
Abstract
The neutrophil-to-lymphocyte ratio (NLR) in peripheral blood reflects the balance between systemic inflammation and immunity and is emerging as a prognostic biomarker in many diseases, but its predictive role for mortality in the general population has not been investigated. We analyzed 1999–2014 National Health and Nutrition Examination Survey mortality-linked data, followed up until 2015. In participants aged > 30 with measurements of differential white blood cell counts, NLR was calculated and categorized into quartiles. Associations of increased NLR with overall or cause-specific mortality were assessed with Cox proportional hazard regression models, adjusted for potential confounders. Increased NLR was associated with overall mortality (hazard ratio [HR] 1.14, 95% confidence interval [CI] 1.10–1.17, per quartile NLR) and mortality due to heart disease (1.17, 1.06–1.29), chronic lower respiratory disease (1.24, 1.04–1.47), influenza/pneumonia (1.26, 1.03–1.54) and kidney disease (1.26, 1.03–1.54). NLR was associated with cancer mortality only in the first follow-up year (HR 1.48, 95% CI 1.11–1.98). The association with chronic lower respiratory disease mortality was stronger in individuals with prevalent lung diseases (HR 1.46, 95% CI 1.14–1.88, Pinteraction = 0.01), while NLR showed positive associations with mortality from heart disease (1.21, 1.07–1.38) and cerebrovascular disease (1.30, 1.04–1.63) only among individuals without these conditions at baseline. NLR is associated with mortality overall and due to certain causes in the general population. Associations over short follow-up intervals and among individuals with conditions at baseline suggest effects of disordered inflammation and immunity on progression of those conditions, while other associations may reflect contributions to disease etiology.
Similar content being viewed by others
Introduction
Inflammation and immunity play a critical role in many chronic diseases1,2,3. The neutrophil-to-lymphocyte ratio (NLR), calculated as a simple ratio between the neutrophil and lymphocyte counts measured in peripheral blood, is a biomarker which reflects the balance between two aspects of the immune system: acute and chronic inflammation (as indicated by the neutrophil count) and adaptive immunity (lymphocyte count). NLR has been extensively evaluated4 and shown to be associated with outcome and predict disease course among patients with a variety of medical conditions including ischemic stroke5,6, cerebral hemorrhage7,8, major cardiac events9,10 and sepsis and infectious diseases11. Furthermore, in cancer patients higher NLR has been associated with poor prognosis12. These adverse associations may reflect the contributions of severe inflammation and poor immune function to the progression of these diseases.
By extension, NLR may be predictive of mortality in the general population, and thus the overall impact of inflammation and immunity on health13. Several studies have reported that higher NLR was significantly associated with overall mortality and mortality due to cardiovascular disease, but not with mortality due to cancer14,15,16,17. In addition, it is important to evaluate associations of NLR with cause-specific mortality over different intervals of follow-up time, because associations over short intervals after baseline measurement of NLR predominantly reflect the effects of disordered inflammation or immunity for people who already have these medical conditions. In contrast, associations over intervals of several years reflect effects of these processes on both the incidence of disease and survival after diagnosis. While some studies have assessed associations over different follow-up intervals for mortality due to cardiovascular disease, cancer or stroke15,17, no study has systematically assessed such associations for multiple diseases.
An improved understanding of the association of NLR with general population mortality will help clarify the role of inflammation and immunity in the development and outcomes of diverse medical conditions. We investigated NLR associations with overall mortality and, for a range of medical conditions, cause-specific mortality in a prospective analysis of a representative sample of the US general population. To distinguish effects of inflammation and immune dysfunction on incidence and progression of disease, we also assessed associations of NLR with cause-specific mortality across different intervals of follow-up time and among individuals with and without specified medical conditions at baseline.
Methods
The National Health and Nutrition Examination Survey (NHANES) is a population-based health survey of adults and children in the US, conducted by the National Center for Health Statistics (NCHS)18. NHANES uses a multistage probability sampling design to produce a nationally representative sample of the non-institutionalized US population. The survey consists of questionnaires administered in the home followed by physical examinations in mobile examination centers (MECs). In this study, we assessed participants from eight 2-year NHANES cycles conducted during 1999–2014. We included adults ≥ 30 years old with peripheral blood white blood count (WBC) and differential measurements.
Demographic information, medical history, and cigarette smoking status were ascertained from questionnaire data. Body mass index (BMI) was calculated from the physical examination weight and height (kg/m2). We inferred the baseline presence of diseases corresponding to the causes of death that we evaluated and risk factors for these conditions through the questionnaire responses and from laboratory measures of diabetes and kidney disease (Supplementary Table S1).
Blood specimens were collected as part of physical examinations, and WBCs were measured in the MECs. The WBC parameters were determined using the Beckman Coulter method of counting and sizing, and the automated differential was based on cell volume, conductivity, and light scatter technology19. We then calculated the NLR as the ratio of the derived neutrophil and lymphocyte counts.
NCHS previously linked NHANES participants with death certificate records from the National Death Index. We used the 1999–2014 NHANES public-use linked mortality files which provided mortality follow-up through December 31, 2015. Mortality outcomes in the public-use files include the following nine leading underlying causes of death (Tables 2, 3, 4): heart disease, cancer, chronic lower respiratory disease, unintentional injuries, cerebrovascular diseases, Alzheimer’s disease, diabetes, influenza and pneumonia, and kidney disease.
Statistical analyses were performed using pre-specified weighting that reflects the differential rates of participant selection as determined by the sample design and the inclusion of multiple NHANES surveys19. We used multiple variable Cox regression to assess NLR associations with overall and cause-specific mortality. Hazard ratios (HRs) were adjusted for age at baseline (i.e., MEC visit; continuous variable); sex; race/ethnicity (non-Hispanic white, non-Hispanic black, Mexican American, other Hispanic, other race/ethnicity); smoking (never, former, current smoker), BMI (< 18.5, 18.5–24.9, 25–29.9, 30+ kg/m2); baseline presence of diabetes mellitus, hypertension, and arthritis; and total WBC count. Follow-up time from the baseline visit was used as the timescale. NLR was categorized into quartiles based on the weighted distribution of results (NLR < 1.54, 1.54–2.00, 2.01–2.67, 2.68+). p values for trend across NLR quartiles were estimated using NLR quartile coded as an ordinal variable (values of 1, 2, 3 and 4) with 1-degree of freedom. We examined non-linear associations of NLR with mortality with restricted cubic spline functions using three knots placed at the 5th, 50th and 95th percentiles (NLRs of 1.00, 2.00 and 4.22)20.
We conducted two secondary analyses to further characterize NLR associations with mortality. First, we assessed associations between NLR and mortality outcomes within different time periods after baseline, with intervals categorized as the first year (0–11 months) and the rest of the follow-up period equally divided into tertiles based on the overall number of deaths (12–49, 50–93, and 94+ months) and tested for interactions between follow-up period and NLR (this interaction test corresponds to a test for proportional hazards). Presentation of results for cells with < 11 deaths were suppressed because of concerns about accuracy of the p values and confidence intervals (CIs). Consequently, for analyses with < 11 deaths in the 0–11-month period, p interactions were estimated for only the categories during 12+ months of follow-up.
Second, we explored whether the documented presence of a specific disease at baseline could affect the associations between NLR and mortality from that disease. We describe the distribution of times from baseline to death due to specified causes in individuals with or without those conditions at baseline. We then assessed HRs relating NLR to cause-specific mortality for diseased and non-diseased individuals, and we tested for heterogeneity by testing for an interaction between disease status and NLR.
All tests of statistical significance were based on two-sided p values of 0.05 and 95% CIs without adjustment for multiple comparisons. Analyses used SAS version 9.4 (SAS Incorporated, Cary, NC, USA) and its survey procedures to account for the complex sample design of NHANES.
Consent to participate
The Institutional Review Board approval and documented consent was obtained from all participants for the use of NHANES data21. We confirm that all methods were carried out in accordance with relevant guidelines and regulations.
Results
A total of 32,454 individuals were included in the study (Table 1). The mean age was 52.0 years at baseline, 48% were males, and 72% were non-Hispanic whites. Forty-eight percent were past or current smokers and 70% were overweight/obese. The prevalence of medical conditions of interest ranged from 10% (diabetes mellitus) to 35% (hypertension). The mean WBC count was 7.2 thousand cells/µl with mean neutrophil count of 4.3 thousand cells/µl and mean lymphocyte count of 2.1 thousand cells/µl. The mean NLR was 2.3. As shown in Table 1, compared with individuals with the lowest quartile of NLR, those with higher quartiles of NLR were older; more likely to be male, non-Hispanic whites, and current or former smokers; and more frequently to report the ascertained baseline medical conditions. Total WBC counts were also higher in participants with higher NLR quartiles.
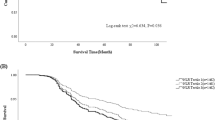
A total of 4975 deaths occurred during 3,008,113 person-years of follow-up (median 86 months, interquartile range 48–135). Figure 1A shows the weighted distribution of baseline NLR values according to vital status at the last follow-up. Individuals who died had higher NLRs compared to those alive, with median NLRs of 2.33 vs. 1.99, respectively, although the overlap was substantial. With regards to specified causes of mortality, we observed that deaths from various medical conditions occurred earlier during follow-up among individuals who had baseline evidence for those conditions than in those without the conditions (Fig. 1B). The number of deaths by cause for each NLR quartile category is shown in Supplementary Table S2.

(A) Distribution of neutrophil-to-lymphocyte ratios among individuals according to vital status on follow up date. Results are weighted using NHANES survey sample weights. The x-axis is truncated at an NLR of 13, and not included in the graph are N = 11 surviving participants (weighted percentage 0.03%) and N = 11 deceased (0.20%) with greater values. (B) Follow-up time (months) in individuals who died from specified diseases, with or without those diseases at baseline.
Table 2 describes associations of NLR with mortality. Increasing NLR was significantly associated with higher overall mortality (HR 1.14, 95% CI 1.10–1.17, per quartile of NLR). Higher NLR was also significantly associated with mortality due to specific causes including heart disease (HR 1.17, 95% CI 1.06–1.29, per quartile of NLR), chronic lower respiratory diseases (1.24, 1.04–1.47), influenza/pneumonia (1.26, 1.03–1.54), and kidney diseases (1.62, 1.21–2.17). For Alzheimer’s disease, quartiles 2, 3, and 4 of NLR were associated with elevated mortality, compared with quartile 1, but the linear trend was not significant (p = 0.06). Also, there were no notable associations of NLR with mortality due to cancer, cerebrovascular disease, accidents, or diabetes mellitus. We did not identify any nonlinear associations of NLR with overall or cause-specific mortality in models that included cubic regression splines (Supplementary Figure S1).
We also assessed NLR associations within different time periods of follow-up (equivalent to an evaluation of the proportional hazards assumption; Table 3). There was a suggestion that the association of NLR with overall mortality was strongest in the first 12 months of follow-up (HR 1.39, 95% CI 1.23–1.57, per quartile of NLR), with lower HRs (95% CIs) of 1.17 (1.11–1.24), 1.18 (1.11–1.24), and 1.03 (0.98–1.08) for 12–49, 50–93, and 94+ months after baseline, but this trend was not statistically significant (Pinteraction = 0.052). Similarly, although there was no association of NLR with cancer mortality for the overall follow-up, the HR was highest in the first 12 months (HR 1.48, 95% CI 1.11–1.98, per quartile of NLR) with a decline in strength over time (Pinteraction = 0.041). The association of NLR with cerebrovascular disease mortality increased over time (Pinteraction = 0.033), although no HR was significant in any interval. Although limited by case counts in the first 12 months after baseline, HRs for influenza/pneumonia appeared to decline over time across the remaining period (Pinteraction = 0.047). There was no significant variation of HRs over time for heart disease, chronic lower respiratory disease or kidney disease.
Finally, in an additional set of analyses we assessed associations of NLR with overall mortality for individuals with or without specific diseases that were present at baseline (Table 4). HRs among individuals with baseline disease were significant for cancer (HR 1.18, 95% CI 1.05–1.32, per quartile of NLR), chronic lower respiratory disease (1.46, 1.14–1.88) and kidney disease (1.81, 1.32–2.47). In contrast, NLR showed positive associations with mortality from heart disease (HR 1.21, 95% CI 1.07–1.38, per quartile of NLR) and cerebrovascular disease (1.30, 1.04–1.63) only among individuals without those conditions at baseline. However, the interaction between NLR and preexisting disease was significant (Pinteraction = 0.01) only for chronic lower respiratory disease.
Discussion
In this prospective study of a representative sample of the US general population, we observed associations of NLR with subsequent overall mortality and mortality related to specific conditions, including heart disease, chronic lower respiratory disease, influenza/pneumonia, and kidney disease. The NLR association with overall mortality appeared strongest in the immediate 1-year period after the baseline blood measurement, and we also observed a strong association with cancer mortality within this period. NLR was significantly associated with cancer or chronic lower respiratory disease mortality in individuals with a prior history of these diseases, and with heart disease and cerebrovascular disease mortality in individuals without prior histories of these diseases. These associations with NLR were independent of total WBC, smoking, BMI, and the presence of other chronic medical conditions.
An increase in NLR is determined by an increase of neutrophils and/or reduction in lymphocytes. Neutrophils play a major role in inflammation in pathologic conditions such as microbial infection, chronic tissue damage, and cancer22,23. An increase in circulating neutrophils is thus suggestive of an acute or chronic inflammatory response. Lymphocytes generate adaptive immune responses to eliminate specific pathogens, infected cells, and, in some instances, premalignant or malignant cells24,25. Decreases in circulating lymphocytes occur in association with recent infection, use of certain medications including chemotherapy, and in some immune-related medical conditions, including rheumatoid arthritis26. Neutrophils and lymphocytes may also be jointly regulated through complex mechanisms. Chronic inflammation can stimulate the release of immunoregulatory granulocytic myeloid-derived suppressor cells from the bone marrow, which can increase to 10% of peripheral WBCs and suppress lymphocyte counts and function16,27. High levels of circulating neutrophils are associated with depressed activity of other immune cells such as T-lymphocytes and natural killer cells28,29.
Although higher NLR was associated with increased overall mortality, the overlap of baseline levels for deceased and surviving participants was large. As expected, mortality due to specific conditions tended to occur earlier in individuals with baseline evidence for that disease than in those without such evidence, indicating that early deaths were in large part related to pre-existing conditions. Associations of NLR with short-term mortality for certain conditions may predominantly reflect the effects of heightened inflammation or reduced immunity on progression of those conditions in individuals who had already been diagnosed or who had preclinical disease. In contrast, significant NLR associations with disease mortality in later follow-up still reflects progression but may also be more related to an etiologic role of inflammation or impaired immune function on the development of the disease.
In secondary analyses, we observed associations of NLR with cancer mortality within the first 12 months of follow-up and among individuals who had a history of cancer at baseline. These findings are most consistent with a role of heightened inflammation or depressed adaptive immunity in shaping survival outcomes after a cancer diagnosis, since deaths from cancer in the first year were unlikely to be related to incident diagnoses within such a short interval. Neutrophils may directly suppress antitumor immune responses or secrete tumor growth promoting factors, while tumor-infiltrating lymphocyte play a role in controlling tumor growth and preventing metastases12,30. Although we could not look at mortality related to specific cancers using the public-use NHANES data, previous studies have demonstrated that an elevated NLR is associated with poor survival after diagnosis for a wide range of cancers12,31. Only a few studies have examined cancer mortality or incidence in the general population. One cohort study reported a nonsignificant trend of increased cancer mortality in association with elevated NLR17. Several studies have assessed NLR in relation to lung cancer incidence or mortality in the general population or among high-risk patients, and most32,33,34 but not all35, have found positive associations.
The mechanisms underlying heart and cerebrovascular diseases overlap to some degree, and the similarity of our results for these two conditions support inflammation or reduced immune function contributing to both diseases. Specifically, we found that NLR was associated with both diseases over long intervals of follow-up (i.e., 12–49 and 50–93 months for heart disease, and 94+ months for cerebrovascular disease) and in individuals without these conditions at baseline. Other studies have reported increased cardiovascular or cerebrovascular disease mortality or incidence in the general population among individuals with higher NLR14,15,16,17. One study noted that NLR levels were positively associated with elevated mortality from cardiovascular disease for up to 8 years after baseline measurement17. These results suggest that NLR could reflect inflammatory/immune processes that shape both the development of heart and cerebrovascular diseases and adverse outcomes from these disorders. Neutrophils secrete inflammatory mediators which contribute to degeneration of blood vessel walls, while lymphocytes may act to inhibit atherosclerosis36. NLR has also been associated with progression of atherosclerosis and higher mortality in patients with various cardiovascular diseases37,38.
NLR levels showed associations with increased mortality from chronic lower respiratory disease and kidney disease, with stronger associations observed in secondary analyses among individuals with baseline histories of these conditions. In addition, we observed associations of NLR with these mortality outcomes out to 49 months and 93 months after baseline for chronic lower respiratory disease and kidney disease, respectively. A recent meta-analysis showed a predictive ability of NLR for acute exacerbations in patients with chronic obstructive pulmonary disease39. Similarly, the prognostic value of NLR in kidney disease progression has been reported40,41. Although we did not observe an overall linear trend, high quartiles of NLR (quartiles 2, 3, and 4 vs. 1) had elevated HRs for mortality due to Alzheimer’s disease. Furthermore, NLR showed a positive relationship with mortality from influenza/pneumonia, which may be explained if individuals with elevated NLR levels are predisposed to respond with excessive inflammation or are unable to mount appropriate adaptive immune responses to pulmonary infections. Of interest, recent data indicate that NLR is a strong predictor of mortality among hospitalized patients with novel coronavirus 2019 disease42. Finally, we did not have clinical information with regards to the severity or the extent of the diseases under evaluation, so we could not assess NLR-mortality associations according to clinical status. For example, cancer survivors who had successful resection may have differed in their systemic inflammatory or immune responses from inoperable cancer patients at advance stage.
NHANES is a nationally representative sample of the non-institutionalized US population. The comprehensive assessment of various risk factors in NHANES allowed us to reliably adjust our analyses for potential confounding factors. Furthermore, standardized data and blood collection and laboratory testing strengthen confidence in our results. To our knowledge, this is the first study to systematically investigate associations of NLR with overall mortality and multiple cause-specific mortality outcomes. Nonetheless, our study has several limitations. Although NHANES includes a large sample, the small number of deaths for some causes limits the statistical power. Some mortality outcomes (e.g., cancer-specific mortality) are heterogenous because the underlying diseases are heterogeneous, so that the association of NLR with specific outcomes may not have been captured. We relied on a single measurement of blood counts, and repeated measurements of NLR over time may provide additional information. Finally, mortality reflects both incidence of a disease and survival following diagnosis and treatment. We had data identifying a limited number of people who had diseases of interest at baseline and on the timing of deaths, but because we lacked data on the incidence of disease after baseline, we could not completely distinguish between associations of NLR with incidence and progression.
In conclusion, our study demonstrates that NLR is predictive of mortality in the US general population. Further studies are warranted to understand the relationship of NLR with the incidence of specific diseases as well as outcomes following diagnosis. There is a large range of NLR values and overlap with regards to overall mortality, but NLR may be clinically useful for risk stratification depending on its combination with other information in particular clinical scenarios, and longitudinal measurements may add predictive utility. Studies examining more specific WBC subsets may further increase our understanding of disease etiology and progression.
Data availability
All data used are publicly available at NHANES website.
Code availability
Code can be provided upon request.
References
Furman, D. et al. Chronic inflammation in the etiology of disease across the life span. Nat. Med. 25, 1822–1832. https://doi.org/10.1038/s41591-019-0675-0 (2019).
Grivennikov, S. I., Greten, F. R. & Karin, M. Immunity, inflammation, and cancer. Cell 140, 883–899. https://doi.org/10.1016/j.cell.2010.01.025 (2010).
Hansson, G. K. Inflammation, atherosclerosis, and coronary artery disease. N. Engl. J. Med. 352, 1685–1695. https://doi.org/10.1056/NEJMra043430 (2005).
Faria, S. S. et al. The neutrophil-to-lymphocyte ratio: A narrative review. Ecancermedicalscience 10, 702. https://doi.org/10.3332/ecancer.2016.702 (2016).
Celikbilek, A., Ismailogullari, S. & Zararsiz, G. Neutrophil to lymphocyte ratio predicts poor prognosis in ischemic cerebrovascular disease. J. Clin. Lab. Anal. 28, 27–31. https://doi.org/10.1002/jcla.21639 (2014).
Liu, Y. L. et al. High neutrophil-to-lymphocyte ratio predicts hemorrhagic transformation in acute ischemic stroke patients treated with intravenous thrombolysis. Int. J. Hypertens. 2020, 5980261. https://doi.org/10.1155/2020/5980261 (2020).
Lattanzi, S. et al. Neutrophil-to-lymphocyte ratio in acute cerebral hemorrhage: A system review. Transl. Stroke Res. 10, 137–145. https://doi.org/10.1007/s12975-018-0649-4 (2019).
Lattanzi, S. et al. Neutrophil-to-lymphocyte ratio improves outcome prediction of acute intracerebral hemorrhage. J. Neurol. Sci. 387, 98–102. https://doi.org/10.1016/j.jns.2018.01.038 (2018).
Park, J. S. et al. Importance of prognostic value of neutrophil to lymphocyte ratio in patients with ST-elevation myocardial infarction. Medicine 97, e13471. https://doi.org/10.1097/MD.0000000000013471 (2018).
Tamhane, U. U. et al. Association between admission neutrophil to lymphocyte ratio and outcomes in patients with acute coronary syndrome. Am. J. Cardiol. 102, 653–657. https://doi.org/10.1016/j.amjcard.2008.05.006 (2008).
de Jager, C. P. et al. Lymphocytopenia and neutrophil-lymphocyte count ratio predict bacteremia better than conventional infection markers in an emergency care unit. Crit. Care 14, R192. https://doi.org/10.1186/cc9309 (2010).
Templeton, A. J. et al. Prognostic role of neutrophil-to-lymphocyte ratio in solid tumors: A systematic review and meta-analysis. J. Natl. Cancer Inst. 106, 1. https://doi.org/10.1093/jnci/dju124 (2014).
Ellis, L. et al. Cancer incidence, survival and mortality: Explaining the concepts. Int. J. Cancer 135, 1774–1782. https://doi.org/10.1002/ijc.28990 (2014).
Shah, N. et al. Neutrophil lymphocyte ratio significantly improves the Framingham risk score in prediction of coronary heart disease mortality: Insights from the National Health and Nutrition Examination Survey-III. Int. J. Cardiol. 171, 390–397. https://doi.org/10.1016/j.ijcard.2013.12.019 (2014).
Suh, B. et al. Elevated neutrophil to lymphocyte ratio and ischemic stroke risk in generally healthy adults. PLoS One 12, e0183706. https://doi.org/10.1371/journal.pone.0183706 (2017).
Kim, S., Eliot, M., Koestler, D. C., Wu, W. C. & Kelsey, K. T. Association of neutrophil-to-lymphocyte ratio with mortality and cardiovascular disease in the Jackson Heart Study and modification by the Duffy antigen variant. JAMA Cardiol. 3, 455–462. https://doi.org/10.1001/jamacardio.2018.1042 (2018).
Fest, J. et al. The neutrophil-to-lymphocyte ratio is associated with mortality in the general population: The Rotterdam Study. Eur. J. Epidemiol. 34, 463–470. https://doi.org/10.1007/s10654-018-0472-y (2019).
National Health and Nutrition Examination Survey. https://wwwn.cdc.gov/nchs/nhanes/default.aspx.
National Health and Nutrition Examination Survey Data; U.S.Department of Health and Human Services, Centers for Disease Control and Prevention: Hyattsville, MD, USA. https://www.cdc.gov/nchs/nhanes/index.htm.
Durrleman, S. & Simon, R. Flexible regression models with cubic splines. Stat. Med. 8, 551–561. https://doi.org/10.1002/sim.4780080504 (1989).
NCHS Research Ethics Review Board (ERB) Approval. https://www.cdc.gov/nchs/nhanes/irba98.htm.
Rosales, C. Neutrophil: A cell with many roles in inflammation or several cell types?. Front. Physiol. 9, 113. https://doi.org/10.3389/fphys.2018.00113 (2018).
Mayadas, T. N., Cullere, X. & Lowell, C. A. The multifaceted functions of neutrophils. Annu. Rev. Pathol. 9, 181–218. https://doi.org/10.1146/annurev-pathol-020712-164023 (2014).
Dunn, G. P., Bruce, A. T., Ikeda, H., Old, L. J. & Schreiber, R. D. Cancer immunoediting: From immunosurveillance to tumor escape. Nat. Immunol. 3, 991–998. https://doi.org/10.1038/ni1102-991 (2002).
Mittal, D., Gubin, M. M., Schreiber, R. D. & Smyth, M. J. New insights into cancer immunoediting and its three component phases–elimination, equilibrium and escape. Curr. Opin. Immunol. 27, 16–25. https://doi.org/10.1016/j.coi.2014.01.004 (2014).
Naeim, F., Nagesh Rao, P., Song, S. X. & Grody, W. W. In Atlas of Hematopathology (eds Naeim, F. et al.) 627–633 (Academic Press, New York, 2013).
Su, Z., Ni, P., Zhou, C. & Wang, J. Myeloid-derived suppressor cells in cancers and inflammatory diseases: Angel or demon?. Scand. J. Immunol. 84, 255–261. https://doi.org/10.1111/sji.12473 (2016).
Petrie, H. T., Klassen, L. W. & Kay, H. D. Inhibition of human cytotoxic T lymphocyte activity in vitro by autologous peripheral blood granulocytes. J. Immunol. 134, 230–234 (1985).
el-Hag, A. & Clark, R. A. Immunosuppression by activated human neutrophils. Dependence on the myeloperoxidase system. J. Immunol. 139, 2406–2413 (1987).
Gooden, M. J., de Bock, G. H., Leffers, N., Daemen, T. & Nijman, H. W. The prognostic influence of tumour-infiltrating lymphocytes in cancer: A systematic review with meta-analysis. Br. J. Cancer 105, 93–103. https://doi.org/10.1038/bjc.2011.189 (2011).
Proctor, M. J. et al. A derived neutrophil to lymphocyte ratio predicts survival in patients with cancer. Br. J. Cancer 107, 695–699. https://doi.org/10.1038/bjc.2012.292 (2012).
Grieshober, L. et al. Methylation-derived neutrophil-to-lymphocyte ratio and lung cancer risk in heavy smokers. Cancer Prev. Res. (Phila.) 11, 727–734. https://doi.org/10.1158/1940-6207.CAPR-18-0111 (2018).
Kang, J. et al. Neutrophil-to-lymphocyte ratio and risk of lung cancer mortality in a low-risk population: A cohort study. Int. J. Cancer 145, 3267–3275. https://doi.org/10.1002/ijc.32640 (2019).
Wong, J. Y. Y. et al. White blood cell count and risk of incident lung cancer in the UK Biobank. JNCI Cancer Spectrum 4, 1–9. https://doi.org/10.1093/jncics/pkz102 (2020).
Sanchez-Salcedo, P. et al. The neutrophil to lymphocyte and platelet to lymphocyte ratios as biomarkers for lung cancer development. Lung Cancer 97, 28–34. https://doi.org/10.1016/j.lungcan.2016.04.010 (2016).
Angkananard, T., Anothaisintawee, T., McEvoy, M., Attia, J. & Thakkinstian, A. Neutrophil lymphocyte ratio and cardiovascular disease risk: A systematic review and meta-analysis. Biomed. Res. Int. 2018, 2703518. https://doi.org/10.1155/2018/2703518 (2018).
Kalay, N. et al. Hematologic parameters and angiographic progression of coronary atherosclerosis. Angiology 63, 213–217. https://doi.org/10.1177/0003319711412763 (2012).
Bhat, T. et al. Neutrophil to lymphocyte ratio and cardiovascular diseases: A review. Expert Rev. Cardiovasc. Ther. 11, 55–59. https://doi.org/10.1586/erc.12.159 (2013).
Ye, Z., Ai, X., Liao, Z., You, C. & Cheng, Y. The prognostic values of neutrophil to lymphocyte ratio for outcomes in chronic obstructive pulmonary disease. Medicine 98, e16371. https://doi.org/10.1097/MD.0000000000016371 (2019).
Yoshitomi, R. et al. High neutrophil/lymphocyte ratio is associated with poor renal outcomes in Japanese patients with chronic kidney disease. Renal. Fail. 41, 238–243. https://doi.org/10.1080/0886022X.2019.1595645 (2019).
Tonyali, S., Ceylan, C., Yahsi, S. & Karakan, M. S. Does neutrophil to lymphocyte ratio demonstrate deterioration in renal function?. Renal. Fail. 40, 209–212. https://doi.org/10.1080/0886022X.2018.1455590 (2018).
Liu, Y. et al. Neutrophil-to-lymphocyte ratio as an independent risk factor for mortality in hospitalized patients with COVID-19. J. Infect. https://doi.org/10.1016/j.jinf.2020.04.002 (2020).
Funding
The study was supported by the Intramural Research Program of the National Cancer Institute.
Author information
Authors and Affiliations
Contributions
M.S. and E.A.E. conceptualized the study. M.S. carried out all analysis and drafted the manuscript. B.I.G., C.S.R. and E.A.E. commented on the manuscript. All authors have read and approved the final version.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Song, M., Graubard, B.I., Rabkin, C.S. et al. Neutrophil-to-lymphocyte ratio and mortality in the United States general population. Sci Rep 11, 464 (2021). https://doi.org/10.1038/s41598-020-79431-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-020-79431-7
This article is cited by
-
The neutrophil-to-lymphocyte ratio is associated with all-cause and cardiovascular mortality among individuals with hypertension
Cardiovascular Diabetology (2024)
-
Clinical courses and outcomes of COVID-19 associated pulmonary aspergillosis in 168 patients with the SARS-CoV-2 omicron variant
BMC Infectious Diseases (2024)
-
Predicting sepsis in-hospital mortality with machine learning: a multi-center study using clinical and inflammatory biomarkers
European Journal of Medical Research (2024)
-
Exploring the relations of NLR, hsCRP and MCP-1 with type 2 diabetic kidney disease: a cross-sectional study
Scientific Reports (2024)
-
A simple tool for evaluation of inflammation in psoriasis: Neutrophil-to-lymphocyte and platelet-to-lymphocyte ratio as markers in psoriasis patients and related murine models of psoriasis-like skin disease
Journal of Molecular Medicine (2024)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
