
Abstract
Potassium voltage-gated channel subfamily Q member 1 (KCNQ1) is one of the strongest susceptibility genes for type 2 diabetes mellitus (T2DM). Association studies between KCNQ1 genetic variants and T2DM have been reported. The multifactorial disease T2DM is caused by interactions between genetic susceptibility and environmental factors. In this study, we examined the associations between the KCNQ1 haplotype, which consists of the major alleles rs3852528, rs11024175, and rs2237892 (ht: ACC), and environmental factors such as alcohol consumption, which are related to the risk of T2DM, in two independent Korean populations. Data from health examination studies, i.e., HEXA (n = 50,357 subjects) and the Ansung–Ansan community-based Korean cohort study (n = 7603), were analyzed. In both cohorts, fasting blood glucose levels were significantly increased in moderate-to-heavy drinkers and carriers of the homozygous ACC haplotype. A significant association between the KCNQ1 haplotype and alcohol consumption in the risk of diabetes was observed in the HEXA (OR 1.587; 95% CI 1.128–2.234) and Ansung–Ansan (OR 2.165; 95% CI 1.175–3.989) cohorts compared with abstainers not carrying the KCNQ1 haplotype. Associations of the KCNQ1 haplotype with alcohol consumption and β-cell function were observed in the Ansung–Ansan cohort. Moderate-to-heavy drinkers with the ACC haplotype had lower fasting insulin levels and mean 60 min insulinogenic index (IGI60) compared with light drinkers and abstainers not carrying the ACC haplotype. These findings indicate that KCNQ1 variants play a synergistic role with alcohol consumption in the development of T2DM and impaired β-cell function.
Similar content being viewed by others

Introduction
Type 2 diabetes mellitus (T2DM) is a worldwide chronic metabolic disease that occurs when pancreatic β-cell function is impaired and insulin cannot be produced, leading to hyperglycemia1,2. T2DM is a multifactorial disease influenced by a combination of genetic and environmental factors.
One such environmental factor is alcohol consumption, which induces many problems in practical every aspect of human life. In particular, chronic alcohol consumption increases the risk of T2DM, leading to disruptions in glucose homeostasis and pancreatic β-cell function, including impaired insulin secretion and β-cell apoptosis3,4. Although the effects of alcohol consumption on the risk of T2DM have been reported by many studies, additional studies investigating the interplay between genetic variants and environmental factors leading to the onset of diabetes are needed.
Various susceptibility genes for T2DM have been identified by meta-analyses of genome-wide association studies (GWAS). Among these genes, the variants of voltage-gated potassium channel subfamily Q member 1 (KCNQ1), a novel diabetes susceptibility gene, have been implicated in diabetes in many studies in various ethnic groups5,6,7. KCNQ1 encodes the pore-forming alpha subunit composed of the KvLQT1 (or Kv7.1) voltage-gated potassium channel and potassium voltage-gated channel subfamily E members (KCNEs)8,9. The KvLQT1 channel is essential for controlling the cellular repolarization process, including regulation of insulin secretion after electrical depolarization of pancreatic β-cells. Numerous KCNQ1 variants are correlated with the prevalence of T2DM and the insulin response, along with increased fasting glucose levels resulting from impaired insulin secretion10. Despite that various KCNQ1 single nucleotide polymorphisms (SNPs) are associated with susceptibility to T2DM, there are limited data on the association between the KCNQ1 haplotype and T2DM. Furthermore, few studies have evaluated the interactions between genetic susceptibility and environmental risk factors in terms of T2DM risk. Here, we evaluated the multifactorial interplay between alcohol consumption and KCNQ1 variants on the risk of developing T2DM in two independent Korean cohort studies: the HEXA (Health Examinees study) and Ansung–Ansan community-based Korean cohort study.
Results
General characteristics of the study population
The number of subjects with KCNQ1 variants was similarly distributed between the two cohorts (Supplementary Table S1). The baseline characteristics of the subjects according to the KCNQ1 haplotype, comprising the major alleles of three SNPs (ht: ACC/ACC), are shown in Table 1. Blood pressure and the levels of triglycerides, cholesterol (HDL and total), and the liver enzymes alanine aminotransferase and aspartate aminotransferase did not differ according to the KCNQ1 haplotype in either cohort. The mean 60 min insulinogenic index (IGI60) values were 13.7 ± 29.6 in non-carriers, 12.4 ± 26.7 in ACC/– carriers, and 11.5 ± 19.3 in ACC/ACC carriers, indicating that subjects carrying the homozygous ACC haplotype (ACC/ACC carriers) tended to have decreased β-cell function in the Ansung–Ansan cohort (p < 0.0651). The fasting blood glucose level and prevalence rate of T2DM were significantly higher in subjects with the KCNQ1 homozygous ACC haplotype than in non-carriers in both cohorts.
The baseline characteristics of the subjects according to their alcohol consumption status (27,024 abstainers and 23,333 drinkers in the HEXA cohort and 3826 abstainers and 3777 drinkers in the Ansung–Ansan cohort) are described in Supplementary Table S2. All drinkers had higher levels of alcoholic markers, including diastolic blood pressure, fasting glucose, HDL-cholesterol, triglycerides, aspartate aminotransferase, and alanine aminotransferase, compared with abstainers. Systolic blood pressure and the total cholesterol level differed significantly according to alcohol consumption only in the HEXA cohort (p < 0.001). The IGI60 value and fasting insulin level were lower in drinkers in the Ansung–Ansan cohort. The T2DM prevalence was not affected by alcohol consumption in either cohort; the prevalence rates of T2DM were 9.9% for abstainers and 10.1% for drinkers in the HEXA cohort and 11.8% for abstainers and 12.5% for drinkers in the Ansung–Ansan cohort.
Effect of the association between the KCNQ1 haplotype and alcohol consumption on fasting blood glucose
The fasting glucose levels were increased in subjects carrying the KCNQ1 haplotype compared with non-carriers, regardless of alcohol consumption, in the two cohort populations (Table 1). In addition, the fasting glucose levels were significantly higher in alcohol drinkers (Supplementary Table S2). We assessed the synergistic effect between alcohol consumption and the KCNQ1 haplotype on the fasting glucose level (Table 2). In both cohorts, moderate-to-heavy drinkers and subjects carrying the ACC haplotype had higher fasting glucose levels than abstainers not carrying the ACC haplotype, and light alcohol consumption has shown increased fasting glucose levels regardless of ACC haplotype. Moderate-to-heavy drinkers with the carrying ACC haplotype had significantly high fasting glucose levels compared with abstainers carrying ACC haplotype.
The effects of the KCNQ1 haplotype and alcohol consumption on T2DM risk
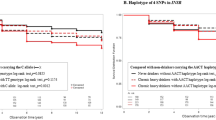
Multivariate logistic regression analysis was performed to assess the association between the KCNQ1 haplotype and alcohol consumption in the risk of T2DM (Table 3). In the HEXA cohort, light drinkers carrying the ACC haplotype exhibited a higher risk of developing T2DM (odds ratio [OR] 1.530; 95% confidence interval [CI] 1.008–2.323) and the T2DM risk was significantly increased in moderate-to-heavy drinkers carrying ACC haplotype (OR 1.587; 95% CI 1.128–2.234) compared with abstainers not carrying the KCNQ1 ACC haplotype, whereas the T2DM risk was not higher in abstainers carrying the ACC haplotype (OR 1.334; 95% CI 0.888–2.003) compared with non-carriers. Also, ACC haplotype heterozygotes and light drinking had risky effects on T2DM in HEXA population. In Ansung–Ansan, subjects carrying the homozygous ACC haplotype showed an increased risk of T2DM (OR 2.588 in abstainers; 95% CI 1.498–4.469; OR 2.165; 95% CI 1.175–3.989 in moderate-to-heavy drinkers). In both cohorts, the risk of T2DM was increased in moderate-to-heavy drinkers who were homozygous for the ACC haplotype compared with abstainers not carrying the ACC haplotype. As shown in Supplementary Table S3, the risk of T2DM showed a similar pattern between subjects carrying the major KCNQ1 SNP alleles and carrying the ACC haplotype. Based on the KCNQ1 genetic factor, which had a more significant effect on the risk of T2DM than environmental factors, subjects with the major alleles of each 3 SNPs and the ACC haplotype had a higher T2DM risk compared with those who did not have the major alleles or the haplotype. These results indicate a significant increase in T2DM risk by the KCNQ1 haplotype and alcohol consumption in HEXA, but the ACC haplotype was a little more influential factor in the Ansung–Ansan cohort.
Effect of the association between the KCNQ1 haplotype and alcohol consumption on β-cell function
As shown in Table 4, the fasting insulin levels decreased consistently with the result of fasting glucose levels by carrying the ACC haplotype and alcohol consumption in Ansung–Ansan cohort. We determined the insulin index on the subjects, excepted patients with T2DM, related to the fasting glucose level, fasting insulin level, IGI60, homeostatic model assessment for insulin resistance, and the insulin sensitivity according to the KCNQ1 haplotype and alcohol consumption to understand the effect on increased fasting glucose levels. Alcohol drinking showed significantly lower fasting insulin levels according to alcohol exposure amount than abstainers. Also, subjects carrying ACC haplotype showed decreased tendency of fasting insulin levels. We detected the association effects between alcohol consumption and carrying KCNQ1 haplotype on the reduction of fasting insulin levels. The IGI60 value tended to be lower in those carrying the ACC haplotype than in non-carriers. Also, drinkers showed a lower the IGI60 value than abstainers regardless of alcohol consumption amount. The IGI60 value was increased in light drinkers compared to moderate-to-heavy drinkers and abstainer carrying ACC haplotype, but not significant. Additionally, many studies have reported an importance of insulin sensitivity than insulin secretion, but there were no significant differences in the homeostatic model assessment for insulin resistance or insulin sensitivity index in the present study (Supplementary Table S4). Previous studies have consistently reported that alcohol consumption contributes to impaired insulin secretion, as found in the present study (Supplementary Table S2). Our results suggest that the interplay between the KCNQ1 ACC haplotype and alcohol consumption increases the risk of T2DM resulting from pancreatic β-cell dysfunction, rather than a change in insulin resistance and/or insulin sensitivity.
Discussion
In the present study, we found an effect of the association between alcohol consumption and KCNQ1 variants on the development of T2DM in two independent cohorts. Drinkers carrying the ACC haplotype showed an increased risk of T2DM and higher fasting glucose levels due to impaired insulin secretion compared with abstainers not carrying the ACC haplotype.
A GWAS conducted by an independent study group identified several SNPs associated with susceptibility to T2DM5,7,11. Notably, KCNQ1 SNPs were correlated with the incidence of T2DM in two independent GWAS of Japanese populations. Furthermore, various SNPs in KCNQ1 have been associated with T2DM susceptibility regardless of ethnicity. KCNQ1 rs2237892, which alters pancreatic β-cell function, is the most well-known susceptibility SNP for T2DM and gestational diabetes mellitus in the Asian population12. The high-risk SNPs rs151290, rs2237892, and rs2237895 have been associated with T2DM due to impaired glucose-stimulated insulin secretion and higher LDL and total cholesterol levels10. The major KCNQ1 SNPs (rs2237897, rs2237892, and rs2283228) showed significant associations with a higher fasting glucose level and reduced insulin response7. Homozygosity for the CC risk allele of rs2237892 was associated with a significantly lower homeostatic model assessment of β-cell function (HOMA-β) and corrected insulin response compared with the other two genotypes. Similar to our findings, individuals with the KCNQ1 variant were susceptible to diabetes in two independent cohorts.
We found that subjects carrying the ACC haplotype had the major alleles rs3852528, rs2237892, and rs1102417, which are independently associated with the risk of developing T2DM. Riyadh et al. reported that the KCNQ1 haplotype consists of the minor alleles rs2237892, rs2283228, and rs2237895, which have a protective effect on T2DM via a homozygous TCA haplotype (TCA-TCA diplotype). KCNQ1 exhibits improved β-cell function, as reflected by a higher HOMA-β value, compared with the other diplotypes6. Consistent with our genetic analysis, carrying the homozygous ACC haplotype results in a higher T2DM prevalence and lower IGI60 value.
Carrying the KCNQ1 haplotype and alcohol consumption increase the effect of the fasting glucose level on β -cell dysfunction, leading to an increased risk of T2DM. Several studies have reported that chronic heavy alcohol consumption impairs β-cell function, leading to a higher risk of T2DM13,14. Although the effect of alcohol intake according to exposure amount and period on the development of T2DM is still controversial, such as J- and linear-curve, alcohol consumption is thought to be a major determinant of T2DM development15,16. In this study, we detected the effects of alcohol consumption on the regulation of the fasting glucose level and insulin secretion. Alcohol intake tended to have linear relation to the increase of fasting glucose by KCNQ1 haplotype carrying in HEXA study, but not in Ansung–Ansan study (Table 2). Also, Moderate-to-heavy drinkers having KCNQ1 haplotype homozygotes showed higher association with T2DM risk in both HEXA and Ansung–Ansan cohorts (Table 3). Moreover, KCNQ1 haplotype carriers had a tendency to lower fasting insulin and IGI60 level according to the higher intake of alcohol in Ansung–Ansan study (Table 4). Therefore, the combination of alcohol consumption and carrying KCNQ1 variants increased the risk of developing T2DM and gradually increased fasting glucose levels with β-cell dysfunction.
KCNQ1 combined with KCNE1 is responsible for positioning the KvLQT1 channel in pancreatic β-cells. The KvLQT1 channel is activated by electrical depolarization resulting from closure of the KATP channel, and it induces subsequent repolarization, leading to termination of insulin secretion via an outwardly opening K+ channel, to regulate ion homeostasis8,17,18. A specific deficiency of KCNQ1 in pancreatic β-cells and loss of function of the KvLQT1 channel are associated with prolonged insulin secretion via inhibition of action potential repolarization19. Rapid repolarization, including KvLQT1 gain of function, interrupts insulin secretion, and blocking the KCNQ1 subunit promotes insulin secretion by inhibiting after-repolarization of action potentials in pancreatic β-cells. Although these variants have not been reported to induce a functional effect on the KvLQT1 channel20, the KCNQ1 polymorphisms rs3852528, rs11024175, and rs2237892, which are located in intron 15 of the KCNQ1 gene on chromosome 11p15, have been reported as susceptible variants to T2DM. The haplotype analyses including these each single variants may reflect more effectively genetic heritability of KCNQ1 on T2DM than those of individual risky variants. Furthermore, many studies have reported correlations of T2DM with impaired β-cell function and the KCNQ1 variant located in the intron. Even if a mutation in that intron did not affect the KvLQT1 channel, several cases affect the functional consequences that the novel mutation in the third base of intron 7 (c.1003G > A) is a splicing-related mutation within the pore domain S6 region of the KvLQT1 channel21. In addition, KCNQ1 variants located in intron 15, such as rs2274196 and rs163184, may induce subsequent changes in gene expression and binding activity. The SNP rs163184 locus is contiguous to rs2237892 and rs2237895, which moderates linkage disequilibrium. The SNP rs163184 locus is contiguous to rs2237892 and rs2237895, which are in moderate linkage disequilibrium with each other22. Overall, these findings suggest that the KCNQ1 variants associated with the ACC haplotype affect the expression of other target genes and/or the transcription of the nearby imprinting region, encompassing CDKN1C, PHLDA2, and Slc22a18, which are related to β-cell proliferation23,24,25,26. Based on our results, further studies are required to validate the correlation and to investigate the effects of KCNQ1 variants within introns that potentially regulate β-cell proliferation or a functional modification of the KvLQT1 channel.
Materials and methods
Study population
Data were obtained from two cohort studies conducted by the Korea National Institutes of Health as part of the Korean Genome and Epidemiology study27. Written informed consent was obtained from all subjects, and this research project was approved by the National Biobank of Korea and the Centers for Disease Control and Prevention, Republic of Korea. This study protocol was approved by the Korean National Institutes of Health Institutional Review Board (2019-03-01-PE-A). All study protocols were carried out in accordance with approved guidelines.
Participants of the HEXA were enrolled from 38 health examination centers and hospitals located in eight regions (metropolitan areas or major cities) of Korea between 2004 and 2013. We used baseline data from HEXA (n = 53,754). Subjects with missing data on alcohol consumption (n = 2924) or the KCNQ1 haplotype (n = 473) were excluded. A total of 50,357 subjects were included in this study. The community-based Ansung–Ansan cohort study has been described in detail previously28. We used data from 8840 subjects living in rural Ansung or urban Ansan. Individuals with missing data on alcohol consumption (n = 828) or type 2 diabetes (n = 409) were excluded, leaving 7603 subjects who were included in this study.
Anthropometric and biochemical analyses
Information on age, family history of diabetes, physical activity, and smoking (pack-years) was obtained using interview-based questionnaires. Body mass index (BMI) was calculated as weight in kilograms divided by height in meters squared. Fasting glucose levels and the lipid profile (total cholesterol, triglycerides, and HDL-cholesterol) were measured using the Hitachi 747 chemistry analyzer (Hitachi Ltd., Tokyo, Japan) following the manufacturer’s recommendations. Insulin levels were measured using the INS-IRMA kit (Biosource, Nivelles, Belgium) and a gamma counter (Packard Instrument Co., Meriden, CT, USA) in the Ansan–Ansung cohort, whereas insulin levels were not measured in the HEXA cohort.
Genotyping
All genotype data were approved and provided by the National Biobank of Korea and the Centers for Disease Control and Prevention, the Republic of Korea (no. 2019-022). Genotyping in the Ansung–Ansan cohort study was performed using the Affymetrix genome-wide human SNP array 5.0, and genotype imputation was performed using IMPUTE2; the 1000 genome projects of the East Asian ancestry sample was used as a reference panel. Genotyping in the HEXA study was performed using the Korean Chip designed by the Center for Genome Science at the Korean National Institutes of Health. The expected genotyping and quality-control information has been described previously in detail29,30.
T2DM and pancreatic β-cell function
T2DM was defined as a fasting glucose level > 126 mg/dL. In addition, subjects who reported currently taking antidiabetic medication and insulin were considered to have T2DM. The subjects were followed until they developed T2DM or the last examination. In the Ansung–Ansan cohort, pancreatic β-cell function was estimated using the oral glucose tolerance test (75 g). The mean 60 min insulinogenic index (IGI60) was calculated as follows: (insulin level [µU/mL]) at 60 min–insulin level at 0 min) ÷ (glucose level [mmol/L] at 60 min–glucose level at 0 min)13.
Measurement of alcohol consumption
Information on alcohol consumption was collected from the two cohorts using an interview-based questionnaire. Subjects were asked whether they had ever consumed at least one alcoholic drink per month; if yes, they were then asked whether they were former or current drinkers. We excluded former drinkers because the drinking period was unclear. Because females were not in the heavy drinking group, we classified the subjects into three groups (abstainers, light, and moderate-to-heavy drinkers) using the baseline alcohol consumption information.
Statistical analysis
Statistical analyses were performed using the SAS software package (ver. 9.4; SAS Institute, Cary, NC, USA). Data are presented as means ± standard deviation, numbers (%), or odds ratios (ORs) with 95% confidence intervals (CIs). Logarithmic transformation was applied to variables with a non-Gaussian distribution. Student’s t-test and One-way ANOVA analysis was conducted to compare the clinical characteristics according to drinking status. The chi-square test was used to compare categorical variables (drinking status and the KCNQ1 haplotype). Multivariate logistic regression analyses were performed to detect the association between T2DM and the KCNQ1 haplotype according to alcohol consumption in the HEXA and Ansan–Ansung cohorts after adjusting for age, sex, smoking, BMI, family history of diabetes, physical activity, and income. All reported p-values are two-tailed, and a p-value < 0.05 was considered significant.
Conclusion
In summary, we determined the characteristics of the KCNQ1 ACC haplotype and the synergistic effect between the KCNQ1 haplotype and alcohol consumption on the increased fasting glucose level and the risk of T2DM along with β-cell dysfunction. This is the first study to examine the effect of the association between KCNQ1 and alcohol consumption on the risk of developing T2DM. However, our study also had some limitations. First, the mechanism of how the KCNQ1 intronic variants interact with alcohol consumption and T2DM remains unclear. Second, we used IGI60 as the index of insulin secretion because 30 min glucose and insulin values were not available. But, the insulinogenic index at 60 min correlates well with IGI30 and can be used as a surrogate of early insulin secretion31. Furthermore, the present study has several strengths, such as the use of a large-scale sample size and replicated results using clinical indicators (glucose and insulin) to identify T2DM in two independent cohorts. These findings potentially suggest that the interaction between the KCNQ1 variants and alcohol consumption contributes to the pathogenesis of T2DM via pancreatic β-cell dysfunction.
References
Ackermann, A. M. & Gannon, M. Molecular regulation of pancreatic beta-cell mass development, maintenance, and expansion. J. Mol. Endocrinol. 38, 193–206. https://doi.org/10.1677/jme-06-0053 (2007).
Cnop, M. et al. Mechanisms of pancreatic beta-cell death in type 1 and type 2 diabetes: Many differences, few similarities. Diabetes 54(Suppl 2), S97–S107. https://doi.org/10.2337/diabetes.54.suppl_2.s97 (2005).
Kim, J. Y. et al. Chronic alcohol consumption potentiates the development of diabetes through pancreatic β-cell dysfunction. World J. Biol. Chem. 6, 1–15. https://doi.org/10.4331/wjbc.v6.i1.1 (2015).
Dembele, K., Nguyen, K. H., Hernandez, T. A. & Nyomba, B. L. Effects of ethanol on pancreatic beta-cell death: Interaction with glucose and fatty acids. Cell Biol. Toxicol. 25, 141–152. https://doi.org/10.1007/s10565-008-9067-9 (2009).
Unoki, H. et al. SNPs in KCNQ1 are associated with susceptibility to type 2 diabetes in East Asian and European populations. Nat. Genet. 40, 1098–1102. https://doi.org/10.1038/ng.208 (2008).
Saif-Ali, R. et al. KCNQ1 haplotypes associate with type 2 diabetes in Malaysian Chinese subjects. Int. J. Mol. Sci. 12, 5705–5718. https://doi.org/10.3390/ijms12095705 (2011).
Tan, J. T. et al. Genetic variation in KCNQ1 associates with fasting glucose and beta-cell function: A study of 3,734 subjects comprising three ethnicities living in Singapore. Diabetes 58, 1445–1449. https://doi.org/10.2337/db08-1138 (2009).
Smith, J. A., Vanoye, C. G., George, A. L. Jr., Meiler, J. & Sanders, C. R. Structural models for the KCNQ1 voltage-gated potassium channel. Biochemistry 46, 14141–14152. https://doi.org/10.1021/bi701597s (2007).
Vanoye, C. G. et al. Distinct subdomains of the KCNQ1 S6 segment determine channel modulation by different KCNE subunits. J. Gen. Physiol. 134, 207–217. https://doi.org/10.1085/jgp.200910234 (2009).
van Vliet-Ostaptchouk, J. V. et al. Common variants in the type 2 diabetes KCNQ1 gene are associated with impairments in insulin secretion during hyperglycaemic glucose clamp. PLoS ONE 7, e32148. https://doi.org/10.1371/journal.pone.0032148 (2012).
Tan, J. T. et al. Polymorphisms identified through genome-wide association studies and their associations with type 2 diabetes in Chinese, Malays, and Asian-Indians in Singapore. J. Clin. Endocrinol. Metab. 95, 390–397. https://doi.org/10.1210/jc.2009-0688 (2010).
Ao, D. et al. The rs2237892 Polymorphism in KCNQ1 influences gestational diabetes mellitus and glucose levels: A case-control study and meta-analysis. PLoS ONE 10, e0128901. https://doi.org/10.1371/journal.pone.0128901 (2015).
Lee, D. Y. et al. Association between alcohol consumption pattern and the incidence risk of type 2 diabetes in Korean men: A 12-years follow-up study. Sci. Rep. 7, 7322. https://doi.org/10.1038/s41598-017-07549-2 (2017).
Jang, H. B., Go, M. J., Park, S. I., Lee, H. J. & Cho, S. B. Chronic heavy alcohol consumption influences the association between genetic variants of GCK or INSR and the development of diabetes in men: A 12-year follow-up study. Sci. Rep. 9, 20029. https://doi.org/10.1038/s41598-019-56011-y (2019).
Baliunas, D. O. et al. Alcohol as a risk factor for type 2 diabetes: A systematic review and meta-analysis. Diabetes Care 32, 2123–2132. https://doi.org/10.2337/dc09-0227 (2009).
Li, X. H., Yu, F. F., Zhou, Y. H. & He, J. Association between alcohol consumption and the risk of incident type 2 diabetes: A systematic review and dose-response meta-analysis. Am. J. Clin. Nutr. 103, 818–829. https://doi.org/10.3945/ajcn.115.114389 (2016).
Ullrich, S. et al. Effects of I(Ks) channel inhibitors in insulin-secreting INS-1 cells. Pflugers Arch. 451, 428–436. https://doi.org/10.1007/s00424-005-1479-2 (2005).
Liu, L., Wang, F., Lu, H., Ren, X. & Zou, J. Chromanol 293B, an inhibitor of KCNQ1 channels, enhances glucose-stimulated insulin secretion and increases glucagon-like peptide-1 level in mice. Islets 6, e962386. https://doi.org/10.4161/19382014.2014.962386 (2014).
Barro-Soria, R. et al. KCNE1 and KCNE3 modulate KCNQ1 channels by affecting different gating transitions. Proc. Natl. Acad. Sci. U.S.A. 114, E7367–E7376. https://doi.org/10.1073/pnas.1710335114 (2017).
Wang, X. et al. Pleiotropic effects of a KCNQ1 variant on lipid profiles and type 2 diabetes: A family-based study in China. J. Diabetes Res. 2020, 8278574. https://doi.org/10.1155/2020/8278574 (2020).
Tsuji-Wakisaka, K. et al. Identification and functional characterization of KCNQ1 mutations around the exon 7-intron 7 junction affecting the splicing process. Biochim. Biophys. Acta 1452–1459, 2011. https://doi.org/10.1016/j.bbadis.2011.07.011 (1812).
Hiramoto, M. et al. A type 2 diabetes-associated SNP in KCNQ1 (rs163184) modulates the binding activity of the locus for Sp3 and Lsd1/Kdm1a, potentially affecting CDKN1C expression. Int. J. Mol. Med. 41, 717–728. https://doi.org/10.3892/ijmm.2017.3273 (2018).
Ou, K. et al. Targeted demethylation at the CDKN1C/p57 locus induces human β cell replication. J. Clin. Investig. 129, 209–214. https://doi.org/10.1172/jci99170 (2019).
Kanduri, C. Kcnq1ot1: A chromatin regulatory RNA. Semin. Cell Dev. Biol. 22, 343–350. https://doi.org/10.1016/j.semcdb.2011.02.020 (2011).
Asahara, S. et al. Paternal allelic mutation at the Kcnq1 locus reduces pancreatic β-cell mass by epigenetic modification of Cdkn1c. Proc. Natl. Acad. Sci. U.S.A. 112, 8332–8337. https://doi.org/10.1073/pnas.1422104112 (2015).
Yu, X. X. & Liao, M. Q. Associations of KCNQ1 polymorphisms with the risk of type 2 diabetes mellitus: An updated meta-analysis with trial sequential analysis. J diabetes Res. 2020, 7145139. https://doi.org/10.1155/2020/7145139 (2020).
Kim, Y. & Han, B. G. Cohort profile: The Korean Genome and Epidemiology Study (KoGES) Consortium. Int. J. Epidemiol. 46, e20. https://doi.org/10.1093/ije/dyv316 (2017).
Yoo, M. G., Kim, H. J., Jang, H. B., Lee, H. J. & Park, S. I. The association between alcohol consumption and β-cell function and insulin sensitivity in Korean population. Int. J. Environ. Res. Public Health 13, 1133. https://doi.org/10.3390/ijerph13111133 (2016).
Moon, S. et al. The Korea Biobank array: Design and identification of coding variants associated with blood biochemical traits. Sci. Rep. 9, 1382. https://doi.org/10.1038/s41598-018-37832-9 (2019).
Cho, Y. S. et al. A large-scale genome-wide association study of Asian populations uncovers genetic factors influencing eight quantitative traits. Nat. Genet. 41, 527–534. https://doi.org/10.1038/ng.357 (2009).
Matthews, D. R. et al. Homeostasis model assessment: Insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 28, 412–419. https://doi.org/10.1007/bf00280883 (1985).
Acknowledgements
Data used in the study were obtained from the Korean Genome Analysis Project (4845-301), the Korean Genome and Epidemiology Study (4851-302), and the Korean Biobank Project (4851-307, KBP-2019-022) supported by the Korean Center for Disease Control and Prevention.
Funding
This study was supported by the Korea National Institutes of Health (2017-NI64001, 2019-NI-088-01).
Author information
Authors and Affiliations
Contributions
H.-J.L. and S.I.P. were responsible for the data integrity and accuracy of the data analyses. H.-J.L. conceived and designed the study. M.-G.Y. performed the statistical analyses, and M.-G.Y., J.Y.P. and H.-J.L. interpreted the data. J.Y.P. and M.-G.Y. wrote the initial draft of the manuscript, and J.H.Y., H.-J.L. and S.I.P. reviewed/edited the manuscript. All authors approved the final version.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Park, J.Y., Yoo, MG., Yun, J.H. et al. Synergistic effect between the KCNQ1 haplotype and alcohol consumption on the development of type 2 diabetes mellitus in Korean cohorts. Sci Rep 11, 21796 (2021). https://doi.org/10.1038/s41598-021-01399-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-021-01399-9
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
