
Abstract
Early dietary exposure may influence infant appetitive feeding behaviour, and therefore their later health. Maternal diabetes in pregnancy is associated with an increased risk of obesity in the offspring. We, therefore, examined third-trimester dietary patterns of women with gestational diabetes, their offspring’s appetitive feeding behaviour at 6 months of age, and relationships between these. We used data from a prospective cohort of women with gestational diabetes and assessed maternal dietary patterns at 36 weeks’ gestation using principal component analysis; infant appetitive feeding behaviour at 6 months of age using the Baby Eating Behaviour Questionnaire; and relationships between these using general linear modelling and chi-square tests. In 325 mother-infant dyads, we identified three distinct maternal dietary patterns: ‘Junk,’ ‘Mixed,’ and ‘Health-conscious.’ The maternal ‘Health-conscious’ pattern was inversely associated with ‘enjoyment of food’ in their sons (β − 0.24, 95% CI − 0.36 to − 0.11, p = 0.0003), but not daughters (β − 0.02, 95% CI − 0.12 to 0.08, p = 0.70), and was positively associated with ‘slowness in eating,’ (β 0.13, 95% CI 0.02 to 0.24, p = 0.01). Third-trimester dietary patterns in women with gestational diabetes may have sex-specific effects on infant appetitive feeding behaviour at 6 months of age.
Similar content being viewed by others

Introduction
A healthy appetite is important for an infant’s optimal growth and long-term health. Appetite is defined as “the internal driving force for search, choice, and ingestion of food”1, and growing evidence suggests that maternal diet in the prenatal and early postnatal period may alter an infants’ appetitive feeding behaviour via a panoply of hormones, genes, and mechanisms including orosensory controls2. Flavour, a major determinant of food preference, is essential in the development of infant appetitive feeding behaviour3,4. It is thought that the developing fetus is first exposed to flavour in utero via maternal dietary components in the amniotic fluid5,6,7 and that the initial exposure may mould future dietary proclivities. For instance, infants of mothers who ate a variety of foods during pregnancy and breastfeeding are reported to be more tolerant of a wide array of flavours compared to their formula-fed counterparts8. Similarly, a cohort study in the UK has reported significant associations between maternal protein and fat intake at 32 weeks of gestation and the offspring’s protein and fat intake at 10 years of age9.
Animal studies support these findings and have shown that alterations in the nutritional environment during gestation may program appetite and the feeding behaviour of the offspring10,11,12,13 Appetite is thought to be regulated by neurobiological processes involving the homeostatic and hedonic systems14. While the homeostatic system boosts eating to satisfy energy needs, hedonic systems are mediated by the associated reward, e.g., palatability of the food, which can encourage eating even beyond energy needs15. The hypothalamus is critical to the optimal functioning of these systems, and alterations in the nutritional environment during critical periods of growth may alter the development of the hypothalamus with a risk for later adverse health consequences16. For example, in rats, high-fat feeding from pre-conception through lactation alters hypothalamic gene expression in the offspring, which may lead to abnormal formation of neuronal projections and the neuronal circuitry controlling appetite in later life10,17. It is also interesting to note that in animals and humans maternal diet in pregnancy, e.g., high fat diet has been shown to play a role in the early colonization of the offspring’s gut18,19. The altered microbiome may then produce metabolites which may epigenetically modify key genes involved in the regulation of the offspring’s appetite20,21,22,23.
Infant appetitive feeding behaviour includes traits such as food responsiveness, slowness in eating, and satiety responsiveness, which contribute to variations in adiposity and weight gain in infants24,25. For instance, food responsiveness measured at 3 months of age is significantly associated with higher BMI z-scores from 6 to 15 months of age and higher weight gain between 3 and 6 months of age26. In contrast, slowness in eating and satiety responsiveness is significantly associated with lower BMI z-scores at 6 months and with less weight gain between 3 and 6 months of age27. Associations between adiposity, satiety responsiveness, and food responsiveness have also been reported among groups of children aged between 3 to 5 and 8 to 11 years28.
Although there is some evidence that maternal diet affects infant appetitive feeding behaviour, the effects are inconsistent, and it is unclear when abnormalities in appetitive traits begin to manifest and to what extent they persist2. Women with gestational diabetes mellitus (GDM) are commonly overweight, at increased risk of developing type 2 diabetes and hypertensive disorders, and have large babies who are also at a higher risk of obesity and metabolic disease in later life29,30. However, we are not aware of any studies that have examined maternal dietary patterns in women with GDM and their relationship with appetitive traits of their offspring. Thus, our study aimed to investigate dietary patterns of women with GDM in late pregnancy, appetitive feeding behaviour in their infants, and the relationship between these. We hypothesised that (1) infants of women with GDM would have obesity-related appetitive traits such as high food responsiveness and high enjoyment of food; (2) unhealthy maternal dietary patterns, high in energy-dense, nutrient-poor discretionary foods, would be associated with higher food responsiveness, enjoyment of food and higher general appetite in infants; and (3) healthy maternal dietary patterns, high in nutrient-dense foods such as fruits and vegetables, would be associated with higher satiety responsiveness and slowness in eating in infants.
Results
Sample characteristics
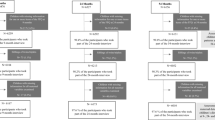
Of the 339 women with dietary data at 36 weeks’ gestation, 8 women with 10 or more dietary items missing, and 6 with implausible energy values were excluded. A final sample of 325 mothers were included in the dietary pattern analyses. Women in the cohort were similar to, i.e., fell within the 95% confidence intervals for, all women who gave birth in New Zealand in 2017 for parity and socioeconomic status, but were slightly older, more likely to be overweight or obese, had an overrepresentation of Asian and underrepresentation of Māori ethnicities, and were less likely to smoke (Table 1).
Of the 325 mothers with dietary data, 247 (76%) completed the infant appetitive feeding behaviour questionnaire. Those who completed the questionnaire were more likely to be of Asian and New Zealand European ethnicities, and to be in the lower socioeconomically deprived quintiles compared with those who did not (Table 1).
At 6 months of age, 35 (14.2%) infants were exclusively breastfed, 152 (61.5%) were predominantly/partially breastfed, while 60 (24.3%) were exclusively formula-fed. The mean age at start of solids was 5.1 (SD 0.72) months.
Overall, ‘enjoyment of food’ for infants in this cohort was negatively skewed. The majority of infants (92.3%) were reported to have high (scores > 3.66 to 5) enjoyment of their milk and feeding times, 54.5% had a high general appetite, and 4.9% had high food responsiveness. Infants who had higher scores for ‘food responsiveness’ had higher general appetite (r = 0.44, p < 0.0001), and higher scores for ‘slowness in eating’ (r = 0.21, p < 0.0008). In contrast, infants who had higher scores for ‘enjoyment of food’ had lower scores for ‘satiety responsiveness’ (r = − 0.22, p < 0.0006) and ‘slowness in eating’ (r = − 0.22, p < 0.0006) (Table 2).
Boys and girls had similar appetitive mean scores and showed a fair to moderate correlation between general appetite, food responsiveness to cues of feeding, and enjoyment of milk and feeding time. In girls but not boys, there was a negative relationship between satiety responsiveness and both food responsiveness and general appetite (Table 2).
Maternal dietary pattern analysis
Using the 57 food items in the semi-quantitative FFQ (food frequency questionnaire) (supplementary Table S1), the principal component analysis (PCA) showed a correlation matrix with correlation coefficients mostly below r < 0.6, a KMO of 0.75, and Bartlett’s sphericity test of < 0.0001. We obtained 19 components with eigenvalues greater than 1 but retained three components based on the inflection point in the scree plot (Fig. 1), and the ease of interpretability of the components (Table 3). The three components explained 28.3% of the total variation in food intake and were labelled: component 1 ‘Junk’—loaded heavily on sweets, sweet drink, pizza, hot chips, potato chips, cake, chocolate, pancake, meat pie, white bread, ice cream, salami, other pasta, alcoholic beverages, jams, international takeaway, low caloric drink, biscuit, sausages, and cream based dairy; component 2 ‘Mixed’ loaded on other root vegetables, cheese, other vegetables, fats, potatoes, kumara, pumpkin, other greens, salad greens, oils, crackers, nuts, water, tomatoes, wholemeal, yoghurt, onions, iodized salt, tea/coffee, beef/pork/lamb, chicken/poultry, and dried fruit; and component 3 ‘Health-conscious’—loaded on high fibre cereals, brown rice, citrus fruits, tuna/salmon, beans/legumes, other fruits, other fish/seafood, other cold breakfast cereals, bananas, apple/pears, fried fish, eggs, and low-fat cheese (Fig. 2). Cronbach’s coefficient α values (95% CI) showed good internal consistency: Junk 0.63 (0.57, 0.69); Mixed 0.81 (0.79, 0.84) and Health-conscious 0.75 (0.71, 0.79). Cronbach’s coefficient α values did not improve after removing cream-based dairy and alcoholic beverages in the Junk pattern (0.63–0.64), and tea/coffee in the mixed pattern (0.81–0.81).

Scree plot for principal component analysis of maternal diet.

Food loadings for the three maternal dietary patterns identified.
Associations between maternal dietary patterns and infant appetitive traits
In the unadjusted analyses, for each standard deviation increase in the maternal ‘Health-conscious’ dietary pattern, there was a decrease of 0.09 in the infant ‘enjoyment of food’ score. In multivariable regression analyses using the parsimonious model and adjusting for sex, weight-for-age z score at 6 months and NZDep (New Zealand Deprivation index) at study entry, increasing scores in the ‘Health-conscious’ maternal dietary pattern was associated with decreased scores on ‘enjoyment of food’ in boys (β − 0.24, 95% CI − 0.36 to − 0.11, p = 0.0003) but not in girls (β − 0.02, 95% CI − 0.12 to 0.08, p = 0.70, p = 0.004 for interaction). Independent and positive associations were also noted between the ‘Health-conscious’ pattern and ‘slowness in eating’ (β 0.13, 95% CI 0.016 to 0.24; p = 0.025). No other associations approached statistical significance (Table 4).
Discussion
In a cohort of 325 women with GDM in New Zealand, we identified three distinct maternal dietary patterns, labelled as ‘Junk,’ ‘Mixed,’ and ‘Health-conscious’, that explained the most variation in food intake assessed at 36 weeks’ gestation. We found, as hypothesised, that the majority of infants in our cohort had a high enjoyment of food score, although fewer than 5% had high food responsiveness. Additionally, we found that overall, the ‘health-conscious’ maternal dietary pattern was inversely associated with ‘enjoyment of food’ in boys but not in girls, and positively associated with ‘slowness in eating’ at 6 months of age.
Several animal studies have examined the effect of maternal diet on feeding behaviour31,32 and neurobiological processes33,34,35 controlling appetite in the offspring. However, to the best of our knowledge, this is the first study to assess the effect of third-trimester diet in women with GDM on a questionnaire-based assessment, i.e., the Baby Eating Behaviour questionnaire (BEBQ) of infant appetitive feeding behaviour at 6 months of age. Our results suggest that a ‘Health-conscious’ maternal dietary pattern is associated with better appetitive control in infants at 6 months of age. Appetitive traits influence an infant’s weight gain36. In particular, while enjoyment of food is positively associated with a higher risk of overweight in childhood37,38, slowness in eating is negatively associated38. Therefore, our findings suggest that a ‘Health-conscious’ dietary pattern in women with GDM may potentially decrease the risk of later overweight/obesity of their offspring, particularly in boys39,40.
The reason for these sex-specific associations is unclear. Sex differences are reported in the prevalence of obesity, with boys at a higher risk across all age groups41. Additionally, it has been reported in some studies that children eat fewer fruits, vegetables, and whole grains than recommended42, and boys are reported to have higher preferences for meat, fish, poultry, and high-fat foods compared to girls who have a higher liking for fruits and vegetables43,44,45. It would be interesting, therefore, to determine whether the maternal health-conscious dietary pattern predicts later dietary preferences, and particularly in boys.
Our findings provide new information about the dietary patterns of women with GDM in late pregnancy. Diet is the cornerstone in the management of women with GDM, yet few studies46,47 have examined maternal dietary patterns in these women. A cohort study conducted in South Korea assessed dietary patterns via factor analysis using a 3-day food record, although the timing of dietary data collection was unclear47. Among the 166 women with GDM two dietary patterns were identified: a “carbohydrate and vegetable pattern” with high loadings of fruits, rice and cereals, fermented vegetables, vegetables, and meat and a “western pattern” characterized by poultry and eggs, fast food, deep-fried food, processed meat and seafood, snacks and desserts, coffee and other beverages, and seaweeds47. While there are similarities between the ‘carbohydrate and vegetable pattern’ and ‘western pattern’ and our ‘Mixed’ and ‘Junk’ patterns, respectively, some diversity is to be expected from the differences across cultures and methodologies. A recent longitudinal cohort study assessed differences in dietary patterns between 280 women with GDM and 5104 without GDM in New Zealand from already established dietary patterns among the cohort46,48. The authors reported four dietary patterns via PCA and using FFQ in the third trimester of pregnancy: ‘Junk,’ ‘Traditional/White bread,’ ‘Fusion Protein’ and ‘Health conscious’46,48. Their dietary patterns were comparable to the patterns defined in our study, supporting generalisability of the patterns among women with GDM in New Zealand.
The three dietary patterns identified in our study explained only 23.8% of the variation in food intake, which could be interpreted as indicating insufficient summarising of the dietary data or possibly that other unidentified phenomena may be present. However, while the regrouping of a large number of different food items, e.g., apples, pears, etc. from the FFQ into a single fruit group markedly improved the percentage of variability explained in our analyses, there was an inevitable trade-off in loss of detail. Thus, we chose not to regroup to reduce the food items as greater detail is reported to improve the precision by which dietary patterns estimate disease risk49. Additionally, the total percent of variance explained by the dietary patterns in our study is consistent with similar studies conducted among pregnant50,51 and non-pregnant women52 in New Zealand, where the percentage of variance explained was 13.8–25%.
This study has several strengths. Firstly, we used a standardised and validated psychometric measure, the BEBQ, to quantify appetitive traits in the infants and a FFQ that was adapted to be culturally appropriate for New Zealand. Secondly, the dietary patterns identified showed good internal consistency, which supports the reliability of the Likert-type scales used in the FFQ. Thirdly, we employed a prospective study design and began follow-up of the infants early postpartum, which will permit further analyses of changes in appetitive behaviour into adulthood in the future.
Women in our study cohort may not be representative of the GDM population in New Zealand, as responders differed from non-responders in ethnicity and socioeconomic status. Other limitations lie in methodologies used in collecting and analysing the maternal dietary and infant appetitive feeding behaviour data. Although the conduct and analysis of food diaries in large trials such as TARGET are deemed cost-prohibitive and time consuming compared to FFQs, food diaries involve real-time documentation of food consumption. Our sole reliance on maternal self-report of dietary intake and infant feeding behaviour, as opposed to observed measures of data collection, may have introduced recall and social desirability bias53,54,55. However, the FFQ we used was shown to have acceptable to good validity when compared to the 8-day dietary record56, and dietary patterns derived from PCA and food records are reported to be similar57,58,59. Additionally, PCA is inherently subjective, with a tendency towards interpretation bias60,61. However, given the similarities between our study dietary patterns and a prior study46, the likelihood of interpretation bias in this study appears low. Also, although we adjusted extensively for potential confounding factors, we cannot rule out the possibility of residual confounding.
This exploratory study provides new insights into the relationships between maternal dietary patterns in women with GDM, and the possible impact of maternal diet during pregnancy on the appetitive feeding behaviour of their infants. Although the ‘Health-conscious’ maternal dietary pattern was related to appetitive feeding behaviours in boys that might be expected to result in decreased obesity risk, it is not known whether these relationships persist, or have any relationship with later growth. Further assessment of these infants as they grow older, are introduced to diverse foods, and transition to independent feeding may help to ascertain long-term health implications.
Conclusion
Appetitive control in infants at high risk of later obesity may be affected by maternal dietary patterns during late pregnancy. We found evidence that among women with GDM, the ‘Health-conscious’ maternal dietary pattern in the third trimester of pregnancy is associated with better appetitive control, particularly in boys, at 6 months of age. Since the risk of obesity is increased in the offspring of women with GDM, appropriate dietary advice in pregnancy may be a potential target for intervention and public health recommendations.
Methods
Study design and setting
This nested cohort study is a secondary analysis of data from the TARGET Trial, a multicentre, stepped-wedge, randomised trial that compared the effects of tighter treatment targets for glycaemic control in women with GDM with less tight targets on maternal and infant outcomes62. Details of the trial protocol are described elsewhere62. Briefly, women with a singleton pregnancy and diagnosed with GDM by an oral glucose tolerance test ≥ 22 weeks’ gestation were recruited from 10 hospitals in New Zealand between 2015 and 2017. The TARGET trial was approved by the Northern A Health and Disability Ethics Committee (14/NTA/163/AMO1). Participants gave written informed consent. TARGET was registered with the Australian New Zealand Clinical Trials Registry—ACTRN 12615000282583. No additional consent was required for the current study using anonymised data from the TARGET Trial, but the study was carried out in accordance with the principles of the Declaration of Helsinki and the University of Auckland Research Code of Conduct.
Participants
Women with GDM who were recruited to the TARGET Trial were included in this nested study with their infants if they had completed a food frequency questionnaire at 36 weeks’ gestation about their diet during the trial; had data on infant sex, gestational age at birth, and pregnancy outcomes; and had participated in the follow-up at 6-months after birth.
Outcomes and measures
Maternal diet
Data on food consumption was collected from study participants via a self-administered, 1-month recall, FFQ at 36 weeks’ gestation. The FFQ was a customized version of the 163-item semi-quantitative FFQ developed by Willett63, with changes made to reflect local dietary habits as per the nationally-representative nutrition survey available at the time64, and further informed by two focus groups of 21 adults aged 30–59 years in New Zealand56. The questionnaire comprised 65 questions, of which 57 were grouped as dairy, eggs and meat, fish and seafood, bread, cereals and starches, fruits, vegetables, fast foods, beverages, sweets, baked goods, and miscellaneous (Supplementary Table S1). Food frequencies were measured on a six-point ordinal scale ranging from “never or less than once per month” to “4–6 times per day”56.
We excluded data from women with more than ten dietary items missing and assumed an item was never consumed for missing data where ten or fewer items were missing65. We also excluded implausible data with reported energy intakes < 500 and > 3500 kcal/day66.
Dietary patterns
Of the 65 food questions in the semi-quantitative FFQ, we used 57 to conduct the PCA, excluding items which were intended for cross-validation and items that were not food group based (Supplementary Table S1). We converted the ordinal maternal dietary data to weekly frequencies of food consumption as follows: never or less than a month = 0, 1–3/month = 0.5, 1/week = 1, 2–4/week = 3, 5–6/week = 5.5, 1/day = 7.0, 2–3/day = 17.5, 4–6/day = 35. To obtain a smaller set of variables that explained maximum variations in the dietary patterns of women with GDM, we performed PCA using the polychoric correlation matrix, which is more appropriate for ordinal data from Likert-type rating scales, and varimax rotation67. We used the PROC FACTOR, method = principal statement in SAS68, and assessed the suitability of the maternal dietary data for PCA via the correlation matrix, Kaiser–Meyer–Olkin (KMO) measure of sampling adequacy, and Bartlett’s sphericity test. KMO values range between 0 and 1, and values closer to 1 affirm the suitability of the data for PCA, while values < 0.50 are unacceptable69,70. We considered Bartlett’s p value less than 0.05 as acceptable and indicating a significant difference between the observed correlation matrix and the identity matrix71. We also assessed the reliability of the Likert-type scales used in the FFQ by evaluating the internal consistency of food items in each identified dietary pattern via Cronbach’s coefficient alpha (α). We considered Cronbach's coefficient α values ≥ 0.70 as good72 and removed food items with poor item-total correlations while assessing the effect of the removal on the reliability of the scale60. We used eigenvalues > 1, the breakpoint in the scree plot, and the interpretability of the components after varimax rotation to determine the number of components to retain73,74,75. We used food items with absolute loading values of ≥ 0.3 to characterise the identified dietary patterns. We calculated weighted component scores as standardised variables and divided subjects into tertiles based on their scores for further analyses. Higher factor scores indicated the degree to which a woman’s diet adhered to the identified dietary pattern72.
Infant feeding practice
Data on infant breastfeeding status and age of introduction of solid food were collected from mothers at 6 months postpartum by questionnaire. We defined exclusively breastfed infants as having received only breast milk and no other liquids or solid foods, except for prescribed medicines, and predominantly breastfed infants as having received breast milk together with other liquids76,77.
Infant feeding behaviour
Data were collected from mothers at 6-months postpartum via a self-administered infant feeding behaviour questionnaire, based on the BEBQ78. The BEBQ was adapted from the validated Children’s Eating Behaviour Questionnaire and modified for use in infants during the exclusive milk-feeding stage79. The BEBQ consists of 18 items developed to measure general appetite and four specific appetitive traits: ‘enjoyment of food’ (4 items), ‘food responsiveness’ (6 items), ‘slowness in eating’ (4 items), and ‘satiety responsiveness’ (3 items) (Supplementary Table S2). We measured general appetite with the question, ‘my baby had a big appetite’ and recorded maternal responses on a 5 point Likert frequency scale with response options of: ‘never,’ ‘rarely,’ ‘sometimes,’ ‘often,’ and ‘always.’ We reverse-scored two items, i.e., “my baby became distressed while feeding” and “my baby finished feeding quickly,” calculated mean scores for each appetitive trait, and grouped appetitive scores as low (1 to ≤ 2.33), medium (> 2.33 to ≤ 3.66), and high (> 3.66 to 5)80, with high scores indicating higher traits.
Covariates
We considered the following covariates for each appetitive variable: continuous—maternal age and total daily energy intake, infant gestational age at birth, birth weight, weight and weight-for-length z scores at 6 months and age at introduction of solids; categorical—prioritised ethnicity (European; Māori; Pacific Peoples; Asian; and Other), and BMI (underweight < 18.5 kg/m2, normal weight 18.5–24.9 kg/m2, overweight ≥ 25 − 29.9 kg/m2, and obese ≥ 30 kg/m2)81; smoking (current smokers vs. non-smokers), parity (primiparous vs. multiparous),TARGET Trial treatment group (tighter vs. less tight glycaemic control), and infant breastfeeding status (exclusively breastfed, predominantly breastfed or formula-fed up to 6 months).
Variable selection was done on the basis of parsimony and biological plausibility after inspection of models fitted to each appetitive variable using a stepwise, Max R square, forward and backward selection. .
NZDep reflects average degrees of socioeconomic deprivation at the mesh block level, using nine variables (income, employment, communication, transport, support, qualification, owned home, and living space) combined from the 2013 census to reflect eight dimensions of deprivation82,83. We divided the NZDep into quintiles with the first quintile representing the least deprived 20%, and the fifth quintile the most deprived 20%. We calculated total daily energy intake from the maternal FFQ data, while all other maternal covariates were assessed via trial entry questionnaires.
Statistical analysis
We conducted the data analyses using SAS version 9.4 (SAS Institute Inc., Cary, NC, USA). We assessed cohort characteristics, compared mother–child dyads with and without infant appetitive feeding data, and maternal reports of their infant’s appetitive traits via means and standard deviations for continuous variables, median (inter-quartile range) for skewed data, and proportions with their respective percentages for categorical variables. We also assessed the normality of the data and relationships between the BEBQ subscales, using Pearson’s product-moment correlation for normal data or Spearman correlation for skewed data. We interpreted correlation coefficients > 0.80–1.00 as strong, > 0.50–0.80 as moderate, > 0.20–0.50 as fair to weak, and 0.00–0.20 as negligible72.
We assessed relationships between maternal dietary pattern scores at 36 weeks’ gestation (independent variable) and BEBQ subscale scores (dependent variable) at 6 months of age using general linear models and adjusting for variables found to be associated with infant appetitive traits including infant sex, gestational age, birth weight, weight-for-age, weight-for-length, z-scores at 6 months of age, and the maternal covariates previously listed43,84,85. In addition to the overall models, we conducted the analyses separately for infants of each sex and examined plots of residuals for evidence of normality, homoscedasticity, the constancy of variance and outliers. Where residuals of dependent variables were not normally distributed, we explored Box-Cox power transformations to improve the curvilinearity.
Data availability
Published data are available to approved researchers under the data sharing arrangements provided by the Maternal and Perinatal Central Coordinating Research Hub (CCRH), based at the Liggins Institute, University of Auckland (https://wiki.auckland.ac.nz/researchhub). Metadata, along with instructions for data access, are available at the University of Auckland’s research data repository, Figshare (https://auckland.figshare.com). Data access requests are to be submitted to Data Access Committee via researchhub@auckland.ac.nz. Data will be shared with researchers who provide a methodologically sound proposal and have appropriate ethical and institutional approval. Researchers must sign and adhere to the Data Access Agreement that includes a commitment to using the data only for the specified proposal, to store data securely and to destroy or return the data after completion of the project. The CCRH reserves the right to charge a fee to cover the costs of making data available, if required.
References
de Graaf, C., Blom, W. A. M., Smeets, P. A. M., Stafleu, A. & Hendriks, H. F. J. Biomarkers of satiation and satiety. Am. J. Clin. Nutr. 79, 946–961 (2004).
Zeltser, L. M. Feeding circuit development and early life influences on future feeding behavior. Nat. Rev. Neurosci. 19, 302–316 (2018).
Fildes, A. et al. The relationship between appetite and food preferences in British and Australian children. Int. J. Behav. Nutr. Phys. Act 12, 116 (2015).
Freitas, A., Albuquerque, G., Silva, C. & Oliveira, A. Appetite-related eating behaviours: an overview of assessment methods, determinants and effects on children’s weight. Ann. Nutr. Metab. 73, 19–29 (2018).
Burgess-Champoux, T., Marquart, L., Vickers, Z. & Reicks, M. Perceptions of children, parents, and teachers regarding whole-grain foods, and implications for a school-based intervention. J. Nutr. Educ. Behav. 38, 230–237 (2006).
Dominguez, P. R. Development and acquisition of flavor and food preferences in children: an update until 2010. J. Food Res. 3, 1 (2013).
Uwaezuoke, S. N. Food preference in toddlers: is it influenced by prenatal maternal diet?. J. Pregnancy Child Health 02, 2 (2015).
Beauchamp, G. K. & Mennella, J. A. Flavor perception in human infants: development and functional significance. Digestion 83(Suppl 1), 1–6 (2011).
Brion, M.-J.A. et al. Maternal macronutrient and energy intakes in pregnancy and offspring intake at 10 y: exploring parental comparisons and prenatal effects. Am. J. Clin. Nutr. 91, 748–756 (2010).
Morris, M. J. & Chen, H. Established maternal obesity in the rat reprograms hypothalamic appetite regulators and leptin signaling at birth. Int. J. Obes. 33, 115–122 (2009).
Muhlhausler, B. S., Adam, C. L., Findlay, P. A., Duffield, J. A. & McMillen, I. C. Increased maternal nutrition alters development of the appetite-regulating network in the brain. FASEB J. 20, 1257–1259 (2006).
Kirk, S. L. et al. Maternal obesity induced by diet in rats permanently influences central processes regulating food intake in offspring. PLoS ONE 4, e5870 (2009).
Mühlhäusler, B. S. Programming of the appetite-regulating neural network: a link between maternal over-nutrition and the programming of obesity?. J. Neuroendocrinol. 19, 67–72 (2007).
Boswell, N., Byrne, R. & Davies, P. S. W. Aetiology of eating behaviours: a possible mechanism to understand obesity development in early childhood. Neurosci. Biobehav. Rev. 95, 438–448 (2018).
Lutter, M. & Nestler, E. J. Homeostatic and hedonic signals interact in the regulation of food intake. J. Nutr. 139, 629–632 (2009).
Bouret, S. G. Nutritional programming of hypothalamic development: critical periods and windows of opportunity. Int. J. Obes. Suppl. 2, S19–S24 (2012).
Barrand, S., Crowley, T. M., Wood-Bradley, R. J., De Jong, K. A. & Armitage, J. A. Impact of maternal high fat diet on hypothalamic transcriptome in neonatal Sprague Dawley rats. PLoS ONE 12, e0189492 (2017).
Ma, J. et al. High-fat maternal diet during pregnancy persistently alters the offspring microbiome in a primate model. Nat. Commun. 5, 3889 (2014).
Chu, D. M. et al. The early infant gut microbiome varies in association with a maternal high-fat diet. Genome Med. 8, 77 (2016).
Norris, V., Molina, F. & Gewirtz, A. T. Hypothesis: bacteria control host appetites. J. Bacteriol. 195, 411–416 (2013).
van de Wouw, M., Schellekens, H., Dinan, T. G. & Cryan, J. F. Microbiota-gut-brain axis: modulator of host metabolism and appetite. J. Nutr. 147, 727–745 (2017).
Fetissov, S. O. Role of the gut microbiota in host appetite control: bacterial growth to animal feeding behaviour. Nat. Rev. Endocrinol. 13, 11–25 (2017).
Vuong, H. E. et al. The maternal microbiome modulates fetal neurodevelopment in mice. Nature 586, 281–286 (2020).
DiSantis, K. I., Collins, B. N., Fisher, J. O. & Davey, A. Do infants fed directly from the breast have improved appetite regulation and slower growth during early childhood compared with infants fed from a bottle?. Int. J. Behav. Nutr. Phys. Act 8, 89 (2011).
Hurley, K. M., Cross, M. B. & Hughes, S. O. A systematic review of responsive feeding and child obesity in high-income countries. J. Nutr. 141, 495–501 (2011).
Quah, P. L. et al. Prospective associations of appetitive traits at 3 and 12 months of age with body mass index and weight gain in the first 2 years of life. BMC Pediatr. 15, 153 (2015).
Quah, P. L. et al. Prospective associations of appetitive traits at 3 and 12 months of age with body mass index and weight gain in the first 2 years of life. BMC Pediatr. 15, 153 (2015).
Carnell, S. & Wardle, J. Appetite and adiposity in children: evidence for a behavioral susceptibility theory of obesity. Am. J. Clin. Nutr. 88, 22–29 (2008).
Prakash, G. T., Das, A. K., Habeebullah, S., Bhat, V. & Shamanna, S. B. Maternal and neonatal outcome in mothers with gestational diabetes mellitus. Indian J. Endocrinol. Metab. 21, 854–858 (2017).
Daly, B. et al. Increased risk of ischemic heart disease, hypertension, and type 2 diabetes in women with previous gestational diabetes mellitus, a target group in general practice for preventive interventions: a population-based cohort study. PLoS Med. 15, e1002488 (2018).
Bellinger, L., Lilley, C. & Langley-Evans, S. C. Prenatal exposure to a maternal low-protein diet programmes a preference for high-fat foods in the young adult rat. Br. J. Nutr. 92, 513–520 (2004).
da Silva, A. A. M. et al. Perinatal undernutrition stimulates seeking food reward. Int. J. Dev. Neurosci. Off. J. Int. Soc. Dev. Neurosci. 31, 334–341 (2013).
Thanos, P. K. et al. Suboptimal maternal diets alter mu opioid receptor and dopamine type 1 receptor binding but exert no effect on dopamine transporters in the offspring brain. Int. J. Dev. Neurosci. Off. J. Int. Soc. Dev. Neurosci. 64, 21–28 (2018).
Laureano, D. P. et al. Intrauterine growth restriction modifies the hedonic response to sweet taste in newborn pups—role of the accumbal μ-opioid receptors. Neuroscience 322, 500–508 (2016).
de Melo Martimiano, P. H. et al. Perinatal malnutrition stimulates motivation through reward and enhances drd1a receptor expression in the ventral striatum of adult mice. Pharmacol. Biochem. Behav. 134, 106–114 (2015).
Russell, C. & Russell, A. Biological and psychosocial processes in the development of children’s appetitive traits: insights from developmental theory and research. Nutrients 10, 692 (2018).
Carnell, S. & Wardle, J. Measuring behavioural susceptibility to obesity: validation of the child eating behaviour questionnaire. Appetite 48, 104–113 (2007).
Webber, L., Hill, C., Saxton, J., Van Jaarsveld, C. H. M. & Wardle, J. Eating behaviour and weight in children. Int. J. Obes. 2005(33), 21–28 (2009).
Fletcher, S., Wright, C., Jones, A., Parkinson, K. & Adamson, A. Tracking of toddler fruit and vegetable preferences to intake and adiposity later in childhood. Matern. Child Nutr. 13, e12290 (2017).
Dalrymple, K. V. et al. Associations between dietary patterns, eating behaviours, and body composition and adiposity in 3-year-old children of mothers with obesity. Pediatr. Obes. 15, e12608 (2020).
Ogden, C. L., Carroll, M. D., Kit, B. K. & Flegal, K. M. Prevalence of obesity and trends in body mass index among US children and adolescents, 1999–2010. JAMA 307, 483–490 (2012).
Rush, E., Savila, F., Jalili-Moghaddam, S. & Amoah, I. Vegetables: New Zealand children are not eating enough. Front. Nutr. 5, 134 (2019).
Cooke, L. J. & Wardle, J. Age and gender differences in children’s food preferences. Br. J. Nutr. 93, 741–746 (2005).
Caine-Bish, N. & Scheule, B. Gender differences in food preferences of school-aged children and adolescents. J. Sch. Health 79, 532–540 (2009).
Rodenburg, G., Oenema, A., Pasma, M., Kremers, S. P. J. & van de Mheen, D. Clustering of food and activity preferences in primary school children. Appetite 60, 123–132 (2013).
Lawrence, R. L., Wall, C. R. & Bloomfield, F. H. Dietary patterns and dietary adaptations in women with and without gestational diabetes: evidence from the Growing Up in New Zealand study. Nutrients 12, 227 (2020).
Shin, M.-K., Kim, Y.-S., Kim, J.-H., Kim, S.-H. & Kim, Y. Dietary patterns and their associations with the diet quality index-international (DQI-I) in Korean women with gestational diabetes mellitus. Clin. Nutr. Res. 4, 216–224 (2015).
Wall, C. R. et al. Dietary patterns in pregnancy in New Zealand-influence of maternal socio-demographic, health and lifestyle factors. Nutrients 8, 300 (2016).
McCann, S. E., Marshall, J. R., Brasure, J. R., Graham, S. & Freudenheim, J. L. Analysis of patterns of food intake in nutritional epidemiology: food classification in principal components analysis and the subsequent impact on estimates for endometrial cancer. Public Health Nutr. 4, 989–997 (2001).
Wall, C. R. et al. Dietary patterns in pregnancy in New Zealand—influence of maternal socio-demographic, health and lifestyle factors. Nutrients 8, 300 (2016).
Thompson, J. M. D. et al. Maternal dietary patterns in pregnancy and the association with small-for-gestational-age infants. Br. J. Nutr. 103, 1665–1673 (2010).
Jayasinghe, S. N. et al. Dietary patterns in New Zealand women: evaluating differences in body composition and metabolic biomarkers. Nutrients 11, 1643 (2019).
Naska, A., Lagiou, A. & Lagiou, P. Dietary assessment methods in epidemiological research: current state of the art and future prospects. F1000Research 6, 926 (2017).
Thompson, F. E. & Byers, T. Dietary assessment resource manual. J. Nutr. 124, 2245S-2317S (1994).
Hebert, J. R., Clemow, L., Pbert, L., Ockene, I. S. & Ockene, J. K. Social desirability bias in dietary self-report may compromise the validity of dietary intake measures. Int. J. Epidemiol. 24, 389–398 (1995).
Sam, C. H. Y. et al. Relative validity and reproducibility of a short food frequency questionnaire to assess nutrient intakes of New Zealand adults. Nutrients 12, 619 (2020).
Hu, F. B. et al. Reproducibility and validity of dietary patterns assessed with a food-frequency questionnaire. Am. J. Clin. Nutr. 69, 243–249 (1999).
Khani, B. R., Ye, W., Terry, P. & Wolk, A. Reproducibility and validity of major dietary patterns among Swedish women assessed with a food-frequency questionnaire. J. Nutr. 134, 1541–1545 (2004).
Korkalo, L. et al. Parents’ reports of preschoolers’ diets: relative validity of a food frequency questionnaire and dietary patterns. Nutrients 11, 159 (2019).
Field, A. Discovering statistics using SPSS (SAGE Publications, Thousand Oaks, 2009).
Moeller, S. M. et al. Dietary patterns: challenges and opportunities in dietary patterns research an Experimental Biology workshop, April 1, 2006. J. Am. Diet. Assoc. 107, 1233–1239 (2007).
Crowther, C. A., Alsweiler, J. M., Hughes, R. & Brown, J. Tight or less tight glycaemic targets for women with gestational diabetes mellitus for reducing maternal and perinatal morbidity? (TARGET): study protocol for a stepped wedge randomised trial. BMC Pregnancy Childbirth 18, 425 (2018).
Willett, W. Nutritional epidemiology (Oxford University Press, Oxford, 2012).
Russell, D. G. et al. NZ food, NZ people: key results of the 1997 National Nutrition Survey (Ministry of Health, Wellington, 1999).
Northstone, K., Ness, A. R., Emmett, P. M. & Rogers, I. S. Adjusting for energy intake in dietary pattern investigations using principal components analysis. Eur. J. Clin. Nutr. 62, 931 (2008).
Rhee, J. J. et al. Comparison of methods to account for implausible reporting of energy intake in epidemiologic studies. Am. J. Epidemiol. 181, 225–233 (2015).
Baglin, J. Improving your exploratory factor analysis for ordinal data: a demonstration using FACTOR. Pract. Assess. Res. Eval. 19, 1–14 (2014).
Willett, W. & Stampfer, M. J. Total energy intake: implications for epidemiologic analyses. Am. J. Epidemiol. 124, 17–27 (1986).
Cerny, B. A. & Kaiser, H. F. A study of a measure of sampling adequacy for factor-analytic correlation matrices. Multivar. Behav. Res. 12, 43–47 (1977).
Kaiser, H. F. An index of factorial simplicity. Psychometrika 39, 31–36 (1974).
Johnson, R. A. & Wichern, D. W. Applied multivariate statistical analysis (Pearson Prentice Hall, Upper Saddle River, 2007).
Hatcher, L. A step-by step approach to using the SAS system for factor analysis and structural equation modeling (SAS Publishing, Cary, 1994).
Cattell, R. B. The scree test for the number of factors. Multivar. Behav. Res. 1, 245–276 (1966).
Fransen, H. P. et al. A posteriori dietary patterns: how many patterns to retain?. J. Nutr. 144, 1274–1282 (2014).
Kaiser, H. F. The application of electronic computers to factor analysis. Educ. Psychol. Meas. 20, 141–151 (1960).
Global strategy for infant and young child feeding (WHO, 2003).
National breastfeeding advisory committee of New Zealand, New Zealand & Ministry of health, New Zealand & Ministry of Health. National Strategic Plan of Action for Breastfeeding, 2008–2012. (Ministry of Health, 2009).
Llewellyn, C. H., van Jaarsveld, C. H. M., Johnson, L., Carnell, S. & Wardle, J. Development and factor structure of the Baby Eating Behaviour Questionnaire in the Gemini birth cohort. Appetite 57, 388–396 (2011).
Wardle, J., Guthrie, C. A., Sanderson, S. & Rapoport, L. Development of the children’s eating behaviour questionnaire. J. Child Psychol. Psychiatry 42, 963–970 (2001).
Vaus, D. A. D. Surveys in social research (Psychology Press, East Sussex, 2002).
WHO. WHO|What is overweight and obesity? WHO https://www.who.int/dietphysicalactivity/childhood_what/en/ (2019).
Atkinson, J., Salmond, C. & Crampton, P. NZDep2013 index of deprivation, vol. 64 (2014).
Critchlow. NZ deprivation index 2013. https://www.critchlow.co.nz/data/gis-demographic-data/nzdepindex2013 (2019).
Howard, A. J., Mallan, K. M., Byrne, R., Magarey, A. & Daniels, L. A. Toddlers’ food preferences. The impact of novel food exposure, maternal preferences and food neophobia. Appetite 59, 818–825 (2012).
Mennella, J. A., Jagnow, C. P. & Beauchamp, G. K. Prenatal and postnatal flavor learning by human infants. Pediatrics 107, E88 (2001).
Acknowledgements
The authors would like to thank the women and infants who participated in the TARGET Trial and members of the TARGET Study Group.
Funding
Emma Amissah was supported by a doctoral scholarship from the University of Auckland, Auckland, New Zealand. Data used for this research were from the TARGET Trial funded by the Health Research Council of New Zealand (ID 14/499). The University of Auckland and Health Research Council of New Zealand had no role in the design, analysis or writing of this article.
Author information
Authors and Affiliations
Contributions
J.E.H, C.R.W, C.A.C, conceived the study; E.A prepared the protocol, conducted the analyses, interpreted the results and wrote all drafts. G.G, C.R.W, C.A.C, and J.E.H contributed to the analyses and all authors contributed to the interpretation of results. J.E.H critically revised all drafts of the paper and all authors reviewed drafts of the manuscript and approved the final version.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Amissah, E., Gamble, G.D., Wall, C.R. et al. The relationship between maternal dietary patterns during pregnancy in women with gestational diabetes mellitus and infant appetitive feeding behaviour at 6 months. Sci Rep 10, 20516 (2020). https://doi.org/10.1038/s41598-020-77388-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-020-77388-1
This article is cited by
-
Prospective relations of maternal reward-related eating, pregnancy ultra-processed food intake and weight indicators, and feeding mode with infant appetitive traits
International Journal of Behavioral Nutrition and Physical Activity (2022)
-
Folic acid supplementation during pregnancy alters behavior in male rat offspring: nitrative stress and neuroinflammatory implications
Molecular Neurobiology (2022)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
