
Abstract
Single nucleotide polymorphisms of the TCF7L2, HHEX, SLC30A8, MTNR1B, SLC2A2 and GLIS3 genes are well established candidate genes for cardiometabolic diseases (CMDs) across different ethnic populations. We investigated their association with CMDs in a mixed ancestry population of South Africa. rs10830963, rs1111875, rs11920090, rs13266634, rs7034200 and rs7903146 SNPs were genotyped by quantitative real time PCR in 1650 participants and Hardy–Weinberg equilibrium (HWE) analyses performed on the SNPs. Diabetes, obesity, hypertension and cardiometabolic traits were compared across genotypes of SNPs in HWE. Linear and logistic regressions adjusting for age, gender and body mass index were used to determine the risk of T2DM, obesity and hypertension. rs7903146 (p = 0.055), rs1111875 (p = 0.465), rs13266634 (p = 0.828), and rs10830963 (p = 0.158) were in HWE. The rs10830963 recessive genotype was able to predict FPG, insulin and HOMA-IR, while the rs1111875 recessive genotype was able to predict total cholesterol, triglyceride, LDL cholesterol and FPG. The rs7903146 recessive genotype was able to predict SBP and LDL cholesterol. The recessive genotypes of MTNRIB and HHEX SNPs were associated with T2DM traits in the study population and could partially explain the high prevalence of T2DM. Further studies are required to confirm these findings and establish candidate genes in the African population.
Similar content being viewed by others


Introduction
Cardio-metabolic diseases (CMDs) including diabetes mellitus, cardiovascular diseases and chronic kidney disease are presently the leading cause of mortality in the world. Diabetes mellitus is characterized by chronic hyperglycemia with disturbances in carbohydrate, fat and protein metabolism, resulting from defects in insulin secretion and/or action1. The global incidence of Type 2 Diabetes Mellitus (T2DM) has increased by 46.6% in the last 10 years rising from 366 million in 2011 to 537 million in 20211. Africa experienced the fastest increase at 63.3% within the same period with accelerated urbanization and the associated lifestyle changes being the key drivers2. According to the 2021 South African Diabetes Report, the prevalence of diabetes has reached 11.3%, the highest in Africa3. Moreover, close to 45.4% of people living with diabetes in South Africa were undiagnosed and 33.3% (13 million) of the adult population had impaired fasting glucose which was observed to be the highest in the world3.
The conventional risk factors including poor and unhealthy diet, lack of physical activity, excessive alcohol intake, and cigarette smoking are responsible for the increase in the prevalence of CMDs4,5. These factors are known to cause metabolic derangements such as obesity, hypertension, dyslipidemia, oxidative stress, insulin resistance and/or pancreatic beta cell dysfunction, which progresses to the CMDs especially T2DM. However, the conventional factors act in the presence of a favorable genetic background, as the risk of T2DM may be different in individuals exposed to the same environmental factors. When either parent has T2DM, an individual has a 40% risk of T2DM, whilst that risk is even more pronounced (70%) when both parents have T2DM6. Moreover, any individual whose sibling has diabetes is three times more likely to develop the disease7.
Type 2 Diabetes Mellitus is a polygenic disorder and occurs due to the interaction between several genes. Early approaches to study the genetics of diabetes used linkage and candidate gene methods that led to the identification of genes associated with T2DM8. With the genome-wide association studies (GWAS) using high-throughput single nucleotide polymorphism (SNP) genotyping technology, several other T2DM SNPs were discovered. The candidate genes identified were observed across different populations and included transcription factor 7 like 2 (TCF7L2) gene, peroxisome proliferator activator receptor gamma (PPAR-γ), haematopoietically expressed homeobox (HHEX), Solute carrier family 30-member 8 (SLC30A8) Cyclin-dependent kinase inhibitor 2A/B (CDKN2A/B) and insulin-like growth factor 2 mRNA binding protein 2 (IGF2BP2)9,10,11,12,13,14. In a recent meta-analysis, the rs7903146 SNP of the TCF7L2 gene was observed to be associated with T2DM in South Asian, East Asian, Caucasian and other (mixed and African) ethnicities15. Similarly, SNPs of the HHEX and MTNR1B genes have been investigated in Asian and Caucasian and identified as candidate genes for T2DM16,17. The HHEX and TCF7L2 gene variants contribute to T2DM by affecting insulin secretion (activating hepatocyte nuclear factor 1α) and action17,18,19, while MTNR1B impairs insulin secretion and glucose homeostasis, by downregulating adenylate or guanylate cyclase activity20.
Most GWAS to unravel SNPs associated with T2DM have been carried out in Caucasians, South Asians, East Asians, mixed populations with very few studies in Africa15,21. Moreover, studies in Africa which are often replication in nature have mostly been carried out in North Africa, with very few studies in sub-Saharan Africa yielding inconsistent findings21,22. Our study therefore aimed to investigate the association between well described SNPs risk factors and T2DM in the mixed ancestry population of Bellville South in Cape Town, South Africa. This population was chosen as it has a higher prevalence of T2DM compared to the general population of South Africa23.
Methodology
Study design and population
This cross sectional study used data from the Cape Town Vascular and Metabolic Health (VMH) study consisting of 1969 male and female participants. They were recruited during a community based survey involving mixed ancestry South Africans residing in the township of Bellville South in Cape Town as previously described24. The mixed ancestry South African population is a well-defined, multiracial ethnic group that comes from a combination of ethnic backgrounds including indigenous South Africans, Caucasians, Griquas and Asians25. Ethical approval was obtained from the Research Ethics Committees of the Cape Peninsula University of Technology and Stellenbosch University (NHREC: REC—230 408–014 and N14/01/003) and the study was conducted in accordance with the principles of the Declaration of Helsinki. The city and community authorities granted permission for the study to be conducted in their municipality and all study participants gave written informed consent before they were included.
Data collection and sampling
Data including demographic characteristics, personal and family medical history, ongoing treatment and smoking habits were collected by trained fieldworkers using a standardized questionnaire on a password-protected personal digital assistant. Physical examination including body weight in kilogram (kg), height in centimetres (cm), waist circumference (WC), hip circumference (HC), systolic blood pressure (SBP) and diastolic blood pressure (DBP) were measured in triplicate as previously described24 with the lowest values used for analysis. After physical examination, blood samples were collected by trained registered nurses from all participants and stored at − 80 °C for biochemical analysis and SNP genotyping. This was closely followed by an oral glucose tolerant test (OGTT) with a 75 g of glucose load in accordance with the World Health Organization (WHO) recommendations. The OGTT test was not performed in patients with known T2DM.
Biochemical analyses
Fasting plasma glucose (FPG) was measured by enzymatic hexokinase method (Beckman Coulter), insulin by a paramagnetic particle chemiluminescence assay (Beckman Coulter) and glycated haemoglobin (HbA1c) by high performance liquid chromatography (Biorad Variant Turbo, BioRad). Total cholesterol (TC) and high-density lipoprotein cholesterol (HDL-C) were measured by enzymatic immune-inhibition, triglycerides (TG) by glycerol phosphate oxidase–peroxidase and low-density lipoprotein cholesterol (LDL-C) by enzymatic selective protection—End Point (Beckman Coulter). A modified Jaffe-Kinetic method was used to measure serum creatinine (Beckman AU, Beckman Coulter, South Africa). Highly sensitive c-reactive protein (hs-CRP) was measured by Enzyme Linked Immuno-Sorbent Assay (ELISA) (BIOMATIK) according to the manufacturers protocol.
DNA extraction and genotyping
Deoxyribonucleic Acid (DNA) was extracted using the salt extraction method26 and the concentration/purity determined using the Nanodrop™ One (Thermo Fisher Scientific, Waltham, MA, USA). All samples with a ratio of absorbance at 260 nm and 280 nm between 1.7 and 2.2 were considered good quality and used for SNP genotyping by real time quantitative polymerase chain reaction (RT-qPCR). Six SNPs (rs10830963, rs1111875, rs11920090, rs13266634, rs7034200 and rs7903146) were genotyped with a TaqMan® Universal PCR Master Mix, according to the manufacturer’s protocol. Enough PCR master mix for the requisite number of reactions was made in a 1.5 ml tube as shown in Table 1, pulse vortexed and then briefly centrifuged. Afterwards, 8 µL of the master mix were pipetted into each of the 96-well plate’s wells. 2 µL of the template DNA sample (5 ng/µL concentration) were then pipetted into the appropriate well. For quality control purposes, a non-template control was also included in each PCR run, with 2 µL of ddH20 used in place of template DNA. When all components of the PCR had been pipetted into the appropriate wells, the 96-well plate was covered with MicroAmp optical caps, and the PCR run on the Applied Biosystems® Quant Studio™ 7 Flex Real-time PCR system (ThermoFisher Scientific) as shown in Fig. 1.

PCR cycling conditions for the SNP genotyping assay.
For each SNP, the three genotypes were determined from the PCR amplification output as follows: a sample was homozygous for the dominant allele when amplification curves were observed only in the VIC channel, homozygous for the recessive allele if an amplification signal in the ROX channel was observed, whilst amplification in both channels indicated a heterozygous genotype. Reagents and primers (TaqMan® SNP Genotyping Assays) were sourced from ThermoFisher Scientific.
The accuracy of SNP genotyping using RT-qPCR was confirmed by comparing genotyping results of 20 randomly selected samples sequenced by Inqaba Biotechnical Industries.
Definitions and calculations
Body mass index (BMI) was calculated as weight (kg)/[height (m)]2 and used to categorize participants as normal weight (BMI < 25 kg/m2), overweight (25 kg/m2 ≤ BMI < 30 kg/m2) and obese (BMI ≥ 30 kg/m2). Waist to hip ratio (WHR) was calculated as WC (cm)/HC (cm). Central obesity was determined using WC > 94 cm in male and WC > 80 cm in female. Hypertension was defined as having systolic blood pressure (SBP) ≥ 140 mmHg or diastolic blood pressure (DBP) ≥ 90 mmHg or known hypertension on treatment27. Dyslipidemia was defined as TC > 5 mmol/L, triglycerides > 1.5 mmol/L, HDL-C < 1.2 mmol/L, LDL-C > 3.0 mmol/L and non-HDL-C > 3.37 mmol/L or taking anti-lipid agents28. Diabetes was defined as fasting plasma glucose ≥ 7.0 mmol/L and/or 2-h post glucose load ≥ 11.1 mmol/L, previously diagnosed or taking antidiabetic medications29.
Insulin resistance (IR) was based on the homeostasis model assessment (HOMA) using the formula:
HOMA - IR = \(\frac{\hbox{Fasting Glucose (nmol/L)}\times \hbox{Fasting Insulin}\,(\upmu\hbox{U}/\mathrm{L})}{22.5}\), Beta cell function was determined by HOMA-β using the formula: HOMA-β = \(\frac{20 \times \hbox{Fasting Insulin}\,(\upmu \hbox{IU}/\hbox{mL})}{\hbox{Fasting Glucose}\,\left(\frac{\hbox{mmol}}{\hbox{mL}}\right)-3.5}\).
Statistical analysis
Data were analysed using the IBM Statistical Package for Social Sciences (SPSS) version 29 software. Categorical variables were reported as counts (percentages) and continuous variables reported as median (25–75th percentiles). Hardy–Weinberg equilibrium (HWE) was tested for all the six SNPs and those in HWE were used for further analysis. Diabetes, obesity, hypertension, dyslipidemia and cardiometabolic traits (SBP, DBP, TC, HDL-C, TG, LDL-C, hs-CRP, FPG, insulin, HOMA-IR, HOMA-B and HbA1c ) were compared across genotypes of SNPs in HWE using the chi-square goodness-of-fit test for categorical variables and median test for continuous variables given that the variables were skewed. Linear regression analyses was performed to test the interactions between cardiometabolic traits and the genotypes of the SNPs investigated while adjusting for age, gender and BMI. Logistic regression analyses was performed to test the interactions between dyslipidemia, diabetes, obesity, hypertension and the genotypes of the SNPs investigated while adjusting for age, gender and BMI. All analyses were performed at 95% confidence interval and the level of significance considered at p < 0.05.
Results
General characteristics of study participants
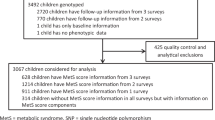
This study consisted of 1650 participants with 71.4% being women (Table 2). The prevalences of diabetes, obesity and hypertension were 22.2%, 39.9% and 34.7% respectively (Table 1). There was a significant difference in age, BMI, WC, HC, WHR, FPG, insulin, HBA1c, HOMA-IR, HOMA-β, TC, HDL-C, LDL-C, hs-CRP, cotinine and gamma glutamyl transferase (γGT) between women and men (all p \(\le\) 0.01).
Genotypic frequencies of the single nucleotide polymorphisms
Amongst the blood samples collected from 1650 study participants, quality DNA was successfully extracted from 1404 samples (85% extraction rate). Each of the SNPs was genotyped in the 1404 samples with undetermined genotypes varying between 1.4 and 9.9%, and all three genotypes were found in all the SNPs investigated. Amongst the 6 SNPs, rs10830963, rs1111875, rs13266634 and rs7903146 were in HWE, while rs11920090 and rs7034200 deviated from the HWE (Table 3). Even though positive controls were used during genotyping and the nucleotides confirmed by sequencing 20 samples, we cannot exclude the presence of genotyping error or non-random mating, which are amongst the causes of HWE deviation. As such, all SNPs deviating from HWE were not analyzed for their association with cardiometabolic traits as these associations could be spurious.
Association between risk genotype and cardiometabolic traits/diseases
Clinical characteristics were compared between the genotypes of the four SNPs in HWE. The results showed that pulse (p = 0.005), fasting plasma glucose (p = 0.01), insulin (p = 0.003), HbA1c (p = 0.037), HOMA-IR (p = 0.006), HOMA-B (p = 0.021) and total cholesterol (p = 0.043) were significantly higher in carriers of the recessive GG genotype of rs10830963 SNP when compared to the wild CC genotype (Table 4). Results of the rs1111875 SNP revealed that individuals with the recessive TT genotype had lower cotinine values compared to those with the dominant CC genotype and the difference was statistically significant (p = 0.014). Moreover, the number of participants with high TC levels were significantly higher amongst carriers of the TT genotype when compared to carriers of the CC genotype (p = 0.03). There was a higher number of individuals with hypertension (p = 0.034) and dyslipidemia characterized by high triglycerides (p = 0.018) amongst carriers of the TT recessive genotype of the rs7903146 SNP compared to carriers of the CC genotype (Table 5).
Linear and logistic regression analysis for the association between single nucleotide polymorphisms and cardiometabolic traits
Linear regression analyses were carried out to determine whether carrying the recessive genotypes of the SNPs investigated could increase the risk of quantitative traits of cardiometabolic diseases while adjusting for age, gender, and BMI (Table 6). The results showed that expression of the recessive genotype of rs10830963 SNP may be suggestive of an increased risk of dysglycemia characterized by increased fasting plasma glucose (β = − 0.789, p = 0.024 compared to the heterozygote genotype), increased fasting insulin (β = − 5.908, p < 0.001 compared to the heterozygote genotype and β = − 5.686, p < 0.001 compared to the homozygote dominant genotype) and increased HOMA-IR (β = − 3.354, p < 0.001 compared to the heterozygote genotype and β = − 3.376, p < 0.001 compared to the homozygote dominant genotype). Similarly, expression of the recessive genotype of rs1111875 SNP may be suggestive of an increased risk of both dysglycemia characterized by high fasting plasma glucose (β = − 0.444, p = 0.031 compared to the dominant genotype) and dyslipidemia characterized by increased total cholesterol (β = − 0.165, p = 0.049 compared to the homozygote dominant genotype) and increased triglyceride (β = − 0.260, p = 0.001 compared to the homozygote dominant genotype). The recessive allele of the rs13266634 SNP was not associated with cardiometabolic traits risks, while the recessive genotype of rs7903146 SNP increased the risk of high blood pressure characterized by high systolic blood pressure (β = − 4.679, p = 0.022 compared to the heterozygote genotype).
Logistic regression analyses adjusting for age, gender and BMI were carried out to evaluate the association between the recessive genotypes of the SNPs and T2DM, obesity, hypertension and dyslipidemia characterized by high TC, high TG, low HDL-C and high LDL-C (Table 6). From these results, the odds of hypercholesterolemia reduced by 33% in carriers of the homozygote dominant genotype (95% CI = 0.49–0.92, p = 0.013) and 34% in carriers of the heterozygote genotype (95%CI = 0.48–0.90, p = 0.009) when compared to carriers of the risk genotype of rs1111875 SNP. Moreover, the odds of high LDL-C reduced by 40% in carriers of the heterozygote genotype (95% CI = 0.39–0.93, p = 0.022) of the rs7903146 SNP when compared to carriers of the risk genotype (Table 7).
Discussion
This study examined the association between six SNPs and cardiometabolic risk profile in a mixed ancestry South African population. The TT recessive genotype of the rs7903146 SNP was significantly higher in patients with hypertension when compared to the CC genotype. While there was no association with diabetes, obesity and dyslipidemia, the SNPs of the TCF7L2 gene (rs7903146), HHEX gene (rs1111875) and MTNR1B gene (rs10830963) were associated with cardiometabolic traits. Individuals with the recessive genotype of rs10830963 SNP had significantly higher fasting plasma glucose (FPG), insulin and HOMA-IR values relative to carriers of the dominant genotype. More participants with the rs1111875 recessive genotype had high total cholesterol and LDL cholesterol compared to those with the dominant genotype. After adjusting for covariates (age, gender, and BMI), the rs10830963 recessive genotype was associated with FPG, insulin and HOMA-IR. The rs1111875 recessive genotype was associated with total cholesterol, triglyceride, LDL cholesterol and fasting glucose, whilst the rs7903146 recessive genotype was associated with systolic blood pressure and LDL cholesterol.
People living in the same environment experience different risk for T2DM and other metabolic diseases, partly due to their genetic differences. Single nucleotide polymorphisms, found in at least one percent of the population, are the most common type of genetic variation that exists, and they occur when one nucleotide in a DNA sequence is replaced by another. Several SNPs have been used as biological markers to identify genes that are associated with diseases. The candidacy gene approach and GWAS have led to the identification of several gene variants associated with T2DM via different metabolic pathways. For instance, the rs10830963 SNP of the Melatonin receptor 1B gene and rs13266634 of the Solute carrier family 2-member 2 encode for proteins which affect insulin secretion and glucose homeostasis pathways, leading to the development of T2DM20,30. On the other hand, rs7903146 and rs1111875 are SNPs of the TCF7L2 and HHEX genes which encode transcription factors involved in the wnt signaling pathways. While rs7903146 mainly affects the insulin sensitivity pathway by the regulation of genes involved in lipid and glucose metabolism31, rs1111875 is involved in beta cell function via the reduction of cell mass and decrease in beta-cell secretory capacity18. Our study reported similar findings on the association between cardiometabolic traits and two of the studied SNPs (rs10830963 and rs1111875). The rs10830963 SNP was observed to affect the insulin resistance pathway, with no effect in beta cell dysfunction. Insulin resistance resulted in significantly higher fasting plasma glucose and insulin levels in the carriers of the risk genotypes. The association of the rs1111875 recessive genotype with dyslipidemia and hyperglycemia in our study suggests the SNP affects insulin sensitivity rather than insulin secretion pathways. While no association was observed between rs10830963 and rs1111875 with these cardio-metabolic diseases, their association with traits of T2DM could be indicative that these SNPs are possible risk factors for T2DM. The absence of association with disease state has also been reported in studies carried out in Indian32 and European populations33. Our study failed to replicate findings on the association between rs7903146 SNP of the TCF7L2 gene and T2DM and its traits including glucose and insulin. The recessive TT genotype of the rs7903146 SNP is a well-known risk factor for T2DM in Caucasian and Asian populations. Moreover, studies in sub-Saharan Africa reported an association between rs7903146 and increased risk for T2DM in Ghana34 and South Africa35. Our study was carried out in a mixed ancestry population which is genetically more diverse compared to the black African, Caucasian and Asian populations, and could be responsible for the difference in the findings. Moreover, our study did not find an association between rs13266634 SNP of the SLC30A8 gene and diseases states (diabetes, obesity and hypertension) or traits (plasma glucose, insulin, blood pressure or lipid profile), whose association with T2DM has been previously reported in Asian36 and European populations37. As such, it is plausible that these SNPs confer risk to T2DM in specific populations and may not necessarily be of concern in the mixed ancestry South Africa population. Our study had some limitations, and this included its cross-sectional nature, which made it difficult to infer causality of disease. Moreover, the discordant findings reported in our study could be because of our study design, which differed from other studies which often investigate associations between SNPs and cardio-metabolic diseases using case–control designs. Due to funding constraints, the genotypes were confirmed by sequencing in less than 1.5% of the samples, which is relatively small. Despite these limitations, the large sample size and the similar genetic background of our study participants significantly added to the growing pool of data on the genetics of T2DM in the mixed ancestry population.
Conclusion
Recessive genotypes of the rs1111875 SNP of the HHEX gene and the rs10830963 SNP of the MTNR1B gene may increase the risk of T2DM in the mixed ancestry South African population. This may be through coding for proteins which affect the insulin signaling pathway without an effect on beta cell function. Other studies confirming such findings in the same population as well as other populations are warranted to fully understand the genetic predisposition to T2DM in the South African population.
Data availability
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
International Diabetes Federation. IDF Diabetes Atlas 10th edn (2021).
Issaka, A., Paradies, Y. & Stevenson, C. Modifiable and emerging risk factors for type 2 diabetes in Africa: A systematic review and meta-analysis protocol. Syst. Rev. 7, 139. https://doi.org/10.1186/s13643-018-0801-y (2018).
International Diabetes Federation South Africa Diabetes report 2010–2045; (Online; Accessed December 2022); https://diabetesatlas.org/data/en/country/185/za.html (2022).
Shaw, J. E., Sicree, R. A. & Zimmet, P. Z. Global estimates of the prevalence of diabetes for 2010 and 2030. Diabetes Res. Clin. Pract. 87, 4–14 (2010).
Deaton, C. et al. The global burden of cardiovascular disease. Eur. J. Cardiovasc. Nurs. 10, 5–13 (2011).
Köbberling, J., & Tillil, H. The genetics of diabetes mellitus. In Empirical Risk Figures for First-Degree Relatives of Non-insulin Dependent Diabetics 201–209 (Academic Press; London, UK, 1982).
Florez, J. C., Hirschhorn, J. & Altshuler, D. The inherited basis of diabetes mellitus: Implications for the genetic analysis of complex traits. Annu. Rev. Genomics Hum. Genet. 4, 257–291 (2003).
Deeb, S. S. et al. A Pro12Ala substitution in PPARγ2 associated with decreased receptor activity, lower body mass index and improved insulin sensitivity. Nat. Genet. 20, 284–287 (1998).
Grant, S. F. et al. Variant of transcription factor 7-like 2 (TCF7L2) gene confers risk of type 2 diabetes. Nat. Genet. 38, 320–323 (2006).
Gaulton, K. J. et al. Comprehensive association study of type 2 diabetes and related quantitative traits with 222 candidate genes. Diabetes 57, 3136–3144 (2008).
Lyssenko, V. et al. Common variant in MTNR1B associated with increased risk of type 2 diabetes and impaired early insulin secretion. Nat. Genet. 41, 82–88 (2008).
Boesgaard, T. W. et al. Variants at DGKB/TMEM195, ADRA2A, GLIS3 and C2CD4B loci are associated with reduced glucose-stimulated beta cell function in middle-aged Danish people. Diabetologia 53, 1647–1655 (2010).
Cai, Y., Yi, J., Ma, Y. & Fu, D. Meta-analysis of the effect of HHEX gene polymorphism on the risk of type 2 diabetes. Mutagenesis 26, 309–314 (2011).
Goyal, Y., Verma, A. K., Joshi, P. C. & Dev, K. Contemplating the role of genetic variants of HHEX, CDKAL1, WFS1 and SLC30A8 genes of TYPE-2 diabetes in Asians ethnic groups. Gene Rep. 17, 10046 (2019).
Ding, W. et al. Meta-analysis of association between TCF7L2 polymorphism rs7903146 and type 2 diabetes mellitus. BMC Med. Genet. 19, 38. https://doi.org/10.1186/s12881-018-0553-5 (2018).
Chambers, J. C. et al. Common genetic variation near melatonin receptor MTNR1B contributes to raised plasma glucose and increased risk of type 2 diabetes among Indian Asians and European Caucasians. Diabetes 58, 2703–2708 (2009).
Tanaka, H. et al. HEX stimulates the hepatocyte nuclear factor 1a-mediated activation of transcription. Arch. Biochem. Biophys. 442, 117–124 (2005).
Pascoe, L. et al. Common variants of the novel type 2 diabetes genes CDKAL1 and HHEX/IDE are associated with decreased pancreatic beta-cell function. Diabetes 56, 3101–3104 (2007).
Staiger, H. et al. Polymorphisms within the novel type 2 diabetes risk locus MTNR1B determine β-cell function. PLOS ONE 3, e3962 (2008).
Stumpf, I., Muhlbauer, E. & Peschke, E. Involvement of the cGMP pathway in mediating the insulin-inhibitory effect of melatonin in pancreatic beta-cells. J. Pineal Res. 45, 318–327 (2008).
Chen, J. et al. Genome-wide association study of type 2 diabetes in Africa. Diabetologia 62, 1204–1211 (2019).
Adeyemo, A. A. et al. ZRANB3 is an African-specific type 2 diabetes locus associated with beta-cell mass and insulin response. Nat. Commun. 10, 3195. https://doi.org/10.1038/s41467-019-10967-7 (2019).
Erasmus, R. T. et al. High prevalence of diabetes mellitus and metabolic syndrome in a South African coloured population: Baseline data of a study in Bellville, Cape Town. S. Afr. Med. J. 102, 841–844 (2012).
Kengne, A. P., Erasmus, R. T., Levitt, N. S. & Matsha, T. E. Alternative indices of glucose homeostasis as biochemical diagnostic tests for abnormal glucose tolerance in an African setting. Prim. Care Diabetes 11, 119–131 (2017).
Henrard, K. Minority Protection in Post-Apartheid South Africa: Human Rights, Minority Rights, and Self-Determination 43 (Greenwood Publishing Group, 2002). ISBN 978-0-275-97353-7.
Miller, S. A., Dykes, D. D. & Polesky, H. F. A simple salting out procedure for extracting DNA from human nucleated cells. Nucleic Acids Res. 16, 1215 (1988).
Williams, B. et al. ESC Scientific document group. ESC/ESH guidelines for the management of arterial hypertension. Eur. Heart J. 39, 3021–3104 (2018).
Clinical Guidelines. Diagnosis, management and prevention of the common dyslipidaemias in South Africa- guideline. South African Medical Association and Lipid and Atherosclerosis Society of Southern Africa Working Group. S. Afr. Med. J. 90, 164–178 (2000).
World Health Organisation. Definition, Diagnosis and Classification of Diabetes Mellitus and its Complications: Report of a WHO Consultation (World Health Org, Geneva, 1999).
Dupuis, J. et al. New genetic loci implicated in fasting glucose homeostasis and their impact on type 2 diabetes risk. Nat. Genet. 42, 105–116 (2010).
Geoghegan, G. et al. Targeted deletion of TCF7L2 in adipocytes promotes adipocyte hypertrophy and impaired glucose metabolism. Mol. Metab. 24, 44–63 (2019).
Phani, N. M. et al. Replication and relevance of multiple susceptibility loci discovered from genome wide association studies for type 2 diabetes in an Indian population. PLOS ONE 11, e0157364 (2016).
Lewis, J. P. et al. Association analysis in African Americans of European-derived type 2 diabetes single nucleotide polymorphisms from whole genome association studies. Diabetes 57, 2220–2225 (2008).
Danquah, I. et al. The TCF7L2 rs7903146 (T) allele is associated with type 2 diabetes in urban Ghana: A hospital-based case–control study. BMC Med. Genet. 14, 96 (2013).
Pirie, F. J. et al. Variants in PPARG, KCNJ11, TCF7L2, FTO, and HHEX genes in South African subjects of Zulu descent with type 2 diabetes. African J. Diabetes Med. 18, 12–16 (2010).
Cheng, L., Zhang, D., Zhou, L., Zhao, J. & Chen, B. Association between SLC30A8 rs13266634 polymorphism and type 2 diabetes risk: a meta-analysis. Med. Sci. Monit. 21, 2178–2189 (2015).
Fan, M. et al. Association of SLC30A8 gene polymorphism with type 2 diabetes, evidence from 46 studies: A meta-analysis. Endocrine 53, 381–394 (2016).
Acknowledgements
We thank the community of Bellville South, the participants for their time, fieldworkers, clinicians and nurses who collected data for the study.
Funding
This research project was funded by the South African Medical Research Council with funds from the National Treasury under its Economic Competitiveness and Support Package (MRC-RFA-UFSP-01-2013/VMH Study) and strategic funds from the South African Medical Research Council received from the South African National Department of Health, the South African National Research Foundation (Grant No. 115450).
Author information
Authors and Affiliations
Contributions
T.E.M. and A.P.K. conceived, designed, and acquired the data. N.E.N. and D.M.M. analyzed the data and drafted the article. G.M.D., T.E.M. and A.P.K. revised the manuscript critically for important intellectual content. All authors agreed to submit to the current journal, gave final approval of the version to be published and agree to be accountable for all aspects of the work.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Ngwa, N.E., Matshazi, D.M., Davison, G.M. et al. Association between the MTNR1B, HHEX, SLC30A8, and TCF7L2 single nucleotide polymorphisms and cardiometabolic risk profile in a mixed ancestry South African population. Sci Rep 13, 17122 (2023). https://doi.org/10.1038/s41598-023-43560-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-023-43560-6
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
