
Abstract
This study aims to investigate the associative and multivariate relationship between different sociodemographic and clinical variables with cortical excitability as indexed by transcranial magnetic stimulation (TMS) markers in subjects with chronic pain caused by knee osteoarthritis (OA). This was a cross-sectional study. Sociodemographic and clinical data were extracted from 107 knee OA subjects. To identify associated factors, we performed independent univariate and multivariate regression models per TMS markers: motor threshold (MT), motor evoked potential (MEP), short intracortical inhibition (SICI), intracortical facilitation (ICF), and cortical silent period (CSP). In our multivariate models, the two markers of intracortical inhibition, SICI and CSP, had a similar signature. SICI was associated with age (β: 0.01), WOMAC pain (β: 0.023), OA severity (as indexed by Kellgren–Lawrence Classification) (β: − 0.07), and anxiety (β: − 0.015). Similarly, CSP was associated with age (β: − 0.929), OA severity (β: 6.755), and cognition (as indexed by the Montreal Cognitive Assessment) (β: − 2.106). ICF and MT showed distinct signatures from SICI and CSP. ICF was associated with pain measured through the Visual Analogue Scale (β: − 0.094) and WOMAC (β: 0.062), and anxiety (β: − 0.039). Likewise, MT was associated with WOMAC (β: 1.029) and VAS (β: − 2.003) pain scales, anxiety (β: − 0.813), and age (β: − 0.306). These associations showed the fundamental role of intracortical inhibition as a marker of adaptation to chronic pain. Subjects with higher intracortical inhibition (likely subjects with more compensation) are younger, have greater cartilage degeneration (as seen by radiographic severity), and have less pain in WOMAC scale. While it does seem that ICF and MT may indicate a more acute marker of adaptation, such as that higher ICF and MT in the motor cortex is associated with lesser pain and anxiety.
Similar content being viewed by others
Introduction
Chronic pain is one of the main causes of disability worldwide1 and a major burden of knee osteoarthritis (OA), causing impaired function and decreased quality of life2. The chronic pain caused by OA sometimes is not correlated with the severity of the peripheral injury. Neuroplastic changes in pain-related circuits, resulting in maladaptive neuroplasticity, lead to a perpetuation of pain3,4. This process has been shown in other chronic pain conditions such as phantom limb pain, fibromyalgia, and low back pain, supporting the idea of a central nervous system modulation of chronic pain5,6. In these cases, central sensitization of nociceptive pathways may be present, which, along with an impairment in the descending pain modulation pathway, plays an essential role in how patients perceive pain in the long term2,7. These modifications on the central nervous system imply an imbalance of the neural stability between excitability and inhibition8. Current evidence has shown that a deficit in neuronal inhibition occurs in patients with motor disability and pain conditions9,10,11 and this lack of cortex inhibition is associated with more disability12. In fact, one of the contributors of pain in these patients may be an impaired cortical inhibitory system that cannot compensate for excessive peripheral increased nociception.
The specific mechanisms involved in excitability-inhibition balance and brain plasticity regulation are not completely understood. In these circumstances, transcranial magnetic stimulation is a commonly used and feasible tool to measure the functional level of motor cortex excitability13,14,15 through markers such as resting motor threshold (rMT), the intensity of a stimulus necessary to produce a motor evoked potential (MEP) which is the electrical signal sent through descending neural pathways when the motor cortex is stimulated, both indirect markers of corticospinal excitability; cortical silent period (CSP), which represents momentary suppression of MEP due to GABAergic inhibition; and short intracortical inhibition (SICI) and intracortical facilitation (ICF), which represent inhibitory and excitatory activation of interneurons within the motor cortex16,17. A systematic review on TMS finding in chronic pain patients reported reduced SP and SICI; however, most of the included studies were underpowered (less than 30 participants), included heterogenous populations, and did not assess which clinical variables are associated with this reduced cortical inhibition18.
Our main hypothesis is that clinical characteristics in OA subjects, such as pain, motor function, and cognitive-emotional behavior, are associated with the quantity of intracortical inhibition (and other parameters of excitability). For this reason, the objective of this study is to investigate the association of different sociodemographic and clinical variables and the cortex excitability conveyed by MT, MEP, CSP, SICI, and ICF TMS markers in subjects with chronic pain caused by knee OA. Considering that the central mechanisms of chronic pain are important in knee OA, the cortical excitability measures (as assessed by TMS) could indicate the neuroplastic alterations in this condition21. Therefore, understanding their association with clinical and demographic factors can possibly contribute to the identification of specific OA populations with less or more maladaptive plasticity (who might chronify pain easily). Knowing these associated factors is the starting point for phenotype chronic pain associated with knee OA and thus develop more precise treatments.
Results
Table 1 summarizes the descriptive characteristics of the study sample. Pain is reported as moderate in both knees and patients present with low cognitive, anxiety, and depression scores.
Short intracortical inhibition (SICI)
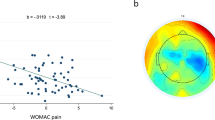
Short Intracortical Inhibition conveyed some significant associated variables in its univariate analysis including age (p = 0.039), gender (p = 0.074), and Berg Balance Scale results (p = 0.053) (Table 2). From our multivariate model, age is depicted as a positive associated variable to SICI (β: 0.011, 95% CI 0.003 to 0.017; p = 0.004); as patients get older, they have less cortical inhibition (as indexed by SICI). Similarly, the WOMAC pain scale scores also portrayed a positive correlation with SICI (β 0.024, 95% CI 0.008 to 0.041; p = 0.004), indicating that the more pain a patient feels, less SICI occurs. A significant negative correlation was found between the Kellgren-Lawrence classification and SICI (β − 0.070, 95% CI − 0.12 to − 0.017; p = 0.001). Given a positive relationship between OA severity and SICI, the more severe K–L classification, larger cortical inhibition. HADS-anxiety also demonstrated a small inverse correlation (β − 0.015, 95% CI − 0.030 to 0.0003, p = 0.046). Moreover, other variables were confounders, such as BMI and Conditioned Pain Modulation (CPM) (Table 2).
Cortex silent period (CSP)
Possible relevant associated variables with CSP in knee OA chronic pain in the univariate analysis were BMI (p = 0.008), left knee Kellgren–Lawrence severity classification (p = 0.075), total arthroplasty (p = 0.026), right knee visual analogue pain scale score (p = 0.014), and total MoCA cognitive assessment scores (p = 0.079) (Table 3). In our multivariate model, we found a strong, positive correlation between the KL average score for both knees was identified (β: 6.755, 95% CI: 0.662 to 12.848; p = 0.030), implying that the more severe OA patients have, the higher their silent period amplitude (therefore, higher intracortical inhibition). Moreover, negative correlations between CSP and age (β: − 0.929, 95% CI − 1.678 to − 0.181; p = 0.016) and MoCA scores (β: − 2.106, 95% CI − 3.64 to − 0.568; p = 0.008) indicate inverse linear relationships meaning that as a patient gets older, their SP is diminished, and the higher cognitive function these patients have, the less CSP they depict. Education level was included in the model as it is a significant confounder given its relationship to MoCA (Table 3).
BMI Body Mass Index, WOMAC Pain/Stiffness/Function Western Ontario and MacMaster Universities Osteoarthritis Index Pain/Stiffness/Function section, HAM-D Hamilton Depression Rating Scale, HAD-Anxiety Hospital Anxiety and Depression Scale-Anxiety section.
Intracortical facilitation (ICF)
Univariate analysis of associated factors to intracortical facilitation (ICF) conveyed significance for time of ongoing pain (p = 0.062), the visual analogue scale pain score (p = 0.03) and the anxiety subscale of the Hospital Anxiety and Depression Scale (HADS) (p = 0.044) (Table 4). The final multivariate model demonstrated significant negative correlation with VAS pain score average (β: − 0.094, 95% CI − 0.175 to − 0.013; p = 0.024), patients with higher VAS pain scores have decreased facilitation. Additionally, we found a positive correlation between facilitation and the WOMAC pain subscale score (β: 0.062, 95% CI 0.011 to 0.113, p = 0.018), facilitation is increased the more pain patients report through this scale in contrast with the VAS correlation. Finally, the HADS anxiety subscale was negatively correlated with ICF (β: − 0.039, 95% CI − 0.078 to − 0.0007, p = 0.046), meaning higher the anxiety level smaller the ICF. Additional variables were included into the model as they were significant confounders such as gender, BMI, and pain threshold (Table 4).
Motor threshold (MT)
In the final, multivariate model, significance was conveyed in age (p = 0.037), the WOMAC pain score (p = 0.035), the bilateral average of the VAS pain score (p = 0.013), and the anxiety section of the Hospital Anxiety and Depression Scale (HADS) (p = 0.034) (Table 5). A linear, inverse relationship was found between age and motor threshold (β: − 0.306, 95% CI − 0.59 to − 0.018, p = 0.037) meaning, there is a decline in motor threshold as one gets older. An inverse relationship was also seen with the HADS for anxiety (β: − 0.813, 95% CI − 1.56 to − 0.062, p = 0.034); the higher the patient's anxiety, according to their score, the lower their motor threshold. Moreover, in the scope of pain, different significant relationships were identified in consonance with the assessment performed; the more pain a patient feels, as reported by their WOMAC score, the higher their motor threshold conveying a positive correlation between the assessment and the marker (β: 1.029, 95% CI 0.075 to 1.980, p = 0.035). Notwithstanding, the higher pain reported by patients on their VAS score, the lower their motor threshold, depicting a negative correlation (β: − 2.003, 95% CI − 3.566 to − 0.438, p = 0.013). Thus, a paradoxical difference between the two pain-rating scales can be observed. We identified the following confounders: gender, conditioned pain modulation (CPM), and time of ongoing pain, which were included into the model.
Motor evoked potential (MEP)
Motor evoked potential (MEP) univariate analysis only shows a positive significant correlation between left total knee arthroplasty (β: 2.664, p = 0.001, 95% CI: 1.097 to 4.230) and MEP in OA (Table 6). Nonetheless, this significance is not upheld in the final multivariate model. Moreover, no other significant findings are portrayed in the final MEP multivariate model, indicating no cognitive-emotional, functional, or pain relationship between the chronic pain related to OA and MEP.
Discussion
Summary of the study’s main findings
This study aimed to explore the association of different sociodemographic and clinical variables and the cortex excitability conveyed by MT, MEP, CSP, SICI, and ICF TMS markers in subjects with chronic pain due to OA. This is one of the first studies exploring the association between TMS measurements of cortex excitability and clinical and demographic variables in a large sample of chronic knee OA pain18, looking to understand better how maladaptive mechanisms linked with chronic pain work and may be expressed by these neurophysiological markers. Our main findings showed important relationships between clinical and demographic variables and cortical excitability markers indexed by TMS. Multivariate analyses conveyed age, OA severity, anxiety, cognitive function, and pain measured by the WOMAC scale as significant variables associated with cortical inhibition (indexed by SICI and CSP), and anxiety and pain associated with intracortical facilitation (represented by ICF and MT) in chronic knee OA pain patients.
Intracortical inhibition and age
We found a direct relationship between age and intracortical inhibition, showing that as subjects with chronic pain get older, inhibition decreases. As discussed above, these findings are similar with our other models, relating the disinhibited state with older patients. Intracortical inhibition develops gradually during the first two decades of life, is maximal during young adulthood, and declines with age19,20. In these studies, Mall et al. have shown that children presented a higher ICI ratio (0.71) when compared with adolescents (0.33), and adults (0.21), meaning that the cortical inhibition tend to decrease with age. Moreover, Peinemann et al. main findings have supported and demonstrated a linear age-related decline in intracortical inhibition in healthy subjects (r = 0.234). It is difficult here to detangle whether this relationship between age and ICI is also enhanced by their OA diagnosis. However, these results show that the mechanism of ICI decreases over time and thus may contribute to worse adaptation in older age.
Additionally, the cortical silent period showed an inverse association with age, this means that as subjects get older, the duration of this period decreases, thus there is less intracortical inhibition. These results are therefore similar to those found regarding the SICI stated above and with some other studies that elderly patients present less cortical inhibition21. An important question that we may answer is that this relationship is not related to the time of ongoing pain since this variable was not significant in our two models (SICI and CSP).
However, age was not seen associated with ICF and MEP in the present study. This lack of association was present in previous research20,22. Therefore, the relationship between the age and intracortical excitability seems to be specific for intracortical inhibition. In fact, results seem to be mixed with some studies showing no association, some of them show less ICF in older people23, and, in others older subjects have shown a higher short ICF24. Thus, more powerful analyses may help to understand this relationship better. Likewise, our study did not detect a relationship between age and MEP. Given that MEP is a general measure of corticospinal excitability and thus has a low specificity, this result also favors the notion that an age-related decrease in intracortical inhibition is specific for this population.
On the other hand, previous studies have shown that the aging process is correlated with the decreasing in the MEP in health subjects25. One limitation of this study is the uneven age distribution, since OA is a disease present in a specific age range26. Therefore, a study with a more uniform distribution of age in a chronic pain population is needed to explore more consistently the relationship of MEP and age in this population.
Intracortical excitability, VAS and WOMAC Pain
Regarding pain, one of the main findings of our study is that there was a direct association with the WOMAC scale for pain, showing that pain-related activity is associated with lower cortical inhibition. These results corroborate with our hypothesis that patients with less physical activity (in this case because of pain) have less cortical inhibition and thus likely less cortical compensation that may lead to more pain27. Our findings support the idea that higher cortical excitability is present in mechanisms of knee osteoarthritis. The relationship between this potential disinhibited state and chronic pain was found in previous studies in patients with chronic pain due to other etiologies, like fibromyalgia18,28.
However, VAS was not associated with measures of intracortical inhibition (CSP and SICI). This is an interesting finding, besides expected. We have shown in several studies that pain intensity does not correlate with ICI6,9. In a review, Santos et al. analyzed ICI and CSP in studies targeting individuals with limb amputation and most of these showed no relationship between cortical excitability and pain intensity9. Additionally, Teixeira et al. were not able to find any association between changing in cortical excitability and pain intensity, analyzing longitudinal data from a clinical trial targeting subjects with phantom limb pain6. However, intracortical inhibition seems to be a marker of adaptation to chronic pain18,29. It may indicate a dysfunctional sensory system and central adaptation. Although, after this system is overcome then pain intensity is likely modulated by other factors, such as emotional affective factors that are likely associated with VAS as shown by other studies30,31.
Furthermore, our study did not find any significant relationship between the cortical silent period and the pain scales used to evaluate knee OA pain in this study, including WOMAC pain. Although we expected that CSP and SICI would have similar results as both measure intracortical inhibition, they measure different inhibitory pathways, while SICI measures GABA-A pathways, CSP is related to the GABA-B system32, what could explain the divergent results. Other studies also relate inverse correlation between CSP and pain modulatory systems, relating the relationship with central sensitization and the existing inflammatory process of knee OA21.
Finally, in our ICF model, similar to the findings for the MT measurement, a negative correlation is found with VAS pain scores and ICF, juxtaposing the WOMAC findings. Given that both VAS and WOMAC are validated and sensitive scales to evaluate pain in knee OA33, their conflicting correlations found in pain according to MT and ICF assessments suggest that these two assessments evaluate different aspects of pain. The WOMAC scale consists of five items, all of which ask the subject about pain while performing a specific movement or motor function34. On the other hand, VAS is a single-question assessment that inquiries about pain in a broadened sense, which relates deeply to the subject’s perception of pain as a whole, rather than when performing specific tasks30. WOMAC pain is a subscale that it is not usually use in isolation for clinical purposes. Although, both scales assess pain including all biopsychosocial domains. VAS and WOMAC pain scales are weighting differently some domains. WOMAC gives more weight to the sensorimotor and movement-related domains of pain perception (although the other domains are still in play). On the other hand, VAS asks a single question about the pain intensity, which encompasses all the biopsychosocial aspect of pain. The different contexts of evaluation brought by these two pain scales could explain the contradicting results in our model. Additionally, our finding regarding the VAS reinforces previous studies’ results, in which the same negative association between the ICF and VAS in patients with phantom limb pain was found6,35,36. All these finds may show that the VAS is not a good tool regarding cortex excitability.
Cartilage damage (Kellgren Lawrence classification) and intracortical inhibition
We found an interesting association between SICI and Kellgren Lawrence Classification, this means that higher K-L scores are associated with more inhibition. The K–L score indicates the amount of cartilage damage. This correlation therefore shows that intracortical inhibition appears to be a mechanism of compensation to the amount of cartilage damage. This also provides a potential explanation for why K-L is not the main determinant of pain. In other words, some subjects with low pain and high K-L have likely larger cortical inhibition. This could be a body temptation to reduce the perception of pain in those patients with the more severe disease. Moreover, this result corroborates with what was found in the CSP model, as stated below.
A significant positive correlation has been found between the Kellgren-Lawrence Classification for OA severity and the cortical silent period meaning that the higher severity of OA, the longer the cortical silent period, meaning more intracortical inhibition. OA severity has been seen to respond differently to chronic pain mechanisms including the process of central pain sensitization37. This is the main reason why central sensitization is still not a broadly recognized mechanism of knee OA pain. Additionally, studies have reported that patients with low pain sensitivity and advanced disease do not respond as well to brain stimulation techniques, indicating that central sensitization might not be a mechanism for all individuals with knee osteoarthritis37.
On the other hand, in our study, no relationship between the OA severity (indexed by K-L classification) and ICF, MT, or MEP was found. This result again shows that intracortical inhibition seems to be a specific marker of compensation to OA, rather than a general change in excitability.
Emotional affective system and intracortical excitability
Anxiety has been intimately related to chronic pain and the modulation of noxious descending pathways. Our results convey a significant negative relationship between anxiety, SICI and ICF. This goes against other studies that convey increased cortical facilitation and decreased inhibition in individuals with psychiatric disorders, conveying dysfunctional GABAergic pathways and increased glutamatergic NMDA activity38. An explanation for our conflicting findings may be that the literature conveys dysfunctional pathways in subjects with diagnosed psychiatric disorders38. Meanwhile, our sample only conveys subjects with mild anxiety traits (as evidenced by the mean HAD-Anxiety scale core of 5.92). Thus, the anxiety levels conveyed by our sample are not enough to trigger malfunctioning cortical pathways and instead, might offer a compensatory mechanism, suggesting a bimodal model of anxiety related to cortical inhibition in pain settings. This model is seen in a study done in healthy subjects depicting that subjects with different levels of anxiety convey different tolerances to pain; patients sensible to anxiety traits have higher pain tolerance and higher levels of anxiety are related to hyperalgesia39.
Although, given we were assessing the primary motor cortex, we found a relatively minor influence of anxiety and depression in intracortical excitability in ICI and ICF, and no association with CSP, MT, and MEP. These results are similar to previous studies that tested the association of emotional measurement and motor cortical excitability40,41. This shows therefore that the effects of the emotional system on pain are independently on the compensation effects of the primary motor cortex on pain.
Cognition and intracortical excitability
Several studies have contributed to understanding the mechanisms behind the relationship between cognition and cortical excitability in the chronic pain field42. The literature also contributes to the understanding of the relationship between cognition and cortical inhibition. We found that MoCA is negatively correlated with CSP, meaning lower MoCA scores indicate longer CSPs. This finding correlates to other results that link cognitive impairment with longer duration CSP found in patients with mild cognitive impairment and Alzheimer's disease43. It is thought that CSP directly displays GABA-B slow inhibition activity which is activated by glutamatergic receptors44. In individuals with cognitive impairment, fast glutamatergic transmissions stimulate GABA-b slow-mediated inhibition which prolongs CSP, explaining the negative correlation between MoCA Scores and CSP43,45. We also hypothesize that the relationship between shorter CSP (therefore, less inhibition) and higher MoCA scores may be related to more avoidance of painful movements in individuals with higher cognition. Subjects with higher cognitive function might be more aware of movements that lead to pain and thus avoid moving at all. The lack of movement “atrophies” cortical inhibition, making individuals with higher cognition feel more pain.
Motor threshold (MT)
The motor threshold presented an inverse association with age, indicating that older the age, lower the MT. One potential interpretation is that as subjects get older and loose capacity of cortical inhibition, they therefore have a lower motor threshold due to inhibitory deficits. These findings reinforce what was found in previous studies in healthy subjects46,47,48 and what we found in our following models using SICI and CSP. In the context of pain, our results convey contrary direction relationships between MT vs. VAS and vs. WOMAC. An inverse relationship is seen between MT and pain reported through the VAS scale, meaning that the more pain reported by a patient on this scale, the lower their motor threshold; thus, confirming the notion of a lower adaptation and thus more pain. This finding relates to other studies in which negative correlations have been found between resting MT and higher pain levels49. Finally for WOMAC the relationship is positive meaning that more pain on this instrument resulted in higher MT. This may also indicate adaptation of subjects trying to move and thus likely adjusting the motor threshold. Noteworthy, we also need to underscore it is known that MT has a high variability inter-subjects50, thus results from this variable need to be interpreted with this caveat.
Quantitative sensory testing (QST) and intracortical excitability
Our models were not able to find a relationship between intracortical excitability and quantitative sensory testing measurements (CPM and pain thresholds). This is one of the most powered studies to analyze this relationship in a multivariate model adjusting for clinical factors that influence both markers, such as age20,51, gender52, emotion53, and cognitive variables54. However, the relationship between the CPM and cortical excitability is not well understood. Some studies have found a relationship between these markers on chronic pain populations55. We hypothesize that the CPM is associated with excitability and inhibition of central pain processing system through multiple independent pathways; therefore, we do not expect always a high correlation with motor cortex excitability in chronic pain.
Limitations
Considering its exploratory nature, our study has some limitations. The lack of a control group in our study prevents us from assuming that the associations found between the cortical excitability measures and sociodemographic and clinical variables indeed pertain to individuals with OA chronic pain. However, since we wanted to understand the factors in OA that drives intracortical excitability (especially inhibitory markers), adding a control group would limit the scope of our associated factors (we could not include disease severity or pain intensity in our statistical models). Moreover, we did not perform corrections for multiple analyses, which could have led to an increase in type two error in our results. Nonetheless, given this is an exploratory study, significant results found in the multivariate analyses still remain valid and compelling for further exploration.
Conclusion
In conclusion, our study could identify clear associations of clinical and demographic variables and cortical excitability in patients with chronic pain caused by knee OA. These associations showed the fundamental role of intracortical inhibition as a marker of adaptation to chronic pain such as that patients with higher intracortical inhibition (likely subjects with more compensation) are younger, have greater cartilage degeneration (indexed by Kellgren-Lawrence severity classification), and have less pain in the WOMAC scale. Also, it is important to note that this variable is not significantly affected by emotional factors and pain measured by VAS. Other markers as MT and CSP corroborate with the primary finding. However, our study has some limitations regarding our methodology and the generalizability of our results. The information revealed here helps us to understand the role of cortex excitability and its changes and characteristics as a biomarker in the pain field. Finally, more research is needed with broader and more general samples to bring more consistency for the role of these biomarkers.
Methods
Subjects
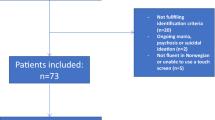
Data were collected from 107 patients with knee osteoarthritis (OA). These patients were obtained from an ongoing, prospective cohort study titled “Deficit of Inhibition as a Marker of Neuroplasticity (DEFINE study) in rehabilitation”56. The DEFINE protocol and this study were approved by the Research and Ethical Comitee of Hospital das Clínicas da Faculdade de Medicina da Universidade de São Paulo (HC FMUSP) (Registration number: 86832518.7.0000.0068). All the proceedings and methods of this study are in accordance with Brazilian research ethics regulations and the Declaration of Helsinki. We included male and female participants, 18 years of age and older that fulfill eligibility criteria for the conventional rehabilitation program of the Instituto de Medicina Fisica e Reabilitacao (IMREA). The diagnosis of osteoarthritis was made through a clinical and radiological (magnetic resonance imaging or computerized tomography; or bilateral knee radiography) diagnosis of knee OA. Individuals with bilateral symptoms who had undergone total knee replacement surgery were included in our sample as they still had unilateral chronic pain related to osteoarthritis (on the other knee) and made up less than 5% (six patients, VAS Pain mean = 4.78, SD = 0.77) of our sample. Individuals with bilateral total knee replacement surgery were excluded. Subjects were excluded if they were pregnant, have active OA with clinical manifestations in joints other than the knee, or if they had any other clinical or social conditions that interfere with the patient’s participation in the rehabilitation program. Characteristics of included knee OA patients are summarized in Table 1.
Study design
This was a cross-sectional study made up of patients with the diagnosis of knee OA from the DEFINE longitudinal cohort study56. Patients admitted to the IMREA’s conventional rehabilitation program with knee OA were invited to participate in the study and included after signing the informed consent form. Patients who agreed to participate in the study underwent a series of neurophysiological and functional assessments before the IMREA rehabilitation program. This program is characterized by an individualized approach, considering the injury’s etiology, the type of disabilities the patient has, general clinical conditions, likely prognosis, and the patient’s socioeconomic factors.
Clinical and functional assessments
Information regarding the participants’ age, gender, time of ongoing pain, height, weight, body mass index, education and cognitive levels were collected for analysis in our regression models with several instruments that allow the global assessment of participants’ pain, motor, cognitive, or emotional function. A summary of all assessments can be seen in the supplementary information file. Some scales, such as cognitive, sleep, and mood scales, were used to characterize the study’s sample, as well as for the management of confounding variables on the multivariate statistical model. Assessments were preferably carried out by the same evaluator. Evaluators were trained to standardized questionnaire applications to reduce assessor bias and variability.
Neurophysiological assessment
The Magstim Rapid® stimulator (The Magstim Company Limited, UK) and a 70 mm coil in figure-of-eight were used, we positioned tangentially to the skull and at an angle of 45 degrees about the sagittal line. The muscular response to the stimulus applied to the motor cortex was recorded using surface electromyography (EMG) with Ag/AgCl electrodes positioned on the target muscle (first dorsal interosseous (FDI) muscle of the hand) and the grounding electrode positioned on the wrist.
Bilateral upper limb assessment was performed. The motor area corresponding to the FDI is the most used motor cortical area in cortical excitability studies due to its greater accuracy57. To locate the cortical area of the hand, it was initially identified from the vertex (intersection between the nasion-inion lines and zygomatic arches). Then, for the identification of the probable hot spot, a mark was made 5 cm from the vertex towards the ear tragus in the coronal plane. The hotspot was determined as the location with the highest and most stable MEP amplitudes over the FDI.
The rMT was defined as the minimum intensity necessary for a single TMS pulse on the hot spot to generate an MEP, with at least 50 μV peak to peak amplitude, in 50% of attempts58. RMT was used as an indirect measure of cortical excitability. In addition, the following measures were used: MEP, in which ten MEP were recorded, with an interval of approximately 7 s between stimuli; cortical silent period (CSP) was measured, which represents the temporary suppression of electromyographic activity during a sustained motor evoked potential voluntary contraction. Finally, we performed paired-pulse protocols of intracortical inhibition (SICI), which was assessed by interstimulus intervals of 2 ms; and intracortical facilitation (ICF) assessed by 10 ms interim stimulus intervals58. For more details on the neurophysiological assessment please see the study protocol published elsewhere56.
For the measurement of neurophysiological markers through TMS, we combined the rMT, CSP, SICI, ICF, and MEP results to obtain a bi-hemispheric average. This approach can be justified due to the bi-hemispheric nature of pain perception59; besides, most of our sample includes patients with bilateral knee OA. We then analyzed the relationship between the bi-hemispheric average of these neuro markers with possible associated variables to their behavior (markers magnitude and direction), including clinical and sociodemographic subject characteristics.
Statistical analysis
Descriptive statistics were used to characterize the study sample, categorical variables were summarized by frequency and percentiles and continuous variables were analyzed by mean and standard deviation (SD). Some of the scales, such as those for mood, pain, cognition, and sleep, were used to characterize the sample, in addition to possibly being used to control confounders in the multivariate model.
We aimed to model the relationship between sociodemographic and clinical variables, as independent variables, and the cortical excitability variables of MT, SICI, ICF, SP, and MEP recorded by TMS, as dependent variables. To select the model covariates, we performed univariate regression analysis for each variable in which variables that reached a p-value < 0.25 were added in the multivariate model. Univariate models were used to not only better select the most significant variables to the final model, but also to minimize the number of tests required to achieve the final model60. Then, to investigate the association between cortex excitability and clinical variables, five separate multivariate linear regression models were created using MT, SICI, ICF, SP, and MEP, as dependent variables, and the significant clinical variables from the univariate analysis. We used a “purposeful selection” method in the process of variable selection to build the models, variables were removed from the models if they were not significant, not a confounder, or not clinical important, thus, we could include in the final models, variables that were not significant in the univariate analysis61. Variables were considered as confounders if they changed the β coefficient of the dependent variable of more than 10%, compared with the previous model. Lastly, to determine the best fit model, the Akaike’s information criteria was used. Models displayed in the results section are the final multivariate models found through this method.
During the modeling process we test linearity assumption visually comparing the scatterplot of each independent variable and a superimposed regression line plot. The homoscedasticity assumption was checked by visual inspection of the scatterplot of the standardized fitted values and standardized residuals62. We defined outliers as values greater than 3 SDs away from the average scores and performed a sensitivity analysis if detected. Finally, we tested the residuals normality using histograms and the Shapiro–Wilk test63 and assumed normality based on the central limit theorem for those with approximate normal distribution. Because this was an exploratory study and to minimize the risk of type II errors, no correction for multiple comparisons was done. We used Stata Statistical Software 15 (Stata Corp LLC) for the statistical analyses.
References
Blyth, F. M., Briggs, A. M., Schneider, C. H., Hoy, D. G. & March, L. M. The global burden of musculoskeletal pain-where to from here?. Am. J. Public Health 109, 35–40. https://doi.org/10.2105/ajph.2018.304747 (2019).
Courtney, C. A., O’Hearn, M. A. & Hornby, T. G. Neuromuscular function in painful knee osteoarthritis. Curr. Pain. Headache Rep. 16, 518–524. https://doi.org/10.1007/s11916-012-0299-2 (2012).
Willett, M. J. et al. The extent of pain is associated with signs of central sensitization in patients with hip osteoarthritis. Pain Pract. 20, 277–288 (2020).
Guler, M. A., Celik, O. F. & Ayhan, F. F. The important role of central sensitization in chronic musculoskeletal pain seen in different rheumatic diseases. Clin. Rheumatol. 39, 269–274 (2020).
Uygur-Kucukseymen, E. et al. Decreased neural inhibitory state in fibromyalgia pain: A cross-sectional study. Neurophysiol. Clin. 50, 279–288 (2020).
Teixeira, P. E. P. et al. Understanding intracortical excitability in phantom limb pain: A multivariate analysis from a multicenter randomized clinical trial. Neurophysiol. Clin. 51, 161–173 (2021).
Arendt-Nielsen, L. et al. Sensitization in patients with painful knee osteoarthritis. Pain 149, 573–581. https://doi.org/10.1016/j.pain.2010.04.003 (2010).
Kleim, J. A. & Jones, T. A. Principles of experience-dependent neural plasticity: Implications for rehabilitation after brain damage. J. Speech Lang. Hear. Res. 51, S225-239. https://doi.org/10.1044/1092-4388(2008/018) (2008).
Candido Santos, L. et al. Intracortical inhibition in the affected hemisphere in limb amputation. Front. Neurol. 11, 720. https://doi.org/10.3389/fneur.2020.00720 (2020).
Hollins, M., Bryen, C. P. & Taylor, D. Effects of chronic pain history on perceptual and cognitive inhibition. Exp. Brain Res. 238, 321–332. https://doi.org/10.1007/s00221-019-05715-8 (2020).
Miller, N. R. et al. Acute and longitudinal changes in motor cortex function following mild traumatic brain injury. Brain Inj. 28, 1270–1276. https://doi.org/10.3109/02699052.2014.915987 (2014).
Demirtas-Tatlidede, A. et al. Long-term effects of contralesional rTMS in severe stroke: Safety, cortical excitability, and relationship with transcallosal motor fibers. NeuroRehabilitation 36, 51–59. https://doi.org/10.3233/nre-141191 (2015).
Baumer, F. M. et al. Cortical excitability, synaptic plasticity, and cognition in benign epilepsy with centrotemporal spikes: A pilot TMS-EMG-EEG study. J. Clin. Neurophysiol. 37, 170–180. https://doi.org/10.1097/wnp.0000000000000662 (2020).
Gilbert, D. L., Isaacs, K. M., Augusta, M., Macneil, L. K. & Mostofsky, S. H. Motor cortex inhibition: A marker of ADHD behavior and motor development in children. Neurology 76, 615–621. https://doi.org/10.1212/WNL.0b013e31820c2ebd (2011).
Kang, J. I., Kim, D. Y., Lee, C. I., Kim, C. H. & Kim, S. J. Changes of motor cortical excitability and response inhibition in patients with obsessive–compulsive disorder. J. Psychiatry Neurosci. 44, 261–268. https://doi.org/10.1503/jpn.180064 (2019).
Ferreri, F. et al. Human brain connectivity during single and paired pulse transcranial magnetic stimulation. Neuroimage 54, 90–102. https://doi.org/10.1016/j.neuroimage.2010.07.056 (2011).
Lefaucheur, J. P. Transcranial magnetic stimulation. Handb. Clin. Neurol. 160, 559–580 (2019).
Parker, R. S., Lewis, G. N., Rice, D. A. & McNair, P. J. Is motor cortical excitability altered in people with chronic pain? A systematic review and meta-analysis. Brain Stimul. 9, 488–500 (2016).
Mall, V. et al. Low level of intracortical inhibition in children shown by transcranial magnetic stimulation. Neuropediatrics 35, 120–125. https://doi.org/10.1055/s-2004-815834 (2004).
Peinemann, A., Lehner, C., Conrad, B. & Siebner, H. R. Age-related decrease in paired-pulse intracortical inhibition in the human primary motor cortex. Neurosci. Lett. 313, 33–36. https://doi.org/10.1016/s0304-3940(01)02239-x (2001).
Tarragó, M. et al. Descending control of nociceptive processing in knee osteoarthritis is associated with intracortical disinhibition: An exploratory study. Medicine 95, e3353. https://doi.org/10.1097/md.0000000000003353 (2016).
Stevens-Lapsley, J. E., Thomas, A. C., Hedgecock, J. B. & Kluger, B. M. Corticospinal and intracortical excitability of the quadriceps in active older and younger healthy adults. Arch. Gerontol. Geriatr. 56, 279–284. https://doi.org/10.1016/j.archger.2012.06.017 (2013).
McGinley, M., Hoffman, R. L., Russ, D. W., Thomas, J. S. & Clark, B. C. Older adults exhibit more intracortical inhibition and less intracortical facilitation than young adults. Exp. Gerontol. 45, 671–678. https://doi.org/10.1016/j.exger.2010.04.005 (2010).
Clark, J., Loftus, A. & Hammond, G. Age-related changes in short-interval intracortical facilitation and dexterity. NeuroReport 22, 499–503. https://doi.org/10.1097/WNR.0b013e3283487480 (2011).
Cantone, M. et al. Age, height, and sex on motor evoked potentials: Translational data from a large Italian cohort in a clinical environment. Front. Hum. Neurosci. 13, 185. https://doi.org/10.3389/fnhum.2019.00185 (2019).
ShaneAnderson, A. & Loeser, R. F. Why is osteoarthritis an age-related disease?. Best Pract. Res. Clin. Rheumatol. 24, 15–26. https://doi.org/10.1016/j.berh.2009.08.006 (2010).
Marcondes, B. F. et al. Pain severity and mobility one year after spinal cord injury: A multicenter, cross-sectional study. Eur. J. Phys. Rehabil. Med. 52, 630–636 (2016).
Cardinal, T. M. et al. Differential neuroplastic changes in fibromyalgia and depression indexed by up-regulation of motor cortex inhibition and disinhibition of the descending pain system: An exploratory study. Front. Hum. Neurosci. 13, 138. https://doi.org/10.3389/fnhum.2019.00138 (2019).
Chang, W. J. et al. Altered primary motor cortex structure, organization, and function in chronic pain: A systematic review and meta-analysis. J. Pain 19, 341–359. https://doi.org/10.1016/j.jpain.2017.10.007 (2018).
Haefeli, M. & Elfering, A. Pain assessment. Eur. Spine J. 15(Suppl 1), S17-24. https://doi.org/10.1007/s00586-005-1044-x (2006).
Von Korff, M., Jensen, M. P. & Karoly, P. Assessing global pain severity by self-report in clinical and health services research. Spine 25, 3140 (2000).
Ziemann, U. et al. TMS and drugs revisited 2014. Clin. Neurophysiol. 126, 1847–1868. https://doi.org/10.1016/j.clinph.2014.08.028 (2015).
Zampelis, V., Ornstein, E., Franzén, H. & Atroshi, I. A simple visual analog scale for pain is as responsive as the WOMAC, the SF-36, and the EQ-5D in measuring outcomes of revision hip arthroplasty. Acta Orthop. 85, 128–132. https://doi.org/10.3109/17453674.2014.887951 (2014).
Gentelle-Bonnassies, S., Le Claire, P., Mezieres, M., Ayral, X. & Dougados, M. Comparison of the responsiveness of symptomatic outcome measures in knee osteoarthritis. Arthritis Care Res. 13, 280–285. https://doi.org/10.1002/1529-0131(200010)13:5%3c280::aid-anr6%3e3.0.co;2-6 (2000).
Pacheco-Barrios, K. et al. Structural and functional motor cortex asymmetry in unilateral lower limb amputation with phantom limb pain. Clin. Neurophysiol. 131, 2375–2382. https://doi.org/10.1016/j.clinph.2020.06.024 (2020).
Uygur-Kucukseymen, E. et al. Decreased neural inhibitory state in fibromyalgia pain: A cross-sectional study. Neurophysiol. Clin. 50, 279–288. https://doi.org/10.1016/j.neucli.2020.06.002 (2020).
Fingleton, C., Smart, K., Moloney, N., Fullen, B. M. & Doody, C. Pain sensitization in people with knee osteoarthritis: A systematic review and meta-analysis. Osteoarthr. Cartil. 23, 1043–1056. https://doi.org/10.1016/j.joca.2015.02.163 (2015).
Veronezi, B. P. et al. Evidence for increased motor cortical facilitation and decreased inhibition in atypical depression. Acta Psychiatr. Scand. 134, 172–182. https://doi.org/10.1111/acps.12565 (2016).
Thibodeau, M. A., Welch, P. G., Katz, J. & Asmundson, G. J. G. Pain-related anxiety influences pain perception differently in men and women: A quantitative sensory test across thermal pain modalities. Pain 154, 419–426. https://doi.org/10.1016/j.pain.2012.12.001 (2013).
Kumar, A., Mattoo, B., Bhatia, R., Kumaran, S. & Bhatia, R. Neuronavigation based 10 sessions of repetitive transcranial magnetic stimulation therapy in chronic migraine: An exploratory study. Neurol. Sci. 42, 131–139. https://doi.org/10.1007/s10072-020-04505-3 (2021).
Passard, A. et al. Effects of unilateral repetitive transcranial magnetic stimulation of the motor cortex on chronic widespread pain in fibromyalgia. Brain 130, 2661–2670. https://doi.org/10.1093/brain/awm189 (2007).
Higgins, D. M., Martin, A. M., Baker, D. G., Vasterling, J. J. & Risbrough, V. The relationship between chronic pain and neurocognitive function: A systematic review. Clin. J. Pain 34, 262–275. https://doi.org/10.1097/ajp.0000000000000536 (2018).
Khedr, E. M., Ahmed, M. A., Darwish, E. S. & Ali, A. M. The relationship between motor cortex excitability and severity of Alzheimer’s disease: A transcranial magnetic stimulation study. Neurophysiol. Clin. 41, 107–113. https://doi.org/10.1016/j.neucli.2011.03.002 (2011).
Werhahn, K. J., Kunesch, E., Noachtar, S., Benecke, R. & Classen, J. Differential effects on motorcortical inhibition induced by blockade of GABA uptake in humans. J. Physiol. 517(Pt 2), 591–597. https://doi.org/10.1111/j.1469-7793.1999.0591t.x (1999).
Mattson, M. P., Pedersen, W. A., Duan, W., Culmsee, C. & Camandola, S. Cellular and molecular mechanisms underlying perturbed energy metabolism and neuronal degeneration in Alzheimer’s and Parkinson’s diseases. Ann. N. Y. Acad. Sci. 893, 154–175. https://doi.org/10.1111/j.1749-6632.1999.tb07824.x (1999).
Mooney, R. A., Cirillo, J. & Byblow, W. D. GABA and primary motor cortex inhibition in young and older adults: A multimodal reliability study. J. Neurophysiol. 118, 425–433. https://doi.org/10.1152/jn.00199.2017 (2017).
Opie, G. M., Ridding, M. C. & Semmler, J. G. Age-related differences in pre- and post-synaptic motor cortex inhibition are task dependent. Brain Stimul. 8, 926–936. https://doi.org/10.1016/j.brs.2015.04.001 (2015).
Smith, A. E., Ridding, M. C., Higgins, R. D., Wittert, G. A. & Pitcher, J. B. Age-related changes in short-latency motor cortex inhibition. Exp. Brain Res. 198, 489–500. https://doi.org/10.1007/s00221-009-1945-8 (2009).
Kittelson, A. J., Thomas, A. C., Kluger, B. M. & Stevens-Lapsley, J. E. Corticospinal and intracortical excitability of the quadriceps in patients with knee osteoarthritis. Exp. Brain Res. 232, 3991–3999. https://doi.org/10.1007/s00221-014-4079-6 (2014).
Cicinelli, P., Traversa, R., Bassi, A., Scivoletto, G. & Rossini, P. M. Interhemispheric differences of hand muscle representation in human motor cortex. Muscle Nerve 20, 535–542. https://doi.org/10.1002/(sici)1097-4598(199705)20:5%3c535::aid-mus1%3e3.0.co;2-a (1997).
Hackett, J., Naugle, K. E. & Naugle, K. M. The decline of endogenous pain modulation with aging: A meta-analysis of temporal summation and conditioned pain modulation. J. Pain 21, 514–528 (2020).
Martel, M. O., Wasan, A. D. & Edwards, R. R. Sex differences in the stability of conditioned pain modulation (CPM) among patients with chronic pain. Pain Med. 14, 1757–1768 (2013).
Nahman-Averbuch, H., Nir, R.-R., Sprecher, E. & Yarnitsky, D. Psychological factors and conditioned pain modulation. Clin. J. Pain 32, 541–554 (2016).
Zadey, S. et al. Higher motor cortical excitability linked to greater cognitive dysfunction in Alzheimer’s disease: results from two independent cohorts. Neurobiol. Aging 108, 24–28 (2021).
Botelho, L. M. et al. A framework for understanding the relationship between descending pain modulation, motor corticospinal, and neuroplasticity regulation systems in chronic myofascial pain. Front. Hum. Neurosci. 10, 308 (2016).
Simis, M. et al. Deficit of inhibition as a marker of neuroplasticity (DEFINE study) in rehabilitation: A longitudinal cohort study protocol. Front. Neurol. 12, 1193 (2021).
Malcolm, M. P. et al. Reliability of motor cortex transcranial magnetic stimulation in four muscle representations. Clin. Neurophysiol. 117, 1037–1046 (2006).
Rossini, P. M. et al. Non-invasive electrical and magnetic stimulation of the brain, spinal cord, roots and peripheral nerves: Basic principles and procedures for routine clinical and research application: An updated report from an IFCN Committee. Clin. Neurophysiol. 126, 1071–1107 (2015).
Schwenkreis, P. et al. Bilateral motor cortex disinhibition in complex regional pain syndrome (CRPS) type I of the hand. Neurology 61, 515–519. https://doi.org/10.1212/wnl.61.4.515 (2003).
Ziliak, S. P values and the search for significance. Nat. Methods 14, 3–4 (2017).
Bursac, Z., Gauss, C. H., Williams, D. K. & Hosmer, D. W. Purposeful Selection of Variables in Logistic Regression Source Code for Biology and Medicine (Springer, 2008).
Osborne, J. W. & Waters, E. Four assumptions of multiple regression that researchers should always test. Pract. Assess. Res. Eval. 8, 2 (2002).
Yap, B. W. & Sim, C. H. Comparisons of various types of normality tests. J. Stat. Comput. Simul. 81, 2141–2155 (2011).
Funding
This study is supported by a grant from FAPESP (SPEC Project, Fund Number 2017/12943-8).
Author information
Authors and Affiliations
Contributions
All authors designed the study. M.S. and M.I. collected the data. F.F., A.M., P.S.M., and K.P.-B. performed statistical analyses. F.F., A.M., P.S.M., and K.P.-B. interpreted the data. Further, A.M. and P.S.M. completed the first draft of the article. All authors participated in the interpretation of the results, the writing of the manuscript, and approved of its final version.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Simis, M., Imamura, M., de Melo, P.S. et al. Increased motor cortex inhibition as a marker of compensation to chronic pain in knee osteoarthritis. Sci Rep 11, 24011 (2021). https://doi.org/10.1038/s41598-021-03281-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-021-03281-0
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
