
Abstract
Adiponectin is a prime determinant of the status of insulin resistance. Association studies between adiponectin (ADIPOQ) gene single nucleotide polymorphisms (SNPs) and metabolic diseases have been reported earlier. However, results are ambiguous due to apparent contradictions. Hence, we investigated (1) the association between ADIPOQ SNPs: −11377C/G, +10211T/G, +45T/G and +276G/T for the risk towards type 2 diabetes (T2D) and, (2) genotype-phenotype association of these SNPs with various biochemical parameters in two cohorts. Genomic DNA of diabetic patients and controls from Gujarat and, Jammu and Kashmir (J&K) were genotyped using PCR-RFLP, TaqMan assay and MassArray. Transcript levels of ADIPOQ were assessed in visceral adipose tissue samples, and plasma adiponectin levels were estimated by qPCR and ELISA respectively. Results suggest: (i) reduced HMW adiponectin/total adiponectin ratio in Gujarat patients and its association with +10211T/G and +276G/T, and reduced ADIPOQ transcript levels in T2D, (ii) association of the above SNPs with increased FBG, BMI, TG, TC in Gujarat patients and (iii) increased GGTG haplotype in obese patients of Gujarat population and, (iv) association of −11377C/G with T2D in J&K population. Reduced HMW adiponectin, in the backdrop of obesity and ADIPOQ genetic variants might alter metabolic profile posing risk towards T2D.
Similar content being viewed by others


Introduction
Metabolic Syndrome (MS) is the new wave of diseases that has hit the human population in the last few decades- the Metabolic Syndrome Era. It has become pandemic and with obesity and type 2 diabetes (T2D) clubbed under the MS umbrella, millions of people around the globe have come under its grip. Though obesity and T2D are ubiquitous, there exists a pattern of prevalence based on ethnicity. A recent report has identified demographic transitions, nutrition and lifestyle in the backdrop of genetic predisposition as the chief factors responsible for the rising trend of obesity associated amongst South Asians1. Over accumulation of visceral adipose tissue (AT) has been identified as one of the major driving factors towards T2D. Adipose tissue is an important regulator of metabolic homeostasis by virtue of the adipokines (pro-inflammatory and anti-inflammatory) that it secretes. In obese conditions, the fine-tuned balance between the pro- and anti-inflammatory adipokines gets altered leading to various metabolic disorders2. These bioactive peptides act locally and distally to calibrate and fine tune various metabolic pathways. Adiponectin is one such calibrator which is abundantly expressed in white adipose tissue3. It circulates in three polymorphic forms, low molecular weight (LMW), moderate molecular weight (MMW) and high molecular weight (HMW). Interestingly, the ratio of plasma HMW adiponectin to total adiponectin is more strongly correlated with plasma glucose levels than any of the forms alone4. Adiponectin gene (ADIPOQ/APM1/GBP28) locus, 3q27, has been strongly associated with a variety of metabolic disorders like- impaired glucose tolerance, obesity, dyslipidemia and T2D5,6,7. Studies undertaken on different ethnic groups have shown positive association of certain SNPs of the adiponectin gene with T2D3,8,9,10,11. However, T2D being a multi-factorial and polygenic metabolic disorder12, significant variations have been reported concerning the genetic architecture underlying T2D amongst different ethnic populations13,14. The SNPs to be studied were selected based on the following criteria: (1) validated SNPs for frequency in Genome Wide Association Studies (GWAS), (2) SNPs with scientific evidence for their role in augmented protein synthesis. ADIPOQ comprises of 2 introns and 3 exons encoding for the 30 kDa adiponectin protein15. Four SNPs were studied, −11377C/G (rs266729) in promoter, +10211T/G (rs17846866) in intron 1, +45T/G (rs2241766) in exon 2 and +276G/T (rs1501299) in intron 2, to examine their association with T2D. Since Indian population is relatively non-homogenous, we conducted our study in native Gujarat, and Jammu and Kashmir (J&K) population independently. We also aimed to study the genotype-phenotype association of the above-mentioned SNPs with Fasting Blood Glucose (FBG), Body Mass Index (BMI), plasma lipid profile and T2D.
Materials and Methods
Study subjects
Two ethnically different populations of India, one from the western Indian state of Gujarat and another from the northern Indian state of J&K were included in the present study. This study was carried out in agreement with the Declaration of Helsinki as approved by the Institutional Ethical Committee for Human Research (IECHR), Faculty of Science, The Maharaja Sayajirao University of Baroda, Vadodara, Gujarat, India (FS/IECHR/2016-9) and Institutional Ethics Review Board (IERB), Shri Mata Vaishno Devi University, Katra, J&K, India (Smvdu/IERB/13/23). It was ensured that at least five previous generations of the study subjects were of the respective ethnicities. Blood collection camps were conducted to guarantee the involvement of all the socio-economic strata in the study. The importance of the study was explained to all the participants and written consent was obtained from all patients, and age and sex-matched control subjects. The study group of Gujarat population included 475 diabetes patients (211 males and 264 females) and 493 control subjects (250 males and 243 females) while, the study group of J&K included 507 diabetes patients (282 males and 225 females) and 300 controls (140 males and 160 females) between the age group of 30 to 67 years. The T2D patients recruited for the study displayed FBG > 125 mg/dL16. Patients suffering from autoimmune diseases or cancer were excluded from the study. Samples of visceral (omental) adipose tissue were taken from individuals of Gujarat population undergoing bariatric surgery and fasting clinical parameters of all the study subjects are as described previously17. A detailed family history of the patients was recorded based on a questionnaire to collect information on first- and second-degree relatives and their history of T2D. The controls selected showed FBG < 110 mg/dL with no prior history of T2D. They were healthy and disease or infection free. The study subjects included both obese and lean individuals and their BMI (weight in kg/height in m2) was calculated by recording height and weight.
Blood collection and DNA extraction
FBG levels were measured by prick method using glucometer (TRUEresult® - Nipro). Blood was obtained from diabetic and ethnically matched controls as per our previous study17. Plasma was used for lipid profiling and assaying plasma HMW adiponectin and total adiponectin levels. PBMCs were separated for DNA extraction by phenol-chloroform method. DNA was stored at −20 °C for further analysis.
Screening of ADIPOQ SNPs
Samples from Gujarat population were genotyped by polymerase chain reaction-restriction fragment length polymorphism (PCR-RFLP) for −11377C/G, +10211T/G and +276G/T. The PCR reaction mixture had a total volume of 20 µL as per our previous study17 with primer dependent annealing temperatures (Table S1). The amplified products were checked by electrophoresis on a 2.0% agarose gel stained with ethidium bromide. Details of the restriction enzymes (Fermentas, Thermo Fisher Scientific Inc., USA) and digested products are mentioned in Table S1. 15 μl of the amplified products were digested with 1U of the corresponding restriction enzyme in a total reaction volume of 20 μl as per the manufacturer’s instruction. The digestion products with 50 base pair DNA ladder (HiMedia, India) were resolved on 3.5% agarose gels stained with ethidium bromide and visualized under UV transilluminator i.e. E-Gel Imager Life Technologies (Fig. S1A–C) and uncropped images of the gels are as in Fig. S3. More than 10% of the samples were randomly selected for confirmation and the results were 100% concordant (analysis of the chosen samples was repeated by two researchers independently) and further confirmed by sequencing. ADIPOQ +45T/ G (rs2241766) SNP was genotyped by TaqMan real time PCR using the pre-designed assay ID c__26426077_10 for allelic discrimination, containing specific probes for each allele marked with VIC and FAM fluorescent dyes (ThermoFisher Scientific, USA). Real-time PCR was performed in 10 µl volume using LightCycler®480 Probes Master (Roche Diagnostics GmbH, Mannheim, Germany) following the manufacturer’s instructions. A no-template control (NTC) was used with the SNP genotyping assay. Samples with each genotype were analyzed together as an internal control. J&K samples were genotyped for −11377C/G (rs266729), +45T/G (rs2241766) and +276G/T(rs1501299) in a panel using High-throughput genotyping MassArray platform (SEQUENOM)18. The success rate of SNP genotyping was > 95%. As a quality control measure of SNP genotyping, three duplicate samples and a negative control was included in each 96 well plate. The concordance rate for genotyping was 99.5%. Further values for SNP +10211T/G (rs17846866) were imputed using CEU data from 1000 genome (Phase 3) as reference dataset and analyzed using PLINK ver 1.07 as the samples were exhausted.
Plasma parameters
In Gujarat population plasma total cholesterol (TC), triglycerides (TG), and high-density lipoprotein cholesterol (HDL-c) levels were measured using commercial kits (Reckon Diagnostics P. Ltd, Vadodara, India). Low-density lipoprotein cholesterol (LDL-c) was calculated using Friedewald’s (1972) formula19. Human total adiponectin and HMW adiponectin ELISA Kits (Elabioscience Biotechnology Inc., USA) with a sensitivity of 0.47 ng/mL and 3.75 ng/mL respectively were used to estimate the levels of total adiponectin and HMW adiponectin in patients and controls. The plasma samples used were freeze-thawed only once. All the plasma estimations were carried out in duplicates with % coefficient of variation within 10%. The plasma samples from J&K population were assayed for various biochemical parameters at a commercial clinical laboratory.
Determination of adiponectin transcript levels
RNA isolation and cDNA synthesis: Total RNA was isolated from visceral adipose tissue (VAT) using Trizol method. RNA integrity and purity were verified by 1.5% agarose gel electrophoresis/ethidium bromide staining and O.D. 260/280 absorbance ratio of 1.9 respectively. To avoid DNA contamination, RNA was treated with DNase I (Puregene, Genetix Biotech) before cDNA synthesis. Transcriptor High Fidelity cDNA Synthesis Kit (Roche Diagnostic GmbH, Mannheim, Germany) was used to prepare cDNA using one microgram of total RNA isolated, according to the manufacturer’s instructions in the Eppendorf Mastercycler gradient (USA Scientific, Inc., Florida, USA). The expression of ADIPOQ and GAPDH, IPO8 and ACTB (reference) transcripts were measured by Light-Cycler® 480 Real-time PCR (Roche Diagnostics GmbH, Manneheim, Germany) using gene- specific primers (Eurofins, Bangalore, India) as shown in Table S1. Real-time PCR was performed using Light-CyclerH 480 SYBR Green I Master (Roche Diagnostics GmbH, Mannheim, Germany) and carried out in the Light-CyclerH 480 Real-Time PCR (Roche Diagnostics GmbH, Mannheim, Germany) as per our previous study17.
Statistical analyses
The normally distributed data for baseline parameters were analyzed by unpaired t-test while Mann-Whitney test was used for data not following normal distribution. Evaluation of the Hardy-Weinberg equilibrium (HWE) was performed for all the SNPs in patients and controls by comparing the observed and expected frequencies of the genotypes using chi-square analysis. The distribution of the genotypes and allele frequencies of ADIPOQ SNPs for patients and control subjects were compared using the chi-square test with 2 × 2 contingency tables respectively using GraphPad Prism 5 software. The genotypes have been analyzed in an additive, dominant and recessive model as there was low genotype frequency of the homozygous minor alleles (<10% frequency). P values less than 0.0125 for genotype and allele distribution were considered as statistically significant as per Bonferroni’s correction for multiple testing. The strength of association of the ADIPOQ SNPs with the risk for T2D was assessed by odds ratio (OR) with 95% confidence intervals (CI). Haplotypes and linkage disequilibrium (LD) coefficients (D′ = D/Dmax) and r2 values for the pair of the most common alleles at each site were obtained using http://analysis.bio-x.cn/myAnalysis.php20. Association studies of SNPs with other parameters were performed using analysis of variance (ANOVA) and Kruskal Wallis test. Adjustments for the possible confounding effects of age, sex, and BMI were also done for the samples. Relative gene expression of ADIPOQ, and GAPDH, IPO8 and ACTB levels and fold change (2−∆∆Cp values) in T2D patients and control groups were plotted and analyzed by unpaired t-test. All the analyses were carried out in GraphPad Prism 5 software. P values less than 0.05 were considered significant for all the association studies. To predict the functional impact of non-coding polymorphisms, ENCODE prediction tool (https://www.encodeproject.org/) was employed21.
Results
Clinical parameters differed significantly between controls and patients in both the populations of Gujarat and J&K (Tables S2 and S3). Patients had significantly higher FBG (p < 0.0001). Moreover, obesity related factors like BMI, TC, TG and LDL-c were significantly elevated (p < 0.0001, p = 0.0360 and p = 0.001, respectively) while HDL-c was significantly decreased (p < 0.0001) in patients as compared to controls in Gujarat population while in the J&K population BMI (p = 0.015), FBG (p < 0.0001) and TG (p = 0.001) levels were significantly higher in T2D patients.
Association of ADIPOQ SNPs with T2D
The genotype and allele frequencies of the ADIPOQ SNPs are summarized in Table 1. The distribution of genotype frequencies for all the polymorphisms investigated was consistent with Hardy-Weinberg Expectations (HWE) (p > 0.05) in both the populations. Analysis of the genotype frequencies of +10211T/G (rs17846866) and +276G/T (rs1501299) SNPs using an additive model revealed them to be significantly associated (p < 0.0001) while the promoter 11377C/G (rs266729) and exonic +45T/G (rs2241766) SNPs were not associated with T2D (Table 1). Further, in Gujarat population a significant association was detected for the intron 1 +10211T/G (rs17846866) when analyzed in the recessive model (OR = 1.797, 95% CI = 1.369–2.359, p < 0.0001) with T2D. Likewise, the intron 2 + 276G/T (rs1501299) SNP was also found to be significantly associated in the recessive model (OR = 2.05, 95% CI, 1.57–2.65, p < 0.0001) as shown in Table 1. However, in J&K population, only promoter −11377C/G (rs266729) polymorphism was found to be associated (p = 0.0101; OR = 1.47, 95% CI = 1.09–1.96) with T2D in the recessive model (Table 1). The frequency of mutant alleles for +10211T/G (rs17846866) and +276G/T (rs1501299) was noted to be significantly higher in diabetic patients as compared to that of control subjects (OR = 2.33 and OR = 1.726, respectively) in Gujarat population.
Haplotype and linkage disequilibrium analysis of ADIPOQ SNPs
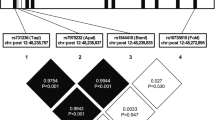
A haplotype evaluation of four polymorphic sites of ADIPOQ was performed in Gujarat population. The estimated frequencies of the haplotypes differed significantly between patients and controls (global p = 7.76 × 10−12) as shown in Table S4. The disease susceptible haplotypes were CGTG (p = 0.0003), CGTT (p = 6.32 × 10−5), GGTT (p = 0.0207) and GGTG (p = 0.0030) (Table S4). Furthermore, the GGTG (p = 3.87 × 10−5) haplotype in particular was found to be significantly higher in obese patients as shown in Table 2. The LD analysis revealed that the four SNPs investigated were in low to moderate LD association (Fig. S2). Haplotype and LD analyses were not performed in the J&K population as only −11377C/G (rs266729) was found to be associated with T2D and the genotypes of +10211T/G (rs17846866) were imputed.
ADIPOQ expression and plasma HMW adiponectin/total adiponectin ratio in patients and controls
A significant reduction in ADIPOQ transcript levels was observed in Gujarat T2D patients as compared to controls after normalization with GAPDH expression (p = 0.0187) as suggested by mean ∆Cp values (Fig. 1A). The 2−ΔΔCp analysis showed approximately 0.84 fold decrease in the expression of ADIPOQ transcript levels in patients as compared to controls (Fig. 1B). Similar results were obtained for ADIPOQ transcript levels when normalized with IPO8 (p = 0.0184) and ACTB (p = 0.0344) (Fig. S4A,C). The 2−ΔΔCp analysis of the same showed approximately 0.87 and 0.82 fold reduction in the expression of ADIPOQ transcript levels in patients as shown in (Fig. S4B,D). Further, there was no significant difference observed between ADIPOQ transcript levels and its SNPs (p > 0.05) as shown in Fig. 1C. Plasma HMW adiponectin and total adiponectin levels, and their ratio monitored in 37 controls and 45 patients showed significant decrease (p < 0.001) in Gujarat patients as compared to controls (Fig. 1D). Healthy females showed higher HMW adiponectin/total adiponectin ratio than healthy males (p < 0.001) (Fig. 1E). A significant drop in the ratio was observed in diabetic males and females when compared with their healthy counterparts (p < 0.05 & p < 0.01 respectively) (Fig. 1E). There was no significant reduction in the HMW adiponectin/total adiponectin ratio between healthy lean and obese individuals. However, the obese patients showed a significant drop compared to lean patients (p < 0.05) (Fig. 1F). Lean and obese diabetic individuals showed reduced HMW adiponectin/total adiponectin ratio as compared to their respective controls (p < 0.05, p < 0.01). The drop in the plasma adiponectin ratio was further accentuated in obese diabetic patients (p < 0.001) (Fig. 1F).

ADIPOQ transcript levels and plasma adiponectin levels in Gujarat population. (A) Relative gene expression of VAT ADIPOQ in controls and patients: Significant decrease in ADIPOQ transcript levels was observed in patients (Mean ∆Cp ± SEM: 1.639 ± 0.3829 v/s 6.681 ± 0.6558; p = 0.0187), (B) Relative fold change of ADIPOQ expression in controls and patients. Expression of ADIPOQ transcripts in T2D patients as compared to controls was decreased by 0.84 fold as determined by the 2-ΔΔCp method. (Controls n = 14; T2D patients n = 10). (C) Association of ADIPOQ polymorphisms with ADIPOQ transcript levels. No association between ADIPOQ polymorphisms and ADIPOQ transcript levels (p > 0.05). HMW adiponectin/total adiponectin ratio in (D) controls versus patients. Plasma HMW adiponectin/total adiponectin ratio in patients were significantly lower than in controls, (E) control and diabetic males and females. HMW adiponectin/total adiponectin ratio in control and patient females were significantly higher than in control and patient males and (F) lean (L) and obese (O) control and diabetic subjects. Obese patients showed significantly reduced HMW adiponectin/total adiponectin ratio (*p < 0.05, **p < 0.01, ***p < 0.001). (Controls n = 37; T2D patients n = 45).
Association of ADIPOQ SNPs and their genotypes with metabolic parameters and HMW adiponectin/total adiponectin ratio
As shown in Table 3, in Gujarat population, the GG genotype of −11377C/G was associated with increased levels of TG, LDL-c and HDL-c (females). The GG genotype of +10211T/G was significantly associated with FBG, BMI, TG, TC, HDL-c and HMW adiponectin/total adiponectin ratio while the TT genotype of +276G/T was significantly associated with increased FBG, BMI, TG, TC and LDL-c and, decreased HDL-c (p > 0.05). Further, +45T/G was not associated with any of the parameters in Gujarat population. However, no significant association of the metabolic parameters was observed with the polymorphisms in J&K population (Table S5).
Bioinformatics analyses
ENCODE data base showed that −11377C/G (rs266729), +10211T/G (rs17846866), +45T/G (rs2241766) and +276G/T (rs1501299) do not overlap with any cis-Response Elements (cREs) or display any cREs within 2 kb. Further, eQTL database GTex shows TG and GG genotypes of rs17846866 to have significantly reduced levels of plasma adiponectin similar to our findings. However, the eQTL data for the rest of the SNPs are not available. Analysis of rs2241766, a synonymous exonic SNP, revealed that the glycine residue at the 15th position remains unchanged (SIFT). Further, the change in codon usage was calculated by applying a relative synonymous codon usage (RSCU) approach to understand the relevance of ribosomal pause in reduced amount of protein being expressed. The delta Relative Synonymous Codon Usage (RSCU) value for the GGT to GGG codon change was calculated to be −0.31. However, no significant association of the +45T/G polymorphism was found with adiponectin levels.
Discussion
Our findings, for the first time, collectively suggest that ADIPOQ CGTG, CGTT, GGTT and GGTG haplotypes were associated with T2D, further GGTG was significantly associated with obesity induced T2D. Also, +10211T/G (rs17846866) and +276G/T (rs1501299) were strongly associated with obesity induced T2D susceptibility in Gujarat population; whereas in J&K population only −11377C/G (rs266729) was found to be associated with T2D. The difference in the association of variants can be attributed to the ethnic differences between the two populations. The findings in Gujarat population are further linked with reduced levels of HMW adiponectin and disease-associated risk factors like FBG, BMI and lipid parameters thereby suggesting their crucial role in metabolic disease susceptibility.
Obese phenotype has been associated with a reduction in the anti-inflammatory and a boost in the pro-inflammatory adipokines. Our previous reports suggest interleukin 1β (IL1β)22, resistin23 and TNFα24 to play an important role in the development of obesity, islet dysfunction and decreased insulin secretion. On the contrary, adiponectin2, omentin-125, melatonin26 and vaspin27 are known to enhance insulin sensitivity. The normal range of total adiponectin in healthy individuals is reported to be 2–20 µg/mL28. The characteristic short stature of South Asians combined with visceral adiposity leads to an increased weight per area distribution defined by body mass index predisposing those to metabolic diseases1,29,30,31. Genome-wide association studies have shown a close association between adiponectin, ADIPOQ SNPs, fasting hyperglycemia and various metabolic diseases though varying from population to population32,33,34. Earlier studies have shown promoter −11377C/G (rs266729) polymorphism to have a positive association with hypoadiponectinemia and risk of developing T2D35 and is supported by the findings in J&K population. As opposed to this, we found this SNP not to be associated with T2D or BMI in Gujarat population supporting the work by Schaffler et al. who also reported the absence of transcription factor binding sites at or around this SNP site36. However, the GG genotype of −11377 C/G (rs266729) did show an association with increased serum triglycerides and LDL-c, and reduced HDL-c in females. In spite of not being associated with T2D, possibly an indirect effect of other SNPs could be the reason for the observed altered association of the −11377 C/G (rs266729) with the serum lipid levels.
Adiponectin gene expression in an adipose tissue is regulated by a 34 bp enhancer located in the first intron37. Therefore, the finding of +10211T/G (rs17846866) located close to the enhancer in the region of the first intron affecting lipid metabolism and adiponectin levels in the present study is of significance. Though the ENCODE data base doesn’t show an overlap of this polymorphism with any cREs or display any cREs within 2 kb; eQTL database GTex shows TG and GG genotypes of +10211T/G (rs17846866) to have significantly reduced levels of plasma adiponectin similar to our findings. Additionally, this SNP is also seen to be associated with increased BMI, FBG, TG, TC and reduced HDL-c. To date, three independent studies, including ours, have established the association of +10211T/G (rs17846866) with three different Indian populations belonging to different demographical and geographical regions, thus further validating the significance of this SNP10,11. However, the results from J&K population did not reveal any such association. +45T/G (rs2241766) is a synonymous SNP with a codon change from GGT to GGG. Though studies on Chinese Han population found an association between +45T/G (rs2241766) and insulin resistance38; our results show no association between +45T/G (rs2241766) and T2D as supported by studies on Italian, French and Swedish populations3,8,9. We report a significant association of +276G/T (rs1501299) with T2D, and serum lipid profile in Gujarat population while no association was found in J&K population. Supporting our data from Gujarat population, similar results were obtained in earlier studies in German39, Swedish40, Italian Caucasian41, French Caucasian3 and South Indian populations35. However, the results of the study by Hara et al.42 in Japanese subjects were in accordance with the results obtained in J&K population. In Gujarat population, the TT genotype conferred approximately double risk for developing T2D against the GG genotype in +276G/T (rs1501299). Furthermore, +276G/T (rs1501299) is also found to be linked with increased BMI, FBG, TG, and TC, and reduced HDL-c in males. These findings also suggest the association of +276G/T (rs1501299) with Non-Alcoholic Fatty Liver Disease (NAFLD), co-morbidity associated with T2D as supported by Wang et al.43. Additionally, we have also found increased levels of TNFα, Free Fatty Acids (FFA) and resistin in obese patients17,44. Since TNFα is shown to be an important regulator of adiponectin multimerization45, our observations of increased TNFα, reduced adiponectin transcript and HMW adiponectin levels in obese patients are self-explanatory. We had also reported a rise in IL1β levels in obese diabetic patients46, asserting the rise in pro-inflammatory adipokine and drop in anti-inflammatory adipokine in obesity-associated low-grade inflammatory condition. Further, adiponectin levels show sexual dimorphism47 and our results further confirm this as females in general demonstrated a higher tendency of HMW adiponectin/total adiponectin ratio than males. Also, a significant drop in adiponectin ratio of lean diabetic individuals was observed which was further pronounced in obese diabetic patients. Moreover, the overall plasma HMW adiponectin/total adiponectin ratio tends to be lower in subjects with the homozygous mutant allele for +10211T/G (rs17846866) and +276G/T (rs1501299). In concordance with our findings, adiponectin levels were strongly and inversely associated with diabetes risk48,49. Alongside, we had also reported the prevalence of a significantly high number of angiotensin convertase enzyme (ACE) I/D polymorphism in the same population50. The ACE D allele has in particular been shown to be associated with increased angiotensin II51 which may be further adding to the down regulation of adiponectin. We suggest that the reduced HMW adiponectin in particular is responsible for insulin resistance as, among the adiponectin isoforms, the HMW isoform binds to its receptor with maximum affinity leading to a potent activation of 5′ AMP-activated protein kinase (AMPK). Thus, the lowered HMW adiponectin may be partly responsible for developing T2D52. The increased level of TG may be due to a decrease in the lipoprotein lipase activity and Very Low-Density Lipoprotein receptor (VLDLr) expression levels, which have been proposed to be modulated by adiponectin53. While HDL-c levels and their particle size are inversely correlated with the catabolic rate of apolipoprotein (ApoA-I), a direct role of reduced adiponectin with increased catabolism of the major ApoA-I present in HDL-c has been proposed54, explaining how hypoadiponectinemia leads to decreased HDL-c levels. The correlation between hypoadiponectinemia and reduced HDL-c levels, as observed by us further strengthens the hypothesis. To summarize, +10211T/G (rs17846866) and +276G/T (rs1501299) are significantly associated with increased FBG, BMI, TG, TC and reduced HMW adiponectin/total adiponectin ratio. More importantly, the haplotype analysis reveals that individuals with GGTG haplotype in particular show an increased tendency towards obesity induced T2D55 (Fig. 2). Thus, we may conclude that adiponectin gene is associated with T2D, nonetheless variation in the susceptibility loci within the gene depends on ethnic variation among different populations. However, further investigations to understand the mechanistic aspects of genetic variants regulating adiponectin levels are warranted in other cohorts.

Role of ADIPOQ SNPs in T2D: The ADIPOQ CGTT, GTTT and GGTG haplotypes in presence of ADIPOQ +10211T/G (rs17846866) and +276G/T (rs1501299) along with decreased transcript, plasma HMW adiponectin and total adiponectin, and increased TNFα, FFA, resistin leads to altered metabolic profile thereby contributing to insulin resistance and T2D in Gujarat population.
Data availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Change history
27 April 2020
An amendment to this paper has been published and can be accessed via a link at the top of the paper.
References
Misra, A. & Shrivastava, U. Obesity and dyslipidemia in South Asians. Nutrients 5, 2708, https://doi.org/10.3390/nu5072708 (2013).
Pramanik, S., Rathwa, N., Patel, R., Ramachandran, A. V. & Begum, R. Treatment avenues for type 2 diabetes and current perspectives on adipokines. Current Diabetes Reviews 14, 201, https://doi.org/10.2174/1573399813666170112142837 (2018).
Vasseur, F. et al. Single-nucleotide polymorphism haplotypes in the both proximal promoter and exon 3 of the APM1 gene modulate adipocyte-secreted adiponectin hormone levels and contribute to the genetic risk for type 2 diabetes in French Caucasians. Human Molecular Genetics 11, 2607, https://doi.org/10.1093/hmg/11.21.2607 (2002).
Lara-Castro, C., Luo, N., Wallace, P., Klein, R. L. & Garvey, W. T. Adiponectin multimeric complexes and the metabolic syndrome trait cluster. Diabetes 55, 249, https://doi.org/10.2337/diabetes.55.01.06.db05-1105 (2006).
Vionnet, N. et al. Genome wide search for type 2 diabetes–susceptibility genes in French Whites: evidence for a novel susceptibility locus for early-onset diabetes on chromosome 3q27-qter and independent replication of a type 2–diabetes locus on chromosome 1q21–q24. The American Journal of Human Genetics 67, 1470, https://doi.org/10.1086/316887 (2000).
Kissebah, A. H. et al. Quantitative trait loci on chromosomes 3 and 17 influence phenotypes of the metabolic syndrome. Proceedings of the National Academy of Sciences 97, 14478, https://doi.org/10.1073/pnas.97.26.14478 (2000).
Mori, Y. et al. Genome-wide search for type 2 diabetes in Japanese affected sib-pairs confirms susceptibility genes on 3q, 15q, and 20q and identifies two new candidate Loci on 7p and 11p. Diabetes 51, 1247, https://doi.org/10.2337/diabetes.51.4.1247 (2002).
Nannipieri, M. et al. Polymorphism of the 3′-untranslated region of the leptin receptor gene, but not the adiponectin SNP45 polymorphism, predicts type 2 diabetes: a population-based study. Diabetes Care 29, 2509, https://doi.org/10.2337/dc06-0355 (2006).
Gu, H. F. et al. Single nucleotide polymorphisms in the proximal promoter region of the adiponectin (APM1) gene are associated with type 2 diabetes in Swedish caucasians. Diabetes 53(suppl 1), S31, https://doi.org/10.2337/diabetes.53.2007.S31 (2004).
Vimaleswaran, K. S. et al. A novel association of a polymorphism in the first intron of adiponectin gene with type 2 diabetes, obesity and hypoadiponectinemia in Asian Indians. Human Genetics 123, 599, https://doi.org/10.1007/s00439-008-0506-8 (2008).
Saxena, M., Srivastava, N. & Banerjee, M. Genetic association of adiponectin gene polymorphisms (+45T/G and +10211T/G) with type 2 diabetes in North Indians. Diabetes & Metabolic Syndrome: Clinical Research & Reviews 6, 65, https://doi.org/10.1016/j.dsx.2012.08.008 (2012).
Hansen, T. Type 2 diabetes mellitus–a multifactorial disease. In AnnalesUniversitatisMariae Curie-Sklodowska.Sectio D: Medicina 1, 544 (2002).
Keaton, J. M. et al. A comparison of type 2 diabetes risk allele load between African Americans and European Americans. Human genetics 133, 1487, https://doi.org/10.1007/s00439-014-1486-5 (2014).
Sim, X. et al. Transferability of type 2 diabetes implicated loci in multi-ethnic cohorts from Southeast Asia. PLoS Genetics 7, e1001363, https://doi.org/10.1371/journal.pgen.1001363 (2011).
Takahashi, M. et al. Genomic structure and mutations in adipose-specific gene, adiponectin. International Journal of Obesity 7, 861 (2000).
American Diabetes Association. Diagnosing diabetes and learning about prediabetes. Alexandria, VA.; 22311 (2014).
Patel, R., Palit, S. P., Rathwa, N., Ramachandran, A. V. & Begum, R. Genetic variants of tumor necrosis factor-α and its levels: A correlation with dyslipidemia and type 2 diabetes susceptibility. Clinical Nutrition 38, 1414–1422, https://doi.org/10.1016/j.clnu.2018.06.962 (2019).
Ali, S. et al. Association of variants in BAT1-LTA-TNF-BTNL2 genes within 6p21.3 region show graded risk to leprosy in unrelated cohorts of Indian population. Human Genetics 131, 703–716 (2012).
Knopfholz, J. et al. Validation of the friedewald formula in patients with metabolic syndrome. Cholesterol, 2014, https://doi.org/10.1155/2014/261878 (2014).
Li, Z. et al. A partition-ligation-combination-subdivision EM algorithm for haplotype inference with multiallelic markers: update of the SHEsis (http://analysis. bio-x. cn). Cell Research 19, 519, https://doi.org/10.1038/cr.2009.33 (2009).
ENCODE integrative analysis (PMID: 22955616; PMCID: PMC3439153).
Nov, O. et al. Interleukin-1β regulates fat-liver crosstalk in obesity by auto-paracrine modulation of adipose tissue inflammation and expandability. PloS One 8, e53626, https://doi.org/10.1371/journal.pone.0053626 (2013).
Nieva-Vazquez, A., Pérez-Fuentes, R., Torres-Rasgado, E., López-López, J. G. & Romero, J. R. Serum resistin levels are associated with adiposity and insulin sensitivity in obese Hispanic subjects. Metabolic Syndrome and Related Disorders 12, 143, https://doi.org/10.1089/met.2013.0118 (2014).
Moller, D. E. Potential role of TNF-α in the pathogenesis of insulin resistance and type 2 diabetes. Trends in Endocrinology & Metabolism 11, 212, https://doi.org/10.1016/S1043-2760(00)00272-1 (2000).
Rathwa, N. et al. Circulatory Omentin-1 levels but not genetic variants influence the pathophysiology of Type 2 diabetes. Cytokine 119, 144, https://doi.org/10.1016/j.cyto.2019.03.011 (2019).
Patel, R., Rathwa, N., Palit, S. P., Ramachandran, A. V. & Begum, R. Association of melatonin & MTNR1B variants with type 2 diabetes in Gujarat population. Biomedicine & Pharmacotherapy. 31(103), 429–34 (2018).
Rathwa, N. et al. Intron specific polymorphic site of vaspin gene along with vaspin circulatory levels can influence pathophysiology of type 2 diabetes. Life Sciences, 117285 (2020).
Turer, A. T. & Scherer, P. E. Adiponectin: mechanistic insights and clinical implications. Diabetologia 55, 2319, https://doi.org/10.1007/s00125-012-2598-x (2012).
Mohan, V. et al. Anthropometric cut points for identification of cardiometabolic risk factors in an urban Asian Indian population. Metabolism 56, 961, https://doi.org/10.1016/j.metabol.2007.02.009 (2007).
Bhardwaj, S. et al. High prevalence of abdominal, intra-abdominal and subcutaneous adiposity and clustering of risk factors among urban Asian Indians in North India. PloS One 6, e24362, https://doi.org/10.1371/journal.pone.0024362 (2011).
Mohan, V. et al. Serum immunoreactive insulin responses to a glucose load in Asian Indian and European type 2 (non-insulin-dependent) diabetic patients and control subjects. Diabetologia 29, 235, https://doi.org/10.1007/BF00454882 (1986).
Ling, H. et al. Genome‐wide Linkage and Association Analyses to Identify Genes Influencing Adiponectin Levels: The GEMS Stud. Obesity 17, 737, https://doi.org/10.1038/oby.2008.625 (2009).
Wu, Y. et al. Genome-wide association study for adiponectin levels in Filipino women identifies CDH13 and a novel uncommon haplotype at KNG1–ADIPOQ. Human Molecular Genetics 19, 4955, https://doi.org/10.1093/hmg/ddq423 (2010).
Heid, I. M. et al. Clear detection of ADIPOQ locus as the major gene for plasma adiponectin: results of genome-wide association analyses including 4659 European individuals. Atherosclerosis 208, 412, https://doi.org/10.1016/j.atherosclerosis.2009.11.035 (2010).
Ramya, K., Ayyappa, K. A., Ghosh, S., Mohan, V. & Radha, V. Genetic association of ADIPOQ gene variants with type 2 diabetes, obesity and serum adiponectin levels in south Indian population. Gene 532, 253, https://doi.org/10.1016/j.gene.2013.09.012 (2013).
Schäffler, A., Langmann, T., Palitzsch, K. D., Schölmerich, J. & Schmitz, G. Identification and characterization of the human adipocyte apM-1 promoter. BiochimicaetBiophysicaActa (BBA)-Gene Structure and Expression 1399, 187, https://doi.org/10.1016/S0167-4781(98)00106-7 (1998).
Qiao, L. et al. C/EBPα regulates human adiponectin gene transcription through an intronic enhancer. Diabetes 54, 1744, https://doi.org/10.2337/diabetes.54.6.1744 (2005).
Tu, Y. et al. Assessment of type 2 diabetes risk conferred by SNPs rs2241766 and rs1501299 in the ADIPOQ gene, a case/control study combined with meta-analyses. Molecular and Cellular Endocrinology 396, 1, https://doi.org/10.1016/j.mce.2014.08.006 (2014).
Stumvoll, M. et al. Association of the TG polymorphism in adiponectin (exon 2) with obesity and insulin sensitivity: interaction with family history of type 2 diabetes. Diabetes 51, 37, https://doi.org/10.2337/diabetes.51.1.37 (2002).
Ukkola, O., Ravussin, E., Jacobson, P., Sjöström, L. & Bouchard, C. Mutations in the adiponectin gene in lean and obese subjects from the Swedish obese subjects cohort. Metabolism 52, 881, https://doi.org/10.1016/S0026-0495(03)00074-X (2003).
Menzaghi, C. et al. A haplotype at the adiponectin locus is associated with obesity and other features of the insulin resistance syndrome. Diabetes 51, 2306, https://doi.org/10.2337/diabetes.51.7.2306 (2002).
Hara, K. et al. Genetic variation in the gene encoding adiponectin is associated with an increased risk of type 2 diabetes in the Japanese population. Diabetes 51, 536, https://doi.org/10.2337/diabetes.51.2.536 (2002).
Wang, B. F., Wang, Y., Ao, R., Tong, J. & Wang, B. Y. AdipoQ T45 G and G276 T Polymorphisms and Susceptibility to Nonalcoholic Fatty Liver Disease Among Asian Populations: A Meta‐Analysis and Meta‐Regression. Journal of Clinical Laboratory Analysis 30, 47, https://doi.org/10.1002/jcla.21814 (2016).
Rathwa, N., Patel, R., Palit, S. P., Ramachandran, A. V. & Begum, R. Genetic variants of resistin and its plasma levels: Association with obesity and dyslipidemia related to type 2 diabetes susceptibility. Genomics 111(4), 980–985 (2018).
He, Y. et al. The multimerization and secretion of adiponectin are regulated by TNF-alpha. Endocrine 51, 456, https://doi.org/10.1007/s12020-015-0741-4 (2016).
Patel, R. et al. Association of neuropeptide-Y (NPY) and interleukin-1beta (IL1B), genotype-phenotype correlation and plasma lipids with Type-II diabetes. PloS One 11(10), e0164437, https://doi.org/10.1371/journal.pone.0164437 (2016).
Luque-Ramírez, M. et al. Sexual dimorphism in adipose tissue function as evidenced by circulating adipokine concentrations in the fasting state and after an oral glucose challenge. Human Reproduction 28(7), 1908, https://doi.org/10.1093/humrep/det097 (2013).
Goto, A. et al. Plasma adiponectin levels, ADIPOQ variants, and incidence of type 2 diabetes: A nested case-control study. diabetes Research and Clinical Practice 127, 254, https://doi.org/10.1016/j.diabres.2017.03.020 (2017).
de Luis, D. A. et al. rs1501299 Polymorphism in the adiponectin gene and their association with total adiponectin levels, insulin resistance and metabolic syndrome in obese subjects. Annals of Nutrition and Metabolism 69, 226, https://doi.org/10.1159/000453401 (2016).
Dwivedi, M. et al. ACE gene I/D polymorphism in type 2 diabetes: the Gujarat population. The British Journal of Diabetes & Vascular Disease 11(3), 153, https://doi.org/10.1177/1474651411412662 (2011).
Alsafar, H. et al. Association of angiotensin converting enzyme insertion-deletion polymorphism with hypertension in emiratis with type 2 diabetes mellitus and its interaction with obesity status. Disease markers, 2015; https://doi.org/10.1155/2015/536041 (2015).
Zhu, N. et al. High-molecular-weight adiponectin and the risk of type 2 diabetes in the ARIC study. The. Journal of Clinical Endocrinology & Metabolism 95(11), 5097, https://doi.org/10.1210/jc.2010-0716 (2010).
Qiao, L., Zou, C., van der Westhuyzen, D. R. & Shao, J. Adiponectin reduces plasma triglyceride by increasing VLDL triglyceride catabolism. Diabetes 57, 1824, https://doi.org/10.2337/db07-0435 (2008).
Verges, B. et al. Adiponectin is an important determinant of apoA-I catabolism. Arteriosclerosis, Thrombosis, and Vascular Biology 26, 1364, https://doi.org/10.1161/01.ATV.0000219611.50066.bd (2006).
Palit, S. P. et al. A Haplotype at Adiponectin Locus: Relevance with Obesity and Type 2 Diabetes. Available at SSRN 3335867 (2019).
Acknowledgements
We thank our medical collaborators Dr. Jaya Pathak, M.D, S.S.G Hospital, Vadodara; Dr. Mahendra Narwaria, Bariatric, GI & Robotic Surgeon, Asian Bariatrics, Ahmedabad, and all the subjects for their participation in this study. R.P. thanks CSIR for awarding SRF. N.R. thanks University Grants Commission-National Fellowship for higher education for ST students, for awarding SRF. S.D.J. thanks UGC, New Delhi for awarding SRF.
Author information
Authors and Affiliations
Contributions
R.B. developed the concept. S.P.P. designed and performed the experiments. S.P.P., R.P. and N.R. contributed to data acquisition and data analysis was performed by S.P.P. S.D.J. contributed towards bioinformatics analyses and interpretation. A.M., M.K.D. and S.S. contributed to the data generation and analysis in J&K population. R.B. and A.V.R. contributed to the critical revision and approval of the article.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Palit, S.P., Patel, R., Jadeja, S.D. et al. A genetic analysis identifies a haplotype at adiponectin locus: Association with obesity and type 2 diabetes. Sci Rep 10, 2904 (2020). https://doi.org/10.1038/s41598-020-59845-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-020-59845-z
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
