
Abstract
Hypotensive events are strongly correlated to the occurrence of perioperative acute kidney injury, but the underlying mechanisms for this are not completely elucidated. We hypothesised that anaesthesia-induced hypotension causes renal vasoconstriction and decreased oxygen delivery via angiotensin II-mediated renal vasoconstriction. Pigs were anaesthetised, surgically prepared and randomised to vehicle/losartan treatment (0.15 mg*kg−1). A deliberate reduction in arterial blood pressure was caused by infusion of propofol (30 mg*kg−1) for 10 min. Renal function and haemodynamics were recorded 60 min before and after hypotension. Propofol induced hypotension in all animals (p < 0.001). Renal blood flow (RBF) and renal oxygen delivery (RDO2) decreased significantly regardless of treatment but more so in vehicle-treated compared to losartan-treated (p = 0.001, p = 0.02, respectively). During recovery RBF and RDO2 improved to a greater extent in the losartan-treated compared to vehicle-treated (+ 28 ml*min−1, 95%CI 8–50 ml*min−1, p = 0.01 and + 3.1 ml*min−1, 95%CI 0.3–5.8 ml*min−1, p = 0.03, respectively). Sixty minutes after hypotension RBF and RDO2 remained depressed in vehicle-treated, as renal vascular resistance was still increased (p < 0.001). In losartan-treated animals RBF and RDO2 had normalised. Pre-treatment with losartan improved recovery of renal blood flow and renal oxygen delivery after propofol-induced hypotension, suggesting pronounced angiotensin II-mediated renal vasoconstriction during blood pressure reductions caused by anaesthesia.
Similar content being viewed by others


Introduction
Acute kidney injury (AKI) is a common surgical complication. Approximately 8–10% of patients develop AKI after general surgery1 and in cardiac and vascular surgery the incidence is even higher (10–40%)2,3,4. AKI is defined as rapidly decreasing renal function graded by changes in serum creatinine levels and/or urine output5,6.
The kidneys receive 20–25% of cardiac output during normal conditions7, but are highly susceptible to ischemia due to heterogeneity in oxygenation8. Intraoperative hypotension and hypovolemia may result in renal ischemia and are known causes of AKI9. Hypotension is a frequent complication to anaesthesia since most agents used to induce anaesthesia cause vasodilation and infrequently reductions in cardiac output10. It has been described that even short (less than 5 min) reductions in mean arterial pressure (MAP) below 55 mmHg is independently associated with perioperative AKI11,12. An acute decrease in MAP outside renal autoregulation reduces renal oxygen delivery (RDO2). Furthermore, unloading baroreceptors increase sympathetic nerve activity and release of endogenous vasoactive hormones, such as catecholamines, renin and angiotensin-II (Ang-II), vasopressin and aldosterone13,14,15. Although this may aid in restoring MAP it theoretically causes a prolonged renal vasoconstriction, even after blood volume and/or pressure is restored.
Angiotensin converting enzyme inhibitors (ACEi) and angiotensin-II type-1 receptor blockers (ARB’s) are common treatments for hypertension16. It is also well accepted that high levels of Ang-II may cause renal damage and that inhibition of Ang-II is renoprotective in early chronic kidney disease17,18,19. These medications are often withheld prior to surgery to avoid perioperative hypotension20. However, Ang-II inhibition during anaesthesia may have beneficial renal effects.
We hypothesise that Ang-II released by propofol-induced hypotension may cause renal ischemia by reducing RDO2 due to prolonged renal vasoconstriction. To investigate this, we studied the effects of losartan (an intravenously administered ARB) on RBF, RDO2 and short-term renal function in pigs subjected to an anaesthesia-induced hypotensive event.
Results
Mean arterial pressure (MAP) was similar in both groups at baseline (vehicle: 93 ± 9 mmHg; losartan: 90 ± 9 mmHg, p = 0.64, Fig. 1a) and remained unchanged by the treatment per se (vehicle: 92 ± 8 mmHg, p = 0.93; losartan: 93 ± 6 mmHg, p = 0.45, Fig. 1a). During the propofol-induced hypotensive event MAP was reduced by 38 mmHg in vehicle-treated (95%CI 30–45 mmHg, p < 0.001, Fig. 1a) and 42 mmHg in losartan-treated (95%CI 34–50 mmHg, p < 0.001, Fig. 1a) without significant intergroup difference. Recovery for 60 min improved MAP by 20 mmHg in vehicle-treated (95%CI 9–31 mmHg, p = 0.001, Fig. 1a) and 26 mmHg in losartan-treated (95%CI 15–37 mmHg, p < 0.001, Fig. 1a), with no significant intergroup difference.

(a) MAP, (b) RBF and (c) RVR at baseline, treatment, hypotension and recovery in vehicle- (n = 11, black) and losartan-treated (n = 11, white) pigs. Data is displayed as mean ± 95%CI. Please refer to the main text for statistical analyses.
At baseline renal blood flow (RBF) did not differ significantly between groups (vehicle: 168 ± 26 ml*min−1, losartan: 142 ± 28 ml*min−1, p = 0.18, Fig. 1b). Treatment had no effect on RBF in any of the groups (vehicle: 160 ± 26 ml*min−1, p = 0.09; losartan: 138 ± 29 ml*min−1, p = 0.81, Fig. 1b). However, RBF was significantly reduced by propofol and this effect was more pronounced in the vehicle-treated animals compared to losartan-treated (− 36 ml*min−1, 95%CI 2–70 ml*min−1, p = 0.001, Fig. 1b). During recovery, RBF improved to a greater extent in the losartan-treated pigs compared to vehicle-treated (+ 28 ml*min−1, 95%CI 8–50 ml*min−1, p = 0.01, Fig. 1b). RBF was still decreased in vehicle-treated animals 60 min after propofol was administered (98 ± 11 ml*min−1, p < 0.001, Fig. 1b). However, in the losartan group RBF had returned to baseline (134 ± 29 ml*min−1, p = 0.47, Fig. 1b).
Renal vascular resistance (RVR) did not differ between groups at baseline (vehicle: 0.52 ± 0.11, losartan: 0.62 ± 0.11 mmHg*min*ml−1, p = 0.18, Fig. 1c). It also remained unchanged by the treatment (vehicle: 0.55 ± 0.11, p = 0.36; losartan: 0.66 ± 0.11 mmHg*min*ml−1, p = 0.40, Fig. 1c). Propofol caused a greater increase in RVR in pigs treated with vehicle compared to losartan (0.2 mmHg*min*ml−1, 95%CI 0.02–0.4 mmHg*min*ml−1, p = 0.036, Fig. 1c). Vehicle-treated pigs also had significantly increased RVR after recovery compared to baseline (0.70 ± 0.12 mmHg*min*ml−1, p < 0.001, Fig. 1c) whereas losartan-treated had significantly decreased RVR compared to baseline (0.54 ± 0.10 mmHg*min*ml−1, p = 0.03, Fig. 1c). However, no significant differences between the groups was demonstrated after 60-min recovery (vehicle: 0.61 ± 0.17, losartan: 0.49 ± 0.09 mmHg*min*ml−1, p = 0.07, Fig. 1c).
Renal oxygenation
Renal oxygen delivery (RDO2) was, as expected, affected in a similar manner as RBF. Baseline RDO2 was not significantly different between the groups (vehicle: 19 ± 3 ml*min−1, losartan: 15 ± 3 ml*min−1, p = 0.06, Fig. 2a) and treatment did not affect RDO2 in either group (vehicle: 18 ± 3 ml*min−1, p = 0.21; losartan: 15 ± 2 ml*min−1, p = 0.72, Fig. 2a). The propofol-induced hypotensive event caused a more pronounced decrease in RDO2 in vehicle-treated pigs (4.5 ml*min−1, 95%CI 0.6–8.3 ml*min−1, p = 0.02, Fig. 2a) compared to losartan-treated. RDO2 recovery after hypotension was also improved by losartan compared to vehicle (+ 3.1 ml*min−1, 95%CI 0.3–5.8 ml*min−1, p = 0.03, Fig. 2a). Compared to baseline vehicle-treated pigs had significantly lower RDO2 after recovery (11 ± 2 ml*min−1, p < 0.001, Fig. 2a). Losartan-treated pigs made a full recovery with regards to RDO2 (14 ± 2 ml*min−1, p = 0.35, Fig. 2a).

(a) RDO2, (b) RVSO2 and (c) RO2ER over time at baseline, treatment, hypotension and recovery in vehicle- (n = 11, black) and losartan-treated (n = 11, white) pigs. Data is displayed as mean ± 95%CI. Please refer to the main text for statistical analyses.
Renal Vein Oxygen Saturation (RVSO2) was not different between groups at baseline (vehicle: 73 ± 3%, losartan: 70 ± 4%, p = 0.29, Fig. 2b). Losartan had no effect on this parameter (70 ± 4%, p = , Fig. 2b). However, in vehicle-treated pigs RVSO2 increased by 3% (96%CI 0–5%, p = 0.02). Propofol-induced hypotension decreased RVSO2 in both vehicle- and losartan-treated (9% 95%CI 2–16%, p = 0.02 and 8% 95%CI 1–15%, p = 0.03, respectively, Fig. 2b), with no intergroup differences. Both groups increased RVSO2 after recovery compared to hypotension (vehicle: 9% 95%CI 2–15%, p < 0.009; losartan: 9% 96%CI 2–15, p = 0.01, Fig. 2b), with no significant intergroup difference.
Renal oxygen extraction rate (RO2ER) was not different at baseline (vehicle: 24 ± 3%, losartan: 25 ± 4%, p = 0.20, Fig. 2c). Vehicle-treated decreased RO2ER during the treatment period (3% 95%CI 0–5%, p = 0.02, Fig. 2c) meanwhile losartan-treated remined unchanged (25 ± 4%, p = 0.49, Fig. 2c). Hypotension increased RO2ER in both groups by 8% in vehicle-treated (95%CI 1–16%, p = 0.02, Fig. 2c) and 8% in losartan-treated (95%CI 0–15%, p = 0.04, Fig. 2c) without intergroup difference. After recovery, RO2ER in both groups normalised (vehicle: 24 ± 3%, p = 0.81; losartan: 26 ± 3%, p = 0.51, Fig. 2c).
Renal oxygen consumption (RVO2) did not differ between groups at baseline (vehicle: 5.0 ± 0.9 mmol*min−1, losartan: 3.3 ± 1.3 mmol*min−1, p = 0.32, Table 1). In vehicle-treated pigs RVO2 decreased significantly (− 0.9 mmol*min−1) during the treatment period (95%CI 0.1–1.8 mmol*min−1, p = 0.04, Table 1) whereas in losartan-treated pigs RVO2 did not change (3.4 ± 1.5 mmol*min−1, p = 0.98, Table 3). Hypotension decreased RVO2 even further in the vehicle-treated pigs (− 0.9 mmol*min−1 95%CI 0.1–1.8 mmol*min−1, p = 0.02, Table 1). In losartan-treated pigs RVO2 increased compared to baseline as response to propfol (+ 0.9 mmol*min−1 95%CI 0.1–1.8 mmol*min−1, p = 0.04, Table 1). During recovery RVO2 remained depressed in pigs treated with vehicle (2.6 ± 0.6 mmol*min−1, p = 0.2) but not losartan (3.2 ± 0.7 mmol*min−1, p = 0.26, Table 1).
Renal Lactate levels (R-Lac) was significantly higher in losartan-treated at baseline (vehicle: 1.3 ± 0.1 mmol*l−1, losartan: 1.6 ± 0.2 mmol*l−1, p = 0.01, Table 1). Vehicle- and losartan-treated pigs remained unchanged by treatment with regards to R-Lac (1.3 ± 0.2 mmol*l−1, p = 0.85 and 1.5 ± 0.2 mmol*l−1, p = 0.31, respectively, Table 1) and by hypotension (1.5 ± 0.2 mmol*l−1, p = 0.11 and 1.8 ± 0.3 mmol*l−1, p = 0.27, respectively, Table 1). After the 60-min recovery-period R-Lac was unchanged in vehicle-treated pigs (1.3 ± 0.2 mmol*l−1, p = 0.35, Table 1) but had decreased in losartan-treated pigs compared to hypotension (0.25 mmol*l−1 95%CI 0.1–0.4 mmol*l−1, p = 0.007, Table 1).
Renal parameters
Plasma creatinine, creatinine clearance, urine output and urinary sodium excretion did not change significantly as an effect of losartan treatment or propofol (Table 1).
Systemic perfusion
Carotid Blood Flow (CBF) was not significantly different at baseline between the groups (vehicle: 148 ± 19 ml*min−1, losartan: 122 ± 23 ml*min−1, p = 0.10, Table 2), and treatment had no effect on CBF in either group (vehicle: 152 ± 20 ml*min−1, p = 0.61; losartan: 129 ± 22 ml*min−1, p = 0.43, Table 2). Hypotension did not significantly change CBF in either vehicle-treated (159 ± 30 ml*min−1, p = 0.50, Table 2) nor losartan-treated (113 ± 18 ml*min−1, p = 0.57, Table 3). CBF remained unchanged in vehicle-treated pigs during recovery (175 ± 32 ml*min−1, p = 0.44, Table 2) but increased in losartan-treated animals compared to hypotension (+ 65 ml*min−1 95%CI 22–107 ml*min−1, p = 0.004, Table 2).
Cardiac Output (CO) was not different at baseline when comparing the two groups (vehicle: 3.1 ± 0.6 ml*min−1, losartan: 3.2 ± 0.4 ml*min−1, p = 0.75, Table 2). Treatment had no significant effect on CO in either group (vehicle: 3.3 ± 0.4 ml*min−1, p = 0.33; losartan: 3.4 ± 0.4 ml*min−1, p = 0.35, Table 2). Propofol-induced hypotension did not affect CO in either group (vehicle: 3.3 ± 0.8 ml*min−1, p = 0.52; losartan: 3.1 ± 0.7 ml*min−1, p = 0.39, Table 3). After recovery CO was not significantly different in vehicle-treated compared to hypotension (4.0 ± 0.7 ml*min−1, p = 0.07, Table 2). However losartan increased CO by 1.0 ml*min−1 during recovery compared to hypotension (95%CI 0.3–1.8 ml*min−1, p = 0.01, Table 2).
Heart Rate (HR) did not differ between groups at baseline (vehicle: 95 ± 11 bpm, losartan: 102 ± 16 bpm, p = 0.47, Table 3) and was not changed by the treatment (vehicle: 102 ± 9 bpm, p = 0.14; losartan: 99 ± 11 bpm, p = 0.42, Table 2) or hypotension (vehicle: 104 ± 8 bpm, p = 0.21; losartan: 100 ± 12 bpm, p = 0.68, Table 2). During recovery HR was not significantly changed in vehicle-treated (112 ± 12 bpm, p = 0.10, Table 3), However losartan increased HR by 13 bpm (95%CI 1–26 bpm, p = 0.04, Table 2).
CVP decreased by 2 mmHg (95%CI 0–3 mmHg, p = 0.04, Table 3) after recovery compared to hypotension without intergroup difference.
PAP decreased by 2 mmHg (95%CI 0–4 mmHg, p = 0.007, Table 3) during hypotension compared to baseline with no intergroup difference. PAP then increased after recovery compared to hypotension without intergroup difference (3 mmHg 95%CI 2–5 mmHg, p < 0.001, Table 3).
PWP and RVP was not significantly changed during the experimental protocol.
Discussion
This study was conducted to evaluate the acute effects of systemic Ang-II antagonism on renal perfusion, oxygenation and function after an anaesthesia-induced hypotensive event. The main finding was that losartan improved recovery of RBF and RDO2 after a hypotensive dose of propofol. The data obtained indicates that RBF may be impaired for a considerable amount of time after hypotension even though usually monitored clinical parameters (i.e. MAP, HR, CO, plasma-lactate or urine output) remained unchanged or have normalised.
Perioperative AKI has been described as an under-recognised problem with few available preventive treatment strategies21. In a majority of cases the underlying mechanism causing renal dysfunction is unknown22,23. Propofol is an agent frequently used to induce general anaesthesia. It is also a potent vasodilator which entails that the most common side-effect is hypotension10.
Ang-II causes powerful systemic vasoconstriction through Ang-II receptor 1 (AT1) binding. This effect is regionally differentiated in that the renal circulation constricts more in comparison to other vascular beds24. Plasma levels of Ang-II are increased by hypotension and decreases RBF and glomerular filtration rate25. In this study we designed an experiment to investigate if renal perfusion was impaired due to Ang-II. The aim was to mimic a clinical anaesthesia induction resulting in an unwanted but transient hypotensive event. Even if hypotension is swiftly corrected the resulting potential increase in Ang-II may cause a persistent reduction in RBF that is difficult to monitor and treat in anaesthetised patients undergoing surgery. Patients that are extra susceptible to renal ischemia, perhaps due to diabetes, hypertension, cardiovascular disease and/or prior kidney disorders may then develop AKI1,26. The reduction in RBF may be insufficient to cause postoperative renal dysfunction in otherwise healthy patients. Previous studies have shown detrimental renal effects of high circulating levels of Ang-II in a variety of settings27. A clinical study showed that inhibition of Ang-II in diabetic CKD patients had beneficial effects on renal oxygenation28. Furthermore, the current study indicates that Ang-II may also be a culprit in acute settings of anaesthesia-induced hypotension.
Continuous medication targeting Ang-II is common in large population of patients, such as CKD, diabetes and cardiovascular disease. These groups of patients also have higher risk for perioperative AKI. Prolonged renal vasoconstriction and decreased RDO2 may provoke a mismatch in O2 consumption and delivery ultimately leading to hypoxia29,30. In current clinical practice it is common procedure to withhold any ACEi/ARB’s prior to surgery. The rationale is to avoid hypotension and cardiac events31. However, the preoperative management of ACEi/ARB’s are extensively debated and currently the data for continuing or withholding preoperative treatment is not clear20,32. It was suggested over 20 years ago that hypertensive patients should continue Ang-II antagonistic treatment before surgery33. On the other hand, Brabant et al. demonstrated significantly higher risk for reduced arterial blood pressure and more treatment-resistant hypotensive events in patients continuing ARB’s compared to other anti-hypertensives34. Interestingly, a recent multicentre study demonstrated no significant differences in AKI outcome in patients with ongoing ARB’s/ACEi compared to patients withholding treatment. The potent vasoconstriction achieved by pharmacological treatment with Ang-II have also been demonstrated to have beneficial effects on blood pressure and reduced need of vasopressors during refractory shock35.
The reductions in RBF and increase in RVR in vehicle-treated pigs were significant 60 min after propofol was discontinued, even though MAP had more or less recovered. Losartan attenuated the renal vasoconstriction and normalised renal blood flow. Although uncertain in this study as we did not measure AngII-levels in plasma, this was likely due to inhibition of excessive release of Ang-II caused by hypotension36. As a result, RDO2 was reduced in the vehicle-treated pigs but greatly improved by losartan. It has also been shown that anaesthesia per se cause release of Ang-II37. Since losartan did not reduce MAP prior to hypotension the contribution of Ang-II to baseline blood pressure during anaesthesia in the current setting is likely small. The lack of pressure effect inhibiting systemic Ang-II is much like what is seen in normotensive conscious humans38.
RVO2 was decreased in the losartan-treated animals during the hypotensive event. Ang-II acts via the AT1-receptor to stimulate Na/K-ATPase and, in theory, thereby increasing renal oxygen consumption. This effect was not noted during the relatively short protocol executed in this study. Unfortunately oxygenation in renal tissue was not measured and it is possible that local hypoxia was present although not to the degree that it was reflected in renal vein blood gases. Furthermore, the subjects were healthy, young pigs with kidneys most likely more resistant to decreased renal blood flow than the average human patient undergoing general anaesthesia.
Other parameters for assessing renal function such as P-Cr, Cr-C, USE and urine output did not change during the course of the protocol. This is most likely due to the acute setting and that more profound renal impairment may be necessary for these markers to be altered in previously healthy individuals39.
Cardiovascular parameters were continuously monitored to ensure that systemic haemodynamics were not negatively affected by losartan and to identify possible mechanisms for changes in RBF. Losartan per se had no adverse effects on haemodynamics during the study protocol. Importantly, CBF remained unaffected by losartan during hypotension suggesting that losartan did not impair cerebral perfusion. Another crucial aspect is that losartan did not augment the hypotension caused by propofol. This is in agreement with the finding that MAP was affected similarly during hypovolaemia in anaesthetised pigs treated with either ACEi/ARB’s or vehicle40.
Limitations
All animals in this study arrived one at the time after a short transport and was assessed by experienced lab-technicians to be calm and non-stressed at time of anaesthesia induction. A mix of male and female pigs was used to eliminate gender variability. It would have been preferable to have blinded this study to rigorise the results, however due to practical reasons this was not feasible. The acute setting limits the information provided on possible long-lasting effects of Ang-II inhibition during anaesthesia. Furthermore, the relatively short duration of ischemia in young and healthy individuals also reduce the likelihood of renal structural damage; therefore no histological samples were collected. The purpose of this study was to demonstrate the physiological effects of Ang-II blockade. However, biomarkers such as urinary kidney injury marker-1 (KIM-1) or neutrophil gelatinase-associated lipocalin (NGAL) could have been analysed in order to detect mild renal injury. Plasma levels of Ang-II were not measured in this study and because of that we cannot definitely conclude that Ang-II levels were elevated in response to hypotension. However, it has been shown in similar animal models36.
Finally, the present study uses a relatively small number of healthy pigs as a large animal model of the human situation. This is to enable research impossible to perform in patients, describing basic mechanisms of action. The results should be interpreted carefully and cannot be directly transferred to the clinic. Still, the prevention of renal vasoconstriction by losartan presented here merits future investigations of the renal effects of Ang-II inhibition in anesthetized human patients.
Conclusion
The present study demonstrate that pre-treatment with losartan prevent renal vasoconstriction and improve recovery of renal blood flow and oxygen delivery after anaesthesia-induced hypotension.
Methods
Ethical approval and animals
All methods were carried out in accordance to relevant guidelines and regulations. Ethical approval for this study (Dnr. 5.8.18-02325/2019) was provided by the Uppsala Animal Ethics Board of the Swedish Board of Agriculture (Jordbruksverket), Sweden on March 29, 2019. Male and female Norwegian Landrace breed/Hampshire/Yorkshire pigs (24 ± 2 kg, 3–4 months old) were purchased from a local farmer in Uppsala, Sweden, to eliminate gender variability. The pigs were born on the farm and housed in group in large cages with water and food ad libitum. A total of 22 pigs were used; 11 vehicle-treated and 11 losartan-treated. Pigs arrived at the laboratory at 8.00 am (a 20-min truck ride in cage) one/two at the time and were randomised to treatment/control group by an ‘every other’ method.
Anaesthesia
At the time of arrival, the pigs were weighed and sedated with an intramuscular injection of tiletamine-zolazepam (Zoletil 6 mg*kg−1) and xylazine (Rompun 2.2 mg*kg−1). After 3 min, pigs were tracheostomised and put under mechanical ventilation and given ketamine (Ketaminol 20 mg) and morphine (20 mg) in a peripheral vein in the ear. Pentobarbital (8 mg*kg-1*h−1) and morphine (0.26 mg*kg−1*h−1) dissolved in a glucose/sodium-solution (sodium chloride 2.5 mg*ml−1 and glucose 25 mg*ml−1) was given for maintenance of anaesthesia and rocuronium (Esmeron 2,5 mg*kg−1*h−1) for muscle relaxation. After finished experimental protocol, pigs were euthanised with potassium chloride.
Surgical preparation
Peripheral vein catheters were placed in each ear for heated (38 °C) infusion of anaesthesia and Ringer’s acetate (15 mg*kg−1*h−1 for the first hour followed by 10 mg*kg−1*h−1). Mechanical ventilation was set to achieve arterial PCO2 4.5–5.5 kPa with FiO2 0.30. Tidal volume (TV) was started at 10 ml*kg-1, respiratory rate (RR) 25 and positive end-expiratory pressure (PEEP) at 5 cm H2O, if needed TV/RR was adjusted to maintain arterial PCO2 4.5–5.5 kPa. The carotid artery on the right side was catheterised with a single lumen catheter for continuous monitoring of MAP and blood sampling. The jugular vein on the right side was catheterised with a 3 lm-catheter for cardiac output, fluid infusion and continuous monitoring of central venous pressure (CVP). Furthermore, a balloon-tipped pulmonary artery catheter (7.5F Swan-Ganz, Edwards Lifesciences, Irvine, CA) was placed into the right jugular vein and advanced into the pulmonary artery for monitoring of pulmonary arterial pressure (PAP), pulmonary wedge pressure (PWP) and blood sampling. The location of the PA-catheter was confirmed by assessing the pressure-curve on the monitor derived from the tip of the catheter. After the right atrium was reached, the catheter was carefully advanced into the pulmonary artery. To confirm correct placement, the balloon was inflated to obtain a pulmonary wedge pressure curve on the monitor. A flow probe (FSB-series 3, Transonic, Ithaca, NY) was placed around the carotid artery on the left side for monitoring of carotid blood flow (CBF). The left jugular vein was catheterised with a single lumen catheter for blood gas analysis. A suprapubic catheter (Foley no. 8. A Datex-Ohmeda S/5 monitor, Madison, WI) was placed in the bladder for urine collection. The pigs were then turned to lay on their right side. A 10 cm incision was made from rib to hip to locate and dissect the left kidney. A flow probe (FSB-series 4) was placed around the renal artery for continuous monitoring of RBF. A single lumen catheter was then placed into the renal vein for monitoring of renal vein pressure (RVP) and blood sampling. All incisions were closed with sutures (Prolene 3.0). After surgical preparation, the pigs were allowed to recover for 45 min before the experiment commenced.
Experimental protocol
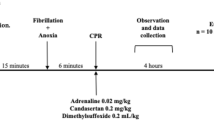
Pigs were block-randomised to no treatment (vehicle, n = 11) or losartan treatment (n = 11). Baseline recordings for 5 min were performed before treatment was started. An intravenous infusion of losartan was commenced with a bolus (0.2 mg*kg−1) followed by a continuous infusion (0.15 mg*kg−1*h−1) similar to previously reported experiments41. Vehicle-treated pigs received no additional infusion. The experiment was divided into four consecutive periods; baseline (5 min before drug administration), treatment (60 min with drug infusion), hypotension (10 min with propofol infusion) and recovery (60 min). Hypotension was induced by continuous infusion of propofol (30 mg*kg−1). At every timepoint (Fig. 3), blood was sampled for blood-gas status and analysis of creatinine, sodium and potassium. Vital parameters were noted by reading of the mechanical ventilator, the monitor for pressures and the Transonic flow-meter. In addition, arterial blood was also collected halfway through the treatment and recovery periods. Urine was continuously collected only over the 60-min periods (treatment and recovery).

Flow chart of the experimental protocol. Pigs were sedated, surgically prepared and then allowed to recover. Baseline measurements were performed before infusion of either losartan or vehicle. The infusion continued for 60 min before hypotension was induced by administering propofol (30 mg*kg−1) continuously over 10 min. After the infusion of propofol was discontinued the animals were followed for an additional 60 min. The protocol was then ended, and pigs were euthanised with intravenous bolus of potassium chloride.
Blood and urine samples were analysed by the in-house hospital laboratory at the Uppsala University Hospital (Clinical Chemistry Laboratory) to evaluate plasma and urinary creatinine (enzymatic method) and sodium/potassium levels (flame photometry). Blood gases were sampled from the carotid artery, renal vein, jugular vein and pulmonary artery to evaluate pO2, PCO2, SO2, haemoglobin, lactate and electrolyte levels (Radiometer Medical ApS, ABL800 FLEX, Brönshöj, Denmark). Parameters that were registered and calculated for results are MAP, RBF, renal vascular resistance (RVR), RDO2, CBF, cardiac output (CO), heart rate (HR), renal venous oxygen saturation (RVSO2), renal venous lactate (RLac), renal oxygen consumption (RVO2), renal oxygen extraction rate (RO2ER), creatinine clearance (Cr-C), plasma creatinine (P-Cr), urine output and urinary sodium excretion (USE). The cardiovascular pressures CVP, PAP, PWP was only monitored to confirm heart and pulmonary function.
Calculations
RVR = (MAP − RVP) * RBF−1.
O2 content = (SO2 * haemoglobin * 1.39) + (pO2 * 0.003).
RDO2 = (RBF * arterial O2 content) * 1000−1.
RVO2 = ((arterial O2 content − renal venous O2 content) * RBF) * 1000−1.
RO2ER = (arterial SO2 − renal venous SO2) * arterial SO2−1.
Urine output = volume * minutes−1.
Cr-C = (urinary Cr * urine output) * P-Cr−1.
USE = urinary Na+ * urine output−1.
Statistical analysis
All data are displayed as mean ± 95% confidence interval. The software Statistica (StatSoft, Uppsala, Sweden) was used for statistical analysis. The repeated measurements analysis of variance with 2 levels of between-subject factors and 4 levels of within-subject factors (RM 2 × 4 ANOVA) was used. Corrections for multiple comparisons were made with specific contrasts as posthoc analysis.
Data availability
All data generated or analysed during this study are included in this published article (and its Supplementary Information files).
References
Biteker, M. et al. Incidence, risk factors, and outcomes of perioperative acute kidney injury in noncardiac and nonvascular surgery. Am. J. Surg. 207, 53–59. https://doi.org/10.1016/j.amjsurg.2013.04.006 (2014).
Chew, S. T., Ng, R. R., Liu, W., Chow, K. Y. & Ti, L. K. Acute kidney injury increases the risk of end-stage renal disease after cardiac surgery in an Asian population: a prospective cohort study. BMC Nephrol. 18, 60. https://doi.org/10.1186/s12882-017-0476-y (2017).
Bihorac, A. Acute kidney injury in the surgical patient: recognition and attribution. Nephron 131, 118–122. https://doi.org/10.1159/000439387 (2015).
Wilson, T. et al. Risk prediction models for acute kidney injury following major noncardiac surgery: systematic review. Nephrol. Dial. Transpl. Off. Publ. Eur. Dial. Transpl. Assoc. Eur. Renal Assoc. 31, 231–240. https://doi.org/10.1093/ndt/gfv415 (2016).
Hoste, E. A. J. et al. RIFLE criteria for acute kidney injury is associated with hospital mortality in critically ill patients: a cohort analysis. Crit. Care https://doi.org/10.1186/cc4915 (2006).
Mehta, R. L. et al. Acute Kidney Injury Network: report of an initiative to improve outcomes in acute kidney injury. Crit. Care 11, R31. https://doi.org/10.1186/cc5713 (2007).
London, G. M., Safar, M. E., Sassard, J. E., Levenson, J. A. & Simon, A. C. Renal and systemic hemodynamics in sustained essential hypertension. Hypertension (Dallas, Tex.: 1979) 6, 743–754 (1984).
Brezis, M., Rosen, S., Silva, P. & Epstein, F. H. Renal ischemia: a new perspective. Kidney Int. 26, 375–383 (1984).
Goren, O. & Matot, I. Perioperative acute kidney injury. Br. J. Anaesth. 115(Suppl 2), ii3-14. https://doi.org/10.1093/bja/aev380 (2015).
Mackenzie, N. & Grant, I. S. Propofol for intravenous sedation. Anaesthesia 42, 3–6 (1987).
Walsh, M. et al. Relationship between intraoperative mean arterial pressure and clinical outcomes after noncardiac surgery: toward an empirical definition of hypotension. Anesthesiology 119, 507–515. https://doi.org/10.1097/ALN.0b013e3182a10e26 (2013).
Sun, L. Y., Wijeysundera, D. N., Tait, G. A. & Beattie, W. S. Association of intraoperative hypotension with acute kidney injury after elective noncardiac surgery. Anesthesiology 123, 515–523. https://doi.org/10.1097/aln.0000000000000765 (2015).
Zerbe, R. L., Feuerstein, G., Meyer, D. K. & Kopin, I. J. Cardiovascular, sympathetic, and renin-angiotensin system responses to hemorrhage in vasopressin-deficient rats. Endocrinology 111, 608–613. https://doi.org/10.1210/endo-111-2-608 (1982).
Zerbe, R. L., Henry, D. P. & Robertson, G. L. Vasopressin response to orthostatic hypotension. Etiologic and clinical implications. Am. J. Med. 74, 265–271 (1983).
Okamoto, H., Hoka, S., Kawasaki, T., Okuyama, T. & Takahashi, S. Dose-dependent increases in the renal sympathetic nerve activity during rapid increase in isoflurane concentration in intact, lower airway-deafferented, and baroreceptor-deafferented rabbits. Anesthesiology 84, 1196–1204 (1996).
Whelton, P. K. et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: executive summary: a report of the American college of cardiology/American heart association task force on clinical practice guidelines. Circulation 138, e426–e483. https://doi.org/10.1161/CIR.0000000000000597 (2018).
Lavoz, C. et al. Angiotensin II contributes to renal fibrosis independently of Notch pathway activation. PLoS ONE 7, e40490. https://doi.org/10.1371/journal.pone.0040490 (2012).
Rodriguez-Romo, R. et al. AT1 receptor antagonism before ischemia prevents the transition of acute kidney injury to chronic kidney disease. Kidney Int. 89, 363–373. https://doi.org/10.1038/ki.2015.320 (2016).
Colucci, J. A. et al. Renin-angiotensin system may trigger kidney damage in NOD mice. J. Renin. Angiotensin Aldosterone Syst. 12, 15–22. https://doi.org/10.1177/1470320310375456 (2011).
Pai, S. L., Chadha, R. M., Irizarry-Alvarado, J. M., Renew, J. R. & Aniskevich, S. Pharmacologic and perioperative considerations for antihypertensive medications. Curr. Clin. Pharmacol. 12, 135–140. https://doi.org/10.2174/1574884712666170918152004 (2017).
Meersch, M., Schmidt, C. & Zarbock, A. Perioperative acute kidney injury: an under-recognized problem. Anesth. Analg. 125, 1223–1232. https://doi.org/10.1213/ANE.0000000000002369 (2017).
Ostermann, M. & Liu, K. Pathophysiology of AKI. Best Pract. Res. Clin. Anaesthesiol. 31, 305–314. https://doi.org/10.1016/j.bpa.2017.09.001 (2017).
Ruggenenti, P., Cravedi, P. & Remuzzi, G. Mechanisms and treatment of CKD. J. Am. Soc. Nephrol. 23, 1917–1928. https://doi.org/10.1681/ASN.2012040390 (2012).
Forsyth, R. P., Hoffbrand, B. I. & Melmon, K. L. Hemodynamic effects of angiotensin in normal and environmentally stressed monkeys. Circulation 44, 119–129. https://doi.org/10.1161/01.cir.44.1.119 (1971).
Korner, P. I., Oliver, J. R., Zhu, J. L., Gipps, J. & Hanneman, F. Autonomic, hormonal, and local circulatory effects of hemorrhage in conscious rabbits. Am. J. Physiol. 258, H229-239. https://doi.org/10.1152/ajpheart.1990.258.1.H229 (1990).
Thakar, C. V., Arrigain, S., Worley, S., Yared, J. P. & Paganini, E. P. A clinical score to predict acute renal failure after cardiac surgery. J. Am. Soc. Nephrol. 16, 162–168. https://doi.org/10.1681/ASN.2004040331 (2005).
Sharma, N., Anders, H. J. & Gaikwad, A. B. Fiend and friend in the renin angiotensin system: an insight on acute kidney injury. Biomed. Pharmacother. 110, 764–774. https://doi.org/10.1016/j.biopha.2018.12.018 (2019).
Manotham, K. et al. Angiotensin II receptor blocker partially ameliorated intrarenal hypoxia in chronic kidney disease patients: a pre-/post-study. Intern. Med. J. 42, e33-37 (2012).
Mimura, I. & Nangaku, M. The suffocating kidney: tubulointerstitial hypoxia in end-stage renal disease. Nat. Rev. Nephrol. 6, 667–678. https://doi.org/10.1038/nrneph.2010.124 (2010).
Welch, W. J. Intrarenal oxygen and hypertension. Clin. Exp. Pharmacol. Physiol. 33, 1002–1005. https://doi.org/10.1111/j.1440-1681.2006.04478.x (2006).
Mets, B. Management of hypotension associated with angiotensin-axis blockade and general anesthesia administration. J. Cardiothorac. Vasc. Anesth. 27, 156–167. https://doi.org/10.1053/j.jvca.2012.06.014 (2013).
Zou, Z. et al. Perioperative angiotensin-converting enzyme inhibitors or angiotensin II type 1 receptor blockers for preventing mortality and morbidity in adults. Cochrane Database Syst. Rev. https://doi.org/10.1002/14651858.CD009210.pub2 (2016).
Laslett, L. Hypertension. Preoperative assessment and perioperative management. West J. Med. 162, 215–219 (1995).
Brabant, S. M., Bertrand, M., Eyraud, D., Darmon, P. L. & Coriat, P. The hemodynamic effects of anesthetic induction in vascular surgical patients chronically treated with angiotensin II receptor antagonists. Anesth. Analg. 89, 1388–1392 (1999).
Khanna, A. et al. Angiotensin II for the treatment of vasodilatory shock. N. Engl. J. Med. 377, 419–430. https://doi.org/10.1056/NEJMoa1704154 (2017).
Aneman, A. et al. Differentiation of the peptidergic vasoregulatory response to standardized splanchnic hypoperfusion by acute hypovolaemia or sepsis in anaesthetized pigs. Acta Physiol. Scand. 166, 293–300. https://doi.org/10.1046/j.1365-201x.1999.00574.x (1999).
Frithiof, R., Mats, R., Johan, U., Stefan, E. & Hans, H. Comparison between the effects on hemodynamic responses of central and peripheral infusions of hypertonic NaCl during hemorrhage in conscious and isoflurane-anesthetized sheep. Shock 26, 77–86. https://doi.org/10.1097/01.shk.0000215314.76370.c3 (2006).
MacGregor, G. A., Markandu, N. D., Smith, S. J., Sagnella, G. A. & Morton, J. J. Angiotensin converting enzyme inhibition reveals an important role for the renin system in the control of normal and high blood pressure in man. Clin. Exp. Hypertens A 5, 1367–1380 (1983).
Waikar, S. S., Betensky, R. A., Emerson, S. C. & Bonventre, J. V. Imperfect gold standards for kidney injury biomarker evaluation. J. Am. Soc. Nephrol. 23, 13–21. https://doi.org/10.1681/asn.2010111124 (2012).
Ryckwaert, F. et al. Haemodynamic effects of an angiotensin-converting enzyme inhibitor and angiotensin receptor antagonist during hypovolaemia in the anaesthetized pig. Br. J. Anaesth. 89, 599–604. https://doi.org/10.1093/bja/aef221 (2002).
Laesser, M., Spak, E., Ewert, S., Aneman, A. & Fandriks, L. Candesartan improves survival following severe hypovolemia in pigs; a role for the angiotensin II type 2 receptor?. Intensive Care Med. 31, 1109–1115. https://doi.org/10.1007/s00134-005-2686-1 (2005).
Acknowledgements
For technical assistance and logistics, we thank the staff at the Hedenstierna laboratory at Uppsala University, Uppsala, Sweden.
Funding
Open Access funding provided by Uppsala University.
Author information
Authors and Affiliations
Contributions
S.F. and R.F. planned the study and S.F. executed the study protocol. S.F. and R.F. analysed the results and drafted the manuscript. S.F. and R.F. approved the final manuscript before submission.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Franzén, S., Frithiof, R. Pre-treatment with the angiotensin receptor 1 blocker losartan protects renal blood flow and oxygen delivery after propofol-induced hypotension in pigs. Sci Rep 10, 17924 (2020). https://doi.org/10.1038/s41598-020-74640-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-020-74640-6
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
