
Abstract
We aimed to assess whether a triple-faceted intervention program administered in the primary care setting could decrease the risk of insufficient adherence to primary care physician (PCP) appointments among this patient population. We conducted a cluster-randomized controlled study to assess the effects of a 1-year intervention. The primary outcome was insufficient adherence to regular PCP attendance for diabetes treatment, defined as failure to visit a PCP within 2 months of an original appointment date. The intervention consisted of mailing patient reminders of their PCP appointments, providing patients with health education aimed at lifestyle modification and benchmarking PCP procedures. Eleven municipal level district medical associations employing 192 PCPs were divided into two subregions for assignment to intervention and control clusters, with 971 and 1,265 patients assigned to the intervention and control groups, respectively. Primary outcome data were available for 2,200 patients. The intervention reduced insufficient adherence to regular PCP appointments by 63% (hazard ratio, 0.37; 95% confidence interval [CI], 0.23–0.58). In conclusion, a triple-faceted intervention program consisting of health education, appointment reminders, and physician benchmarking may decrease the risk of incomplete adherence to regular PCP appointments by diabetes patients.
Similar content being viewed by others

Introduction
The incidence and prevalence of type 2 diabetes are rapidly increasing worldwide1,2,3,4, including in Japan, where a national survey estimated that the number of patients with diabetes had increased from 6.9 to 9.5 million between 1997 and 20125,6. This rate of increase is a significant concern because epidemiologic studies have indicated that type 2 diabetes is an independent risk factor for cardiovascular diseases as well as microvascular complications. In support of this indication of the potential broad-reaching impact of diabetes, the incidence of cardiovascular disease is reported to be approximately twice as high in patients with diabetes as in healthy age-matched individuals7. In response to these findings, researchers and clinicians have underscored the need for intensive control of glycemic response and lipid and blood pressure levels to reduce risk of cardiovascular disease and microvascular complications in patients with diabetes8.
Although clinical guidelines recommend both nonpharmacological and pharmacological interventions to control diabetes-associated complications9, patients cannot benefit from these interventions if they are lost to follow-up. The current rate of adherence to diabetes treatment in Japan is approximately 80–90%10,11, which is similar to the estimates in the United States, Scotland, Canada12, and United Kingdam13. Patients who do not regularly visit their primary care physicians (PCPs) tend to have poorer glycemic and obesity control14,15,16, both of which may lead to poor health outcomes that ultimately result in the development of diabetic complications17. Furthermore, nonadherence to diabetes treatment and relapse after temporary improvement may explain a substantial amount of uncontrolled diabetes18. Strengthening the healthcare provider–patient relationship and performing certain administrative actions, such as calling or mailing reminders to patients prompting them to make or keep appointments, could increase clinic attendance and subsequently increase glycemic monitoring and disease control for these patients8,14,15. However, to our knowledge, there are no published reports on whether provision of a multifaceted intervention program in the primary care setting that includes these components reduces the treatment dropout rate of diabetes patients in a real-world clinical setting. To address this research gap, the Japan Diabetes Outcome Intervention Trial 2 (J-DOIT2) investigated whether provision of a triple-faceted intervention program in the primary care setting could decrease the risk of insufficient adherence to regular PCP appointments by patients that have been diagnosed with type 2 diabetes and tested the hypothesis that intervention efficacy will vary according to specific patient characteristics.
Methods
Ethics statement
This study was approved by Ethics Committee of the Office of Strategic Outcomes Research Program, Japan Foundation for the Promotion of International Medical Research Cooperation, in accordance with the Declaration of Helsinki and relevant ethical guidelines in Japan. All participants received a precise explanation of the study and provided their written informed consent.
Study design
Specific details regarding the study participants and the methods used in this 1-year, prospective, cluster-randomized interventional study have been described elsewhere (Trial Registration: UMIN000002186, https://upload.umin.ac.jp/cgi-open-bin/ctr_e/ctr_view.cgi?recptno = R000002663; date of registration: July 13, 2009)19. In brief, PCPs within each district medical association (DMA) in Japan were divided into two groups according to the geographical location of the PCP’s clinic and the DMA branch to which the PCP belonged; neighboring clinics belonging to the same DMA branch were included in the same group. Therefore, clusters formed were composed of PCPs belonging to the same DMA branches and their patients with diabetes.
DMAs and PCPs
To be eligible for the study, a DMA needed to have approximately 20 PCPs who were able to participate in the study. We estimated that the study required 125 patients with diabetes from each DMA. In addition, the DMA had to be capable of establishing a diabetes treatment network consisting of PCPs, physicians specializing in diabetes, physicians specializing in kidney disease, and ophthalmologists. The PCP eligibility criteria were as follows: a membership to a recruited DMA, being a nonspecialist in the treatment of diabetes, and a realistic capability of enrolling 10 or more consenting patients with diabetes to the study. PCPs who had participated in a study with similar interventions during the preceding 5 years were excluded. Fifteen municipal level DMAs in Japan were recruited through an announcement made by the Japan Medical Association, a nationwide professional organization representing physicians throughout Japan. From this pool, 192 PCPs at 11 DMAs consented to participate in the study.
Patients
The patient inclusion criteria were as follows: a diagnosis of type 2 diabetes prior to registration and aged 40–64 years at enrollment. As we aimed to focus on generations who tend to actively work and have relatively high diabetes prevalence, the age groups of 40–64 years were selected. The exclusion criteria included undergoing hemodialysis, hospitalization, bedridden condition, nursing home residence, blindness, amputated lower limbs, diagnosis of a malignant tumor within the preceding 5 years, pregnancy or potential pregnancy, having two or more medical doctors in charge of diabetes care (except for the treatment of diabetes complications), and type 1 diabetes. There was no study restriction on plasma glucose level or glycated hemoglobin A1c (HbA1c) value.
Randomization
After registration of the 11 DMAs, each DMA was divided into two subregions or clusters. The study statistician, blinded to the cluster of each DMA, used statistical software to randomly allocate a code of 0 (control) or 1 (intervention) to each of the subregions within each of the 11 DMAs. The other assignments were then made with stratification by DMA, such that each DMA was composed of one control cluster and the remaining as intervention clusters.
Data collection
Clinical research coordinators (CRCs) obtained study data from each patient’s medical chart. Patients in both groups were asked to complete a self-administered questionnaire pertaining to their lifestyle and diabetes-related distress. Distress was measured using the Problem Areas in Diabetes (PAID) scale. CRCs visited each PCP clinic to collect follow-up data, including laboratory results, dates of completed patient appointments, and patients’ next appointment dates.
Interventions
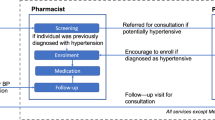
The interventions consisted of sending reminders regarding their regular PCP appointments and providing patients with health education aimed at lifestyle modification via a treatment support center that had been established for these purposes beforehand. Reminders for regular medical visits consisted of a letter sent 1 week before the established next visit day (NVD). If this appointment was missed, another letter was sent 2 weeks after the NVD. If required, a telephone call was made to the patient 4 weeks after the NVD. If the patient did not visit the PCP within 6 weeks of the NVD, the PCP or a clinic staff member contacted the patient by either letter or telephone.
Lifestyle modification intervention was provided to encourage progress toward behavioral changes in diet and exercise. Certified diabetes educators, registered dieticians, or public health nurses participating in the standardized program for behavioral theory on patient education provided counseling, which was tailored for each patient according to his or her PCP’s instructions with regard to the target body weight, recommended food intake, and exercise therapy. Patients received six sessions of lifestyle advice through telephone calls, each lasting between 15 and 30 min. Alternatively, some DMAs trained certified diabetes educators and provided them with a location for face-to-face counseling. With these DMAs, there were four face-to-face advice sessions, each lasting approximately 30 min. Furthermore, the PCPs in the intervention group received feedback letters regarding the indicators for themselves as well as the benchmarks for each indicator. All interventions continued for 1 year.
Outcome measures
The primary study outcome was adherence to regular PCP visits for diabetes treatment. Non-adherence was defined as failure to attend follow-up appointments regularly, that is, failure to visit a PCP within 2 months of the original appointment. The time to the first non-adherence to attend the PCP was defined as the primary outcome measure. The study’s secondary outcome measures were patients’ HbA1c level, random blood glucose level, body mass index (BMI), and systolic and diastolic blood pressure. Other prespecified outcome measures include quality of diabetes treatment, patients’ behavioral stages of change, and patients’ clinical data such as lipid profile and body weight19. Among them, results of quality of diabetes treatment have been previously published20.
Sample size estimation
Based on the main outcome parameter of insufficient adherence to regular PCP appointments, a sample size estimation was established via a power calculation performed according to the method reported by Hayes and Bennett21. As moderate variations in cluster size have little impact on the sample size estimation21, we further assumed that all clusters are of equal size. Based on the results of the previously completed J-DOIT2 pilot study, the effect size of the intervention was estimated to be a 45% reduction in insufficient adherence, an incidence of the primary outcome measure of 71.6 per 1,000 person-years, and a coefficient of variation of 0.43. Based on these assumptions, a two-tailed alpha of 5%, and a beta of 10%, it was estimated that if 125 patients were recruited per cluster, 15 clusters per arm would be needed, requiring a sample of at least 3,750 patients.
Statistical analysis
The characteristics of patients in the intervention and control groups were calculated as proportions, means, and standard deviations. Because randomization was at the cluster level, patient-level characteristics were not likely to be as balanced as they would be if randomization had been performed at the patient level. We examined the balance of covariates using fixed-effects linear regression for continuous confounders (e.g., age) and fixed-effects binomial or multinomial logistic regression for categorical confounders (e.g., gender), with consideration of clustering within each DMA. Adherence to regular visits was analyzed as the time from entry into the study until the first event, that is, the first missed appointment. Patient data were censored at the end of the follow-up period for this trial (1 year). To test the study hypothesis, we used a Cox proportional hazard model that included a Huber–White sandwich estimator for clustered data. Primary data were analyzed using the intention-to-treat principle. Next, to test the hypothesis that the effectiveness of the intervention varied according to individual patient characteristics (age group [40–59 vs. 60–65 years], gender [male vs. female], HbA1c level [<8% vs. ≥8%], working status [working vs. nonworking], and PAID quartiles), we conducted a stratified analysis of these covariates. The HbA1c data were converted to equivalent values of the National Glycohemoglobin Standardization Program according to a statement made by the Japan Diabetes Society22.
We used linear regression, taking clustering into account, to estimate the association between the intervention and secondary outcomes (HbA1c level, random blood glucose level, systolic and diastolic blood pressure, and BMI). The measure of effect was the mean difference in outcomes derived by subtracting the baseline value from that of the last observation between the intervention and control groups. All statistical tests were two sided with an alpha level of 0.05. All analyses were performed using Stata/MP version 12.0 (Stata Corporation, College Station, TX, USA).
Results
Figure 1 summarizes this trial’s allocation of study clusters and eligible patients. Study participants were recruited between July 2009 and September 2009. After an intervention and a control group were established within each of the 11 eligible DMAs by random assignment, all 1,091 and 1,387 patients in the collective intervention and control groups, respectively, were assessed for study eligibility. From these groups, 971 and 1,265 patients who were determined to be eligible were assigned to the intervention and control groups, respectively. All 22 clusters were followed for 1 year (until October 2010).

Flow chart of study cluster enrollment and patient selection procedures. DMAs, district medical associations.
Patient baseline characteristics are presented in Table 1. The mean patient age was 56.5 years; 37.5% were women, and their mean HbA1c level was 7.4%, with no significant differences between the intervention and control groups with one exception: patients in the intervention group were more likely to be administered diabetes medication of any kind (P = 0.049). Protocol compliance was 86.8% (5,097 of 5,872) for reminders sent 1 week before the scheduled NVD, 28.9% (486 of 1,680) for those sent 2 weeks after the NVD, 48.2% (143 of 331) for those sent 4 weeks after the NVD, and 76.7% (46 of 60) for those sent 6 weeks after the NVD. On an average, patients in the intervention group received 4.4 sessions on lifestyle modification.
During a median follow-up period of 1.1 years, there were 135 patients with insufficient adherence to PCP visits. As illustrated by the Kaplan–Meier curves for the intervention and control groups (Fig. 2), the primary study outcome of a reduction in the incidence of insufficient adherence to regular attendance was significantly different between the intervention and control groups (P < 0.001; log-rank test). Specifically, the frequencies of insufficient adherence were 82.5 per 1,000 person-years and 30.4 per 1,000 person-years in the control and intervention groups, respectively (Table 2). The estimated hazard ratio, defined here as the risk of insufficient adherence by the intervention group vs. the control group, was 0.37 (95% confidence interval [CI], 0.23–0.58; P < 0.001). This significant effect of intervention persisted even after adjustment for the type of diabetes therapy.

Kaplan–Meier estimates of insufficient adherence to primary care attendance by patients with diabetes. Solid line: control group; broken line: intervention group.
Table 2 and Fig. 3 summarize the analysis results stratified according to subgroup. These results showed that the effect of intervention was not significantly modified by age, gender, extent of glycemic control, employment status, or diabetes distress as measured by the PAID scale. Patients in the intervention group experienced significant reductions in HbA1c level (−0.17%; 95% CI, −0.27 to −0.07; P = 0.004), random blood glucose level (−8.15 mg/dl; 95% CI, −11.29 to −5.03; P < 0.001), and BMI (−0.21; 95% CI, −0.33 to −0.10; P = 0.002), but not in systolic (P = 0.292) or diastolic (P = 0.761) blood pressure.

Effect of intervention on the primary outcome stratified according to the baseline characteristics. Black squares: point estimates of the hazard ratio; bars: confidence intervals. PAID, problem areas in diabetes scale.
Discussion
To date, very few data have been reported that support the strategy of providing interventions as an effective method for increasing patient adherence to a treatment regimen23. One example of a positive outcome was from a before-after study, which suggested a benefit from providing information on appointments, mainly by a telephone call24. To our knowledge, our study is the first cluster-randomized controlled trial to evaluate the effectiveness of a triple-faceted intervention for improving the adherence to regularly scheduled primary care visits by diabetes patients. Our results showed that such a coordinated intervention reduced the risk of insufficient adherence to regular primary care visits in patients with diabetes by 63%.
A plan for continuing care is an essential feature in the management of patients with diabetes. Clinical guidelines recommend regular visits be scheduled for better diabetes care25; however, controlled clinical trials addressing adherence to regular visits by patients with diabetes are rare. Prior to our study, only one reported patient-level randomized controlled trial had attempted to address this issue26. This previous study evaluated 854 noninstitutionalized patients with diabetes who were more than 15 years old and were treated with insulin or oral hypoglycemic agents. These patients had attended a hospital outpatient department in Indianapolis within the previous year and had another scheduled appointment on record. The intervention was similar to the one presented here: patients were provided reminders of appointments, and if a patient missed his or her appointment, he or she was contacted again by telephone or letter. However, the overall reduction in the number of missed appointments in that study was not statistically significant. In contrast, our study showed that, in our patient population, insufficient adherence to regular visits is an almost entirely correctable problem.
There are several possible explanations for the difference in outcomes between the two studies. First, as shown in previous research, the quality of the patient–provider relationship is associated with patient adherence to diabetes treatment27. In this regard, lifestyle modification intervention, one of the components of our study, was offered to subjects based on their specific stages according to the transtheoretical model of behavior change28. This approach may have helped establish good healthcare provider–patient relationships, which in turn may have improved patient adherence to their regular PCP appointments. Second, the previous study was a patient-level randomized controlled trial, whereas our study used a cluster-randomized controlled trial design, which reduced the contamination of the intervention effect among study participants. Third, the difference in the study settings may have also influenced the effectiveness of the intervention. Our study was conducted in the primary care setting rather than in the hospital, which may help explain the difference in efficacy, which might have facilitated the ability to improve the patient experience and their adherence to the intervention.
We found that the combination of patient education with appointment reminders and benchmarking of PCP procedures was effective in maintaining adherence to regular clinic visits, although this result needs to be interpreted cautiously. In a subgroup analysis, the effect of the intervention was not different between different age groups, but this result does not guarantee that the intervention will be effective in age groups other than those included in this trial. Furthermore, we did not include patients younger than 40 years, since the intervention was ineffective in this age group during an earlier phase of the trial. In fact, intervention tended to worsen the adherence in this generation, although the difference was not statistically significant29. Additional studies are required to investigate other methods of improving the adherence of younger patients to continuous diabetes care.
This trial also showed that education on lifestyle modification was effective in improving HbA1c level, random plasma glucose level, and BMI, but not for blood pressure control. Previous studies have produced contradictory results on the effectiveness of lifestyle modification intervention in improving blood pressure. The Turin study30, a 5-year randomized controlled trial that evaluated the effectiveness of structured group education programs in patients with diabetes, showed that such programs are effective in reducing BMI and HbA1c levels and improving patient quality of life but not for improving fasting plasma glucose levels. However, this study involved a relatively small number of patients (n = 120).
Insufficient adherence to regular PCP appointments might have a direct influence on clinical outcomes because it reduces the continuity of care, resulting in missed opportunities to check for comorbidities or titrate medications; delays appropriate interventions and referrals to specialists by PCPs; and hinders the development of a good healthcare provider–patient relationship31. Development of a sustained, reliable relationship may influence both patient and physician behaviors in a manner that would improve self-care and glucose control. From the patient perspective, a good relationship may improve their sense of trust in their PCP. As this relationship improves, patients may become more comfortable in divulging critical information pertaining to their social context that is relevant to their health and healthcare. This information may improve physician decision-making concerning patient’s disease management and could contribute to the effectiveness of the intervention on secondary outcomes.
This study has several strengths. First, it evaluated a large number of patients and included DMAs located throughout Japan. Second, the intervention was designed to be implemented in the primary care setting. Third, the trial had a robust cluster design that effectively reduced contamination between practices. There are several limitations that merit to discuss. First, the intervention and control groups were not well matched with respect to the type of diabetes therapy being administered. However, such an imbalance is not uncommon in cluster randomized controlled trials32. Moreover, the significant effect of the intervention persisted even after adjusting for this difference. Second, our sample size did not reach the goal based on the sample size calculation, possibly resulting in insufficient power and thus imprecise findings. However, we observed a statistically significant risk reduction probably because the effect size was much larger than we expected.
In conclusion, this study demonstrates that a triple-faceted intervention consisting of healthcare education aimed at modifying lifestyle and an appointment reminder system with benchmarking of PCP procedures can significantly decrease poor patient compliance and improve patient adherence to regularly scheduled PCP appointments. Because it is unclear if specific aspects of the intervention were responsible for this outcome, future research should attempt to identify the efficacy of the individual components of intervention. Widespread application of the intervention program evaluated in this study may result in a large decrease in the patient dropout rate from participation in regular diabetes treatment, a key to the prevention of long-term diabetic complications33, potentially leading to large reductions in medical costs.
Data availability
To comply with our privacy and data security policies, the data of current study are available only for researchers who meet our criteria for access to confidential data. For researchers who have an interest in using the data, please contact the corresponding author.
Change history
19 October 2020
An amendment to this paper has been published and can be accessed via a link at the top of the paper.
References
Ikeda, N. et al. What has made the population of Japan healthy? Lancet 378, 1094–1105, https://doi.org/10.1016/S0140-6736(11)61055-6 (2011).
King, H., Aubert, R. E. & Herman, W. H. Global burden of diabetes, 1995–2025: prevalence, numerical estimates, and projections. Diabetes. Care. 21, 1414–1431 (1998).
Amos, A. F., McCarty, D. J. & Zimmet, P. The rising global burden of diabetes and its complications: estimates and projections to the year 2010. Diabet. Med. 14(Suppl 5), S1–85 (1997).
Whiting, D. R., Guariguata, L., Weil, C. & Shaw, J. IDF diabetes atlas: global estimates of the prevalence of diabetes for 2011 and 2030. Diabetes Res. Clin. Pract. 94, 311–321, https://doi.org/10.1016/j.diabres.2011.10.029 (2011).
Ministry of Health. National Diabetes Survey, http://www.mhlw.go.jp/toukei/kouhyo/indexkk_4_1.html (1997).
Ministry of Health & Labour and Welfare. National Health and Nutrition Survey, http://www.mhlw.go.jp/bunya/kenkou/eiyou09/01.html (2007).
Coutinho, M., Gerstein, H. C., Wang, Y. & Yusuf, S. The relationship between glucose and incident cardiovascular events. A metaregression analysis of published data from 20 studies of 95,783 individuals followed for 12.4 years. Diabetes Care 22, 233–240 (1999).
Gaede, P. et al. Multifactorial intervention and cardiovascular disease in patients with type 2 diabetes. N. Engl. J. Med. 348, 383–393 (2003).
Noto, H., Tsujimoto, T., Sasazuki, T. & Noda, M. Significantly increased risk of cancer in patients with diabetes mellitus: a systematic review and meta-analysis. Endocr. Pract. 17, 616–628, https://doi.org/10.4158/ep10357.ra (2011).
Ministry of Health & Labour and Welfare. The second Health Japan 21 project, http://www.mhlw.go.jp/bunya/kenkou/dl/kenkounippon21_02.pdf (2012).
Masuda, Y. et al. Personal features and dropout from diabetic care. Env. Health Prev. Med. 11, 115–119, https://doi.org/10.1265/ehpm.11.115 (2006).
Cramer, J. A. A systematic review of adherence with medications for diabetes. Diabetes Care 27, 1218–1224 (2004).
Tunceli, K., Iglay, K., Zhao, C., Brodovicz, K. G. & Radican, L. Factors associated with adherence to oral antihyperglycemic monotherapy in patients with type 2 diabetes mellitus in the United Kingdom. Diabetes Res. Clin. Pract. 109, e27–31, https://doi.org/10.1016/j.diabres.2015.05.031 (2015).
Hammersley, M. S., Holland, M. R., Walford, S. & Thorn, P. A. What happens to defaulters from a diabetic clinic? Br. Med. J. 291, 1330–1332 (1985).
Karter, A. J. et al. Missed appointments and poor glycemic control: an opportunity to identify high-risk diabetic patients. Med. Care 42, 110–115, https://doi.org/10.1097/01.mlr.0000109023.64650.73 (2004).
Jacobson, A. M., Adler, A. G., Derby, L., Anderson, B. J. & Wolfsdorf, J. I. Clinic attendance and glycemic control. Study of contrasting groups of patients with IDDM. Diabetes Care 14, 599–601 (1991).
Fukuda, H. & Mizobe, M. Impact of nonadherence on complication risks and healthcare costs in patients newly-diagnosed with diabetes. Diabetes Res. Clin. Pract. 123, 55–62, https://doi.org/10.1016/j.diabres.2016.11.007 (2017).
Graber, A. L., Davidson, P., Brown, A. W., McRae, J. R. & Woolridge, K. Dropout and relapse during diabetes care. Diabetes Care 15, 1477–1483 (1992).
Izumi, K. et al. Multifaceted intervention to promote the regular visiting of patients with diabetes to primary care physicians: rationale, design and conduct of a cluster-randomized controlled trial. The Japan Diabetes Outcome Intervention Trial-2 study protocol. Diabetol. Int. 1, 83–89 (2010).
Hayashino, Y. et al. A cluster randomized trial on the effect of a multifaceted intervention improved the technical quality of diabetes care by primary care physicians: The Japan Diabetes Outcome Intervention Trial-2 (J-DOIT2). Diabet. Med. 33, 599–608, https://doi.org/10.1111/dme.12949 (2016).
Hayes, R. J. & Bennett, S. Simple sample size calculation for cluster-randomized trials. Int. J. Epidemiol. 28, 319–326 (1999).
Kashiwagi, A. et al. International clinical harmonization of glycated hemoglobin in Japan: From Japan Diabetes Society to National Glycohemoglobin Standardization Program values. J. Diabetes Investigation 3, 39–40, https://doi.org/10.1111/j.2040-1124.2012.00207.x (2012).
Vermeire, E. et al. Interventions for improving adherence to treatment recommendations in people with type 2 diabetes mellitus. Cochrane Database of Syst. Rev., CD003638, https://doi.org/10.1002/14651858.CD003638.pub2 (2005).
Hardy, K. J., O’Brien, S. V. & Furlong, N. J. Information given to patients before appointments and its effect on non-attendance rate. BMJ 323, 1298–1300 (2001).
Association, A. D. Standards of medical care in diabetes–2013. Diabetes Care 36(Suppl 1), S11–66, https://doi.org/10.2337/dc13-S011 (2013).
Smith, D. M., Weinberger, M. & Katz, B. P. A controlled trial to increase office visits and reduce hospitalizations of diabetic patients. J. Gen. Intern. Med. 2, 232–238 (1987).
Ciechanowski, P. S., Katon, W. J., Russo, J. E. & Walker, E. A. The patient-provider relationship: attachment theory and adherence to treatment in diabetes. Am. J. Psychiatry 158, 29–35 (2001).
Prochaska, J. O. & Velicer, W. F. The transtheoretical model of health behavior change. Am. J. health promotion: AJHP 12, 38–48 (1997).
Hayashino, Y. et al. Depressive Symptoms, not Completing a Depression Screening Questionnaire, and Risk of Poor Compliance with Regular Primary Care Visits in Patients with Type 2 Diabetes: The Japan Diabetes Outcome Intervention Trial 2 (J-DOIT2) Study Group. Exp Clin Endocrinol Diabetes, https://doi.org/10.1055/s-0030-1265213.
Trento, M. et al. A 5-year randomized controlled study of learning, problem solving ability, and quality of life modifications in people with type 2 diabetes managed by group care. Diabetes Care 27, 670–675 (2004).
Parchman, M. L., Pugh, J. A., Noel, P. H. & Larme, A. C. Continuity of care, self-management behaviors, and glucose control in patients with type 2 diabetes. Med. Care 40, 137–144 (2002).
Davies, M. J. et al. Effectiveness of the diabetes education and self management for ongoing and newly diagnosed (DESMOND) programme for people with newly diagnosed type 2 diabetes: cluster randomised controlled trial. Bmj 336, 491–495, https://doi.org/10.1136/bmj.39474.922025.BE (2008).
Lerman, I. Adherence to treatment: the key for avoiding long-term complications of diabetes. Arch. Med. Res. 36, 300–306, https://doi.org/10.1016/j.arcmed.2004.12.001 (2005).
Acknowledgements
The authors thank Dr. Maki Goto for her helpful support in preparing the manuscript; Dr. Ryotaro Bouchi for his helpful advice in preparing the revised manuscript. We also appreciate the support of the J-DOIT2 study group including the members of the district medical associations of Shimotsuga County and City (Tochigi Prefecture), Chiba City (Chiba Prefecture), Itabashi Ward (Tokyo Metropolis), Iida (Nagano Prefecture), Takaoka City (Toyama Prefecture), Motosu (Gifu Prefecture), Omihachiman City and Gamo County (Shiga Prefecture), Yodogawa Ward of Osaka City (Osaka Prefecture), Tokushima City (Tokushima Prefecture), Kokura of Kitakyushu City (Fukuoka Prefecture), and Naha City (Okinawa Prefecture). This work was supported by grants from the Japan Agency for Medical Research and Development (Practical Research Project for Life-Style related Diseases including CVD and Diabetes); the Ministry of Health, Labour and Welfare of Japan (Strategic Outcomes Research Program for Research on Diabetes; Comprehensive Research on Life-Style Related Diseases including CVD and Diabetes H25-016); and the Japan Society for the Promotion of Science KAKENHI (Grant‐in‐Aid for Scientific Research) grant number 15H04779. The funding source had no role in study design, data collection, data analysis, data interpretation, the writing of the report, or the decision to submit the article for publication.
Author information
Authors and Affiliations
Contributions
M.N., Y.H., K.Y., H.S., K.I. and M. Kobayashi conducted the study. M.N., Y.H., A.G. and M. Kato analysed the data, and drafted the manuscript. K.Y., H.S., K.I. and M. Kobayashi critically reviewed the manuscript and added important intellectual content.
Corresponding author
Ethics declarations
Competing interests
The authors have read the journal’s policy and have the following conflicts: Dr. Noda serves as a chairperson of the evaluation committee of the Evidence-based Practice Guideline for the Treatment of Diabetes in Japan edited by Japan Diabetes Society. He also served as a member of the editorial committee of the Treatment Guide for Diabetes in Japan edited by Japan Diabetes Society and the Health Japan 21 (the second term) plan development committee. Dr. Noda received honoraria from Taisho Toyama Pharmaceutical Co. Ltd, MSD K.K., Novo Nordisk Pharma Ltd, outside of the submitted work. Other authors declare no competing financial or non-financial interest.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Noda, M., Hayashino, Y., Yamazaki, K. et al. A cluster-randomized trial of the effectiveness of a triple-faceted intervention promoting adherence to primary care physician visits by diabetes patients: J-DOIT2 large-scale trial (J-DOIT2-LT). Sci Rep 10, 2842 (2020). https://doi.org/10.1038/s41598-020-59588-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-020-59588-x
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
