
Abstract
The quality of life (QoL) of men with optimal outcomes after robot-assisted radical prostatectomy (RARP) is largely unexplored. Thus we assessed meaningful changes of QoL measured with the EORTC QLQ-C30 24 months after RARP according to postsurgical Cancer of the Prostate Risk Assessment score (CAPRA-S) and pentafecta criteria. 2871 prostate cancer (PCa) patients with completed EORTC QLQ-C30 were stratified according to CAPRA-S, pentafecta (erectile function recovery, urinary continence recovery, biochemical-recurrence-free survival (BFS), negative surgical margins) and 90-day Clavien–Dindo-complications (CDC) ≤ 3a. Multivariable logistic regression analyses (LRM) aimed to predict improvement of EORTC QoL. Mean preoperative QoL values did not significantly differ between CAPRA-S low- (LR) vs. high-risk (HR, 75.7 vs. 75.2; p = 0.7) and pentafecta vs. non-pentafecta groups (75.6 vs. 75.2; p = 0.6). After RARP, stable QoL rates for CAPRA-S LR vs. HR and pentafecta were 30, 26 and 30%, respectively. Corresponding improved QoL rates were 44, 32 and 47%. In LRM, CAPRA-S and pentafecta criteria were independent predictors of improved QoL. We conclude that most favourable combined outcomes after RARP might confer stable or even improved QoL but up to one third of patients might experience deterioration. This warrants further investigation how to capture the underlying cause and to address and potentially solve these perceived negative effects despite successful RARP.
Similar content being viewed by others

Introduction
Radical prostatectomy (RP) remains a standard treatment option for localised prostate cancer (PCa) with well documented local and long-term PCa control1,2,3. RP patients ideally wish to recover quickly and to preserve a satisfactory long-term quality of life (QoL). Moreover, compared to open RP, robot-assisted radical prostatectomy (RARP) might confer added benefit of better perioperative outcomes4,5,6. Monitoring these outcomes and associated QoL is essential to improve preoperative patient counselling, RARP technique and post-RARP rehabilitation7,8.
It is highly conceivable but largely unexplored that certain combinations of favourable pathological, functional or oncological outcomes of RARP are perceived with best QoL. Specifically, the pentafecta criteria includes a combination of biochemical recurrence (BCR)-free survival, recovery of urinary continence and of erectile function at a specific time-point, as well as negative surgical margin status and absence of surgical complications9,10. Another favourable combined outcome is the postsurgical Cancer of the Prostate Risk Assessment score low risk score (CAPRA-S)11. A low-risk CAPRA-S is based on favourable surgical and pathological characteristics, such as low pre-surgical PSA < 20 ng/ml, pathological Gleason pattern ≤ 4 + 4 and ideally negative surgical margin and localized disease (i.e. no extracapsular extension, seminal vesicle invasion and lymph node invasion12).
For purpose of QoL assessment, the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 (EORTC QLQ-C30) is widely used in cancer patients, including PCa. It is a validated patient-reported outcome measurement (PROM) tool that covers functional scales, symptoms, single items and global QoL13,14,15. Accordingly, it is regularly utilized in clinical trials16 that compare treatment methods, e.g. RP vs. radiotherapy1,17,18,19. In daily clinical practice, as in our institution, it also serves for monitoring QoL after RARP over time20.
It is of note that previous series on EORTC QLQ-C30 and RP mainly relied on exploratory analyses, e.g. mean change of individual EORTC QLQ-C30 scales over time and did not stratify according to specific functional or oncological scenarios. Moreover, most series omitted multivariable analyses19,21,22,23,24 and relied on ORP patients19,21,22. In general, comprehensive data on RARP and EORTC QLQ-C30 is sparse. To date, none applied the EORTC QLQ-C30 Summary Score in the context of RARP, which incorporate most functional and symptom scales and single items. None applied minimal clinically important differences (MCIDs) after RARP to enable intuitive interpretation of QoL effects. Finally, none dedicatedly examined effect of specific favourable patient-centric combined outcomes such as pentafecta or low-risk CAPRA-S on QoL.
Thus, we examined the impact of CAPRA-S risk categories and pentafecta criteria on EORTC QLQ-C30 global QoL and Summary Score in patients treated with RARP and report relevant respective improvement vs. deterioration rates.
Material and methods
Overall, 2871 consecutive PCa patients with complete pathological, surgical and complications data who received RARP at our institution between 5/2006 and 12/2018 were identified. Analyses were restricted to men with complete data on EORTC QLQ C30 at baseline and 24 months after surgery, who were preoperatively continent and who had corresponding follow-up information of urinary continence recovery and information on baseline erectile function. Patients with neoadjuvant androgen deprivation therapy, suspected metastases or with previous local therapy of the prostate were excluded. RARP specimen grading was performed according to 2014 International Society of Urological Pathology standards25.
EORTC-QLQ-C30 and minimum clinically important differences
The questionnaire includes 30 items that can be summarized into 15 scales, i.e. five functional scales (physical, role, emotional, cognitive and social), three symptom scales (fatigue, nausea/vomiting and pain), six singe items (dyspnea, insomnia, appetite loss, constipation, diarrhea, financial impact of disease) and a global QoL (QL).
For our study we utilized the QL and the EORTC QLQ-C30 Summary Score. Latter is calculated by the sum of 13 scales (QL and financial impact are excluded), divided by the number 1311,26,27,28. For calculation, the symptom scales are reversed to obtain a uniform direction of every scale.
We classified MCIDs, i.e. difference of pre- vs. 24 months postoperative EORTC QLQ-C30 scale, as “stable/no change” based on ≤ 5, “minor” based on > 5–10, “moderate” on > 10–20 and “major” on > 20 points29. A positive vs. negative change was classified as improvement vs. deterioration, respectively.
Outcomes
The CAPRA-S is a scoring system based on pre-surgical PSA, pathological Gleason score, surgical margin status, extracapsular extension, seminal vesicle invasion and lymph node invasion12,30. The Patients were stratified according to CAPRA-S into low- (LR), intermediate- (IR) and high-risk (HR) group, based on respective score ranges of 0–2, 3–5 and ≥ 612.
Preoperative potency and recovery of erectile function were defined as combination of International Index of Erectile Function (IIEF-5) score ≥ 1831 and/or score ≥ 3 at the second question32. Recovery of urinary continence was defined as fulfilling following criteria: up to one pad usage within 24 h (safety pad) or score of ≤ 2 at the International Consultation on Incontinence Questionnaire-Urinary Incontinence Short Form Questions 1 and 2 (“How often do you leak urine?” and “How much urine do you usually leak (whether you wear protection or not)?”)33 or finally, the International Continence Society male questionnaire score of ≤ 1 at each of the three questions I2, I3 and I4. For preoperative continence, no preoperative pad usage was allowed. BCR was defined as consecutive PSA rise ≥ 0.2 ng/ml.
Those with recovery of erectile function- and urinary continence and BCR-free-survival within 24 months were classified as having met the trifecta criteria, i.e. ideal functional and oncological outcomes 24 months post-RARP. Those men with preoperative erectile dysfunction, were still modeled as having met the trifecta-criteria if urinary continence recovery and BCR-free-survival within 24 months was observed. Complications were coded according to the Clavien-Dindo classification (CDC)34. Finally, those, who met the combined criteria of negative surgical margins, CDC ≤ 3a and 24-months trifecta were classified as pentafecta group (vs. non-pentafecta).
Statistical analyses
Chi-square test was used for categorical and t-test for continuous variables. For multivariable analyses, we performed logistic regression analyses (LRM) to predict (a) improvement (i.e. at least > 5 points positive change at the individual EORTC QLQ-C30 scale) and (b) absence of deterioration (i.e. stable or even improved EORTC QLQ-C30 scales). LRM was modeled with preoperative EORTC QLQ-C30 scale of interest (QL or Summary Score), 90-day CDC (0-3a[REF] vs. ≥ 3b, i.e. requiring intervention under general anesthesia), CAPRA-S risk groups (LR [REF.] vs. IR vs. HR), which incorporates the surgical margin status, and the 24 months trifecta criteria (non-fulfillment [REF] vs. fulfillment).
All tests were two-sided with a statistical significance set at p < 0.05. Analyses were performed with the statistical package for R (R foundation for Statistical Computing, version 3.2.2).
Ethics approval
The institutional review board at the St. Antonius-Hospital, Gronau, approved the retrospective study design and access to the patients’ medical records. All methods were carried out in accordance with the Declaration of Helsinki. Written informed consent was obtained from individual participants in the study.
Compliance with ethical standards
All authors of this research paper have directly participated in the planning, execution, or analysis of the study. All authors of this paper have read and approved the final version submitted. The contents of this manuscript have not been copyrighted or published previously. The contents of this manuscript are not under consideration for publication elsewhere.
Results
Table 1 demonstrates the baseline characteristics. Median age of the total cohort was 63 years (IQR 59–67) and median PSA was 7.3 ng/ml (IQR 5.4–10.7). RARP ISUP Gleason Grades 1, 2, 3 and ≥ 4 were 36, 29, 22 and 13%, respectively. Respective proportions of pT2, extracapsular extension, seminal vesicle invasion, positive surgical margin and lymph node invasion were 65, 25, 7.7%, 11 and 6.5%. Based on aforementioned clinicopathological metrics, patients were classified as CAPRA-S low-, intermediate and high-risk in 53, 32 and 15% respectively.
The 90-day CDC rates ≤ 3a of the total cohort were 97.6%. At 24 months post-RARP, rates of erectile function and urinary continence recovery, as well as BCR-free survival of the total cohort were 63, 96 and 86%, respectively. Based on negative surgical margin and aforementioned metrics, 24-month pentafecta rates were 51%.
Table 2 demonstrates pre- vs. post-operative mean QL and Summary Score and respective MCID proportions, stratified according to CAPRA-S risk groups and pentafecta vs. non-pentafecta groups. Before RARP there was no statistically significant difference in the QL (75.7, SD 19.4 vs. 75.2, SD 19.4; p = 0.7) nor in Summary Score (91.0, SD 9.2 vs. 91.2 SD 9.2; p = 0.8) between CAPRA-S LR vs. HR. Conversely, 24 months after RARP, there was a statistically significant difference in the QL (79.3, SD 19.3 vs. 73.7, SD 20.7; p < 0.001), as well as Summary Score (90.2, SD 11.5 vs. 87.6, SD 13.4; p < 0.001).
Before RARP, between pentafecta vs. non-pentafecta groups, there was no statistically significant difference in the QL (75.6, SD 19.7 vs. 75.2, SD 18.7; p = 0.6) nor Summary Score (91.3, SD 9.0 vs. 90.7, SD 9.3; p = 0.08). Conversely, 24 months after RARP, there was a statistically significant difference in the QL (80.8, SD 18.3 vs. 74.1, SD 20.2; p < 0.001), as well as Summary Score (91.2, SD 10.3 vs. 87.4, SD 13.1; p < 0.001).
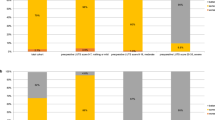
At 24 months after RARP, between CAPRA-S LR vs. HR, QL remained stable in 30 vs. 26% and improved in 44 vs. 32% (p < 0.001). These amounted to 74 vs. 58% without any deterioration in QL. Similarly, the Summary Score remained stable in 56 vs. 51% and improved in 21 vs. 15% (p < 0.001). These amounted to 77 vs. 66% without any deterioration in the Summary Score.
At 24 months after RARP, between pentafecta vs. non-pentafecta groups, QL remained stable in 30 vs. 28% and improved in 47 vs. 34% (p < 0.001). These amounted to 78 vs. 62% without any deterioration in QL. Similarly, the Summary Score remained stable in 60 vs. 50% and improved in 20 vs. 15% (p < 0.001). These amounted to 80 vs. 65% without any deterioration in the Summary Score.
Table 3 shows the multivariable logistic regression model for prediction of improvement of QL and Summary Score at 24 months after robot-assisted radical prostatectomy. LRM included CAPRA-S risk groups and the remaining criteria (i.e. trifecta and CDC) that are utilized for the pentafecta criteria, as well as the preoperative mean score of either QL or Summary Score. Specifically, LRM for prediction of improved QL at 24 months after RARP, yielded following independent predictors: higher preoperative score (OR 0.94, 95% CI 0.93–0.94; p < 0.001), higher risk group of CAPRA-S (HR vs. LR[REF] OR 0.60, 95% CI 0.46–0.78; p < 0.001) as well as 90-d surgical complications that require surgical intervention in general anesthesia (CDC ≥ 3b vs. 0-3a[REF] OR 0.49, 95% CI 0.24–0.99; p = 0.048) were associated with lower chance of improved QoL. Conversely, fulfilment of trifecta criteria was associated with virtually doubled odds of improved QL (OR 1.91, 95% CI 1.59–2.29; p < 0.001).
LRM for prediction of improved Summary Score at 24 months after RARP yielded similar results. However, CDC did not reach independent predictor status for aforementioned scales (OR 0.94, 95% CI 0.42–2.10; p = 0.9).
Finally, LRM for prediction of at least stable or improved QL (or Summary Score) at 24 months, which represents a broader definition of a desirable outcome than just improvement, yielded comparable results (Supplemental Table 1).
Discussion
To date, postoperative QoL metrics in combination with MCID are still rarely reported in context of specific functional or oncological profiles of PCa patients, which were treated with RARP. Interpretability of QoL change is furthermore limited due averaged data, e.g. observed mean EORTC QLQ-C30 values before and after surgery. This requires rectification since QoL metrics serve as important patient counselling tool before surgery, monitoring after surgery and benchmarking tool for comparison with other institutions35,36. Thus, we compared the impact of specific pathological PCa profiles and of the widely adopted pentafecta criteria on key measurements of the EORTC QLQ-C30.
Our study revealed important findings. First, median preoperative QL and Summary Score values were virtually identical between CAPRA-S groups, as well as pentafecta vs. non-pentafecta groups. Such preoperative balance indicates validity of our MCID findings, since MCIDs are calculated as the difference between preoperative vs. postoperative values. Moreover, our preoperative values are highly consistent with randomized trials and indicate a healthy baseline functioning in the majority of our RARP patients and adequate patient selection17,18,19.
Second, despite balanced and healthy baseline values, we are the first to report substantial proportions of RARP patients who improve upon their preoperative global QoL (47%) and Summary Score (20%). Reassuringly, depending on scale, the vast majority of pentafecta patients, 77% (QL) to 80% (Summary Score) do not show any deterioration after RARP, but either remain stable or improve further.
Third of those pentafecta patients reporting deterioration, 8–10%, about a third, are only classified as minor. It is important to note, that deterioration might occur in a specific scale but be absent in another. This is evidenced by the mean change of QL, which is positive in CAPRA-S LR and pentafecta patients and negative in the Summary Score even in the same patients. This is consistent with the general observation of perceived deterioration in cancer patients despite successful treatment and favourable prognosis37.
Fourth, this phenomenon of discrepant perception in scales is further substantiated by multivariable analyses. Despite congruent patterns of the respective impact of CAPRA-S LR and pentafecta profiles on individual QL and Summary Score scales, LRM clearly demonstrated that CAPRA-S risk profiles are independent of the pentafecta criteria. For example, an individual with CAPRA-S high-risk profile and simultaneous pentafecta criteria might perceive certain scales as deteriorated due to greater weight on PCa risk than outcomes. In consequence, pathology and functional outcomes, should be considered in patients counselling.
It is important to note that a high-risk CAPRA-S score strongly correlates with adjuvant/salvage androgen deprivation therapy and/or radiotherapy, which is expected12,30. Accordingly, in context of QoL, an increasing CAPRA-S should also be interpreted as higher risk of biochemical recurrence and administration of additional therapy after RARP that potentially further contributes to a negative impact on QoL1,18,32,38,39,40.
With regard to functional outcomes, erectile aid such as phosphodiesterase type-5 inhibitors or intraurethral/intracavernosal application of alprostadil and urinary continence treatments such as male sling procedures or artificial urinary sphincter implantation ideally promote recovery of erectile function or urinary continence, respectively. These might translate to stable or improved QoL. This notion is substantiated by about 44% of preoperatively potent patients in our pentafecta group, who used erectile aids at time of erectile function recovery.
Finally, it is also important to point out that CAPRA-S LR vs. HR represents a distinct contrast, whereas pentafecta vs. non-pentafecta does not. Specifically, the difference is highly variable and might only contain minor differences compared to the very strict concept of pentafecta. However, this notion strengthens our findings of significant differences between pentafecta vs. non-pentafecta effects on QoL.
Our study has limitations. First, despite regular adoption of EORTC QLQ-C30 in randomized cancer trials, most MCIDs are not validated yet for PCa. We utilized the widely accepted MCID definition by Osoba et al.29 Although it was based on patients with breast and small-cell lung cancer, several subsequent series confirmed 10 point changes or more as being clinically significant after collating results from various studies and various cancer sites including PCa41,42. Our approach of MCIDs enables superior interpretation compared to simply reporting mean value as the majority of preceding series.
Second, we are also the first to report the validated EORTC QLQ-C30 Summary Score for RARP patients to complement global QoL11,26,27,28. Specifically, the Summary Score was validated as prognostic factor for survival11. Moreover, we aimed to improve interpretability and robustness of the scales/items in concatenated fashion as opposed to presenting each individual scales/items. Since the Summary Score represents a mean of aforementioned components, MCIDs could be applied accordingly. However, MCIDs are not validated yet for the Summary Score. Nonetheless, the direction and extent of change is transparently demonstrated in our study.
Third, since pentafecta outcomes are composed of time-to-event variables it is mandatory to focus on a specific time point after RARP, e.g. 24 months, for purpose of examining the relationship between the pentafecta outcome and QoL. This represents an inherent flaw of the pentafecta concept. For example, longer post-RARP follow-up will be associated with higher oncological failure rates that lead to pentafecta exclusion vs. increased recovery rates that lead to pentafecta inclusion. At 24 months post-RARP, QoL is likely more influenced by functional recovery than BCR. Conversely, post-RARP QoL might further improve or deteriorate after 24 months, since previous series indicate that QoL values stabilize after up to 6 years in absence of further interventions20.
Finally, it is important to note that surgical expertise is essential to achieve favorable combined outcomes and that different learning curves are needed for specific outcomes43,44. Specifically, previous series reported a shorter learning curve for achieving satisfactory outcomes for continence, followed by a longer curve for potency and then for surgical margins45. This is evidenced by a significantly higher surgical expertise in the pentafecta group (median 767, IQR 174–212 vs. 552, IQR 140–1750; p < 0.001). In the same context, generalizability of our findings are limited since our department represents a specialized prostate cancer center with highly experienced robotic surgeons.
Conclusions
We confirm that favourable pathology, oncological and functional outcomes independently confer not only stability, but even positive change on specific QoL measurements in the vast majority of RARP patients. However, optimal outcomes after treatment do not guarantee best perceived QoL, since up to one third of patients might experience deterioration. This warrants further investigation of how to capture the underlying cause and how to finally address and potentially solve these perceived negative effects of PCa despite successful RARP.
Data availability
Full availability.
Code availability
Full availability.
Abbreviations
- BCR:
-
Biochemical recurrence
- CAPRA-S:
-
Postsurgical Cancer of the Prostate Risk Assessment score
- CDC:
-
Clavien–Dindo classification
- EORTC QLQ-C30:
-
European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30
- HR:
-
High risk
- IIEF-5:
-
International Index of Erectile Function
- LR:
-
Low risk
- LRM:
-
Multivariable logistic regression analyses
- MCID:
-
Minimal clinical improvement difference
- PCa:
-
Prostate cancer
- PROM:
-
Patient-reported outcome measurement
- PSA:
-
Prostate specific antigen
- RARP:
-
Robot-assisted radical prostatectomy
- RP:
-
Radical prostatectomy
- SD:
-
Standard deviation
- QL:
-
Global quality of life
- QoL:
-
Quality of life
References
Hamdy, F. C. et al. 10-year outcomes after monitoring, surgery, or radiotherapy for localized prostate cancer. N. Engl. J. Med. 375, 1415–1424. https://doi.org/10.1056/NEJMoa1606220 (2016).
Abdollah, F. et al. Functional outcomes of clinically high-risk prostate cancer patients treated with robot-assisted radical prostatectomy: A multi-institutional analysis. Prostate Cancer Prostatic Dis. 20, 395–400. https://doi.org/10.1038/pcan.2017.26 (2017).
Lei, J. H. et al. Systematic review and meta-analysis of the survival outcomes of first-line treatment options in high-risk prostate cancer. Sci. Rep. 5, 7713. https://doi.org/10.1038/srep07713 (2015).
Reisz, P. A. et al. Assessing the quality of surgical care for clinically localized prostate cancer: Results from the CEASAR study. J. Urol. 204, 1236–1241. https://doi.org/10.1097/JU.0000000000001198 (2020).
Lee, M. J., Park, D. A. & Lee, S. H. Utility after robot-assisted radical prostatectomy compared to conventional approaches for localized prostate cancer [socioeconomic perspective study]. Prostate Cancer Prostatic Dis. 22, 461–466. https://doi.org/10.1038/s41391-018-0119-9 (2019).
Suh, J. et al. Differences in risk factors for biochemical recurrence after radical prostatectomy stratified by the degree of obesity: Focused on surgical methods. Sci. Rep. 10, 10157. https://doi.org/10.1038/s41598-020-67237-6 (2020).
Lopez, P., Taaffe, D. R., Newton, R. U., Buffart, L. M. & Galvao, D. A. What is the minimal dose for resistance exercise effectiveness in prostate cancer patients? Systematic review and meta-analysis on patient-reported outcomes. Prostate Cancer Prostatic Dis. 24, 465–481. https://doi.org/10.1038/s41391-020-00301-4 (2021).
Leyh-Bannurah, S. R. et al. Improvement of quality of life and symptom burden after robot-assisted radical prostatectomy in patients with moderate to severe LUTS. Sci. Rep. 11, 16757. https://doi.org/10.1038/s41598-021-95525-2 (2021).
Patel, V. R. et al. Pentafecta: A new concept for reporting outcomes of robot-assisted laparoscopic radical prostatectomy. Eur. Urol. 59, 702–707. https://doi.org/10.1016/j.eururo.2011.01.032 (2011).
Patel, V. R. et al. Continence, potency and oncological outcomes after robotic-assisted radical prostatectomy: Early trifecta results of a high-volume surgeon. BJU Int. 106, 696–702. https://doi.org/10.1111/j.1464-410X.2010.09541.x (2010).
Husson, O. et al. The EORTC QLQ-C30 summary score as prognostic factor for survival of patients with cancer in the “real-world”: Results from the population-based PROFILES registry. Oncologist. 25, e722 (2020).
Punnen, S. et al. Multi-institutional validation of the CAPRA-S score to predict disease recurrence and mortality after radical prostatectomy. Eur. Urol. 65, 1171–1177. https://doi.org/10.1016/j.eururo.2013.03.058 (2014).
Aaronson, N. K. et al. The European Organization for Research and Treatment of Cancer QLQ-C30: A quality-of-life instrument for use in international clinical trials in oncology. J. Natl. Cancer Inst. 85, 365–376. https://doi.org/10.1093/jnci/85.5.365 (1993).
Giesinger, J. M. et al. Past and current practice of patient-reported outcome measurement in randomized cancer clinical trials: A systematic review. Value Health 24, 585–591. https://doi.org/10.1016/j.jval.2020.11.004 (2021).
Efficace, F. et al. Patient-reported outcomes as independent prognostic factors for survival in oncology: Systematic review and meta-analysis. Value Health 24, 250–267. https://doi.org/10.1016/j.jval.2020.10.017 (2021).
Duchesne, G. M. et al. Health-related quality of life for immediate versus delayed androgen-deprivation therapy in patients with asymptomatic, non-curable prostate cancer (TROG 03.06 and VCOG PR 01–03 [TOAD]): A randomised, multicentre, non-blinded, phase 3 trial. Lancet Oncol. 18, 1192–1201. https://doi.org/10.1016/S1470-2045(17)30426-6 (2017).
Crook, J. M. et al. Comparison of health-related quality of life 5 years after SPIRIT: Surgical prostatectomy versus interstitial radiation intervention trial. J. Clin. Oncol. 29, 362–368. https://doi.org/10.1200/JCO.2010.31.7305 (2011).
Donovan, J. L. et al. Patient-reported outcomes after monitoring, surgery, or radiotherapy for prostate cancer. N. Engl. J. Med. 375, 1425–1437. https://doi.org/10.1056/NEJMoa1606221 (2016).
Giberti, C., Chiono, L., Gallo, F., Schenone, M. & Gastaldi, E. Radical retropubic prostatectomy versus brachytherapy for low-risk prostatic cancer: A prospective study. World J. Urol. 27, 607–612. https://doi.org/10.1007/s00345-009-0418-9 (2009).
Lardas, M. et al. Quality of life outcomes after primary treatment for clinically localised prostate cancer: A systematic review. Eur. Urol. 72, 869–885. https://doi.org/10.1016/j.eururo.2017.06.035 (2017).
Bach, P., Döring, T., Gesenberg, A., Möhring, C. & Goepel, M. Quality of life of patients after retropubic prostatectomy-pre-and postoperative scores of the EORTC QLQ-C30 and QLQ-PR25. Health Qual. Life Outcomes 9, 1–9 (2011).
Loppenberg, B. et al. Effect of perioperative complications and functional outcomes on health-related quality of life after radical prostatectomy. Qual. Life Res. 23, 2743–2756. https://doi.org/10.1007/s11136-014-0729-1 (2014).
Pompe, R. S. et al. Short- and long-term functional outcomes and quality of life after radical prostatectomy: Patient-reported outcomes from a tertiary high-volume center. Eur. Urol. Focus 3, 615–620. https://doi.org/10.1016/j.euf.2017.08.001 (2017).
Jurys, T. & Durmala, J. Quality of life assessment using EORTC QLQ questionnaires in the prostate cancer population treated with radical prostatectomy: A systematic review. Scand. J. Urol. 55(2), 90–97 (2021).
Epstein, J. I. et al. The 2014 International Society of Urological Pathology (ISUP) Consensus Conference on gleason grading of prostatic carcinoma: Definition of grading patterns and proposal for a new grading system. Am. J. Surg. Pathol. 40, 244–252. https://doi.org/10.1097/PAS.0000000000000530 (2016).
Pompili, C. et al. EORTC QLQ-C30 summary score reliably detects changes in QoL three months after anatomic lung resection for Non-Small Cell Lung Cancer (NSCLC). Lung Cancer 123, 149–154. https://doi.org/10.1016/j.lungcan.2018.07.021 (2018).
Giesinger, J. M. et al. Replication and validation of higher order models demonstrated that a summary score for the EORTC QLQ-C30 is robust. J. Clin. Epidemiol 69, 79–88 (2016).
Giesinger, J. M. et al. Thresholds for clinical importance were established to improve interpretation of the EORTC QLQ-C30 in clinical practice and research. J. Clin. Epidemiol. 118, 1–8. https://doi.org/10.1016/j.jclinepi.2019.10.003 (2020).
Osoba, D., Rodrigues, G., Myles, J., Zee, B. & Pater, J. Interpreting the significance of changes in health-related quality-of-life scores. J. Clin. Oncol. 16, 139–144. https://doi.org/10.1200/JCO.1998.16.1.139 (1998).
Cooperberg, M. R., Hilton, J. F. & Carroll, P. R. The CAPRA-S score: A straightforward tool for improved prediction of outcomes after radical prostatectomy. Cancer 117, 5039–5046. https://doi.org/10.1002/cncr.26169 (2011).
Ficarra, V. et al. Retropubic, laparoscopic, and robot-assisted radical prostatectomy: A systematic review and cumulative analysis of comparative studies. Eur. Urol. 55, 1037–1063. https://doi.org/10.1016/j.eururo.2009.01.036 (2009).
Leyh-Bannurah, S. R. et al. Perioperative and postoperative outcomes of robot-assisted radical prostatectomy in prostate cancer patients with prior transurethral subvesical deobstruction: Results of a high-volume center. J. Urol. 206, 308–318. https://doi.org/10.1097/JU.0000000000001776 (2021).
Avery, K. et al. ICIQ: A brief and robust measure for evaluating the symptoms and impact of urinary incontinence. Neurourol. Urodyn. 23, 322–330. https://doi.org/10.1002/nau.20041 (2004).
Dindo, D., Demartines, N. & Clavien, P. A. Classification of surgical complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 240, 205–213. https://doi.org/10.1097/01.sla.0000133083.54934.ae (2004).
Mitchell, K. R. et al. Exploratory factor analysis of a patient-centered cancer care measure to support improved assessment of patients’ experiences. Value Health 23, 351–361. https://doi.org/10.1016/j.jval.2019.10.004 (2020).
O’Callaghan, M. E. et al. Tools for predicting patient-reported outcomes in prostate cancer patients undergoing radical prostatectomy: A systematic review of prognostic accuracy and validity. Prostate Cancer Prostatic Dis. 20, 378–388. https://doi.org/10.1038/pcan.2017.28 (2017).
Wang, S. Y. et al. Association between time since cancer diagnosis and health-related quality of life: A population-level analysis. Value Health 19, 631–638. https://doi.org/10.1016/j.jval.2016.02.010 (2016).
Dacal, K., Sereika, S. M. & Greenspan, S. L. Quality of life in prostate cancer patients taking androgen deprivation therapy. J. Am. Geriatr. Soc. 54, 85–90. https://doi.org/10.1111/j.1532-5415.2005.00567.x (2006).
Ervandian, M. et al. Late urinary morbidity and quality of life after radical prostatectomy and salvage radiotherapy for prostate cancer(). Scand. J. Urol. 51, 457–463. https://doi.org/10.1080/21681805.2017.1354314 (2017).
Cheung, A. S. et al. Quality of life decrements in men with prostate cancer undergoing androgen deprivation therapy. Clin. Endocrinol. (Oxf.) 86, 388–394. https://doi.org/10.1111/cen.13249 (2017).
King, M. T. The interpretation of scores from the EORTC quality of life questionnaire QLQ-C30. Qual. Life Res. 5, 555–567. https://doi.org/10.1007/BF00439229 (1996).
Cocks, K. et al. Evidence-based guidelines for interpreting change scores for the European Organisation for the Research and Treatment of Cancer Quality of Life Questionnaire Core 30. Eur. J. Cancer 48, 1713–1721. https://doi.org/10.1016/j.ejca.2012.02.059 (2012).
Bravi, C. A. et al. The impact of experience on the risk of surgical margins and biochemical recurrence after robot-assisted radical prostatectomy: A learning curve study. J. Urol. 202, 108–113. https://doi.org/10.1097/JU.0000000000000147 (2019).
Thompson, J. E. et al. Superior biochemical recurrence and long-term quality-of-life outcomes are achievable with robotic radical prostatectomy after a long learning curve-updated analysis of a prospective single-surgeon cohort of 2206 consecutive cases. Eur. Urol. 73, 664–671. https://doi.org/10.1016/j.eururo.2017.11.035 (2018).
Lavery, H. J. et al. The advanced learning curve in robotic prostatectomy: A multi-institutional survey. J. Robot. Surg. 3, 165. https://doi.org/10.1007/s11701-009-0154-6 (2009).
Funding
Open Access funding enabled and organized by Projekt DEAL. We acknowledge support from the University of Muenster.
Author information
Authors and Affiliations
Contributions
S.R.L.B. had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. Study concept and design: J.H.W., S.R.L.B., M.M., T.K. Acquisition of data: J.H.W., C.W., A.S., N.L., T.K., P.R., M.M., S.R.L.B., K.U., T.J. Analysis and interpretation of data: T.K., M.M., J.H.W., S.R.L.B., C.W., M.O., N.K. Drafting of the manuscript: T.K., J.H.W., S.R.L.B., M.M., M.K., T.J. Critical revision of the manuscript for important intellectual content: J.H.W., C.W., A.S., N.L., T.K., M.M., M.O., S.R.L.B., N.K., T.J. Statistical analysis: S.R.L.B., C.W. Obtaining funding: K.U. Administrative, technical, or material support: M.M., K.U., N.K. Supervision: S.R.L.B., C.W., J.H.W. Other: None.
Corresponding author
Ethics declarations
Competing interests
Jorn H. Witt is a paid proctor und consultant for Intuitive Surgical and Board member of the German Society of Robot-assisted Urology. Christian Wagner is a paid proctor and consultant for Intuitive Surgical and Board member of the German Society of Robot-assisted Urology. The other authors have no conflicts of interest to declare.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Karagiotis, T., Witt, J.H., Jankowski, T. et al. Two-year quality of life after robot-assisted radical prostatectomy according to pentafecta criteria and cancer of the prostate risk assessment (CAPRA-S). Sci Rep 12, 244 (2022). https://doi.org/10.1038/s41598-021-04289-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-021-04289-2
This article is cited by
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
