
Abstract
Mosquito-borne diseases remain a major cause of morbidity and mortality across the tropical regions. Despite much progress in the control of malaria, malaria-associated morbidity remains high, whereas arboviruses—most notably dengue—are responsible for a rising burden of disease, even in middle-income countries that have almost completely eliminated malaria. Here I discuss how new interventions offer the promise of considerable future reductions in disease burden. However, I emphasize that intervention programmes need to be underpinned by rigorous trials and quantitative epidemiological analyses. Such analyses suggest that the long-term goal of elimination is more feasible for dengue than for malaria, even if malaria elimination would offer greater overall health benefit to the public.
Similar content being viewed by others


Main
Deaths from malaria have almost halved since 20001,2,3, despite rapidly growing populations in many endemic regions. Improvements in vector control and (to a lesser extent) treatment are the principal drivers behind this decline4,5, however, development—leading to improved housing and increased urbanization across the tropics—has also been an important contributing factor6. The declines have been particularly marked outside sub-Saharan Africa, with only 10% of malaria deaths now occurring outside this region7. Over the same period, the burden of disease from dengue has risen markedly, often in those countries that have the largest reductions in malaria disease8,9 (Fig. 1). Part of the increase in burden reflects population growth and urbanization in the tropics, but greater connectivity of human populations10 (which leads to all four dengue serotypes now regularly being detected in all endemic countries11), entomology (Aedes aegypti, the principal dengue vector, is more highly adapted to urban environments12) and climate change (increasing the geographical limits of endemic transmission13) have also played a part.

WHO estimates shown for malaria, combining estimates from the 2015 and 2017 World Malaria Reports3,7; other estimates1,8 are substantially higher but show the same overall trends. In the absence of WHO estimates, estimates of dengue-associated mortality from the 2016 Global Burden of Disease study are shown8. Top, malaria deaths in Africa. Bottom, dengue deaths and malaria deaths outside Africa.
The number of malaria deaths globally remains over 30-fold higher than those from dengue (Fig. 1), although this ratio is less extreme if one only considers disease burden outside Africa. Furthermore, given the availability of highly effective artemisinin-based malaria treatments, a large proportion of remaining mortality induced by malaria reflects gaps in access to treatment or suboptimal diagnosis4,5. Conversely, dengue affects urban populations with better (although often not perfect) access to healthcare. No effective dengue antiviral drugs or monoclonal antibodies are currently available for dengue treatment, although improvements in case management have led to substantial reductions in case fatality ratios in situations in which the current best standard of care is available14. The unpredictability and explosive nature of dengue epidemics also imposes substantial stresses on healthcare systems, and can cause a lot of anxiety for the public, particularly in contexts in which the burden of disease from most other infections has been markedly reduced in recent decades through vaccination and access to treatment.
Emerging arboviral infections have also caused substantial public concern in recent years15. Chikungunya emerged in Latin America and the Caribbean in 201316,17, followed by Zika in 201518. Both caused large-scale epidemics over an approximately two-year period, before the accumulation of population immunity in populations across the region led to marked decreases in incidence19,20,21. Despite availability of a highly effective vaccine, yellow fever has also caused relatively large, unpredicted epidemics in Angola and Brazil in the last two years, necessitating rapid large-scale immunization campaigns22. However, the true burden of disease caused by both chikungunya and Zika is highly uncertain, in large part because of a lack of systematic surveillance across much of the world and, for Zika, the very mildly symptomatic nature of most infections. The health consequences of infection with both viruses remain poorly characterized and it is unclear to what extent either virus can be considered truly endemic in the human population globally, or whether these viruses, like yellow fever, are dependent on a sylvatic cycle of transmission. These gaps in our knowledge18 make assessing the public health need for effective interventions highly challenging.
The perceived increasing threat (and disease burden) posed by arboviral infections and the recent global emphasis on reducing the disease burden of malaria has led to increasing investment in the development of new interventions and the intensification of current vector control in many endemic low- and middle-income countries (LMICs). The first vaccines for both malaria and dengue offer some promise for disease reduction but their imperfect and complex efficacy profiles mean that neither represents a panacea and their uptake has therefore been slow23,24,25,26,27. However, the accelerated roll-out of long-lived insecticide-treated nets (LLINs) across sub-Saharan Africa over the last decade has led to major declines in malaria incidence, with improved treatment further reducing disease burden4. This is not to imply that these gains can be taken for granted—insecticide resistance28 and/or failure to sustain intervention coverage pose risks of rapid bounce-back. However, by contrast, the evidence that current vector control measures for dengue are having significant impact is limited at best29,30,31,32. Although differences in the ecology of the principal vectors (for example, in landing periodicity33) for the two classes of infections clearly affect the effectiveness of different interventions, I propose that the failure of dengue control to date is principally a consequence of intrinsic differences in the epidemiology of arboviral and malaria infections. These differences necessitate fundamentally different goals for control policy planning for these two classes of infections. I will then review how new technologies for vector control that are currently under development offer the potential to deliver pronounced reductions in disease burden and potentially even elimination in the coming 10–20 years.
Goals of vector control
For all infections, the goals of control are the reduction of disease incidence and, preferably, transmission. Elimination requires reducing transmission to levels that are less than self-sustaining: in the parlance of mathematical epidemiology, reducing the basic reproduction number (the number of secondary infections caused by a typical index infection in a naive population), R0, to below 1. Given the lack of vaccines with high efficacy for all mosquito-borne infections other than yellow fever and Japanese encephalitis, the main goal of public health interventions for these infections has been to reduce human exposure through vector control. The rationale for malaria is clear: in high transmission areas, a child might be infected multiple times in a year, with each new infection posing a risk of disease. Reducing exposure by a certain proportion then leads to an immediate and comparable reduction in the incidence of disease—a reduction that can be further improved by improving access to effective antimalarial therapy. Clinical immunity nuances this picture but does not fundamentally change the broad conclusion—although exposures at a later age have a lower risk of disease (severe disease particularly), this risk declines gradually, and both age and exposure have a role in this gradual decline34.
The same rationale does not hold true for arboviral infections. Unlike malaria (although controversy remains about the extent to which that pathogen can be viewed as a collection of semi-independent antigenically diverse strains35), all arboviruses are thought to generate neutralizing homotypic immunity after infection; this means that individuals can experience only one infection with each virus in their lives. Dengue is composed of four distinct (but immunologically cross-reactive) viral serotypes, and therefore four infections are possible. However, secondary dengue infections are responsible for the great majority of severe disease36,37,38,39, with tertiary and quaternary infections thought to be largely asymptomatic40. The immunizing nature of arboviral infections has profound consequences for vector control. Completely preventing an individual from being exposed in one year has no impact on lifetime disease risk if a high-level risk of exposure resumes the following year—the only effect of such transient interventions is to postpone infection. The same reasoning applies to partially effective controls. Consider a high transmission setting in which individuals have a 20% risk of dengue infection each year. On average, children will be 5-years old when they experience their first infection, and about 12-years old when they experience their second. Imagine a vector control intervention that reduces exposure by 50%—thus reducing the infection risk to 10% per year. The net long-term effect of this intervention is only to increase the age at which individuals experience their first and second infections—to 10 and 23 years, respectively, for this example. This may paradoxically increase overall disease burden, if dengue disease severity increases with age41.
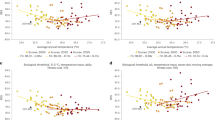
This argument can be formalized; Fig. 2a shows the relationship between disease risk and the effectiveness of vector controls at reducing exposure predicted by previously validated mathematical models of dengue and malaria transmission. This malaria model has been used extensively to inform control planning, and was validated against historical prevalence and incidence data both in the absence and presence of control measures42,43,44. The dengue model was previously fitted to the Sanofi–Pasteur dengue vaccine trial data and used to explore the potential impact of large-scale use of the Sanofi–Pasteur vaccine and Wolbachia23,45. For malaria, reductions in disease increase almost linearly with coverage. For dengue, the response curve is highly nonlinear, with marginal reductions in lifetime disease risk until the level of exposure reduction is sufficient to reduce R0 close to 1 (around 70% effectiveness, for this example). I conclude that for vector controls against dengue (or other arboviruses) to have a major long-term impact, they must come close to stopping sustained transmission—that is, achieving elimination. Figure 2a also highlights that elimination, in theory, should require considerably less effort for dengue than for malaria—in high transmission settings, R0 for dengue is around 4, whereas for malaria it is over 100 (with a large degree of local geographical heterogeneity for both infections4,46,47). Therefore, vector control for dengue needs to reduce exposure by 80% to achieve elimination, but for malaria the reduction required is over 99%.

a, Published mathematical transmission dynamic models of each disease23,42 are used to show the long-term effect of varying (i) coverage levels of LLINs for malaria in a sub-Saharan African hyperendemic setting with an (assumed constant) entomological inoculation rate in the absence of controls of 500 (R0 of approximately 700); (ii) the proportion of dengue exposure blocked by a hypothetical dengue vector control measure (100% coverage assumed) in a setting in which seroprevalence in 9-year olds is 80% on average before the introduction of controls (R0 of approximately 4). b, The temporal impact of controls on annual disease incidence. Controls are introduced in year 20 (50% LLIN coverage assumed for malaria, 50% effective controls for dengue). Inter-annual climate variation is not included in either model, so malaria incidence is constant over time before interventions. Dengue incidence varies markedly year-to-year due to semi-chaotic serotype cycling.
However, focusing only on the long-term effects of interventions neglects the transient temporal effects that the large-scale introduction of an intervention may have on transmission (simulated in Fig. 2b using the models used to generate Fig. 2a). Short- and long-term impacts differ less for malaria than dengue because of the more limited effect of host immunity in modulating disease transmission. The loss of clinical immunity largely explains the rebound in malaria in Fig. 2b. But herd-immunity is fundamental to dengue transmission dynamics; in endemic areas, at any point in time much of the population is immune to any one serotype, so when a new epidemic occurs, it only affects the minority of the population (typically children) who have not yet acquired immunity. Over time, a dynamical equilibrium is reached between viral transmission rates and the level of population immunity, which leads to the effective reproduction number (the average number of secondary infections caused by a typical index case in the presence of population immunity), R, to hover around 1. An exception to this is found in marginally endemic areas that have not yet been affected by all serotypes, where the initial epidemic following invasion with a novel serotype can be much larger than typical48; however, following such an initial epidemic, the resulting immunity also causes R for the invading serotype to fall below 1.
In this context, suddenly introducing a new intervention population-wide disrupts this equilibrium, even if the reduction in transmission achieved is insufficient to cause long-term elimination. An intervention that achieves a sustained 20% reduction in exposure would initially reduce R from 1 to 0.8—leading to a temporary cessation of transmission. New births into the population then gradually reduce population immunity, increasing R, and sustained transmission would resume once R once again reached 1. With an annual birth cohort size of, for example, 2% of the total population, it would take up to 10 years for R to increase from 0.8 back to 1. Stopping dengue epidemics for such a time clearly sounds like an impressive outcome, but it is important to note that it would not necessarily lead to a reduction in lifetime disease risk for individuals in the affected population unless more effective interventions could be introduced before the end of the 10-year interim period.
Transient impacts on transmission also need to be taken into account when interpreting data from cluster-randomized trials of vector control interventions. The effect size that is observed in trials of transmission-reduction interventions (such as community mobilization49) over timescales of 1 to 2 years will implicitly include the large transient effect on incidence described above, and thus short-term measured effectiveness (for example, reduction in infection rates over one year) would be expected to be considerably greater than the underlying long-term effectiveness of the intervention (as quantified by the fractional reduction in the achieved R0).
Most of the above arguments around the goals and probable impact of interventions against dengue also hold for chikungunya and Zika, albeit the period between epidemics is much longer and more unpredictable than for dengue18. There is one exception, that is, protecting vulnerable populations for a short period. Congenital Zika syndrome is predominantly associated with maternal exposure to Zika in the first trimester of pregnancy50,51. Therefore, an intervention that targets individuals (for example, spatial repellents) that reduces exposure for a three-month period might achieve a substantial reduction in the burden of disease caused by a Zika epidemic, even if that intervention has a minimal effect on community levels of transmission. However, just as vector controls that target community transmission require rigorous assessment in randomized trials, so do interventions that aim to reduce personal exposure.
The high level of geographical, environmentally driven heterogeneity in the R0 of mosquito-borne infections provides nuances, but it does not invalidate these arguments. However, such heterogeneity—and the existence of hotspots with high transmission rates—increases the challenges involved in achieving elimination, albeit with the upside that control in areas with lower transmission rates may be easier than expected from geographically coarse estimates of transmission intensity.
Assessing effectiveness of vector control measures
Why then has there been so little recent success in controlling dengue (especially in LMICs), whereas major reductions in disease for malaria have been achieved? Singapore (which is not a LMIC) is perhaps the only formerly hyper-endemic country in recent decades to have achieved high levels of dengue control (although Cuba achieved similar success in the 1970s)52. However, even Singapore has experienced increases in the incidence of dengue incidence in recent years associated with declining levels of population immunity53. Nevertheless, substantial reductions in malaria transmission have been achieved in some of the poorest countries of the world in the last decade4,5.
Part of the answer lies in differences in vector ecology. Anopheles gambiae, the primary vector of Plasmodium falciparum in sub-Saharan Africa, principally bites at night (and therefore inside houses), which means that LLINs54,55 (and indoor residual spraying (IRS)56,57) are highly effective at reducing human exposure. A. aegypti bites during the day (with peaks of activity in the morning and afternoon) both inside and outside houses33. Furthermore, the mating patterns and breeding site preferences of A. aegypti are better adapted to urban landscapes58 than most anopheline species (although there is evidence of urban adaptation of the latter59).
However, while the ecology of A. aegypti limits the effectiveness of ‘simple’ interventions such as bednets30, vector control for arboviruses has also suffered from a profound lack of rigorous evidence to support the effectiveness of the individual measures that are currently in use29,30,31,32,52. In contrast to malaria, for which large cluster-randomized trials with human infection endpoints generated the necessary evidence base to support the scale-up of LLIN and IRS use, randomized trials of vector control approaches for dengue are mostly absent, or have typically been underpowered and only measured entomological rather than epidemiological (that is, human disease) endpoints32. ‘Integrated vector management’ is the recommended approach for vector control of both malaria and dengue, defined as “a rational decision-making process for the optimal use of resources for vector control”60. Ironically, the evidence does not currently exist to make rational decisions for dengue vector control, caused by a lack of trial data that support the effectiveness of current control measures at reducing dengue disease.
Most of the current activities to develop vector control strategies against dengue across the tropics are therefore driven more by the understandable hope that reducing mosquito numbers will only benefit public health, than by a quantitative evidence base that directs investments in vector control towards intervention policies that will result in a substantial public health impact. Furthermore, any impact that such interventions might have is often decreased by a tendency of public health authorities to implement vector control measures in response to ongoing dengue epidemics, rather to sustain consistent control all year round. For the reasons outlined in the previous section, reactive short-lived interventions will at best protect individuals transiently, but will leave them susceptible to infection during the next epidemic. Again, Singapore is perhaps the exception—both in terms of the intensity of vector control activities (and the resources made available to sustain these activities) and the mostly consistent, sustained nature of their implementation53.
In recent years, these shortcomings have been increasingly recognized, culminating in the Vector Control Advisory Group of the WHO (World Health Organization) issuing new guidance that specifies that data from randomized trials with epidemiological endpoints will be required for WHO to recommend new interventions in future61. Furthermore, a number of studies have provided improved guidance on appropriate trial design for dengue vector control trials32,62, highlighting the need for trials to be sufficiently powered to allow for the high degree of spatiotemporal heterogeneity in the incidence of vector-borne diseases, to utilize clusters of sufficient size and spacing to minimize contamination or boundary effects, to have a sufficiently long period of follow-up and to measure epidemiological outcomes. Meeting these requirements is without a doubt challenging, and necessitates that trials are considerably larger (and consequently more expensive) than comparable trials for malaria for which higher and more stable infection rates mean that trials can have a smaller scale.
Indeed, only one dengue vector control intervention study—of the ‘Camino Verde’ approach to community mobilization49—has approached best practice in trial design. However, even in that case, extrapolation of the study results to predict likely long-term, large-scale effectiveness of the intervention is challenging. The small scale of individual clusters (140 households) means that the measured effectiveness may have been affected by individuals living in intervention areas being exposed to infection outside those areas. This ‘contamination’ issue could indicate that the 25–30% reduction in incidence that is seen in the trial underestimates the true effect size that would be seen if the intervention is implemented at larger scale. Conversely, for the reasons outlined in the previous section, the effect size measured in that trial (and all other short-term trials) over the approximately one-year period of follow-up would be expected to incorporate a short-term perturbative effect of the intervention on dengue transmission, and may therefore overestimate long-term effectiveness.
Assessing the likely long-term impact of interventions from relatively short-term trial data are therefore challenging, not only to adjust for contamination and the typically short-term period of follow-up, but also because the transmission intensity (R0) of all mosquito-borne infections show high levels of spatiotemporal variation4,46,63. Therefore, the effect size seen in one context may overestimate the effectiveness of the same intervention applied in a higher transmission intensity context, or underestimate the effects of the intervention in a lower transmission intensity setting. Repeating studies in a range of contexts can mitigate this issue, but this is costly. Mathematical modelling of each trial incorporating details of the transmission context, period of follow-up and cluster size is therefore required to derive estimates of effectiveness that can be used to predict the likely long-term impact of large-scale use of novel interventions across a variety of transmission contexts. Such analyses are not straightforward (and are not a substitute for long-term follow-up data on effectiveness), but have been undertaken for LLINs and IRS for malaria42,44, and for both the CYD-TDV (also known by the trade name Dengvaxia, developed by Sanofi–Pasteur) dengue23,24 and RTS,S (also known by the trade name Mosquirix, developed by GlaxoSmithKline)26,64,65 malaria vaccines, and have been planned for the analysis of trials of Wolbachia as a dengue control measure45,62.
Intervention trials for Zika and chikungunya—whether of vector controls, vaccines or treatment—are even more challenging than for dengue66, because of the longer inter-epidemic period and the highly unpredictable nature of epidemic timing. The traditional trial design of recruiting cohorts of participants, randomizing to intervention or control and monitoring outcomes is therefore likely to be prohibitively expensive—owing to the very large numbers of participants and sites needing to be included. Although model-based analysis of available surveillance data can improve the efficiency of site selection67, reactive designs may be more efficient long-term68. Such a trial might involve gaining ethical and regulatory approval to proceed in advance for a large number of potential trial sites, but only triggering recruitment of participants and intervention implementation at a site once transmission is detected there. That said, given their shared vectors and similar transmissibility, vector control interventions that show high efficacy against dengue are likely to also show comparable efficacy against Zika and chikungunya.
The promise of new interventions
Although the large-scale roll-out of LLINs (together with targeted use of IRS) across sub-Saharan Africa in the last decade has had a major effect on both malaria transmission and disease, even very high coverage levels of these interventions and effective treatment are predicted to be insufficient to eliminate malaria from the highest transmission settings42,44. Insecticide resistance also poses a growing threat28. Mass drug administration can have a very large short-term effect on malaria prevalence69 (by reducing the parasite reservoir in humans), but unless administration at high coverage levels is repeated indefinitely, such effects are transient, since transmission quickly restarts once infection is reimported from untreated areas70. Similarly, seasonal malaria chemoprevention can be highly effective at reducing disease incidence71 but is only appropriate for moderate to high transmission settings with highly seasonal transmission. Furthermore, both mass drug administration and seasonal malaria chemoprevention pose the risk of accelerating the development of wide-scale artemisinin drug resistance in the parasite population.
For dengue, the situation is worse. As described above, there are currently no interventions in large-scale use in LMICs that are likely to be having any major impact on dengue transmission or disease burden52. The intensive vector control interventions adopted largely successfully by Singapore (and high-income settings such as Florida and Queensland) are not easily translated to most LMICs and are likely to be unaffordable for those countries.
In addition to further evaluation and scale-up of current interventions, new intervention technologies are therefore needed to make elimination a feasible policy goal for either dengue or malaria. Over the last two decades, major investment and effort has been committed to the development of both vaccines and novel vector controls, with varying degrees of success.
Vaccines
The CYD-TDV dengue and RTS,S malaria vaccines, the first to be licensed for either infection, are both the result of over twenty years of development effort. Past development efforts have been hindered by the antigenic/immunological complexity of the pathogens and the lack of an obvious commercial market that is sufficient to justify development costs.
In the phase III trial, over two years of follow-up, RTS,S showed 28% (95% confidence interval, 22–33%) efficacy against clinical malaria in children who received three doses over a three-month period, and 36% (95% confidence interval, 31–41%) efficacy in children who additionally received a month-20 booster dose27. Efficacy was a little lower in infants and against severe malaria. Data from phase II and III studies and associated mathematical modelling of these data demonstrated waning of efficacy over time25,27, which was correlated with a decrease in anti-circumsporozoite antibody titres65. This modelling also showed that anti-circumsporozoite antibody titres were a correlate of vaccine-induced protection64,65. The model of vaccine action proposed by these analyses also explained the observed negative correlation between vaccine efficacy and the transmission intensity seen at trial sites, and the faster decay of efficacy seen in higher transmission settings.
For CYD-TDV, two large phase III studies (in Asia and Latin America) both showed approximately 60% efficacy against virologically confirmed clinical dengue disease in the one year following completion of a three-dose vaccine schedule72,73. Efficacy varied by serotype, increased with age and was higher for severe dengue. In the immunological subset of trial participants for whom dengue serological status was measured before the first dose, vaccine efficacy was approximately 75% in individuals who were dengue seropositive, but much lower (and non-significant) in individuals who were dengue seronegative. However, in the first year of long-term follow-up, a statistically significant excess risk of hospitalized dengue disease was observed in vaccine recipients in the youngest age group (2–5 years old). Since no evidence of excess risk was seen in children over 9 years of age in either trial, Sanofi–Pasteur proceeded with submitting the vaccine for regulatory approval with an age indication of use only in children over 9. The most parsimonious and plausible hypothesis that explains these results is that the vaccine acts akin to a silent natural dengue infection23. Seronegative recipients of the vaccine are immunologically primed (akin to natural primary infection), so that their first breakthrough natural infection has the higher severity associated with natural secondary infection in unvaccinated individuals. Conversely, seropositive recipients of the vaccine will have their antibody titres against all four serotypes boosted to the high levels seen after secondary infection in unvaccinated individuals—leading to the first breakthrough infection having the low severity associated with natural tertiary infection.
Mathematical modelling was key to extrapolating from the trial results to assess the likely public health impact of large-scale use of both vaccines, and these analyses had a key role in informing WHO recommendations. For RTS,S, modelling predicted that the vaccine could prevent 1 malaria death per 200 vaccine recipients in moderate to high endemicity settings, making it highly cost-effective compared with many other vaccines26, albeit less cost-effective than LLINs74. WHO recognized the notable potential public health benefits offered by the vaccine, but because of the potential difficulty of delivering a four-dose vaccine schedule and in light of the meningitis safety signal, recommended that large-scale pilot implementation programmes should be conducted75, which are now due to start this year in Ghana, Kenya and Malawi.
For CYD-TDV, modelling indicated that large-scale vaccination might reduce the incidence of symptomatic and hospitalized dengue disease by up to 25% in high transmission intensity settings. However, vaccination was predicted to potentially increase the incidence of hospitalized dengue in low transmission intensity (and thus low seroprevalence) settings23,24. WHO recommendations reflected this risk, suggesting that seroprevalence surveys across the population should be undertaken to assess transmission intensity before vaccination roll-out, and that the vaccine should only be used in settings in which over 70% of vaccine recipients were likely to be seropositive76. These recommendations have now changed to recommend vaccination only in individuals who test seropositive in light of recent data collected by Sanofi–Pasteur that has conclusively demonstrated that seronegative recipients of all ages experience a higher risk of hospitalized dengue disease throughout the long-term follow-up of the trials77.
A number of next-generation dengue and malaria vaccines are currently under development. Two other tetravalent live-attenuated dengue vaccines are currently in phase III trials, with initial results due in the next 12 months. It is unclear whether either will also pose risks of use in seronegative recipients that are similar to CYD-TDV, but similarities in the immunogenicity profiles of all three vaccines makes this a possibility78. A variety of next-generation pre-erythrocytic, blood-stage and transmission-blocking malaria vaccines are under clinical development79, but none have yet entered phase III studies. For both infections, it is therefore arguably unlikely that vaccines will become available in the next decade that can on their own offer the promise of disease elimination. However, that is not to say that vaccines will not have an impact in that time frame: both current vaccines and next generation late-stage candidates may make a considerable contribution to reducing disease burden, combinations of vaccines targeting different parasite life stages may offer synergistic levels of protection against malaria, and some potential exists for the development of ‘universal’ dengue vaccines80.
Novel vector control technologies
New insecticides and delivery systems continue to be developed; and perhaps the most interesting and potentially transformative are those interventions that target obligate life-cycle stages such as sugar or blood feeding. Although not a new idea, attractive toxic sugar bait technology81—which targets sugar-feeding and therefore potentially increases mortality in both male and female mosquitoes—has been advancing rapidly in recent years, with very promising results (at least in anopheline species) seen in recent small-scale trials82. Similarly, ivermectin (and newer longer-lived mosquitocidal drug candidates) could cause substantial suppression of mosquito populations and thus malaria transmission if used as part of a mass treatment intervention83. However, the approaches to vector control that offer the potential of transformative impacts are those that may give long-term (or even permanent) reductions in disease transmission after only a single implementation period, either by reducing mosquito density or reducing vector competence. Two such technologies are under active development: Wolbachia and gene-drive approaches to genetic modification of mosquito species (Fig. 3).

a, Wolbachia-infected mosquitoes are refractory to arboviruses and are able to invade wild-type populations owing to cytoplasmic incompatibility, which leads to crosses between wild-type females and Wolbachia-infected males that are non-viable. b, A Y-linked X-shredder homing-endonuclease gene (HEG) that induces male mosquito survival biases the sex ratio, since a high proportion (here shown as all) of progeny in their crosses with wild-type females are male and will inherit the homing endonuclease genes. c, Illustrative invasion dynamics (releases occurring on day 50). Wolbachia exhibits frequency dependent invasion dynamics, with a threshold frequency determined by fitness costs of infection (here assumed to be 30%). Therefore, invasion can occur when the release size equals 50% of the resident wild-type population, but not at 20%. Mosquitoes that carry Y-linked X-shredder homing endonuclease genes can invade at any frequency (here assumed to be 5% of resident population size) and cause the adult mosquito population to crash.
Wolbachia is a genus of bacteria that naturally infects many insects84, strains of which have been deliberately transfected into A. aegypti mosquitoes. Wolbachia typically transmits vertically by achieving high densities in insect eggs. It confers a frequency-dependent fitness advantage relative to uninfected insects through a mechanism of cytoplasmic incompatibility, which results in crosses between Wolbachia-infected male insects and wild-type females (which would otherwise result in uninfected progeny) that are unviable (Fig. 3a). As a biological vector control measure, this offers the advantage that following initial releases of Wolbachia-infected mosquitoes into a wild-type population, the frequency of Wolbachia infection will rise to very high levels as the released mosquitoes interbreed with wild-type insects (Fig. 3c). Initially, Wolbachia was envisaged as a means to reduce mosquito density, by using a strain (wMelPop) that imposed life-shortening fitness costs on mosquito hosts. However, Wolbachia-infected A. aegypti were also found to have substantially lower vector competence for a broad range of arboviruses85, including dengue86. It is this phenotype that is being exploited—using the less pathogenic wMel strain—by the World Mosquito Program (https://www.worldmosquitoprogram.org/), the leading development project for Wolbachia technology in A. aegypti. Mathematical modelling of data from experimental dengue-infection studies in wMel-infected and wild-type A. aegypti suggests that successful large-scale release and establishment of wMel-infected mosquitoes could reduce dengue transmission intensity (R0) by 75%87—sufficient to achieve elimination of dengue transmission for decades in even high transmission settings, and permanent elimination in low to moderate transmission settings45. Following an extensive programme of small-scale releases, a cluster randomized trial with epidemiological endpoints is now underway in Yogyakarta, Indonesia, with larger non-randomized pilot release studies ongoing in Medellin, Colombia and Rio de Janeiro, Brazil (World Mosquito Program (https://www.worldmosquitoprogram.org/)). Although at a much earlier stage, Wolbachia may also have some potential as a malaria control measure88.
Gene-drive systems for genetically modified mosquitoes89,90 offer similar advantages to Wolbachia in potentially allowing finite releases of modified mosquitoes to invade wild-type populations and rise to high frequencies. A variety of gene drive systems have been explored experimentally and theoretically91,92, but the two most developed technologies are homing endonuclease genes and CRISPR–Cas9. Both rely on homology-dependent repair to be copied from one chromosome to its homologous chromosome during mitosis of germline cells or meiosis89,90. In the vector control context, most attention to date has been given to engineering constructs that supress mosquito populations. Biasing the sex ratio towards males is one approach to achieving this. So-called X-shredder constructs achieve this by expressing endonucleases that are only expressed during spermatogenesis and that cleave the X chromosome, rendering it non-functional93. Inserting such constructs into the Y chromosome would generate a highly invasive genetically modified mosquito that in theory could be introduced into a wild-type population once and would eventually drive that population to extinction94,95 (Fig. 3b, c). In Aedes aegpti, targeting male-determining factors using germline Cas9 expression could give similar results91,96, although research is at an earlier stage compared with anopheline systems. Development of constructs that reduce vector competence is another area of active research89, and a variety of potential targets have been identified for both malaria97,98 and arboviruses99.
Both Wolbachia and gene-drive technologies face several challenges. First, gaining public acceptance and regulatory approval requires a rigorous risk assessment/management process and intensive stakeholder engagement. Such barriers are clearly higher for genetically modified organisms than purely biological control measures such as Wolbachia. Second, use of these interventions will impose intense selection pressures that are likely to drive the evolution of resistance in either the target pathogen (in the case of Wolbachia or vector competence gene drive constructs) or the vector (for population suppression genetic constructs, and perhaps for Wolbachia), and the long-term phenotypic stability of Wolbachia in A. aegypti is yet to be determined. Although several modelling studies have been undertaken, knowledge gaps in vector ecology (for example, regarding the intensity of density-dependent regulation of larval populations, the extent and nature of overwintering mechanisms) make prediction of the impact of these interventions uncertain, especially for gene-drive systems.
Towards elimination
Although current interventions have proven insufficient so far, the novel vector control technologies described above may make elimination of dengue or malaria a feasible goal, even in the highest transmission settings. However, despite the greater progress in controlling malaria than dengue in recent decades, the scale of the challenge to eliminate malaria from the highest transmission hyperendemic settings is larger. The R0 of dengue probably rarely exceeds 6, which means that reducing transmission by approximately 85% should be sufficient for permanent elimination in nearly all settings. Plus, for the reasons outlined above, even interventions that achieve a (sustained) 30% reduction in R0 should cause marked reductions in dengue incidence for decades if applied at sufficient scale—buying time for more effective interventions to be developed. By contrast, the R0 for P. falciparum is in the hundreds in the highest transmission settings, requiring a >99% reduction in transmission intensity to achieve elimination. In addition, there are multiple Plasmodium species that are capable of causing disease in humans, and multiple competent vector species even outside the A. gambiae complex. Nevertheless, even if malaria elimination (and eventual eradication) remains a more distant goal, the vector tools that are currently under development offer the promise of delivering order-of-magnitude reductions in transmission and disease.
While elimination may be the long-term goal of control programmes, disease reduction must remain the priority in the short to medium term. In this context, a wider range of current and near-to-market interventions are relevant—both vector control measures and vaccines. One of the greatest challenges will be to make optimal use of limited resources (especially in low-income settings) to deliver the greatest public health impact. Rigorous epidemiological analysis and mathematical modelling will be key to ensuring such optimal deployment—for the extrapolation of clinical trial data to predict population impact of each intervention in a wider range of settings and in combination with other control measures. Rigorous monitoring and evaluation is also essential to evaluate the real-world effectiveness of interventions. The epidemiology, vector ecology and transmission intensity of both arboviruses and malaria is highly geographically variable, requiring intervention policies to be tailored to the local environment. Modelling has been pivotal in facilitating the characterization of this heterogeneity4,46.
There is unlikely to be a single ‘silver bullet’ intervention that is sufficient to control either class of infections, so policy formulation will require setting-specific selection of interventions from the overall portfolio of available tools that have good evidence supporting their effectiveness. Such optimization should account for the potential synergistic benefits of combining interventions with different mechanisms of action (for example, vector control and vaccines). Intervention effectiveness is only one of the criteria relevant to making that selection—cost, ease of delivery and public acceptability (and thus achievable coverage) are equally important. Such optimization is now possible using integrated disease transmission and health economic models44,74, although reliable surveillance and intervention effectiveness data are essential to calibrate such models. Last, data analytics (spanning dynamical modelling, statistical analysis and machine learning) will become increasingly critical to cope with the ever-growing volumes of surveillance, genomic, remote sensing and other (for example, mobile phone100) data becoming available—to synthesize multiple data streams and derive actionable insights to inform public health policy-making.
References
Gething, P. W. et al. Mapping Plasmodium falciparum mortality in Africa between 1990 and 2015. N. Engl. J. Med. 375, 2435–2445 (2016).
Murray, C. J. L. et al. Global malaria mortality between 1980 and 2010: a systematic analysis. Lancet 379, 413–431 (2012).
WHO. Estimated malaria deaths by region. http://www.who.int/gho/malaria/epidemic/deaths/en/ (2016).
Bhatt, S. et al. The effect of malaria control on Plasmodium falciparum in Africa between 2000 and 2015. Nature 526, 207–211 (2015). This study estimates the impact of different malaria interventions and treatment on infection prevalence and disease incidence.
Cibulskis, R. E. et al. Malaria: global progress 2000–2015 and future challenges. Infect. Dis. Poverty 5, 61 (2016).
Tatem, A. J., Gething, P. W., Smith, D. L. & Hay, S. I. Urbanization and the global malaria recession. Malar. J. 12, 133 (2013).
WHO. World malaria report 2017. http://www.who.int/malaria/publications/world-malaria-report-2017/en/ (2017).
GBD 2016 Causes of Death Collaborators. Global, regional, and national age–sex specific mortality for 264 causes of death, 1980–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet 390, 1151–1210 (2017).
Stanaway, J. D. et al. The global burden of dengue: an analysis from the Global Burden of Disease Study 2013. Lancet Infect. Dis. 16, 712–723 (2016).
Tian, H. et al. Increasing airline travel may facilitate co-circulation of multiple dengue virus serotypes in Asia. PLoS Negl. Trop. Dis. 11, e0005694 (2017).
Messina, J. P. et al. Global spread of dengue virus types: mapping the 70 year history. Trends Microbiol. 22, 138–146 (2014).
Jansen, C. C. & Beebe, N. W. The dengue vector Aedes aegypti: what comes next. Microbes Infect. 12, 272–279 (2010).
Campbell, L. P. et al. Climate change influences on global distributions of dengue and chikungunya virus vectors. Phil. Trans. R. Soc. B 370, 20140135 (2015).
Kalayanarooj, S., Rothman, A. L. & Srikiatkhachorn, A. Case management of dengue: lessons learned. J. Infect. Dis. 215, S79–S88 (2017).
Weaver, S. C., Charlier, C., Vasilakis, N. & Lecuit, M. Zika, chikungunya, and other emerging vector-borne viral diseases. Annu. Rev. Med. 69, 395–408 (2018).
Leparc-Goffart, I., Nougairede, A., Cassadou, S., Prat, C. & de Lamballerie, X. Chikungunya in the Americas. Lancet 383, 514 (2014).
Pialoux, G., Gaüzère, B.-A., Jauréguiberry, S. & Strobel, M. Chikungunya, an epidemic arbovirosis. Lancet Infect. Dis. 7, 319–327 (2007).
Lessler, J. et al. Assessing the global threat from Zika virus. Science 353, aaf8160 (2016). A comprehensive review of the epidemiology of Zika, the public health threat posed by Zika infections and current uncertainties.
Cohen, J. Where has all the Zika gone? Science 357, 631–632 (2017).
Ferguson, N. M. et al. Countering Zika in Latin America. Science 353, 353–354 (2016).
Netto, E. M. et al. High Zika virus seroprevalence in Salvador, Northeastern Brazil limits the potential for further outbreaks. MBio 8, e01390-17 (2017).
Shearer, F. M. et al. Existing and potential infection risk zones of yellow fever worldwide: a modelling analysis. Lancet Glob. Health 6, e270–e278 (2018).
Ferguson, N. M. et al. Benefits and risks of the Sanofi–Pasteur dengue vaccine: modeling optimal deployment. Science 353, 1033–1036 (2016).
Flasche, S. et al. The long-term safety, public health impact, and cost-effectiveness of routine vaccination with a recombinant, live-attenuated dengue vaccine (Dengvaxia): a model comparison study. PLoS Med. 13, e1002181 (2016). This study presents the model comparison exercise that informed initial WHO recommendations on the use of the Sanofi dengue vaccine.
Olotu, A. et al. Seven-year efficacy of RTS,S/AS01 malaria vaccine among young African children. N. Engl. J. Med. 374, 2519–2529 (2016).
Penny, M. A. et al. Public health impact and cost-effectiveness of the RTS,S/AS01 malaria vaccine: a systematic comparison of predictions from four mathematical models. Lancet 387, 367–375 (2016). This study presents the model comparison exercise that informed WHO recommendations on the use of the RTS, S malaria vaccine.
RTS,S Clinical Trials Partnership. Efficacy and safety of RTS,S/AS01 malaria vaccine with or without a booster dose in infants and children in Africa: final results of a phase 3, individually randomised, controlled trial. Lancet 386, 31–45 (2015).
Hemingway, J. et al. Averting a malaria disaster: will insecticide resistance derail malaria control? Lancet 387, 1785–1788 (2016).
Achee, N. L. et al. A critical assessment of vector control for dengue prevention. PLoS Negl. Trop. Dis. 9, e0003655 (2015).
Bowman, L. R., Donegan, S. & McCall, P. J. Is dengue vector control deficient in effectiveness or evidence?: Systematic review and meta-analysis. PLoS Negl. Trop. Dis. 10, e0004551 (2016).
Heintze, C., Velasco Garrido, M. & Kroeger, A. What do community-based dengue control programmes achieve? A systematic review of published evaluations. Trans. R. Soc. Trop. Med. Hyg. 101, 317–325 (2007).
Wilson, A. L. et al. Evidence-based vector control? Improving the quality of vector control trials. Trends Parasitol. 31, 380–390 (2015). This paper outlines good practice for the design of field trials of vector control interventions.
Barrozo, R. B., Schilman, P. E., Minoli, S. A. & Lazzari, C. R. Daily rhythms in disease-vector insects. Biol. Rhythm Res. 35, 79–92 (2004).
Griffin, J. T. et al. Gradual acquisition of immunity to severe malaria with increasing exposure. Proc. R. Soc. B 282, 20142657 (2015).
Gupta, S., Trenholme, K., Anderson, R. M. & Day, K. P. Antigenic diversity and the transmission dynamics of Plasmodium falciparum. Science 263, 961–963 (1994).
Clapham, H. E., Cummings, D. A. T. & Johansson, M. A. Immune status alters the probability of apparent illness due to dengue virus infection: evidence from a pooled analysis across multiple cohort and cluster studies. PLoS Negl. Trop. Dis. 11, e0005926 (2017).
Guzman, M. G., Alvarez, M. & Halstead, S. B. Secondary infection as a risk factor for dengue hemorrhagic fever/dengue shock syndrome: an historical perspective and role of antibody-dependent enhancement of infection. Arch. Virol. 158, 1445–1459 (2013).
Katzelnick, L. C. et al. Antibody-dependent enhancement of severe dengue disease in humans. Science 358, 929–932 (2017).
Salje, H. et al. Reconstruction of antibody dynamics and infection histories to evaluate dengue risk. Nature 557, 719–723 (2018).
Gibbons, R. V. et al. Analysis of repeat hospital admissions for dengue to estimate the frequency of third or fourth dengue infections resulting in admissions and dengue hemorrhagic fever, and serotype sequences. Am. J. Trop. Med. Hyg. 77, 910–913 (2007).
Thai, K. T. D. et al. Age-specificity of clinical dengue during primary and secondary infections. PLoS Negl. Trop. Dis. 5, e1180 (2011).
Griffin, J. T. et al. Potential for reduction of burden and local elimination of malaria by reducing Plasmodium falciparum malaria transmission: a mathematical modelling study. Lancet Infect. Dis. 16, 465–472 (2016).
Griffin, J. T. et al. Reducing Plasmodium falciparum malaria transmission in Africa: a model-based evaluation of intervention strategies. PLoS Med. 7, e1000324 (2010).
Walker, P. G. T., Griffin, J. T., Ferguson, N. M. & Ghani, A. C. Estimating the most efficient allocation of interventions to achieve reductions in Plasmodium falciparum malaria burden and transmission in Africa: a modelling study. Lancet Glob. Health 4, e474–e484 (2016). This study uses mathematical modelling to assess optimal allocation of different malaria interventions in different transmission settings across Africa.
Dorigatti, I., McCormack, C., Nedjati-Gilani, G. & Ferguson, N. M. Using Wolbachia for dengue control: insights from modelling. Trends Parasitol. 34, 102–113 (2018).
Bhatt, S. et al. The global distribution and burden of dengue. Nature 496, 504–507 (2013).
Salje, H. et al. Dengue diversity across spatial and temporal scales: local structure and the effect of host population size. Science 355, 1302–1306 (2017). This study uses genetic and epidemiological data to quantitatively characterize the spatial range and local population drivers of dengue virus transmission.
Reiner, R. C. Jr et al. Time-varying, serotype-specific force of infection of dengue virus. Proc. Natl Acad. Sci. USA 111, E2694–E2702 (2014).
Andersson, N. et al. Evidence based community mobilization for dengue prevention in Nicaragua and Mexico (Camino Verde, the Green Way): cluster randomized controlled trial. Br. Med. J. 351, h3267 (2015).
Cauchemez, S. et al. Association between Zika virus and microcephaly in French Polynesia, 2013–15: a retrospective study. Lancet 387, 2125–2132 (2016).
Johansson, M. A., Mier-y-Teran-Romero, L., Reefhuis, J., Gilboa, S. M. & Hills, S. L. Zika and the risk of microcephaly. N. Engl. J. Med. 375, 1–4 (2016).
Reiner, R. C. Jr et al. Quantifying the epidemiological impact of vector control on dengue. PLoS Negl. Trop. Dis. 10, e0004588 (2016).
Ooi, E.-E., Goh, K.-T. & Gubler, D. J. Dengue prevention and 35 years of vector control in Singapore. Emerg. Infect. Dis. 12, 887–893 (2006).
Fullman, N., Burstein, R., Lim, S. S., Medlin, C. & Gakidou, E. Nets, spray or both? The effectiveness of insecticide-treated nets and indoor residual spraying in reducing malaria morbidity and child mortality in sub-Saharan Africa. Malar. J. 12, 62 (2013).
Lengeler, C. Insecticide-treated bed nets and curtains for preventing malaria. Cochrane Database Syst. Rev. 2, CD000363 (2004).
Pluess, B., Tanser, F. C., Lengeler, C. & Sharp, B. L. Indoor residual spraying for preventing malaria. Cochrane Database Syst. Rev. 4, CD006657 (2010).
West, P. A. et al. Indoor residual spraying in combination with insecticide-treated nets compared to insecticide-treated nets alone for protection against malaria: a cluster randomised trial in Tanzania. PLoS Med. 11, e1001630 (2014).
Powell, J. R. & Tabachnick, W. J. History of domestication and spread of Aedes aegypti—a review. Mem. Inst. Oswaldo Cruz 108, 11–17 (2013).
De Silva, P. M. & Marshall, J. M. Factors contributing to urban malaria transmission in sub-Saharan Africa: a systematic review. J. Trop. Med. 2012, 819563 (2012).
WHO. Integrated vector management. http://www.who.int/neglected_diseases/vector_ecology/ivm_concept/en/. Accessed 17 February 2018.
Department of Control of Neglected Tropical Diseases. How to design vector control efficacy trials. Guidance on phase III vector control field trial design. Report No. WHO/HTM/NTD/VEM/2017.03 http://www.who.int/neglected_diseases/vector_ecology/resources/WHO_HTM_NTD_VEM_2017.03/en/ (World Health Organization, 2017).
Wolbers, M., Kleinschmidt, I., Simmons, C. P. & Donnelly, C. A. Considerations in the design of clinical trials to test novel entomological approaches to dengue control. PLoS Negl. Trop. Dis. 6, e1937 (2012).
Snow, R. W., Guerra, C. A., Noor, A. M., Myint, H. Y. & Hay, S. I. The global distribution of clinical episodes of Plasmodium falciparum malaria. Nature 434, 214–217 (2005).
White, M. T. et al. A combined analysis of immunogenicity, antibody kinetics and vaccine efficacy from phase 2 trials of the RTS,S malaria vaccine. BMC Med. 12, 117 (2014).
White, M. T. et al. Immunogenicity of the RTS,S/AS01 malaria vaccine and implications for duration of vaccine efficacy: secondary analysis of data from a phase 3 randomised controlled trial. Lancet Infect. Dis. 15, 1450–1458 (2015). This study analyses the data from the phase III trials of the RTS,S malaria vaccine to derive a mechanistic model of vaccine action and propose a predictive correlate of protection.
Blackman, M. A., Kim, I.-J., Lin, J.-S. & Thomas, S. J. Challenges of vaccine development for Zika virus. Viral Immunol. 31, 117–123 (2018).
Asher, J. et al. Preliminary results of models to predict areas in the Americas with increased likelihood of Zika virus transmission in 2017. Preprint at https://www.biorxiv.org/content/early/2017/09/18/187591 (2017).
WHO. Efficacy trials of ZIKV vaccines: endpoints, trial design, site selection. http://www.who.int/blueprint/what/norms-standards/ZIKV_final_report_public_version.pdf (2017).
Eisele, T. P. et al. Short-term impact of mass drug administration with dihydroartemisinin plus piperaquine on malaria in Southern Province Zambia: a cluster-randomized controlled trial. J. Infect. Dis. 214, 1831–1839 (2016).
Brady, O. J. et al. Role of mass drug administration in elimination of Plasmodium falciparum malaria: a consensus modelling study. Lancet Glob. Health 5, e680–e687 (2017).
Bigira, V. et al. Protective efficacy and safety of three antimalarial regimens for the prevention of malaria in young Ugandan children: a randomized controlled trial. PLoS Med. 11, e1001689 (2014).
Capeding, M. R. et al. Clinical efficacy and safety of a novel tetravalent dengue vaccine in healthy children in Asia: a phase 3, randomised, observer-masked, placebo-controlled trial. Lancet 384, 1358–1365 (2014).
Villar, L. et al. Efficacy of a tetravalent dengue vaccine in children in Latin America. N. Engl. J. Med. 372, 113–123 (2015).
Winskill, P., Walker, P. G., Griffin, J. T. & Ghani, A. C. Modelling the cost-effectiveness of introducing the RTS,S malaria vaccine relative to scaling up other malaria interventions in sub-Saharan Africa. BMJ Glob. Health 2, e000090 (2017).
World Health Organization. Malaria vaccine: WHO position paper—January 2016. Wkly Epidemiol. Rec. 91, 33–51 (2016).
World Health Organization. Dengue vaccine: WHO position paper—July 2016. Wkly Epidemiol. Rec. 91, 349–364 (2016).
WHO. Updated questions and answers related to information presented in the Sanofi Pasteur press release on 30 November 2017 with regards to the dengue vaccine Dengvaxia. http://www.who.int/immunization/diseases/dengue/q_and_a_dengue_vaccine_dengvaxia/en/ (2017).
Screaton, G. & Mongkolsapaya, J. Which dengue vaccine approach is the most promising, and should we be concerned about enhanced disease after vaccination?: The challenges of a dengue vaccine. Cold Spring Harb. Perspect. Biol. 10, a029520 (2018).
WHO. Tables of malaria vaccine projects globally. http://www.who.int/immunization/research/development/Rainbow_tables/en/ (2017).
Barba-Spaeth, G. et al. Structural basis of potent Zika–dengue virus antibody cross-neutralization. Nature 536, 48–53 (2016).
Fiorenzano, J. M., Koehler, P. G. & Xue, R.-D. Attractive toxic sugar bait (ATSB) for control of mosquitoes and its impact on non-target organisms: a review. Int. J. Environ. Res. Public Health 14, 398 (2017).
Qualls, W. A. et al. Indoor use of attractive toxic sugar bait (ATSB) to effectively control malaria vectors in Mali, West Africa. Malar. J. 14, 301 (2015).
Slater, H. C., Walker, P. G. T., Bousema, T., Okell, L. C. & Ghani, A. C. The potential impact of adding ivermectin to a mass treatment intervention to reduce malaria transmission: a modelling study. J. Infect. Dis. 210, 1972–1980 (2014).
Werren, J. H., Baldo, L. & Clark, M. E. Wolbachia: master manipulators of invertebrate biology. Nat. Rev. Microbiol. 6, 741–751 (2008).
Moreira, L. A. et al. A Wolbachia symbiont in Aedes aegypti limits infection with dengue, Chikungunya, and Plasmodium. Cell 139, 1268–1278 (2009).
Walker, T. et al. The wMel Wolbachia strain blocks dengue and invades caged Aedes aegypti populations. Nature 476, 450–453 (2011).
Ferguson, N. M. et al. Modeling the impact on virus transmission of Wolbachia-mediated blocking of dengue virus infection of Aedes aegypti. Sci. Transl. Med. 7, 279ra237 (2015). This study combines experiemental work and modelling to estimate the likely impact of replacing wild-type A. aegypti with Wolbachia-infected mosquitoes on dengue disease transmission.
Bian, G. et al. Wolbachia invades Anopheles stephensi populations and induces refractoriness to Plasmodium infection. Science 340, 748–751 (2013).
Adelman, Z. N. Genetic Control of Malaria and Dengue (Academic, Amsterdam, 2015).
Gabrieli, P., Smidler, A. & Catteruccia, F. Engineering the control of mosquito-borne infectious diseases. Genome Biol. 15, 535 (2014).
Adelman, Z. N. & Tu, Z. Control of mosquito-borne infectious diseases: sex and gene drive. Trends Parasitol. 32, 219–229 (2016).
Marshall, J. M. & Taylor, C. E. Malaria control with transgenic mosquitoes. PLoS Med. 6, e1000020 (2009).
Galizi, R. et al. A synthetic sex ratio distortion system for the control of the human malaria mosquito. Nat. Commun. 5, 3977 (2014).
Burt, A. Site-specific selfish genes as tools for the control and genetic engineering of natural populations. Proc. R. Soc. B 270, 921–928 (2003). This study was one of the first to provide a rigorous population genetic assessment of the potential of using homing endonuclease genes to drive genetic modification of vector populations for disease control purposes.
Deredec, A., Godfray, H. C. J. & Burt, A. Requirements for effective malaria control with homing endonuclease genes. Proc. Natl Acad. Sci. USA 108, E874–E880 (2011).
Li, M. et al. Germline Cas9 expression yields highly efficient genome engineering in a major worldwide disease vector, Aedes aegypti. Proc. Natl Acad. Sci. USA 114, E10540–E10549 (2017).
Gantz, V. M. et al. Highly efficient Cas9-mediated gene drive for population modification of the malaria vector mosquito Anopheles stephensi. Proc. Natl Acad. Sci. USA 112, E6736–E6743 (2015).
Wang, S. & Jacobs-Lorena, M. Genetic approaches to interfere with malaria transmission by vector mosquitoes. Trends Biotechnol. 31, 185–193 (2013).
Severson, D. W. & Behura, S. K. genome investigations of vector competence in Aedes aegypti to inform novel arbovirus disease control approaches. Insects 7, 58 (2016).
Wesolowski, A. et al. Quantifying the impact of human mobility on malaria. Science 338, 267–270 (2012).
Acknowledgements
I thank the Medical Research Council, the National Institute of Health Research Health Protection Research Unit programme, the National Institute of General Medical Sciences ‘MIDAS’ programme and the Bill and Melinda Gates Foundation for research funding. Among many others, A. Ghani, A. Burt and S. O’Neill have informed my understanding of this topic during many illuminating discussions.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The author declares no competing interests.
Additional information
Publisher’s note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Ferguson, N.M. Challenges and opportunities in controlling mosquito-borne infections. Nature 559, 490–497 (2018). https://doi.org/10.1038/s41586-018-0318-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41586-018-0318-5
This article is cited by
-
Modelling the dynamic basic reproduction number of dengue based on MOI of Aedes albopictus derived from a multi-site field investigation in Guangzhou, a subtropical region
Parasites & Vectors (2024)
-
A mosquito salivary protein-driven influx of myeloid cells facilitates flavivirus transmission
The EMBO Journal (2024)
-
Mosquito control by abatement programmes in the United States: perspectives and lessons for countries in sub-Saharan Africa
Malaria Journal (2024)
-
Effects of climatic and environmental factors on mosquito population inferred from West Nile virus surveillance in Greece
Scientific Reports (2023)
-
MosChito rafts as effective and eco-friendly tool for the delivery of a Bacillus thuringiensis-based insecticide to Aedes albopictus larvae
Scientific Reports (2023)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
