
Abstract
Acute lymphoblastic leukaemia (ALL) is the most common childhood cancer and has a high survival rate when properly managed. Prognosis is correlated with many factors such as age, gender, white blood cell (WBC) count, CD10, French-American-British (FAB) classification, and many others. Many of these factors are included in this study as they play a major role in establishing the best treatment protocol. This study aims to demonstrate clinical and laboratory features of childhood ALL in Syria. They were treated at Children’s University Hospital, the only working major cancer centre in Syria at the time of the study. Data of 203 patients who aged 0–14 years were obtained for this study. Most patients (48.8%) aged (5–9) years with a male predominance (60.9%). The major features for ALL included lymphadenopathy (82.9%), presenting with systemic symptoms (74.9%), T-ALL subclass (20.2%), L2 FAB classification (36.1%), low educational levels for fathers (53%) and mothers (56.2%), having a high risk (48.4%), and having a duration of symptoms before evaluation for more than 4 weeks (42.6%). Only three (1.5%) patients had normal full blood counts (FBC) and only one (0.5%) patient had an isolated high WBC count at time of presentation. Most patients had either abnormal platelet count (89.3%) or low haemoglobin level (88.8%) when presenting with only (2.0%) having normal levels for both. This suggests that having normal haemoglobin and platelet count can be used for quick screening in crisis time like in Syria for prioritising patients. Many prognostic factors were significantly different from medical literature which emphasises the importance of local studies in the developping countries. This study included a high prevalence of T-all, L2 FAB classification, high-risk and other variables which require further studies to evaluate the aetiology of these features, especially that treatment protocols may have a higher mortality in developing countries when not adjusted to local variables.
Similar content being viewed by others
Introduction
Acute lymphoblastic leukaemia (ALL) is the most common cancer in childhood, with a prevalence up to 25% of cancers in children who are under the age of 15 years1. Although ALL is curable, many parts of the world may not have access to modern treatment. Approximately eight to nine of every ten children that have ALL are considered long-term survivors and cured in developed countries, but these reults markedly differ in developping countries2,3. These positive outcomes are due to having access to top treatments at the most advanced institutions2. Although the five-year survival rate is 93.5% when using the newest protocols and top chemotherapy, some cases of relapse still occur4. Nevertheless, top treatment cannot be accessed by all countries as many factors may get involved such as resource scarcity5. Few studies were concerned with paediatric ALL in the Middle East6. Little is known about childhood ALL in the Middle East and further studies are needed to establish standard data for future regional collaborative research as it provides a baseline for future protocols in ALL as they needed to be adjusted to the local variables. This raises a challenge as it is not easy to conduct medical research such as medical trials in developing countries due to the unavailability of porper funding and institutions which makes this quite challenging. In this article, the epidemiology and characterstics of ALL patients along with ALL variables such as prognostic risk and subtype are studied. Our study aims to define the risk factors and features associated with ALL in Syria.
Materials and methods
Study design
Our cross-sectional study was conducted in the Children’s University Hospital of Damascus University. The data was collected from patients’ records and covered the period between 21st August 2017 and 21st August 2018. This hospital is the major paediatric cancer centre among two centres in Syria and provides free healthcare to patients. The other centre was in Aleppo and was not working properly in the study period due to the conflict in Aleppo, resulting in most of leukaemia cases to be referred to Damascus.
Sampling and data collecting
This study included children with ALL who aged 0 to 14 years. ALL was diagnosed before initiating chemotherapy by bone marrow aspiration and immune phenotyping. Information was obtained from the hospital’s records which were taken by the physicians at time of diagnosis and information was provided by the child’s caregiver.
Demographics and family history
Data about general characteristics of patients such as age, gender, and province of origin was recorded (Table 1). Caregivers were asked by hospital physicians to determine the history of cancer and leukaemia in the family. Family history was obtained based on the family of the affected child having malignancies in their direct family.
French-American-British (FAB) classification
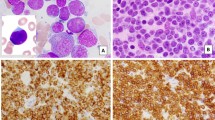
A skilled professor in haematology was involved in determining FAB classification7 for each ALL patient whether it was L1, L2 or L3. As FAB does not have independent prognostic significance and it is subjective, it is no longer recommended1. FAB classification was the first classification for ALL8, and it is based on morphology and cytochemical staining. However, it remains effective despite cytogenetic tests as it can add diagnostic accuracy in some cases9 Furthermore, using FAB system is convenient in developing countries as it is easy to conduct in regular labs and does not require much resources10. It is also used when there is no alternative which is why it is used in Syria.
Risk determination
Berlin-Frankfurt-Münster (BFM) risk groups determination was used1. However, in this study standard and intermediate risk groups were merged into one group that has both characteristics and treated as intermediate risk. This change is more convenient due to lack of resources to determine the genes and it is easier for management and application. In addition, long-term treatment response was beyond this study scope.
Patient’s prognostic risk was defined as standard or high. Poorer prognosis is correlated with age of younger than 1 year and older than 10 years, white blood cell (WBC) count higher than 50 × 109 cells/L at time of diagnosis, extramedullary disease, biologic and cytogenetic changes such as having Philadelphia chromosome, T-ALL, positive cerebrospinal fluid (CSF) and testicular involvement, inability to tolerate standard chemotherapy, slow-rate response to initial therapy, the speed and how low leukemia cell count drops after initial therapy, minimal residual disease (MRD) and bone marrow aspiration and FAB determination in the beginning of treatment; these were all considered in the determination of each patient’s prognosis to conduct the correct chemotherapy protocol8. MRD was determined by a blood smear on day 8 and steroid response.
Patients with hereditary risk factors such as Down syndrome, neurofibromatosis, Bloom syndrome, Fanconi anemia, ataxia telangiectasia, Li-Fraumeni syndrome, and constitutional mismatch repair deficiency were excluded from this study.
Definitions
Systemic symptoms were defined as having fever, anorexia, weight loss, or fatigue. Chest x-ray (CXR) was considered positive when it had a mediastinal enlargement or hilar lymphadenopathy. WBC count of (1.5–11.5 × 109 cells/L), haemoglobin level of (11–16 g/dL), and platelet count of (150–400 × 109 cells/L) were considered normal. A positive family history is when a direct family member has a history of malignancy, regardless of type of cancer or age of presentation.
We defined having a positive CD10 as having 21% or higher CD10 on flow cytometry. Educational levels were divided into 3 groups as in Syria these three groups tend to significantly differ; low education level is for a parent whose higher degree is elementary or lower, medium educational level is when the highest degree is the ninth or 12th grade, and finally high educational level is when having a university degree or higher.
Genetic testing
No routine genetic testing was conducted due to unavailability of resources and other countries boycot the high-tech materials and medications which made them very expensive for the government to obtain for this centre. However, genetic testing was, conducted when a hereditary syndrome was highly suspected and therefore these patients could be excluded from this study, but genes prevalence such as Philadelphia gene is not valid to use in this study as genetic testing is not routinely done, and therefore the data was not retrieved.
Consent and ethical approval
Informed written consent was taken before using and publishing the data. It was taken from the parent and/or the legal guardian of the child. The study was approved by the ethics committee of Damascus University. We confirm that all research was performed in accordance with relevant guidelines/regulations.
Data analysis
Data was processed by the software IBM SPSS version 26 for Windows (SPSS Inc, IL, USA). The statistical analysis used was Chi-square test for determination of statistical significant differences within the groups. We measured odds ratios (ORs) and the 95% confidence intervals when comparing groups by using Mantel–Haenszel test by using the same software. When two-tailed P value was less than 0.05, the results were considered to be statistically significant.
Results
Characteristics of the sample
Our study was conducted on 203 ALL patients who aged (0–14) years. The peak age in our study was (5–9) years comprising 48.5% of the cases with a male predominance (60.9%). Characteristics of ALL children in Syria, including gender, age, geographic distribution, parents’ educational level, main presenting symptom, hepato-splenomegaly, lymphadenopathy, ALL-subtype, haemoglobin, WBC and platelet count when diagnosed, CXR, CD10, FAB classification and prognostic risk are demonstrated in (Table 1). Patients distribution in Syrian provinces is shown in (Fig. 1) according to the province of origin.

Showing age, gender, and province of origin for ALL patients.
Date of the full blood count (FBC) of 197 patients was recorded; only three (1.5%) patients had normal FBC (normal haemoglobin, WBC count and platelet counts) when diagnosed and only one (0.5%) patient had an isolated high WBC count with normal haemoglobin and platelet counts. However, only 21 (10.7%) patients had normal platelet counts, only 22 (11.2%) patients had normal haemoglobin, and only four (2.0%) of the patients having normal haemoglobin and platelet counts when diagnosed.
Having systemic symptoms (74.9%), anaemia (88%) with 35% having severe anaemia, low platelet count (87.4%) with 25.3% having platelet count lower than (20 × 109 cells/L), lymphadenopathy (82.9%), and hepato-splenomegaly (73.9%) were the most frequent observations in our study.
Variables according to gender
Comparison between males and females with ALL characteristics is demonstrated in Table 2. T-ALL was more frequently correlated with male gender P = 0.0019 (OR, 3.750; 95% CI 1.565–8.986). Lymphadenopathies were less common in females comparing to males P = 0.0286 (OR, 0.439; 95% CI 0.208–0.928) and males had a longer duration of symptoms before evaluation (more than 4 weeks) when compared to females P = 0.0145 (OR, 2.054; 95% CI 1.149–3.671). No statistically significant difference was found when comparing gender with having family history, parents’ educational levels, hepato-splenomegaly, haemoglobin, WBC and platelet count, CXR, CD10 positivity, prognostic risk and FAB classification (P > 0.05). Classification and ALL subtype according to province of origin are demonstrated in Fig. 2.

Showing gender, province of origin, subtype, FAB classification of ALL patients, and risk.
Variables according to age groups
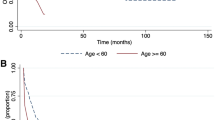
Comparison between age groups with characteristics of ALL is demonstrated in Table 3. T-ALL was found more frequently than B-ALL in the oldest age group (10–14) when compared with the age group (5–9) P = 0.0030 (OR, 3.690; 95% CI 1.529–8.929) or with the age group (0–9) P = 0.0001 (OR, 4.975; 95% CI 2.160–11.494). The prognostic risk was found to be higher in older patients (10–14) than the younger patients (5–9) P = 0.0001 (OR, 7.500; 95% CI 2.405–23.386) and the youngest patients (0–9) P < 0.0001 (OR, 8.492; 95% CI 2.812–25.643). CD10 was found to be negative more frequently in the age group (0–9) when compared with (10–14) age group P = 0.0146 (OR, 0.352; 95% CI 0.149, 0.833).
L2 was found more frequently than L1 in (10–14) age group when compared with (5–9) age group P = 0.0488 (OR, 2.567; 95% CI 0.991–6.649) or with (0–9) age group P = 0.0252 (OR, 2.702; 95% CI 1.108–6.588). Less hepato-splenomegaly was found in the older age group (10–14) when compared with the younger age group (5–9) P = 0.0090 (OR, 0.324; 95% CI 0.136–0.771) or with the age group (0–9) P = 0.0076 (OR, 0.344; 95% CI 0.154–0.770). However, no statistically significant difference was found when comparing gender, duration of symptoms before evaluation, haemoglobin, WBC and platelet count, CXR, parents’ educational level, lymphadenopathy, or family history with any age group (P > 0.05).
Variables according to ALL subtype
Comparison between T-ALL and B-ALL with characteristics of ALL is demonstrated in Table 4. WBC count was found to be less frequently higher than normal (higher than 11 × 109 cells/L) in B-ALL P < 0.0001 (OR, 0.200; 95% CI 0.083–0.482). However, haemoglobin was found to be more frequently low in B-ALL patients P = 0.0012 (OR, 4.421; 95% CI 1.723–11.345). CXR was found to be less positive in B-ALL P < 0.0001 (OR, 0.109; 95% CI 0.046–0.259). CD10 was found to be more frequently positive in B-ALL patients P < 0.0001 (OR, 32.500; 95% CI 12.462–84.755) and prognostic risk to be lower in B-ALL patients P < 0.0001 (OR, 0.016; 95% CI 0.002–0.122). L1 was found less frequently in T-ALL patients P = 0.0401 (OR, 0.432; 95% CI 0.192–0.974). No statistically significant difference was found between T-ALL and B-ALL when compared with family history, parents’ educational level, hepato-splenomegaly, time until diagnosis, and platelet count P > 0.05.
Variables according to risk group
Comparison between high risk and low risk patients with characteristics of ALL is demonstrated in Table 5. Positive family history was found more frequently in patients with standard risk P = 0.0438 (OR, 2.916; 95% CI 0.992–8.570). However, CD10 was found less frequently in patients with high risk P < 0.0001 (OR 0.129; 95% CI 0.050–0.331) and L2 was found more frequently in patients with high risk P = 0. 0227 (OR 2.267; 95% CI 1.114–4.613). No statistically significant difference when comparing patient risk with their parents’ educational level (P > 0.05).
Variables according to FAB classification
Comparison between L1 and L2 patients with characteristics of ALL is demonstrated in Table 5. CD10 was found less frequently positive in L2 patients P = 0.0143 (OR 0.361; 95% CI 0.157–0.829) and L2 patients had a higher probability of having a father with high educational level P = 0.0307 (OR 3.422; 95% CI 1.096–10.690). However, no statistically significant difference was found when comparing L1 and L2 with haemoglobin, WBC and platelet count, mother educational level and family history.
Other variables
Having hepato-splenomegaly was more frequently correlated with high WBC count P = 0.0055 or with abnormal WBC count P = 0.0057, and with higher rate of low platelets P = 0.0095 or abnormal platelet P = 0.0079 compared with normal platelets. Lymphadenopathy was found to be correlated with high WBC count P = 0.0123 or abnormal WBC count P = 0.0144, and with higher prognostic risk P = 0.0418. In patients with low platelets (less than 150 × 109 cells/L), having hepato-splenomegaly was found to be more frequently correlated with even lower platelet count (less than 20 × 109 cells/L) P = 0.0452.
Discussion
Age and gender
The mean age group of our study is slightly older than the (3–6) years reported by the Multi-Institutional International Collaborative Study (CALLME1) by the Middle East Childhood Cancer Alliance (MECCA) in which they comprised 33.8%6, older than what was found in the US of (1–4) years comprising (42.9%)11,12, and one international study that covered 184 countries which found the peak age to be (0–4) years13, but was close to the age reported in the Tehran study with a mean age of 5.5 years14 and a Brazilian study which had the average age of diagnosis of 6.3 ± 0.5 years15. Gender ratio of M/F in our study was (1.56:1) which was slightly higher than the CALLME1 study (1.4:1), the US study (1.35:1), the international study (1.4:1), and the Tehran study (1.32:1), but lower than what was found in the Brazilian study (1.9:1) but there was no significant difference (P > 0.05) when comparing our study with all previous studies.
Symptoms, FBC and organomegaly
Most patients presented with systemic symptoms (74.9%) similar to the Tehran study in which the patients had fever (51.2%), organomegaly (31.4%) and pallor (19.2%) and to the Brazilian study which found that hepatomegaly, splenomegaly, fever and lymphadenopathy were the most common clinical features. Most patients (42.6%) in our study required more than 4 weeks to get diagnosed which was similar to the CALLME1 study which found that the mean time before evaluation to be 1.35 months. However, in our study (25.9%) of patients needed less than 2 weeks to get evaluated.
Having systemic symptoms, anaemia which is usually severe, low platelets, lymphadenopathy, and hepato-splenomegaly were the most frequent observations in most of our patients similar to many studies, but with different prevalence such as the CALLME1 study where the prevalence was for fever (75.5%), pallor (79.2%), lymphadenopathy (62.6%) (P = 0.0001 when compared to our study), hepatomegaly (59.5%), and splenomegaly (60.8%), and the Brazilian study where the prevalence was for anaemia (85%) with (35%) having severe anaemia of Hb < 7 g/dl (P > 0.05), low platelet counts of less than (100 × 109 cells/L) in (65%) of the patients with (10.5%) having platelet counts less than (20 × 109 cells/L) (P = 0.0177), lymphadenopathy (43.4%) (P = 0.0003 when comparing these numbers to our study), hepatomegaly (63%), and splenomegaly (57.8%). Our study had significantly higher prevalence of the aforementioned factors when comparing to these studies.
The most frequent haemoglobin level group in our study was (11–7 g/dL) and platelet count group was (50–150 × 109 cells/L). These were within ranges of CALLME1 study where mean haemoglobin level was (7.9 g/dL) and platelet count mean was (66.1 × 109 cells/L) and the Brazilian study where mean haemoglobin level was (8.24 g/dL). However, high WBC count was only found in half of our sample which is similar to what was found in the Brazilian study where the average WBC counts at diagnosis was (31.8 × 109 cells/L).
ALL has many factors for negative prognosis such as high WBC count when presenting, CD10 negativity, lymphadenopathy and having extra-medullary disease1. Most patients in our study had either abnormal platelet counts or low haemoglobin level when diagnosed with only (2.0%) of the patients having normal levels for both which means that they can be used when patients presenting with ALL is speculated at crisis time such as the war in Syria to prioritise patients; Our findings are similar to what was found in Brazil where (4%) of the patients had normal FBC (P > 0.05 when comparing to this study). Positive findings on CXR were found in (18.4%) in our study which was higher than what was found in the Brazilian study (11.8%) (P > 0.05 when comparing to this study). Other prognostic factors include age, gender, and race1. Patients in the older age group (10–14) were found to have a worse prognostic risk (85.7% of them had high risk). However, most studies showed a good prognosis for the age group (1–9)1.
Other variables
Overall, parents’ educational level was low in ALL patients as more than the half of fathers and mothers had low educational level. Positive family history in our study was lower than in the Tehran study (16.3%) (P > 0.05). In our study, high-risk patients had more positive family history, but more negative CD10 and higher prevalence of L2. Moreover, L2 was also correlated with more negative CD10, higher parents’ educational level and worse prognostic risk. This finding is similar to a study which found that high educational level of mothers was associated with higher risk of ALL16.
T-ALL and lymphadenopathies were more commonly found in males (82.5% of T-ALL cases were males). However, males required a shorter period before evaluation which could reflect that symptoms might have been more severe with males. T-ALL, high risk category and L2 were also found more frequently in the older patients, reflecting a poorer prognosis in these patients. High WBC count at diagnosis, high risk and more findings on CXR were found more in T-ALL patients than B-ALL, but lower haemoglobin in B-ALL patients was more frequent than T-ALL. L2 was also found more frequently in T-ALL patients.
T-ALL is known to affect males more than females which can explain that being a male was correlated with a higher risk17 although L1 and L2 affected both genders equally in our study (P > 0.05), and L2 was also correlated with a poorer prognosis. FAB classification in our patients showed a higher rates of L2 and L3 (P = 0.0001 when comparing our result with other studies) in comparison with the CALLME1 study where FAB classification was L1 = 77.4%, L2 = 20.4% and L3 = 21%, and with a Brazilian study L1 = 83% and L2 = 17%15, but L1 incidence in our study was close to what was found in Tehran L1 = 57.6% and L2 + L3 = 42.4% (P > 0.05). However, another study found that L1 accounted for (85–89%) of the cases, L2 (14.1%) and L3 (0.8%)18.
T-ALL prevalence in our study was higher than the CALLME1 study where T-ALL = 14.8% (P = 0.079 when comparing these two studies), and the Brazilian study where T-ALL = 10.5% (P = 0.0867 when comparing these two studies) which reflect multiple factors that could be affecting these findings. Higher risk patients were more frequent in Syria (48.4%) than what was found in the CALLME1 study where high risk patients comprised (36.0%) (P = 0.0108) and what was found in Brazil where high risk patients comprised (46%) (P > 0.05). Therefore, ALL patients in Syria have more frequently poor prognosis which could be due to other factors being involved in the period of the study such as the war. T-ALL is known for its poorer prognosis12,19. This all could explain the very high prevalence of high-risk ALL in Syria as these poor prognostic factors had a higher prevalence when comparing our study with other studies. It is crucial to study all prognostic factors to conduct an adequate treatment plan, so that patients are not under- or overtreated20. All the prognostic factors should be determined prior to treatment as an intense treatment protocol can eliminate the effect of some of the unfavourable factors and decrease relapse as protocols differ among risk groups1,21,22. T-ALL and L3 (Burkett) incidence can be related to virus exposure23. Using FAB system is convenient in developing countries as it is easy to conduct in regular labs and does not require much resources10, and it remains effective despite cytogenetic tests as it can add diagnostic accuracy in some cases9. L2 was found to have a higher relapse and mortality rate18 which is similar to our finding of L2 being correlated with higher risk. A weak or negative CD 10 expression is correlated with ZNF384, and KMT2A in blasts which often express high levels of FLT3 rearrangement, t(4;11)(q21;q23) in particular which accompanies a poorer outcome1. However, leukemic cells which demonstrate a germline of KMT2A gene configuration are correlated with positive CD10 expression in precursor-B ALL and have a better outcome1. Nevertheless, CD10 prognostic significance independently from KMT2A rearrangement is not clear1.
The much higher L2 and high risk prevalence comparing to other studies may reflect an underlying cause, such as from war or environment as many practices in Syria may contain leukemogenesis such as unprotected pesticide usage, mate drinking and hookah smoking, mainly in low educational level population24. It is suggested that the protocols that were developed in the advanced centres might increase the rate of death as these protocols are not adjusted to the local conditions of low- and mid-income countries2,3, and therefore more studies are required in developing countries such as Syria for adjustment of protocols that change ALL variables. Although the cost of treatment in Syria is covered, there is data suggesting that families within low SES are correlated with worse prognosis in children as determination of indirect costs is difficult8 which can explain having lower educational parents was correlated with poorer prognosis in our study.
In conclusion, in this study we have discussed multiple features and risk factors of ALL and compared characteristics of ALL children in Syria in the Middle East with multiple studies from the Middle East and multiple regions across the globe. The data covered most aspects of ALL and its prevalence in addition to factors which are correlated with worse prognosis such as L2 FAB classification, negative CD10, male gender, T-ALL, and low parental educational level. The results suggest high T-ALL, L2, and high risk prevalence which could reflect underlying factors and poor survival rates, especially that treatment protocols may have a higher mortality in developing countries when not adjusted to local variables. The results also suggests that having normal haemoglobin and platelet count can be used for quick screening in crisis time like in Syria for prioritising patients.
This is the first detailed study to demonstrate the epidemiology of ALL in Syria and its relation to other factors. It also suggests common risk factors that might worsen the prognosis while comparing with multiple studies from different countries. This study was also conducted at war-torn Syria which also could be the factor for this phenomenon. It also enforces the significance of FAB classification and its relation to higher risks of ALL. The different findings also enforce the importance of local studies in developping countries as they might have considerably different factors than the developed countries.
Data availability
Data will be available on request from the corresponding author.
References
Childhood Acute Lymphoblastic Leukemia Treatment (PDQ(R)): Health Professional Version, in PDQ Cancer Information Summaries. Updated on February 6, 2020: Bethesda (MD).
Rivera, G. K. & Ribeiro, R. C. Improving treatment of children with acute lymphoblastic leukemia in developing countries through technology sharing, collaboration and partnerships. Expert Review of Hematology 7(5), 649–657 (2014).
Abdelmabood, S. et al. Treatment outcomes of children with acute lymphoblastic leukemia in a middle-income developing country: high mortalities, early relapses, and poor survival. Jornal de Pediatria 96(1), 108–116 (2020).
Pui, C.-H. & Evans, W. E. A 50-Year Journey to Cure Childhood Acute Lymphoblastic Leukemia. Seminars in Hematology 50(3), 185–196 (2013).
Mosadeghrad, A. M. Factors Affecting Medical Service Quality. Iran J Public Health 43(2), 210–20 (2014).
Al-Mulla, N. A. et al. Childhood acute lymphoblastic leukemia in the Middle East and neighboring countries: A prospective multi-institutional international collaborative study (CALLME1) by the Middle East Childhood Cancer Alliance (MECCA). Pediatric Blood & Cancer 61(8), 1403–1410 (2014).
Zafar, M. N. FAB classification of acute lymphoblastic leukaemia (ALL) and its relevance to ALL in Karachi children. J Pak Med Assoc 35(8), 233–6 (1985).
Terwilliger, T. & Abdul-Hay, M. Acute lymphoblastic leukemia: a comprehensive review and 2017 update. Blood Cancer Journal 7(6), e577–e577 (2017).
Sachdeva, M. U. et al. Role of FAB classification of acute leukemias in era of immunophenotyping. Indian J Pathol Microbiol 49(4), 524–7 (2006).
Angelescu, S. et al. Value of multifaced approach diagnosis and classification of acute leukemias. Maedica (Buchar) 7(3), 254–60 (2012).
Siegel, D. A. et al. Rates and Trends of Pediatric Acute Lymphoblastic Leukemia — United States, 2001–2014. MMWR. Morbidity and Mortality Weekly Report 66(36), 950–954 (2017).
Howlader N, N.A., Krapcho M, Miller D, Brest A, Yu M, Ruhl J, Tatalovich Z, Mariotto A, Lewis DR, Chen HS, Feuer EJ, Cronin KA (eds). SEER Cancer Statistics Review, 1975-2016, National Cancer Institute. Bethesda, MD,. Available from, https://seer.cancer.gov/csr/1975_2016/.
Miranda-Filho, A. et al. Epidemiological patterns of leukaemia in 184 countries: a population-based study. The Lancet Haematology 5(1), e14–e24 (2018).
Azim Mehrvar, M. F., et al. Epidemiological Features of Childhood Acute Leukemia at MAHAK’s Pediatric Cancer Treatment and Research Center (MPCTRC), Tehran, Iran. BCCR Journal (2015).
Lustosa de Sousa, D. W. et al. Acute lymphoblastic leukemia in children and adolescents: prognostic factors and analysis of survival. Revista Brasileira de Hematologia e Hemoterapia 37(4), 223–229 (2015).
Kaye, S. A. et al. Maternal reproductive history and birth characteristics in childhood acute lymphoblastic leukemia. Cancer 68(6), 1351–1355 (1991).
Dores, G. M. et al. Acute leukemia incidence and patient survival among children and adults in the United States, 2001-2007. Blood 119(1), 34–43 (2012).
Miller, D. R. et al. Prognostic Importance of Morphology (FAB Classification) in Childhood Acute Lymphoblastic Leukaemia (ALL). British Journal of Haematology 48(2), 199–206 (1981).
Holmes, L. et al. Age Variance in the Survival of United States Pediatric Leukemia Patients (1973–2006). ISRN. Public Health 2012, 1–10 (2012).
Pui, C.-H. Acute lymphoblastic leukemia in children. Current opinion in oncology 12(1), 3–12 (2000).
Pui, C.-H. et al. Outcome of treatment for childhood cancer in black as compared with white children: the St Jude Children’s Research Hospital experience, 1962 through 1992. Jama 273(8), 633–637 (1995).
Freyer, D. R. et al. Postrelapse survival in childhood acute lymphoblastic leukemia is independent of initial treatment intensity: a report from the Children’s Oncology Group. Blood 117(11), 3010–3015 (2011).
Oliveira, P. D., de Carvalho, R. F. & Bittencourt, A. L. Adult T-cell leukemia/lymphoma in South and Central America and the Caribbean: systematic search and review. International Journal of STD & AIDS 28(3), 217–228 (2016).
Kakaje, A., et al. Breastfeeding and acute lymphoblastic leukaemia: Potential leukemogenesis in children in developing countries. Available at SSRN: https://ssrn.com/abstract=3517418 or http://dx.doi.org/10.2139/ssrn.3517418 (January 10, 2020)
Acknowledgements
We would like to thank Prof Lina Khouri for her help and support during this study.
Author information
Authors and Affiliations
Contributions
A.K. Conceptualization; Data curation; Formal analysis; Investigation; Methodology; Project administration; Supervision; Validation; original draft; Writing - review & editing. M.A. Data curation; Formal analysis; Software; original draft; Writing - review & editing. A.G. Software; Methodology; Conceptualization; Validation; Writing editing; investigation. B.K. Software; Methodology; Conceptualization; investigation. B.M. Software; Project administration; Conceptualization; Writing editing; investigation. B.Z. Software; Project administration; investigation. O.H. Project administration; Resources; Validation.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Kakaje, A., Alhalabi, M.M., Ghareeb, A. et al. Rates and trends of childhood acute lymphoblastic leukaemia: an epidemiology study. Sci Rep 10, 6756 (2020). https://doi.org/10.1038/s41598-020-63528-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-020-63528-0
This article is cited by
-
Fatigue in children who have recently completed treatment for acute lymphoblastic leukemia: a longitudinal study
Health and Quality of Life Outcomes (2024)
-
Making sense of the cancer journey: Pediatric cancer survivors’ and their parents’ autobiographical memories
Journal of Cancer Survivorship (2024)
-
Long-term response to autologous anti-CD19 chimeric antigen receptor T cells in relapsed or refractory B cell acute lymphoblastic leukemia: a systematic review and meta-analysis
Cancer Gene Therapy (2023)
-
Relationship between cardiac mechanical properties and cardiac magnetic resonance imaging at rest in childhood acute lymphoblastic leukemia survivors
The International Journal of Cardiovascular Imaging (2023)
-
Excessive vincristine exposure in a child being treated for acute lymphoblastic leukaemia with underlying Dubin–Johnson syndrome: a case report
Cancer Chemotherapy and Pharmacology (2023)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
