two groups in factors that could affect SWE measurements. The median value of the elastic modulus was 5.70 kPa in the PC patients and 5.66 kPa in the NPP group, which was not significantly different (P = 0.785). On the contrary, the range was 8.64 kPa and 4.72 kPa, with a significantly greater range in the PC patients (P = 0.001). In conclusion, the median elastic modulus measured by 2D-SWE was not significantly different between PC and NPP, and evaluating the obtained elastic modulus itself is not useful in differentiation. However, the variability was significantly greater in PC than in NPP. Evaluating the range of elasticities will provide additional information in SWE, which may be useful in the diagnosis of PC.
Similar content being viewed by others

Introduction
Ultrasonic elastography is a technique for measuring the stiffness of tissues. Shear wave elastography (SWE) is a recently developed technique to measure the shear wave speed (SWS) within a region of interest (ROI) generated by push pulses by repeatedly emitting exploratory ultrasound pulses to objectively and quantitatively evaluate tissue stiffness1,2,3,4. This enables a non-invasive and simple evaluation of tissue stiffness. SWE has been reported to be useful in the evaluation of liver fibrosis and steatosis, and its clinical significance is gradually becoming clear5,6. Recently, SWE has also been reported to be useful in the pancreas, such as for the diagnosis of fibrosis in chronic pancreatitis7. However, few SWE-related reports for the diagnosis of pancreatic cancer (PC) are available. Although PC often forms a stiff mass8, whether the tissue stiffness of PC can be correctly evaluated by SWE is not clear. The aim of this study was to determine whether we could differentiate PC from normal pancreatic parenchyma (NPP) by SWE measured using a state-of-the-art ultrasound instrument, the EPIQ 7G (Philips Medical Systems, Bothell, WA).
Materials and methods
Study design
This was a single-center, case–control study. This research was conducted in strict compliance with the Declaration of Helsinki and in accordance with the ethical guidelines for medical research involving human subjects. Written informed consent was obtained from all patients in this study. The study was conducted with the approval of the Ethics Committee of Nagoya University Hospital (approval number: 2014-0399).
Patients
We retrospectively reviewed 98 NPP, 22 PC and 4 mass-forming pancreatitis (MFP, 2 chronic pancreatitis and 2 type 1 autoimmune pancreatitis) patients who underwent SWE using the EPIQ 7G at Nagoya University Hospital between January 2019 and October 2019. In all PC patients, a mass was detected in the pancreas on CT within 2 weeks before transabdominal ultrasound (US). Using the CT image as a guide, all of the lesions could be identified on US, and SWE measurement was possible in all 22 cases. A pathological diagnosis was obtained in all PC cases by surgery (n = 13) or endoscopic ultrasound-guided fine-needle aspiration (EUS-FNA) (n = 9), and the histological type was adenocarcinoma in all patients. The median tumour diameter of PC was 31 mm (20.8–37.0), and the locations of the tumours were the head in 13 cases, the body in 7 cases, and the tail in 2 cases, with distant metastasis identified in 5 cases (Table 1).
The 98 NPP patients were enrolled from among the 332 patients who underwent US using the EPIQ 7G during the study period and had no history of pancreatic disease and no abnormalities on CT or endoscopic ultrasound (EUS) imaging within 3 months before US, such as cyst or expansion or narrowing of the pancreatic duct. In these 98 patients, the pancreatic parenchyma of the body could be clearly depicted on US in 84 cases, and SWE measurement was possible in all of these cases.
The 4 MFP patients were also enrolled from among the 332 patients shown above. All 4 patients had CT and EUS-FNA at the initial assessment, and the final diagnosis was made with 1 follow-up of at least 12 months. The locations of the lesions were the head in 3 cases and the body in 1 case.
Finally, SWE measurement was possible in a total of 110 patients (22 PC, 84 NPP and 4 MFP cases), and the SWE values were evaluated in these cases. The examination was performed by one gastroenterologist, who has experience with more than 3000 transabdominal ultrasounds and is a specialist in the Japanese Society of Ultrasound Medicine, and one gastroenterologist who is a full member of the Japanese Society of Ultrasound Medicine.
SWE measurement
The EPIQ 7G instrument was used in all cases. The transducer was a convex transducer, C5-1. The SWE was measured in the ElastQ mode onboard the instrument. The ElastQ mode is the 2-dimensional SWE (2D-SWE) on the EPIQ7G, which allows the size of the area of interest to be extended to a maximum of 6 cm × 5 cm, and the measurement area can be set to any area of the colour-mapped stiffness map. When performing SWE with ElastQ mode, a confidence map is also generated within the area of interest using smart analysis of echo and shear wave signals. The confidence map reflects a value for each pixel, providing an indication of quality across the stiffness map. The areas with low confidence values are shown as colour defects in the stiffness map. Several factors can lower the confidence value: tissue areas with blood flow (vessels), low echogenicity (such as the gallbladder), low shear wave strength (as when scanning deep in a technically difficult patient), or with large tissue motion (as with no breath pause). In this study, interquartile range (IQR)/median, which is a quantitative measurement, rather than the confidence map, which is a qualitative measurement, was used as an indicator of reliability. The SWE is saved as a video (raw data) lasting a few seconds and can be rewound to measure the SWE from any still image. In this study, a 6-s video was saved uniformly. The patient was instructed to hold his or her breath when the evaluation site was clearly depicted in B-mode and was within the area of interest, and the video was saved. In the NPP group, the area of interest was set in the body of the pancreas, which could be clearly described, and in the PC and the MFP group, the area of interest was set where the maximum diameter of the lesion could be clearly described (Fig. 1). Three videos were stored at the same site, and SWE was measured after the examination. For the measurement, one still image was manually selected from each movie with the least colour defect of the target area in the stiffness map. The measurement was performed with a circular ROI, and the diameter was unified to 5 mm. Schellhaas et al. have evaluated the influenced of ROI size in the assessment of liver stiffness using 2D-SWE, and concluded that the size of the ROI (5, 10, 20 mm) seemed to be of minor importance with comparable results and it was more important to perform multiple measurements9. Since the pancreas is smaller than the liver, we set the ROI size to 5 mm so that we can measure at multiple locations. As there is no clear consensus on the setting of SWE measurements in the pancreatic region, we set the threshold to 60%, which is the standard setting of liver SWE measurements. The ROI was set at three locations per image where the IQR/median was 30% or less, and if multiple locations (10 locations) did not result in 30% or less, the three locations with the lowest IQR/median were selected. The SWE measurement screen also displays a colour map, but location of the ROI was set using the IQR/median as an indicator, regardless of the colour distribution. A total of nine measurements were stored for each of the three stored videos in the same way, and the median of the nine measurements (kPa) was defined as the elastic modulus of the evaluation site.

Shear wave elastography (SWE) images and measurements. (a) SWE images of normal pancreatic parenchyma. The left side image shows a B-mode image, and the right side image shows a stiffness map. Multiple regions of interest can be set anywhere in the stiffness map, and the SWE results are described in the center of the display. (b) SWE images of pancreatic cancer.
Examination items and statistical analysis
The reproducibility and reliability of ultrasonic elastography is a challenging issue, and it has been reported that the measured values differ depending on the instrument10. It has also been reported that values vary not only by disease but also by background factors such as age, BMI, and distance from the probe to the measurement target11. Thus, this study was performed in the following five steps.
-
1.
Normal values of SWE and intraclass correlation coefficient (ICC) of SWE measurement in the pancreas in ElastQ mode
The ICC was calculated for the NPP group, and the intra-rater reliability was evaluated. In this study, three still images were selected from the video saved in ElastQ mode, three SWE measurements were taken at three locations per image, and a total of nine measurements were evaluated. In the intra-rater reliability study, the median value of three measurements in the same image was used as the value per image, and ICC (1,1) and ICC (1,3) were calculated to verify whether the SWE could be reliably measured by three images. The elastic modulus calculated by this method was defined as the normal value of the pancreas.
-
2.
Differences in clinical background between the NPP group and PC group
Age, sex, body mass index (BMI), medical history (hypertension, dyslipidaemia, diabetes), the distance between the pancreatic parenchyma and the body surface, the distance between the PC tumour area and the body surface, and blood biochemical tests were compared between NPP and PC patients. The distance between the pancreatic parenchyma and the body surface was set as the distance from the proximal edge of the pancreatic body, which is the thickest part of the body where SWE is measured, to the probe. Similarly, the distance between PC tumours and the body surface was defined as the distance from the proximal edge of the tumour to the probe at the site of SWE measurement.
-
3.
Comparison of elastic modulus between the NPP group and PC group
Based on the SWE values in the normal pancreas obtained in (1) above, the median SWE values of the NPP group and PC group were compared.
-
4.
Comparison of the variability of elastic modulus between the NPP group and PC group
Because of the expected high tissue heterogeneity in PC12, we calculated the minimum values, maximum values and ranges (the difference between the maximum and minimum values) within the measurements as well as the median values obtained from multiple measurements in each patient and compared the variability between the NPP group and PC group.
-
5.
Comparison of elastic modulus and its variability between the PC group and MFP group
The median SWE values and the variability of the PC group and MFP group ware compared.
Fisher's exact test was used for categorical variables, and the Mann–Whitney U test or the Kruskal–Wallis test was used for continuous variables; the ICCs (1,1) and (1,k) were calculated using the classification of Shrout and Fleiss13. A P value of less than 0.05 was considered statistically significant. We analysed the receiver operating characteristic curves for the mean and range values of the elastic modulus. SPSS ver. 26 (SPSS, Inc., Tokyo, Japan) was used for all analyses.
Results
-
1.
In one image measurement (three measurements) in the NPP group, the ICC (1,1) was ρ = 0.668 (IQR 0.566–0.757), and the ICC (1,3) was ρ = 0.858 (0.796–0.904) (Table 2). Pancreatic elastic modulus [median (IQR)] in the NPP group determined from a total of nine measurements in three images was 5.66 (4.39–7.84) kPa. This value was compared with the elastic modulus in the PC group determined in (3).
-
2.
Significant differences in albumin, AST, ALT, ALP, γGTP, CA19-9, and a history of diabetes were found between the NPP group and the PC group, but no differences were observed between the two groups in factors that could affect SWE measurement, such as age, BMI, and the distance between the probe and the measurement target (Table 3).
-
3.
The median elastic modulus of the PC group was 5.70 (3.48–11.55) kPa, which was not significantly greater than that of the NPP group (P = 0.785) (Fig. 2). The ROC curve using the median value of nine measurements gave an AUC = 0.52, with a sensitivity of 31.8%, specificity of 91.7%, positive predictive value of 50.0%, and negative predictive value of 83.7% when 11.00 kPa was the cut-off value (Fig. 3a).
-
4.
Each results is shown in Table 4. The median of the minimum values, maximum values, and range values were evaluated for one image (three measurements), two images (six measurements), and three images (nine measurements). The minimum values with 3, 6, and 9 measurements were 4.25/3.85/3.75 kPa in the NPP group and 3.92/3.21/3.05 kPa in the PC group, respectively, with significantly smaller values in the PC group with nine measurements (P = 0.040). The maximum values with three, six, and nine measurements were 6.37/7.55/8.69 kPa in the NPP group and 8.34/12.05/13.15 kPa in the PC group, respectively, with significantly larger values in the PC group with six and nine measurements (P = 0.009, P = 0.008, respectively). The range values with three, six, and nine measurements were 1.80/3.55/4.72 kPa in the NPP group and 3.40/6.83/8.64 kPa in the PC group, respectively, with significantly higher values in the PC group (P = 0.043, P = 0.003, P = 0.001, respectively). The ROC curve using the range value of nine measurements gave an AUC 0.728, with a sensitivity of 59.1%, specificity of 84.5%, positive predictive value of 50%, and negative predictive value of 88.8% when 7.88 kPa was the cut-off value (Fig. 3b).
-
5.
The median elastic modulus of the MFP group was 3.94 (3.18–9.26) kPa, which was not significantly different from that of the PC group (P = 0.352). The range value with nine measurements was 3.41 kPa in the MFP group, which was significantly smaller than that of the PC group (P = 0.021). There was no significant difference in the elastic modulus between NPP and MFP (P = 0.177).

Comparison of elastic modulus between normal pancreatic parenchyma (NPP) group and pancreatic cancer (PC) group. The median values of each group are compared using a t-test, and the error bars show interquartile range.

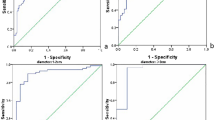
The receiver operating characteristic curve for the diagnostic ability of the mean (a) and range (b) values for pancreatic cancer. (a) With a cut-off value of 11.00 kPa, the sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) of SWE for the diagnosis of pancreatic cancer were 31.8%, 91.7%, 50.0%, and 83.7%, respectively. (b) With a cut-off value of 7.88 kPa, the sensitivity, specificity, PPV, and NPV of SWE for the diagnosis of pancreatic cancer were 59.1%, 84.5%, 50.0%, and 88.8%, respectively.
Discussion
In this study, we investigated the usefulness of SWE as an objective and quantitative evaluation method for PC and found that there was no difference in the elastic modulus measured in PC and NPP. However, the variability of elastic modulus within each patient was significantly greater in PC than in NPP.
Elastography of the pancreas has been studied in various ways. Itoh et al.14 found that elastography using EUS (EUS-EG) is useful in the diagnosis of pancreatic fibrosis. Kuwahara et al.15 also found that EUS-EG is useful for the objective evaluation of chronic pancreatitis. Some reports on the usefulness of EUS-EG for the qualitative evaluation of pancreatic tumours are available16,17,18,19, but most studies on elastography of the pancreas are conducted using EUS, and only a few reports show that elastography using transabdominal US is useful for the evaluation of pancreatic tumours8. The reason for this is that the pancreas is located deep inside the body, and in some cases, it is difficult to obtain a stable image with transabdominal ultrasound. Compared to strain elastography, which uses the external force generated in the body, SWE has a fixed shear wave for each instrument and is more repeatable and quantifiable than the former. SWE has already been reported to be useful in the evaluation of liver fibrosis and steatosis, and the optimal number of measurements and other procedures are being established6. However, it is not known in detail whether reproducible measurement values can be obtained for the pancreas or what the optimal measurement conditions are. Furthermore, although SWE is a quantitative evaluation, the measurement values obtained may differ depending on the instrument10, and we believe it is necessary to evaluate the measurement conditions for each instrument.
In this study, we first examined the optimal number of measurements of the ElastQ mode of the EPIQ 7G used in this study. It was shown that appropriate SWE values were obtained by measuring SWE in three images, meaning that nine measurements were performed. Conventional SWE is point shear wave elastography (pSWE), which is a technique to obtain a single measurement value at any point by referring to the B-mode. However, 2D-SWE, which has been installed in the high-end models of each instrument in recent years, is capable of measuring a wide range of areas at the same time, and it is possible to make appropriate measurements intuitively and visually by displaying a colour map. Kuwahara et al.20 reported that the number of measurements required for pSWE reproducibility was five, while Hashizume et al.21 reported that the number of measurements required to obtain reliable data using the propagation display of 2D-SWE was three. In this study, the optimal number of measurements obtained was three by using the stiffness map and IQR/median as a reference to determine the measurement locations. 2D-SWE improves the reproducibility and is considered to be a technique that can be applied to the pancreas.
Very few reports have evaluated the stiffness of PC using SWE, but the available reports indicate that PC is stiffer than normal pancreatic tissue. Zaro et al.22 found that the mean SWE of PC was significantly higher than that of healthy pancreas tissue in a pilot study of 33 patients, including 18 controls with healthy pancreases and 14 PC (adenocarcinoma) patients. D'Onofrio et al.23 found that the median SWE was significantly higher in 62 PC (adenocarcinoma) patients than in 40 individuals with healthy pancreases. Additionally, by strain elastography, PC is considered a stiffer tissue than normal pancreatic tissue and other surrounding tissue8. In the present study, the median elastic modulus was not significantly higher in PC cases, but the variability of the elastic modulus inside the same lesion was significantly greater in PC cases. PC tumours are known to be characterized by molecular pathological heterogeneity12, and such histological heterogeneity may have influenced the measurement results. In the present study, we focused on the minimum value, maximum value and range of elastic modulus to evaluate the variability. The minimum elastic modulus value in PC was significantly smaller than NPP with nine measurements (P = 0.040, respectively), and the maximum elastic modulus value in PC was also significantly higher than NPP with six and nine measurements (P = 0.009, P = 0.008, respectively). These results indicate that PC consists of stiffer tissues than NPP but also contains soft tissues with elastic modulus similar to that of NPP. The range was also significantly greater in PC with three, six, and nine measurements (P = 0.043, P = 0.003, P = 0.001, respectively). The specificity of the ROC curve using the range was 84.5% with a cut-off value of 7.88 kPa, the positive predictive value was 50%, and the negative predictive value was 88.8%. Considering the high negative predictive value described above, when a lesion demonstrates high elastic modulus but low variability, the possibility of a non-cancerous lesion should be considered. Other pancreatic tumours, such as pancreatic neuroendocrine tumours and solid pseudopapillary neoplasms, are considered to be more homogeneous tumours than PC24,25,26,27 and have less variation from case to case. Although other pancreatic tumours were not investigated in this study, quantitatively evaluating the histological characteristics of tumours by measuring SWE in other solid pancreatic tumours may be possible. It may also be useful in differentiating PC and inflammatory changes such as MFP. In this study, although there were no differences in the median elastic modulus between the two groups, the variability of MFP was significantly smaller than that of PC. Because of the small number of MFP cases, it may be difficult to conclude that SWE is useful in differentiating PC and MFP from our results, but we believe that we have shown the potential usefulness.
There are some limitations in this study. First, there were no pathological diagnoses in the control group, so there may have been a mixture of pancreatic diseases that were not detectable from the history and imaging findings. Second, this study did not include other pancreatic tumours. Third, this was a single-center, retrospective observational study with a small number of patients, particularly the patients with PC and MFP, and the findings need to be investigated in a larger cohort of prospective, multicenter studies in the future including other pancreatic tumours.
Conclusions
2D-SWE showed that elastic modulus measured was not different between PC and NPP, but the variability of elastic modulus was significantly greater in PC than in NPP. Evaluating the obtained elastic modulus itself is not useful in differentiating PC from NPP. However, evaluating the range of elasticities that can be obtained relatively easily will provide additional information in SWE, which may be useful in the diagnosis of PC.
Data availability
The datasets generated and analysed during the current study are available from the corresponding author on reasonable request.
Change history
28 September 2022
A Correction to this paper has been published: https://doi.org/10.1038/s41598-022-21219-y
Abbreviations
- SWE:
-
Shear wave elastography
- SWS:
-
Shear wave speed
- PC:
-
Pancreatic cancer
- NPP:
-
Normal pancreatic parenchyma
- BMI:
-
Body mass index
- IQR:
-
Interquartile range
- EUS:
-
Endoscopic ultrasound
- EUS-FNA:
-
Endoscopic ultrasound-guided fine-needle aspiration
- 2D-SWE:
-
Two-dimensional shear wave elastography
- ICC:
-
Intraclass correlation coefficient
- EUS-EG:
-
Elastography using endoscopic ultrasound
- pSWE:
-
Point shear wave elastography
References
Sarvazyan, A. P., Rudenko, O. V., Swanson, S. D., Fowlkes, J. B. & Emelianov, S. Y. Shear wave elasticity imaging: A new ultrasonic technology of medical diagnostics. Ultrasound Med. Biol. 24, 1419–1435. https://doi.org/10.1016/S0301-5629(98)00110-0 (1998).
Nightingale, K., Soo, M. S., Nightingale, R. & Trahey, G. Acoustic radiation force impulse imaging: In vivo demonstration of clinical feasibility. Ultrasound Med. Biol. 28, 227–235. https://doi.org/10.1016/S0301-5629(01)00499-9 (2002).
Nightingale, K., McAleavey, S. & Trahey, G. Shear-wave generation using acoustic radiation force: In vivo and ex vivo results. Ultrasound Med. Biol. 29, 1715–1723. https://doi.org/10.1016/j.ultrasmedbio.2003.08.008 (2003).
Friedrich-Rust, M. et al. Liver fibrosis in viral hepatitis: Noninvasive assessment with acoustic radiation force impulse imaging versus transient elastography. Radiology 252, 595–604. https://doi.org/10.1148/radiol.2523081928 (2009).
Kudo, M. et al. JSUM ultrasound elastography practice guidelines: Liver. J. Med. Ultrason. 40, 325–357. https://doi.org/10.1007/s10396-013-0460-5 (2013).
Iijima, H. et al. Comparison of liver stiffness assessment by transient elastography and shear wave elastography using six ultrasound devices: Liver stiffness by six ultrasound devices. Hepatol. Res. https://doi.org/10.1111/hepr.13319 (2019).
Kuwahara, T. et al. Quantitative evaluation of pancreatic tumor fibrosis using shear wave elastography. Pancreatology 16, 1063–1068. https://doi.org/10.1016/j.pan.2016.09.012 (2016).
Uchida, H. et al. Feasibility of tissue elastography using transcutaneous ultrasonography for the diagnosis of pancreatic diseases. Pancreas 38, 17–22. https://doi.org/10.1097/MPA.0b013e318184db78 (2009).
Schellhaas, B. et al. Two-dimensional shear-wave elastography: A new method comparable to acoustic radiation force impulse imaging?. Eur. J. Gastroenterol. Hepatol. 29, 723–729. https://doi.org/10.1097/meg.0000000000000846 (2017).
Gilligan, L. A., Trout, A. T., Bennett, P. & Dillman, J. R. Repeatability and agreement of shear wave speed measurements in phantoms and human livers across 6 ultrasound 2-dimensional shear wave elastography systems. Investig. Radiol. 55, 191–199. https://doi.org/10.1097/rli.0000000000000627 (2020).
Petzold, G., Hofer, J., Ellenrieder, V., Neesse, A. & Kunsch, S. Liver stiffness measured by 2-dimensional shear wave elastography: Prospective evaluation of healthy volunteers and patients with liver cirrhosis. J. Ultrasound Med. 38, 1769–1777. https://doi.org/10.1002/jum.14866 (2019).
Vincent, A., Herman, J., Schulick, R., Hruban, R. H. & Goggins, M. Pancreatic cancer. Lancet 378, 607–620. https://doi.org/10.1016/S0140-6736(10)62307-0 (2011).
Shrout, P. E. & Fleiss, J. L. Intraclass correlations: Uses in assessing rater reliability. Psychol. Bull. 86, 420–428. https://doi.org/10.1037//0033-2909.86.2.420 (1979).
Itoh, Y. et al. Quantitative analysis of diagnosing pancreatic fibrosis using EUS-elastography (comparison with surgical specimens). J. Gastroenterol. 49, 1183–1192. https://doi.org/10.1007/s00535-013-0880-4 (2014).
Kuwahara, T. et al. Quantitative diagnosis of chronic pancreatitis using EUS elastography. J. Gastroenterol. 52, 868–874. https://doi.org/10.1007/s00535-016-1296-8 (2017).
Dyrla, P. et al. Elastography in the diagnosis of pancreatic malignancies. Adv. Exp. Med. Biol. 1133, 41–48. https://doi.org/10.1007/5584_2018_303 (2019).
Chacaltana Mendoza, A., Jerez Lanza, V. F., Llatas Perez, J., Li Salvatierra, B. & Vera Calderon, A. Usefulness of endoscopic ultrasound guided elastography in the assessment of solid pancreatic lesions. Rev. Gastroenterol. Peru 39, 38–44 (2019).
Okasha, H. H. et al. Endoscopic ultrasound (EUS) elastography and strain ratio, could it help in differentiating malignant from benign pancreatic lesions?. Medicine (Baltimore) 97, e11689–e11689. https://doi.org/10.1097/MD.0000000000011689 (2018).
Chantarojanasiri, T. & Kongkam, P. Endoscopic ultrasound elastography for solid pancreatic lesions. World J. Gastrointest. Endosc. 9, 506–513. https://doi.org/10.4253/wjge.v9.i10.506 (2017).
Kuwahara, T. et al. Usefulness of shear wave elastography as a quantitative diagnosis of chronic pancreatitis. J. Gastroenterol. Hepatol. 33, 756–761. https://doi.org/10.1111/jgh.13926 (2018).
Hashizume, K. et al. The propagation display method improves the reproducibility of pancreatic shear wave elastography. Ultrasound Med. Biol. 45, 2242–2247. https://doi.org/10.1016/j.ultrasmedbio.2019.04.003 (2019).
Zaro, R., Dina, L., Pojoga, C., Vesa, S. & Badea, R. Evaluation of the pancreatic tumors by transabdominal Shear Wave Elastography: Preliminary results of a pilot study. Med. Ultrason. 20, 285–291. https://doi.org/10.11152/mu-1492 (2018).
D’Onofrio, M. et al. Acoustic radiation force impulse with shear wave speed quantification of pancreatic masses: A prospective study. Pancreatology 16, 106–109. https://doi.org/10.1016/j.pan.2015.12.003 (2016).
Tanaka, Y. et al. Frequent beta-catenin mutation and cytoplasmic/nuclear accumulation in pancreatic solid-pseudopapillary neoplasm. Cancer Res. 61, 8401–8404 (2001).
Abraham, S. C. et al. Solid-pseudopapillary tumors of the pancreas are genetically distinct from pancreatic ductal adenocarcinomas and almost always harbor beta-catenin mutations. Am. J. Pathol. 160, 1361–1369. https://doi.org/10.1016/s0002-9440(10)62563-1 (2002).
Hammel, P. R. et al. Pancreatic involvement in von Hippel-Lindau disease. The Groupe Francophone d’Etude de la Maladie de von Hippel-Lindau. Gastroenterology 119, 1087–1095. https://doi.org/10.1053/gast.2000.18143 (2000).
Chen, M., Van Ness, M., Guo, Y. & Gregg, J. Molecular pathology of pancreatic neuroendocrine tumors. J. Gastrointest. Oncol. 3, 182–188. https://doi.org/10.3978/j.issn.2078-6891.2012.018 (2012).
Author information
Authors and Affiliations
Contributions
M.Y., T.I. (the 2nd author), E.O., and H.K. were involved in the conception and design of this study. T.I. (the 4th author), K.F., M.N., and F.K. performed the analysis and interpretation of the data. M.Y., T.I. (the 2nd author), E.O., and T.H. drafted the main document. M.I., H.K., and M.F. made critical revision of the article for important intellectual content. All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Competing interests
Yoshikawa M and Ishikawa T received a research grant from Philips Medical Systems to conduct the study. The funder played no role in the conduct of the study or in the writing of the manuscript. Ohno E, Iida T, Furukawa K, Nakamura M, Honda, T, Ishigami M, Kinoshita F, Kawashima H, and Fujishiro M declare no potential conflict of interest.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The original online version of this Article was revised: The original version of this Article contained an error. In the Materials and methods section, under the subheading ‘Study design’, the approval number of the Ethics Committee was incorrect. Full information regarding the corrections made can be found in the correction for this Article.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Yoshikawa, M., Ishikawa, T., Ohno, E. et al. Variability measurements provide additional value to shear wave elastography in the diagnosis of pancreatic cancer. Sci Rep 11, 7409 (2021). https://doi.org/10.1038/s41598-021-86979-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-021-86979-5
This article is cited by
-
The role of EUS elastography-guided fine needle biopsy in the histological diagnosis of solid pancreatic lesions: a prospective exploratory study
Scientific Reports (2022)
-
Pancreatic shear wave elastography in children with type 1 diabetes: relation to diabetes duration, glycemic indices, fasting C-peptide and diabetic complications
Pediatric Radiology (2022)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
