
Abstract
A femoral neck fracture is currently one of the most common types of fracture in clinical practice. The incidence continues to increase due to traffic accidents, trauma, and osteoporosis. This research includes a biomechanical study and a clinical retrospective study. In the biomechanical studies, three groups’ effects (Control Group: 3CCS, DHS group, and study Group: 3CCS + mFNSS group) were compared by vertical compression tests, torsion tests, and fatigue tests. All the data were collected and analyzed. We subsequently performed a retrospective analysis of 131 patients with femoral neck fractures. The operative time, intraoperative blood loss, quality of postoperative fracture reduction, and follow-up observation of fracture healing, screw retreatment rates and fixation failure rates, as well as femoral head necrosis rates and hip function in two groups with 3CCS and 3CCS + mFNSS were compared. By the biomechanical study, we found that 3CCS + Mfnss group were biomechanically superior to 3CCS group and superior to the DHS group in terms of resistance to torsion. However, it was less effective than the DHS group in compressive strength and fatigue resistance. In terms of clinical application, 3CCS + mFNSS group was found to have lower screw retreatment rates and femoral head necrosis rates, and to have better fracture healing rates than group with 3CCS, indicating that medial support screws can effectively resist the vertical shear forces of fracture ends and promote the stability and healing of fracture ends, as well as to reduce the incidence of postoperative complications.
Similar content being viewed by others


Introduction
A femoral neck fracture is currently one of the most common types of fractures in clinical practice, occurring in approximately 3.6% of total body fractures and 57% of hip fractures1. Due to car accidents, trauma and other causes, the incidence of femoral neck fractures continues to increase, and the age of onset is no longer limited to the elderly, especially high-energy trauma can also cause femoral neck fractures among young adults. Regarding the classification of femoral neck fractures, Pauwels classification is one of the most commonly used classification methods for femoral neck fractures in clinical practice. Although this classification does not fully take into account situations such as fracture end displacement, from the biomechanical view of fracture healing, Pauwels classification has its advantages2,3. Pauwels type III means the Pauwels angle is more than 50\°4,5,6. Because the broken ends of the fracture are subjected to high vertical shear forces and are prone to hip varus, collapse, and displacement of the proximal femur bone, nonunion and disruption of the femoral head blood supply occur at both ends of the fracture, and avascular necrosis occurs2,7. Also, fracture injury involves vertical shear force, and the shear load is higher, which makes a higher clinical failure rate of internal fixation7. At present, perioperative management of patients with femoral neck fracture has attracted more and more attention. In particular, the concept of rapid rehabilitation has become increasingly demanding for surgeons and nursing teams. For the preoperative management of patients with femoral neck fracture, we cannot simply apply skin traction or bone traction to maintain the force line to reduce the pain of the patients, because some scholars have pointed out the need for the nursing team to effectively communicate with the competent physician at any time to make reasonable treatment plan adjustment according to the patient’s situation8.What’s more, the treatment of femoral neck fractures with internal fixation mainly uses 3 cannulated compression screws, dynamic hip screws, medial femoral buttress plate, proximal femur locking plate, intramedullary nail fixation, etc.9,10,11,12. The fixation method using 3 cannulated compression screws is widely used because of closed reduction and percutaneous nail placement, which reduces soft tissue damage and protects the biological environment of the fracture end2,7,13,14, and 3CCS placed in an inverted triangular fashion has the best fixation strength. However, for Pauwels type III femoral neck fractures, when 3CCS are used for treatment, the incidence of complications such as nonunion and femoral head necrosis is relatively high, with an 18% overall revision rate15. The main reason is that the fracture line of Pauwels type III fractures is relatively vertical, and the shearing force between the fracture ends is large. So, the conventional parallel screws have poor holding power on the fracture broken ends, which will easily cause displacement between the fracture ends and thus nonunion during postoperative weight bearing16.
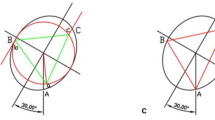
Gotfried et al.17 put forward the two concepts of positive support and negative support. Positive support refers to the inner upper edge of the distal fracture end of the femoral neck fracture protruding to the inside of the distal inner edge of the proximal fracture end. And the negative support refers to the medial inferior edge of proximal fracture end (femoral neck, head) protruding to the medial superior edge of distal fracture end of femoral neck. According to clinical observations, negative support is highly correlated with the failure of reduction of femoral neck fractures. Negative support can easily lead to recurring femoral head displacement and then varus. Therefore, negative support should be avoided during the reduction process. While positive support can have the opposite effect of negative support17,18. In order to improve the stability of Pauwels III femoral neck fractures, Mir and Collinge applied medial support plates to treat vertical femoral neck fractures11. Fixing the fracture line with the anti-sliding support plate can resist shear force19. A modified Smith-Peterson approach is used to place a support plate on the inside of the femoral neck, which can directly visualize the fracture site for anatomical reduction20. However, this surgical method is too traumatic. Therefore, based on the traditional inverted triangle fixation method, we envisaged to drive a 7.3 mm cannulated compression screw 4-6 cm below the greater trochanter and pass through the cortex above the contralateral lesser trochanter. Below the fractured end of the proximal fracture, a positive support is artificially formed, which is called the medial femoral neck support screw (Figs. 1, 2).

Model of medial femoral neck support screw.

Specimens of medial femoral neck support screw.
We aim to compare the biomechanical stability of three internal fixation methods through biomechanical tests, that is, 3 cannulated compression screws combined with femoral neck medial support screws (3CCS + mFNSS), traditional 3 cannulated compression screws (3CCS) and dynamic hip screws (DHS), and compare the advantages and disadvantages of the methods above through a clinical retrospective study, providing a theoretical basis for the clinical treatment of Pauwels type III femoral neck fractures.
Materials and methods
Biomechanical study of three types of internal fixation methods for Pauwels type III fractures of the femoral neck
Sample preparation
Nine recent adult antiseptic femoral specimens (provided by the Department of Anatomy of Zhejiang University School of Medicine) were selected, and were used in accordance with the Declaration of Helsinki. The specimens included femur pairs of 7 males and 2 females. Muscles and soft tissues were removed, and presence of deformities, fractures and tumors was ruled out. The femur was cut off at the knee joint, and the femoral neck was sawn off according to Pauwels 70° to make a femoral neck fracture model. Nine (18 in total) sets of femoral specimens were randomly divided into 3 groups of 6 in each group, the bone mineral density was checked by dual-energy X-ray bone densitometer, and the bone mineral density of each group of samples was analyzed. The results showed that there was no statistically significant difference in the distribution of bone mineral density among the samples of each group (P > 0.05). Each with three 7.3 mm cannulated (IDEAL MEDICAL, Jiangsu Ideal Medical science & technology co., LTD, Suzhou, Jiangsu, China) compression screws inverted triangle fixation (3CCS, group A) (Fig. 3), and DHS fixation (IDEAL MEDICAL, Jiangsu Ideal Medical science & technology co., LTD, Suzhou, Jiangsu, China) (DHS, group B) (Fig. 4), three 7.3 mm cannulated compression screws inverted triangle combined with 1 medial femoral neck support screw fixation (3CCS + mFNSS, Group C) (Fig. 5). Three cannulated screws were used to fix the femur according to the conventional method. The support screw was located under the distal screw of the inverted triangle and was kept 2 cm away the femoral trochanter. The head of the screw was 5 mm out of the femoral neck, just supporting the proximal fractured end of the Pauwels III femoral neck. The fixation of the specimens was performed under the fluoroscopy of the c-arm X-ray machine, and all specimens were anatomically reduced.

Three cannulated compression screws (3CCS) (Note: Positive and lateral X-ray film after internal fixation).

Dynamic hip screw (DHS) (Note: Positive and lateral X-ray film after internal fixation).

Medial femoral neck support screw combined with three cannulated compression screws (3CCS + mFNSS) (Note: Positive and lateral X-ray film after internal fixation).
Biomechanical test
The condyle of the femur was placed in a self-made clamp to simulate the weight-bearing situation of a normal individual on one foot in a standard anatomic posture, distal femoral fixation was performed with screws, and the gap between the clamp and the femur was filled and fixed using German Dantener super-hard plaster type IV (Germany, Dentona Co.). Compression test, torsion test and fatigue test are carried out in sequence. During the torsion test, the femoral head was fixed with a special clamp, and the gap between the femoral head and the clamp was filled with German Dantener super-hard plaster type IV.
Compression test
The specimens from the three groups were fixed on a Zwick / Z010 biomechanical testing machine (Zwick, Germany). By mounting the extensometer vertically on both sides under the osteotomy line (provided by the laboratory of Materials Mechanics, Zhejiang University, China), each femur was first pre-compressed at 100 N for 5 times to remove creep, and then the extensometer was zeroed (Fig. 6). The specimens were loaded vertically at 20 N/s, and the pressures were recorded by the mechanical testing machine as 500 N, 600 N, and 700 N, and the strain gauge values of the extensometer were taken down. Each femur was measured 3 times and the corresponding average value was taken. The extensor measured strain values were converted to displacement values, and their stiffness was obtained separately.

Compression test.
Torsion test
Specimens from the three groups were fixed on a ctt-1000 torsional testing machine (xinsansi company, China) (Fig. 7). Each femur was first pre-compressed 5 times at 3° to facilitate creeping out, and then subjected to torsion at loading speed of 0.5°/s. T The direction of the torsion was to twist the femoral shaft was laterally (simulating the abduction movement of the human hip joint). And the corresponding values were recorded. Each femur was measured 3 times and the corresponding mean value was taken, and its stiffness was calculated separately.

Torsion test.
Fatigue test
The specimens of the 3 groups were fixed on a suns890-100 fatigue testing machine (China, Sansi Co.) (Fig. 8). High frequency extensometers (provided by the laboratory of Materials Mechanics, Zhejiang University) were mounted vertically on both sides of the osteotomy line by a 100–700 n sine wave loading at 2 Hz frequency, cycle 10,000 times. This cycle is an amount of activity that mimics the hip joint of a normal person for 4–6 weeks. 4–6 weeks after surgery is the most important period for the strong fixation of fractures. The values of the extensometer strain were recorded after 10,000 cycles and converted into residual deformation at the broken end of the femoral fracture. (The residual deformation is also called unrecoverable deformation. The structure is deformed under load, and the deformation can only be partially recovered after unloading the load, and the unrecoverable part is called residual deformation).

Fatigue test.
Statistical analysis
Doctor Ruan used SPSS 22.0 and Origin 9.0 statistical software were used for statistical analysis of the obtained data. The measurement data was expressed as (\(\overline{{\text{X}}}\) ± S) . After it was verified that data was normally distributed and the homogeneity of variance is met, the repeated variance analysis was performed. We used the SNK (Student–Newman–Keuls) test for pairwise comparisons. Test level α = 0.05, P < 0.05 is statistically significant.
Clinical application
General clinical information
This experiment was approved by the Medical Ethics Committee of the No.1 People's Hospital of Yuhang District, Hangzhou, China. The study was conducted in accordance with code of ethics of the Declaration of Helsinki. All study subjects signed informed consent. n = 131 patients were enrolled from January 2015 to December 2017. Inclusion criteria were: (1) Age > 18 years and < 65 years, (2) X-ray examination showed that the fracture was significantly displaced, Pauwels type III (Pauwells angle > 50°), (3) Femoral neck fractures were all fresh fractures, and the fracture time was less than 3 weeks, (4) The proximal anatomy of the femur was normal before the fracture, and there was no history of hip disease, (5) BMD showed T > − 2.5. Exclusion criteria include femoral neck fractures with unclosed epiphyses, femoral neck fractures of the subhead and base, old femoral neck fractures, those with a history of hip disease or pathological fractures, and those who cannot tolerate surgery. According to the different surgical methods, patients were divided into a control group (n = 75) and a research group (n = 56) (Fig. 9). There was no statistically significant difference in general data between the two groups (P > 0.05). Table 1 presented all the details of the comparison of general characteristics among two groups.

Clinical research flow chart.
Surgical method
Reduction method
The patient underwent continuous external hard or combined anesthesia and was placed in the supine position. All femoral neck fractures were treated under the auxiliary reduction with the help of the bone traction bed. Generally, the traction of the affected limbs was required to restore the shortened deformity, and the internal and external rotation of the lower limbs was used to correct the rotational deformity. The fluoroscopy of the affected hip is needed to judge the anteversion angle of the femoral neck. The fluoroscopy of the hip joint is used to determine the femoral neck shaft angle. If necessary, the healthy hip can be seen. The trochanter shape is used as a comparison to evaluate the degree of correction of lower limb rotation. The reduction quality of femoral neck fracture adopts the standard proposed by Haidukewych et al. When the displacement of the broken end is less than 2 mm and any plane abnormal angle is less than 5°, it is “excellent”; when the displacement is 2–5 mm or the angle is 5°–10°, it is “good”, when the displacement is 5–10 mm or at an angle of 10°–20°, the reset is considered “normal”, and when the displacement is > 10 mm or at an angle > 20°, it is judged as “poor”.
Inverted triangular cannulated compression screw (3CCS)
After disinfection, a straight incision or a small percutaneous incision was made 5 cm below the greater trochanter, and 1 introducer needle was drilled percutaneously parallel to the femoral head with a guide wire to make parallel to the femoral neck axis and anteversion, and then fluoroscopy was performed again to clarify the needle position. 2 parallel introducers were punched again, depending on the position of the introducer needle. Once the position is satisfactory, an appropriate cannulated compression screw type is selected based on the length of the guide pin and arranged in form of inverted triangles in the femoral neck. It should be noted that the tip of the cannulated screw is 5 mm below the cartilaginous surface of the femoral head, the screw threads must all pass through the fracture line, and the inferior screw attempts to follow the superior femoral distance, and, if necessary, a gasket is added to the screw tail so as not to sink the caudal end of the nail into the cortex. After driving the compression screw, the guide needles were withdrawn separately, and the lateral hip fluoroscopy was performed. If the position was good, the incision was closed with irrigation.
Inverted triangular cannulated compression screw (3CCS + mFNSS)
After disinfection, a straight incision or a small percutaneous incision was made 5 cm below the greater trochanter of the femur, 1 introducer needle was drilled percutaneously parallel to the femoral head with a guide wire to the femoral neck axis and anteversion, and then fluoroscopy was performed again to clarify the needle position. 2 parallel introducers were punched again, depending on the position of the introducer needle, 2 parallel introducers were drilled 2 cm below the femoral trochanter position with satisfactory placement, and 2 cm below the femoral trochanter position. With 1 parallel introducer pin punched into place just below the fracture line of the femoral neck, an appropriate length of medial support screw punched into the femoral neck was chosen according to the length of the introducer needle so that the superior end of the screw just weighed out of the fracture line. The proximal end of the fracture was punched over the medial support screw, and appropriate cannulated compression screws punched into the femoral neck were chosen according to the length of the 3 introducer pins punched into before, arranged in form of inverted triangles in the femoral neck.
Postoperative management
Postoperative routine infection prevention, intravenous antibiotics for 1d, and encourage the quadriceps muscle contraction, ankle dorsiflexion and plantar flexion activities, and crutches without weight-bearing on the first day after surgery. On the second postoperative day, X-ray, CT plain scan + 3D reconstruction was performed. Six weeks after surgery, patients started walking without crutches. X-rays and CT films were reviewed in January, March, June, September, December, and 24 months after surgery.
Efficacy evaluation
-
(1)
Compare the operation-related indexes of the two groups of patients: operation time, intraoperative bleeding, and postoperative fracture healing time. The radiographs were taken after the operation and evaluated using garden’s index21.The reposition quality is divided into four grades, the first grade is excellent: the positive position is 160° , the side position is 180° , the second grade is good: the positive position is 155° , the side position is 180° , the third grade is normal: the positive position is < 150° , or the side position > 180° , the fourth grade is poor, the positive position is 150° , the side position is > 180° . And the excellent + good rate = excellent rate + good rate.
-
(2)
The fracture healing, the screw retreatment rate and fixation failure rate, the necrosis rate of the femoral head, and the hip function were observed at the follow-up visit. The evaluation criteria of hip function were referred to the Harris scoring criteria22. A total score of 100, 90 and above is considered excellent, 80–89 is considered good, 70–79 is considered normal, and 70 or below is considered poor. The rate of excellent + good = (excellent + good)/total cases × 100%. Postoperative complications were compared by telephone or outpatient review at 24 months. Resolution of nails and varus appearance on radiographs were recorded.
Statistical method
Doctor Ruan used SPSS 22.0 statistical software package to analyz the data, the measurement data was expressed by (\(\overline{{\text{X}}}\) ± S), and t test was used. The count data was tested by the X2 test. P < 0.05 is considered as statistically significant.
Results
Biomechanical test results
Compression test
The vertical load- shift relations of three internal fixation methods in the vertical compression tests were shown in Fig. 10. The linear correlation between vertical load and average vertical shift are established by correlation coefficients R of 3CCS, 3CCS + mFNSS, DHS equal to 0.99983, 0.98758, 0.99992. This means that the specimen deforms elastically within such range of vertical load. The average compression stiffness of the 3CCS, 3CCS + mFNSS, and DHS are 1560.06 N/mm, 2481.39 N/mm, and 8333.33 N/mm, respectively. This was consistent with the linear fit of the three groups: the DHS had the highest stiffness, 3CCS + mFNSS, was the second, and the 3CCS was the worst. When the vertical length was 500 N, 600 N and 700 N, the shift of 3CCS + mFNSS Pauwels type III fractures of femoral cervical occipital nails was significantly smaller than that of traditional 3CCS fixation, and the differences were statistically significant (P < 0.05). However, with a fixed ratio of DHS, the shift was relatively large and the difference is statistically significant (P < 0.05).

Left, vertical displacement under the load of 400, 600 and 800 N; right: linear fitting of average vertical shift and vertical load.
Torsion test
The vertical load-shift relations of three internal fixation methods during in the torsion test were shown in Fig. 11. The linear correlation between torsion angle and average torque were established by correlation coefficients R of 3CCS, 3CCS + mFNSS, DHS equal to 0.99983, 0.98758, 0.99992. This indicates the elastic deformation of femoral neck specimens within such range of torsion angle. The average torsional stiffness of 3CCS, 3CCS + mFNSS, DHS are 2.27 N.m/°, 3.54 N.m/°, and 3.33 N.m/°, respectively. The torsional rigidity of 3CCS + mFNSS was the largest, followed by DHS, and the 3CCS were the smallest. This was in nice agreement with the slope of the torsion angle-average torque fitting line. When the torsion angle is 1°–5°, the torque of the femoral neck Pauwels type III fracture fixed 3CCS + mFNSS was significantly greater than that of the 3CCS and DHS fixation, and the differences were statistically significant (all P < 0.05).

Left, torque under torsion angle of 1–5°; right: linear fitting of torque and torsion angle.
Fatigue test
In the fatigue test, the residual deformations of the fracture end of the three groups of femoral neck fractures after 10,000 cycles were compared. The residual deformation by 3CCS + mFNSS (1.080 ± 0.018 mm) was smaller than that by 3CCS (1.150 ± 0.025 mm). This difference was statistically significant (P < 0.05). But this value is greater than the one by DHS (0.396 ± 0.017 mm) and the difference is statistically significant (P < 0.05).
Clinical results
Comparison of two groups’ clinical indicators
In the study group, the operative time ranged from 74 to 157 min, with a mean of 117.21 ± 13.72 min, intraoperative blood loss ranged from approximately 16 to 29 ml, with a mean of 21.05 ± 3.42 ml, and the rate of good + excellent quality of fracture reduction was 57.14% (32/56). In the control group, the operative time ranged from 34 to 78 min, with a mean of 44.15 ± 6.53 min, intraoperative blood loss is from approximately 5 to 30 ml, with a mean of 9.01 ± 2.95 ml. The rate of good + excellent quality of fracture reduction was 58.67% (44 / 75). Intraoperative bleeding and operative time were longer in the study group than that in the control group (P < 0.05). There was no significant difference in the quality of fracture reduction between the groups (P > 0.05).
Comparison of postoperative follow-up and complications
The incisions in both groups were of grade A healing. In the study group, 2 patient developed screw retreatment (screw retreatment rate 3.57%), 1 patient had osteonecrosis of the femoral head (necrosis rate 1.79%), and 54 patients had fracture healing (healing rate 96.43%), whereas in the control group, 13 patients developed screw retreatment (screw retreatment rate 17.33%), 9 patients had osteonecrosis of the femoral head (necrosis rate 12.00%), and 64 patients had fracture healing (healing rate 85.33%), and the study group had lower rates of nail retreatment and osteonecrosis of the femoral head than the control group. The fracture healing rate was superior to that of the control group, and the difference was statistically significant (P < 0.05). Table 2 shows a comparison of two groups of clinical indicators. Table 3 shows a cmparison of postoperative follow-up and complications. See Figs. 12a,b, 13a,b, 14a–c) for typical cases.

(a, b) The positive side radiographs of the injured side of the patient at the time of admission (Note: The patient was a 47-year-old male. He was admitted to the hospital for 2 h due to a high fall injury).

(a, b) The X-ray positive radiographs reviewed on the second day after surgery (Note: The patient was a 47-year-old male. He was admitted to the hospital for 2 h due to a high fall injury).

(a) The situation of percutaneous insertion of the guide needle after closed reduction during surgery. (b) The placement of the medial femoral neck brace. Due to the need to form positive support and resist shear forces, this screw is placed first. (c) is the placement of 3 cannulated screws and the medial femoral neck support screws to observe whether the placement of the screw is appropriate (Note: The patient was a 47-year-old male. He was admitted to the hospital for 2 h due to a high fall injury).
Discussion
Most patients with femoral neck fractures under the age of 65 have tough bones, and fractures are mostly caused by high-energy injuries such as traffic injuries, injuries from falls from heights, and heavy crushing. Such fractures have a high rate of reoperation, as well as a high rate of nonunion and osteonecrosis of the femoral head. Related studies have reported that the rate of postoperative nonunion is 10–33% and that of avascular necrosis of the femoral head is 20–30%23,24. And the causes of many complications of this fracture can be divided into two major categories: biological factors, which include blood supply, bone mineral density (BMD), age, and oxygen tension in the medullary cavity, as well as biomechanical factors, which include fracture classification, surgical reduction situation, etc.25,26. Recently, some scholars have focused on reducing the incidence of postoperative complications by changing the biomechanical pattern of internal fixation and the local biological environment, etc. In addition, in the Pauwels classification of femoral neck fractures, the stresses at the fracture ends of Pauwels type I and II are compressive stresses, while for the Pauwels type III, the stresses at the fracture ends are shear stresses27, and greater angulation is associated with greater fracture shear, which is detrimental to the healing of postoperative fractures. Reports indicate that nonunion occur in 16–59% of Pauwels type III femoral neck fractures and osteonecrosis of the femoral head occur in 11–86% of Pauwels type III femoral neck fractures28. The key points for the success of fracture treatment in Pauwels type III femoral neck fractures are: maintaining the stability of reduction and fixation without disrupting the blood supply to the femoral head, and the ability of the fixative to resist vertical shear forces. Multiple cancellous screws are most commonly used in the treatment of young patients with femoral neck fractures. And the potential advantage of using cancellous screws is their easier placement. In addition, cancellous screws can be placed percutaneously, and other advantages include preservation of bone volume, improved rotational function, preservation of blood supply to the hip, etc.
In this study, biomechanical testing was performed using conventional 3CCS, DHS internal fixation and 3CCS + mFNSS for the treatment of Pauwels type III femoral neck fractures, respectively. From the results of biomechanical studies, only 3CCS showed the worst test results in all aspects, while DHS showed excellent results in both compression test and fatigue test. However, in terms of the torsion test, 3CCS + mFNSS are the best performers. From the biomechanical results, it can be found that 3CCS + mFNSS can all be fixed by percutaneous placement of screws after closed reduction compared with the conventional 3CCS and can be biomechanically superior because they can effectively resist the shear forces on the fracture ends. Compared with DHS, though it is a little deficient in vertical compression as well as fatigue resistance, DHS has complicated surgical operations and cannot be done percutaneously in a real sense, and the postoperative incidence of femoral neck shortening is high, as well as it can easily lead to gluteal weakness and affect the stability and function of the hip joint. Some studies have shown that DHS affects the blood supply of the femoral head much more than 3CCS alone29. In addition, DHS also causes substantial bone loss, making salvage surgery more difficult. Bhandari et al.16 argued that DHS would be difficult to implement as a salvage procedure once the procedure failed.
In the clinical retrospective study, we comparatively analyzed 131 patients with femoral neck fractures treated with percutaneous internal fixation using two internal fixation methods, which is 3CCS and 3CCS + mFNSS. Surgical data as well as postoperative follow-up data were analyzed, and 3CCS + mFNSS was longer than the conventional fixation of only 3CCS in terms of intraoperative bleeding as well as operative time, (P < 0.05). However, there was no significant difference in the quality of fracture reduction (P > 0.05). During the follow-up, there was one case of cannulated compression screw retreatment in the 3CCS + mFNSS group, which caused nonunion of fracture, but no necrosis of femoral head. 8 in the 3CCS group had cannulated compression screw retreatment, and 5 patients developed avascular necrosis of the femoral head, and the difference was statistically significant. In the comparison of hip function (Harris score), 3CCS + mFNSS group was superior to the 3CCS group, and the difference was statistically significant. From the clinical results, the medial support screw can effectively improve the fracture healing rate. It can also combat the failure of internal fixation caused by excessive vertical shear and reduce the risk of osteonecrosis of the femoral head. At the same time, good biomechanical stability can improve the functional recovery of hip joint, which is consistent with the results of the biomechanical research. The insertion of the medial support screw may cause a small increase in the operation time, intraoperative blood loss and fluoroscopy times. Although it was statistically significant, these three factors had little significance in the specific operation because of the small base.
Advantages of the medial support screw include: (1) Among the existing surgical techniques for Pauwels type III femoral neck fractures and under the premise of ensuring the original percutaneous manipulation stay unchanged, adding only one screw can effectively resist the shearing force of the fracture end. It can provide reliable positive support to the medial side. As that screw of the femoral neck support screw penetrate out under the fracture line, the vertical shear stress at the proximal fracture end can be reduced, so that the blood supply damage caused by the movement of the fracture broken end after fracture surgery and the fracture nonunion caused by overlarge stress at the fracture fix end are reduced. Our biomechanical study also confirm that femoral neck support screws perform better than cannulated lag screws in vertical compression, torsion, and fatigue tests. (2) Follow the correct method to place the medial support screw may not add the risk of subtrochanteric fractures. Because some scholars proposed that biomechanical tests as well as clinical studies suggested that the two screws at the level of the lateral femoral trochanter converged more than 2 cm caudally to disperse the stress greatly and reduce the risk of subtrochanteric fracture30,31. And in our biomechanics research, no subtrochanteric fracture occurred in the small trochanter level, inverted triangle and medial femoral support screw tests. The point of support screw insertion was kept as far as 2 cm away from the most distal screw of inverted triangle, and parallel inverted triangle screw orientation placement was not necessary to be pursued. However, it has also been reported that32,33,34,35, femoral neck fracture screw fixation located at the level of the lesser trochanter increases the risk of fracture by heightening the subtrochanteric stress. But biomechanical tests performed by Erica et al.36 indicated that the screws caused subtrochanteric fracture at the level of the lesser trochanter, which mainly occurred in osteoporotic femurs. In this study, we excluded people over 65 years of age, which may have biased our clinical results toward the population study results. However, in the Chinese Clinical Guidelines, for people over 65 years of age, although internal fixation treatment is available, physicians prefer femoral head replacement or total hip replacement for this population with the expectation that patients will achieve early ambulatory functional rehabilitation exercises with reduced risk of prolonged bed rest. At the same time, because of elderly patients, especially male patients, hip replacement surgery can increase the risk of heterotopic ossification37.Therefore, our clinical enrollment cases excluded osteoporotic patients older than 65 years, and no subtrochanteric fracture was found in the long-term postoperative follow-up, which may certainly be related to our small clinical sample size and not long enough follow-up. From a retrospective review, we obtained good clinical results, but long-term follow-up studies as well as multicenter large sample studies in our later years are still needed.
Disadvantages of the medial support screw include: (1) Disadvantages of the medial support screw include: (1) This study is a retrospective study, so it may be at risk for several sources of bias, among which confounding. Statistical analysis of the collected data may therefore not well present the true clinical results. (2) The sample size of clinical retrospective study is small, which may produce false positives and false negatives for statistical analysis results, thus interfering with our accurate judgment of the study, and also misleading our clinical work and other orthopedic doctors. (3) Adding a femoral neck supporting screw is bound to damage the tissues around the hip joint more than 3CCS, and at the same time increase the operation time, bleeding risk and fluoroscopic exposure risk. Because of the high nail placement position requestment, it is not very friendly to surgery doctors who are new to this technique. In the early stage of developing this technique, it takes us a lot of time to adjust the position in order to obtain a good femoral neck positive support. Therefore, for doctors who are launch to this technique for the first time, we suggest to read the film carefully before operation, and design the puncture path and position in advance in combination with CT and 3D printing technology, so as to avoid repeated puncture and positioning during operation, and increase the risk of blood supply damage of femoral head and occupational radiation exposure. (4) Our study has a short follow-up time, which can not reflect the long-term effect of the two surgical methods. Therefore, we need to continue to follow up the patients to get more prepared clinical results. However, as far as the short-term results are concerned, the femoral neck supporting screw designed by us still has certain advantages.
Conclusions
Through biomechanical research, 3CCS + mFNSS can effectively resist the vertical shear force of Pauwels type III fractures, and at the same time has good stability to the fracture end. At the same time, reasonable nail placement can effectively avoid the risk of fracture. Through clinical retrospective research, 3CCS + mFNSS can effectively reduce the nonunion rate of fractures and bring fewer complications than 3CCS. It can bring new clinical treatment ideas for the internal fixation of patients with Pauwels type III fractures in the future.
References
Ju, D. G. et al. Nationwide analysis of femoral neck fractures in elderly patients: A receding tide. JBJS 99(22), 1932–1940 (2017).
Luttrell, K., Beltran, M. & Collinge, C. Preoperative decision making in the treatment of high-angle “vertical” femoral neck fractures in young adult patients: an expert opinion survey of the orthopaedic trauma association’s (OTA) membership. J. Orthop. Trauma 28(9), e221–e225 (2014).
Collinge, C. A., Mir, H. & Reddix, R. Fracture morphology of high shear angle “vertical” femoral neck fractures in young adult patients. J. Orthop. Trauma 28(5), 270–275 (2014).
Pauwels, F. Der Schenkelhalsbruch, ein mechanisches Problem. Grundlagen des Heilvorganges: Prognose und kausale Therapie. 63(Suppl) (1935).
Shen, M. et al. An update on the Pauwels classification. J. Orthop. Surg. Res. 11(1), 1–7 (2016).
Wang, S. H. et al. Using a modified Pauwels method to predict the outcome of femoral neck fracture in relatively young patients. Injury 46(10), 1969–1974 (2015).
Freitas, A. et al. Biomechanical study of different internal fixations in Pauwels type III femoral neck fracture—A finite elements analysis. J. Clin. Orthop. Trauma 14, 145–150 (2020).
Biz, C. et al. Clinical practice and nursing management of pre-operative skin or skeletal traction for hip fractures in elderly patients: a cross-sectional three-institution study. Int. J. Orthop. Trauma Nurs. 32, 32–40 (2019).
Yang, J.-J. et al. Risk factors for nonunion in patients with intracapsular femoral neck fractures treated with three cannulated screws placed in either a triangle or an inverted triangle configuration. JBJS 95(1), 61–69 (2013).
Davey, M. S. et al. Two-hole versus four-hole plate dynamic hip screw: A systematic review of current evidence. Irish J. Med. Sci. 189, 1–6 (2020).
Mir, H. & Collinge, C. J. M. H. Application of a medial buttress plate may prevent many treatment failures seen after fixation of vertical femoral neck fractures in young adults. Med. Hypotheses 84(5), 429–433 (2015).
Guo, J. et al. Intramedullary nails with cannulated screw fixation for the treatment of unstable femoral neck fractures. J. Int. Med. Res. 47(2), 557–568 (2019).
Imren, Y. et al. Biomechanical comparison of dynamic hip screw, proximal femoral nail, cannulated screw, and monoaxial external fixation in the treatment of basicervical femoral neck fractures. Acta Chir Orthop. Traumatol. Cech. 82(2), 140–144 (2015).
Widhalm, H. K. et al. A comparison of dynamic hip screw and two cannulated screws in the treatment of undisplaced intracapsular neck fractures—Two-year follow-up of 453 patients. J. Clin. Med. 8(10), 1670 (2019).
Slobogean, G. et al. Complications following young femoral neck fractures. Injury 46(3), 484–491 (2015).
Bhandari, M. et al. Operative management of displaced femoral neck fractures in elderly patients: An international survey. JBJS 87(9), 2122–2130 (2005).
Gotfried, Y., Kovalenko, S. & Fuchs, D. Nonanatomical reduction of displaced subcapital femoral fractures (Gotfried reduction). J. Orthop. Trauma 27(11), e254–e259 (2013).
Xiong, W.-F. et al. Inferior calcar buttress reduction pattern for displaced femoral neck fractures in young adults: a preliminary report and an effective alternative. J. Orthop. Surg. Res. 14(1), 1–8 (2019).
Stacey, S. C. et al. Tips and tricks for ORIF of displaced femoral neck fractures in the young adult patient. Eur. J. Orthop. Surg. Traumatol. 26(4), 355–363 (2016).
Ye, Y. et al. Medial buttress plate augmentation of cannulated screw fixation in vertically unstable femoral neck fractures: Surgical technique and preliminary results. Injury 48(10), 2189–2193 (2017).
Garden, R. S. Stability and union in subcapital fractures of the femur. J. Bone Jt. Surg. Br. Vol. 46(4), 630–647 (1964).
Harold, R. E. et al. Patient-Reported Outcomes Measurement Information System Correlates With Modified Harris Hip Score in Total Hip Arthroplasty. Orthopedics 44(1), e19–e25 (2020).
Pauyo, T. et al. Management of femoral neck fractures in the young patient: A critical analysis review. World J. Orthop. 5(3), 204 (2014).
Madhu, T. S. et al. Treatment of developmental dislocation of hip: Does changing the hip abduction angle in the hip spica affect the rate of avascular necrosis of the femoral head?. J. Pediatr. Orthop. 22(3), 184–188 (2013).
Wang, T. et al. Analysis of risk factors for femoral head necrosis after internal fixation in femoral neck fractures. Orthopedics 37(12), e1117–e1123 (2014).
Schweitzer, D. et al. Factors associated with avascular necrosis of the femoral head and nonunion in patients younger than 65 years with displaced femoral neck fractures treated with reduction and internal fixation. Eur. J. Orthop. Surg. Traumatol. 23(1), 61–65 (2013).
Noda, M. et al. Biomechanical study using the finite element method of internal fixation in Pauwels type III vertical femoral neck fractures. Arch. Trauma Res. 4(3), e23167 (2015).
Parker, M. J. Results of internal fixation of Pauwels type-3 vertical femoral neck fractures. JBJS 91(2), 490–491 (2009).
Madsen, F. et al. Fixation of displaced femoral neck fractures: A comparison between sliding screw plate and four cancellous bone screws. Acta Orthop. Scand. 58(3), 212–216 (1987).
Filipov, O. & Gueorguiev, B. J. I. Unique stability of femoral neck fractures treated with the novel biplane double-supported screw fixation method: a biomechanical cadaver study. Injury 46(2), 218–226 (2015).
Filipov, O. B. Biplane double-supported screw fixation of femoral neck fractures: Surgical technique and surgical notes. J. Am. Acad. Orthop. Surg. 27(11), e507 (2019).
Karr, R. K., Schwab, J. P. J. C. O. & Research, R. Subtrochanteric fracture as a complication of proximal femoral pinning. Clin. Orthop. Relat. Res. 194, 214–217 (1985).
Oakey, J. W. et al. Does screw configuration affect subtrochanteric fracture after femoral neck fixation?. Clin. Orthop. Relat. Res. 443, 302–306 (2006).
Kloen, P. et al. Subtrochanteric fracture after cannulated screw fixation of femoral neck fractures: A report of four cases. J. Orthop. Trauma 17(3), 225–229 (2003).
Pelet, S. et al. Sub-or intertrochanteric fracture following screw fixation of an intracapsular proximal femoral fracture: true complication or technical error?. Swiss Surg. 9(2), 82–86 (2003).
Crump, E. K. et al. Does screw location affect the risk of subtrochanteric femur fracture after femoral neck fixation? A biomechanical study. Clin. Orthop. Relat. Res. 478(4), 770–776 (2020).
Biz, C., Pavan, D., Frizziero, A., Baban, A. & Iacobellis, C. Heterotopic ossification following hip arthroplasty: A comparative radiographic study about its development with the use of three different kinds of implants. J. Orthop. Surg. Res. 14(10), 176 (2015).
Author information
Authors and Affiliations
Contributions
Z.G.: Design the study M.W.*: Design the study B.S.: Complete literature review and finish the draft X.C.: Conduct experiment and data analysis D.R.: Complete literature review and finish the draft.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Gao, Z., Wang, M., Shen, B. et al. Treatment of Pauwels type III femoral neck fracture with medial femoral neck support screw: a biomechanical and clinical study. Sci Rep 11, 21418 (2021). https://doi.org/10.1038/s41598-021-01010-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-021-01010-1
This article is cited by
-
Novel screw fixation placement configuration for the treatment of Pauwels type III femoral neck fractures: a finite element analysis
Medical & Biological Engineering & Computing (2023)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
