
Abstract
Trachoma is a neglected tropical disease caused by infection with conjunctival strains of Chlamydia trachomatis. It can result in blindness. Pathophysiologically, trachoma is a disease complex composed of two linked chronic processes: a recurrent, generally subclinical infectious–inflammatory disease that mostly affects children, and a non-communicable, cicatricial and, owing to trichiasis, eventually blinding disease that supervenes in some individuals later in life. At least 150 infection episodes over an individual’s lifetime are needed to precipitate trichiasis; thus, opportunity exists for a just global health system to intervene to prevent trachomatous blindness. Trachoma is found at highest prevalence in the poorest communities of low-income countries, particularly in sub-Saharan Africa; in June 2021, 1.8 million people worldwide were going blind from the disease. Blindness attributable to trachoma can appear in communities many years after conjunctival C. trachomatis transmission has waned or ceased; therefore, the two linked disease processes require distinct clinical and public health responses. Surgery is offered to individuals with trichiasis and antibiotic mass drug administration and interventions to stimulate facial cleanliness and environmental improvement are designed to reduce infection prevalence and transmission. Together, these interventions comprise the SAFE strategy, which is achieving considerable success. Although much work remains, a continuing public health problem from trachoma in the year 2030 will be difficult for the world to excuse.
Similar content being viewed by others



Introduction
Trachoma is one of 20 diseases and disease groups designated as neglected tropical diseases by the World Health Organization (WHO)1. It is the most common infectious cause of blindness2. The disease can be conceptualized as progressing in two phases. In the first phase, repeated infection3,4 with conjunctival strains5 of the bacterium Chlamydia trachomatis (Ct) results in a chronic keratoconjunctivitis (inflammation of the cornea and conjunctiva), including an inflammation of the conjunctiva known as active trachoma. Rounds of severe conjunctival inflammation lead to scarring of the eyelid6,7, which is the start of the second disease phase. This scarring can cause inward rotation of the eyelashes so that they come into contact with the eyeball, a condition known as trichiasis. Trichiasis may be accompanied by a distortion of the eyelid known as entropion8, in which part or all of the eyelid margin is rolled inward. Scratching of the cornea by in-turned eyelashes predisposes to corneal opacity, vision impairment and blindness. The presence of any of these Ct-induced pathological processes or clinical signs is trachoma. However, to fully grasp the nature of this disease, it is imperative to also consider the devastating effects of trichiasis and vision impairment on affected individuals, their families and their communities9. In economic terms alone, these effects combine to reduce global productivity by billions of dollars each year10.
Trachoma is a disease of poverty — it affects the poorest of the poor11. In Europe and most of North America, trachoma disappeared decades ago as living standards improved and without the implementation of specific interventions12. Similar trends have been seen in some low-income and middle-income countries with previously hyperendemic disease13,14,15. In addition, during the past few decades, deliberate interventions to control trachoma have been associated with dramatic declines in its global burden16,17. However, prevalence has remained high in some populations despite prolonged intensive intervention with a comprehensive, four-component strategy recommended by WHO18.
In this Primer, we provide an overview of the epidemiology, pathophysiology, clinical features and diagnosis of trachoma as well as of the management, control and elimination of disease, at both the individual and population level. We also propose key areas for future research.
Epidemiology
Global trachoma prevalence data are published annually by WHO17 and summarized on the WHO Global Health Observatory. Data at a finer scale are available on the Trachoma Atlas. As of March 2022, 44 countries were known to require interventions against trachoma, of which 26 were in the WHO African Region.
Associations
Poverty
At any spatial scale at which observations are made, trachoma is found in the poorest people. Risk of active trachoma is higher in households with crowded sleeping arrangements11,19,20,21; sharing a bedroom with someone else who has active trachoma doubles an individual’s risk22. In trachoma-endemic communities, individuals with trachomatous trichiasis (TT) are likely to be poorer than age-matched and gender-matched peers without TT and are less likely than those peers to participate in economically productive activities even after controlling for visual impairment11. In trachoma-endemic countries, the disease affects the population groups that are poorest, most marginalized and most remote from services (particularly water and sanitation)23. At the regional and global level, concentration of trachoma in the poorest countries is evident17,24.
Poverty is both a cause and consequence of blindness25. Trachoma can trap affected individuals, families and communities in successive generations of despair.
Age
In trachoma-endemic populations, individuals are often first exposed to conjunctival Ct during the first months of life26. Ct infection and active trachoma occur most commonly during childhood; in infected individuals, Ct loads are higher at younger ages26,27,28,29,30,31. In hyperendemic areas, the frequencies with which infection and active trachoma are observed decrease with age after a peak in those aged 2–5 years. TT, corneal opacity and visual impairment are unusual before adulthood and observed frequencies increase with age27,32.
Gender
In childhood, boys and girls tend to be equally affected by active trachoma33,34. For TT, in pooled data, women have 1.8 times higher odds of being affected than men35, although this odds ratio can approach 4 in some settings33,36. The excess risk is generally attributed to women being exposed to conjunctival Ct more frequently than men as they get older because of women’s disproportionate contribution to childcare duties in most societies37. More direct biological effects of oestrogen, oestrogen receptor abundance or sex-linked differences in the immune response to Ct38 have not been ruled out.
Mechanisms/pathophysiology
Chlamydia trachomatis
Ct is a gram-negative bacterium that infects humans at the epithelial layer of mucosal surfaces. Different Ct serovars, originally distinguished using micro-immunofluorescence39, have a characteristic tissue tropism and are associated with different disease complexes: A, B, Ba and C with trachoma, D through K with urogenital chlamydia, and L1, L2 and L3 with lymphogranuloma venereum (Box 1).
Ct has a unique biphasic developmental cycle40. It moves between host cells as the infectious form, called the elementary body (diameter ~0.30 μm). Using mostly receptor-mediated endocytosis, the elementary body gains entry to a human epithelial cell within a vacuole formed of host cell membrane and chlamydial proteins, which then develops into a peri-nuclear inclusion41. Inside the inclusion, it reorganizes into its more metabolically active, replicating, non-infectious form, the reticulate body (diameter ~1.2 μm). After ~72 h, the reticulate body transforms into 100–1,000 elementary bodies that are released via host cell lysis. In the intracellular environment, Ct evades detection and dampens the host immune response via several mechanisms40.
The elementary body has a rigid cell wall, which facilitates survival under unfavourable conditions. The major outer membrane protein is the most abundant cell wall surface protein, comprising ~60% of cell wall mass. It is involved in host cell surface adhesion and is encoded by a single-copy chromosomal gene, OmpA42. Variation in this protein characterizes the 19 different Ct serovars. Whole-genome sequencing revealed that the preference of different serovars for particular anatomical niches is not absolute. Extensive recombination in the OmpA region has resulted in exchange of genetic material both within and between conjunctival, urogenital and lymphogranuloma venereum strains43. Urogenital strains are generally able to synthesize their own tryptophan, whereas conjunctival strains typically have inactivating mutations in the gene encoding tryptophan synthase44. One possible explanation is that ocular serovars are able to access a source of tryptophan (or one of its biosynthetic precursors) within the conjunctival sac or infected cells, and that that source is unavailable to pathogens in the urogenital tract44. Of note, tryptophan itself is not found in human tears45. The mechanism by which conjunctival Ct survives in this milieu and whether its peculiar biochemistry could be exploited against human disease is unknown.
Other Ct proteins in addition to the major outer membrane protein are produced in a complex sequence at different stages in the developmental cycle46; these include heat shock proteins that protect Ct in stress conditions. These proteins, such as cHsp60, are implicated in disease pathogenesis and are recognized by pathogen recognition receptors of the innate immune system, including Toll-like receptors47.
Transmission of Ct
Transmission of conjunctival Ct infection has been the subject of considerable scrutiny, yet methods to directly investigate transmission routes in trachoma-endemic communities were not applied until 2018. Important epidemiological evidence used to generate biologically plausible hypotheses on transmission includes the focal nature of infection and disease, with spatial clustering of cases identified at bedroom, household, compound, neighbourhood and community levels31,48,49,50,51,52,53,54,55,56; the association of active trachoma with visible eye and nose discharge on children’s faces57,58,59; and the association of active trachoma with observed fly-eye contact53,60,61,62. All of the above tend to be observed in populations that are relatively overcrowded57,62,63 and have poor access to water and sanitation59,63,64,65,66. Infected eye discharge or cultured Ct can induce active trachoma when directly inoculated into an eye19,67, suggesting that simple mechanical transfer of infectious material from an infected to an uninfected eye may be all that is necessary to create a transmission event. Because tears drain into the nose and Ct can be identified in the noses of children with active trachoma68,69, nasal discharge may also be important in transmission of infection. Together, these observations implicate three principal routes of transmission: direct person-to-person transfer of infected secretions on human fingers; spread via fomites such as shared bedding or towels; and carriage on eye-seeking flies, particularly female Musca sorbens, which preferentially obtain protein from human exudates for egg production70. It is not yet known with certainty whether Ct infects and replicates within vector fly species but laboratory-based work on flies from the same genus71 shows that viable Ct can be retrieved from flies for up to 48 h after feeding. Fingers, fomites and flies are sometimes referred to as the ‘three Fs’ of trachoma transmission.
Evidence now substantiates these proposed routes. Ct DNA can be detected on flies caught leaving the faces of children in trachoma-endemic communities55,70,72,73. In Ethiopian households in which no residents had current conjunctival Ct infection and which were located close to other households in which one or more residents did have conjunctival Ct infection, some flies caught leaving the faces of children were positive for Ct DNA. This implicates flies as potential carriers of conjunctival Ct between households as well as within them55. In a prospective trial, fly control with insecticide space spraying, which involves the creation of a liquid fog throughout community outdoor spaces, although not seen to be a sustainable intervention at scale, reduced the prevalence of active trachoma74, confirming the importance of flies as vectors.
A study published in 2020 demonstrated the presence of Ct DNA at other extra-ocular sites: on the skin of human faces and hands, clothing, a sleeping surface, and a washing jug in households in which one or more residents had conjunctival Ct infection55. In households in which all residents had Ct-negative conjunctival swabs, none of these extra-ocular sites had detectable Ct DNA55. Experiments employing viability PCR, which uses propidium monoazide pre-treatment to prevent amplification of DNA from non-viable bacteria, suggest that at least some Ct remains viable on plastic, cotton cloth and skin for >24 h (ref.75), providing additional support for the roles of fingers and fomites in transmission.
Conjunctival Ct infection and active trachoma
Epidemiological observations have informed mathematical models of trachoma, which suggest that >100 conjunctival Ct infections in an individual’s lifetime are required to generate clinically significant conjunctival scarring and that 150 infections are required to precipitate TT76. As most episodes of infection occur in childhood, children who go on to develop TT later in life are likely to be re-infected several times each month, with transfer of Ct back and forth from one child to another.
The limited longitudinal data available indicate that a primary infection episode in a child is characterized by a short ‘preclinical’ phase of a few days before the development of signs of inflammation77. In adult human volunteer experiments, clinical inflammation developed ~10 days after conjunctival Ct inoculation78. Established infections are characterized, particularly in younger preschool age children, by a generalized follicular and papillary conjunctivitis, particularly evident in the conjunctiva of the upper eyelid. At the tissue level, the generalized papillary inflammation involves a mixed inflammatory cell infiltrate, including lymphocytes, macrophages and neutrophils. Lymphoid follicles are formed mostly of B cell aggregations in the conjunctival stroma. After the development of clinical inflammation, infection remains detectable for a few days to many weeks77. The human immune response then controls the infection, clearing it or reducing it to undetectable levels. However, conjunctival inflammation persists, and may last for many weeks after infection becomes undetectable; in untreated children aged 4–15 years, infection may be cleared after 3–8 weeks, whereas clinical signs of inflammation continue for 6–18 weeks79. Resolution of infection is thought to depend on a cell-mediated immune response, effected through IFNγ80. Adults tend to have shorter episodes of infection and disease, although the relative frequency of exposure to reinfection in children and adults cannot be quantified77. This protection in older individuals is thought to be mediated through acquired T cell-dependent cell-mediated responses that either prevent or more rapidly resolve infection80.
The different time courses of conjunctival infection and active trachoma explain the partial mismatch observed between infection and disease at the individual level54,81,82,83. This disparity has important implications for trachoma programmes, as individually targeted antibiotic treatment decisions based on observable conjunctival inflammation of at least moderate intensity would miss many infected individuals with a mild clinical response. Antibiotic mass drug administration (MDA) is the most practical way of trying to treat all individuals infected with conjunctival Ct within large trachoma-endemic populations84.
Development of scarring sequelae
The association between increasing age and increasing prevalence of cicatricial sequelae of trachoma (conjunctival scarring, TT and corneal opacity) indicate that these signs are cumulative. Several longitudinal studies have investigated their natural history and pathophysiology85. To date, five studies have examined the rates and risk factors for progression from conjunctivae without scarring through active trachoma to the development of conjunctival scarring6,7,86,87,88. Their findings show a consistent and substantially increased risk of subsequent incident scarring associated with intense conjunctival papillary inflammation, particularly when observed at multiple time points6,7,86,88. Evidence linking subsequent scarring to the presence of a follicular conjunctivitis (without concomitant intense papillary inflammation) or to repeated or constant Ct infection is much less convincing. Only two published cohort studies of incident scarring have prospectively tested for Ct infection. Neither of these has identified a relationship between ongoing Ct infection and incident or progressive scarring after adjusting for clinical inflammation7,88.
Two large prospective studies conducted in Ethiopia and the United Republic of Tanzania have followed the progression of pre-existing conjunctival scarring in adults, including tests for the presence of Ct89. Both found strong evidence of a relationship between progression of scarring and the repeated observation of papillary inflammation of the conjunctiva. Conjunctival Ct infection was very rare in these cohorts, and the infections that were detected were not associated with progression. However, it is possible that study participants were infected occasionally for very short periods77, which multiple cross-sectional samples could easily miss.
Taken together, these studies point to a central role for chronic severe inflammation in scarring development (Fig. 1). Such severe responses are not found in all people exposed to conjunctival Ct, indicating that variations in the human immune response may be important co-determinants of scarring risk although it is not possible to quantify individual exposure to repeated reinfection. At the population level, a higher prevalence of inflammatory trachoma in children correlates with a higher prevalence of trichiasis in adults90. Available data also suggest that additional pro-inflammatory stimuli, such as other bacteria and ocular surface dryness81, contribute to the progression of scarring initiated by Ct-related inflammation91.

Pathogenesis of visual impairment in trachoma and the SAFE strategy interventions intended to prevent or slow those processes. The two linked chronic processes that are involved in pathogenesis are shown: a recurrent, generally subclinical infectious–inflammatory disease that mostly affects children; and a non-communicable, cicatricial, increasingly painful, eventually blinding disease that supervenes in some individuals later in life. (1) Resolution of Chlamydia trachomatis infection and restoration of the uninflamed conjunctiva is accompanied by (2) some residual conjunctival scarring; (3) repeated reinfection drives the chronic cicatricial process. (4) Conjunctival scarring reduces the volume and alters the composition of the tear fluid, which normally acts as a mechanical barrier (via continual flow) and contains molecules that are part of the innate immune system. Where trichiatic eyelashes abrade the cornea, breaching of the epithelium (the most superficial layer of the cornea) enables penetration of bacteria into the corneal stroma. (5) Antibiotics treat prevalent C. trachomatis infections (and some other prevalent bacterial infections), whereas facial cleanliness and environmental improvement are intended to reduce the incidence of new infections, that is, reduce transmission intensity. (6) No specific interventions have been trialled or deployed to try to reduce the likelihood of incident trichiasis in individuals who have conjunctival scarring. Of note, SAFE strategy components are intended to reduce the accumulation of conjunctival scarring in those who do not yet have it and in those who do. (7) Surgery reduces progressive corneal opacification and ocular surface irritation, which is crucial for symptom relief. Surgery has no effect to correct existing ocular surface dryness. (8) In many conditions that blind through corneal opacification, keratoplasty (corneal transplantation) is used to reduce or reverse visual impairment. In an individual with corneal opacity due to trachoma, changes in the tear film and corneal vascularization are predicted to reduce the likelihood of long-term graft survival. In addition, populations affected by trachoma tend to have very poor access to keratoplasty services.
Immunopathological basis of scarring trachoma
Trachoma offers an unusual opportunity to directly observe and investigate the pathophysiology of an inflammatory scarring disease process, with potential relevance to disease processes elsewhere. Multiple long-term natural history studies have been conducted, applying a range of techniques (histopathology, immunohistochemistry, in vivo confocal microscopy, human gene expression profiling or human genetics) and relating these to the clinical course80. In addition, non-human primate models have been developed as part of Ct vaccine development work, which have contributed substantially to our understanding of trachoma pathophysiology3,92,93,94.
Biopsy and in vivo confocal microscopy studies of children with active trachoma demonstrate that it is characterized by a mixed conjunctival inflammatory cell infiltrate, including macrophages, T cells, neutrophils and dendritic cells95,96. Organized lymphoid follicles are scattered throughout the conjunctival stroma, composed largely of B cells surrounded by a mantle of proliferating lymphocytes (Fig. 2).

Schematic of the histology of the normal conjunctiva, the conjunctiva in the presence of active trachoma and conjunctiva in the presence of trachomatous scarring. a | The normal conjunctiva has a non-keratinized, stratified epithelium of 3–5 cell layers, containing interspersed goblet cells that secrete mucin. The tear film covers the epithelium. The deeper lamina propria accommodates blood vessels, lymphoid cells and other connective tissue elements. b | When infected with Chlamydia trachomatis, inflammation is manifest through telangiectasia of capillaries and small venules, and a mixed inflammatory cell infiltrate. Collections of B cells, T cells and macrophages form lymphoid follicles in the lamina propria; B cells form the core and the bulk of their mass. When sufficiently large, lymphoid follicles distort the contour of the overlying epithelium (not shown) and can be seen in the everted tarsal conjunctivae. c | In the scarred conjunctiva, goblet cells are depleted. The tear film is reduced in volume and changed in composition. An increasingly disorganized scar is found in the lamina propria. Scars may also be found in the tarsal plate (not shown). ECM, extracellular matrix.
In biopsy specimens from adults with conjunctival scarring, extensive connective tissue disruption can occur with loss of the regular stromal architecture and replacement with disorganized collagen and other elements97. Compared with controls, scarred tissue also has marked increases in CD45+ inflammatory cells, whose abundance fluctuates with the intensity of clinical inflammation98. Specific staining indicates that natural killer cells are a prominent component of the cellular infiltrate in scarred conjunctivae, suggesting that innate responses may be relevant in this damaged tissue98. Staining of scarred conjunctivae against a panel of cytokines and scarring disease markers reveals prominent increases in epithelial expression of connective tissue growth factor (CTGF) and the antimicrobial peptide S100A7; in addition, expression levels of IL-1β are increased in the substantia propria99.
In vitro infection studies of epithelial cells have found a marked innate pro-inflammatory response, with the production of several cytokines: IL-6, IL-8, growth-regulated oncogene-α (GROα) and granulocyte–macrophage colony-stimulating factor (GM-CSF)100,101 (Fig. 3). This finding is consistent with data from in vivo investigations into conjunctival gene expression profiles using swabs taken from the conjunctival surface102,103,104,105. The initial innate response to Ct is likely to be driven directly by infected epithelial cells, recognizing the presence of the organism through their pattern-recognition receptors, leading to a chronic inflammatory response. This suggestion is sometimes referred to as the cellular paradigm for the pathogenesis of Ct-driven scarring disease106. The alternative hypothesis, that is, the immunological paradigm, suggests that inflammation and tissue damage are driven through a cell-mediated immune or delayed-type hypersensitive response to chlamydial antigens such as cHsp60. Although well established in animal models, direct evidence from human studies corroborating this is limited80,94,106.

Immune responses triggered by Chlamydia trachomatis (Ct) infection; the infection can resolve or progress to eyelid scarring. Shown are the cytokines, human cellular enzymes, growth factors and other proteins involved in the regulation of the extracellular matrix whose expression is known to be upregulated or downregulated in the presence of replicating Ct, during infection resolution or in the ongoing pro-inflammatory state leading to progressive deposition of conjunctival scar. 23A RC, IL-23A-responsive cells; APC, antigen-presenting cell; CTGF, connective tissue growth factor; DEFB4A, defensin; GM-CSF, granulocyte–macrophage colony-stimulating factor; GROα, growth-regulated oncogene-α; IDO1, indoleamine-2,3-dioxygenase; MMP, matrix metalloproteinase; NK, natural killer; PMN, polymorphonuclear leukocyte; TH, T helper.
Resolution of Ct infection is thought to be dependent on IFNγ from a CD4+ T helper 1 (TH1) cell-mediated immune response. Gene expression studies in children in trachoma-endemic populations show a marked increase in conjunctival expression of IFNγ and TH1 cell-related factors (IL-12B and indoleamine-2,3-dioxygenase (IDO1)) and in natural killer cell pathways (characterized by NCR1, CD56 and CD247)102,103,104. In children with active trachoma but no detectable Ct, levels of IFNγ are not particularly elevated, suggesting that this response is rapidly regulated following the resolution of infection. Infection and active trachoma are also both associated with profiles that are consistent with a prominent TH17 response, with increased expression of IL-17, IL-21 and IL-22 (ref.104). Some data indicate that TH17–IL-17 responses might contribute to a worsening of the inflammatory/scarring response in animal models107.
Intense conjunctival inflammation is the key clinical manifestation linked with the development of scarring. In cross-sectional studies, intense inflammation is associated with increased expression of a range of pro-inflammatory factors such as S100A7, defensin (DEFB4A), IL-1β, IL-17A, CCL18 and neutrophil chemotactic factor CXCL5 (ref.104). These often seem to persist after Ct infection has resolved. Interestingly, several markers (S100A7, IL-1β, IL-17A and CXCL5) are also consistently elevated in adults with established conjunctival scarring and visible inflammation89.
In the context of this chronic inflammatory milieu, with the recruitment and activation of a diverse population of leukocytes, the conjunctival tissue is repeatedly damaged and scar tissue is formed during healing. Matrix metalloproteinases (MMPs) are a large and diverse family of proteases that are central to the regulation of connective tissue in health and disease. Studies in trachoma-endemic populations have found increased expression of MMP7, MMP9 and MMP12 in children with intense conjunctival inflammation and adults who have established scarring with inflammation89,102,104,108. In a cohort study of Tanzanian children assessed every 3 months for 4 years, progressive scarring was strongly associated with increased proportions of follow-up points at which clinical inflammation was seen88 as well as with increased expression of pro-inflammatory chemokines (CXCL5, CCL20, CXCL13 and CCL18), cytokines (IL-23A, IL-19 and IL-1B), MMP12, and S100A7 and reduced expression of SPARCL1 (ref.105).
Increased expression of several fibrogenic growth factors, including CTGF, FGF, TGFβ1 and PDGF, has also been associated with clinical inflammation in active trachoma and scarring89,104,108. These factors have a pro-fibrotic effect, probably largely mediated through increased deposition of connective tissue elements by stromal fibroblasts. Interestingly, cultured conjunctival fibroblasts from individuals with trachomatous scarring have a markedly contractile pro-fibrotic phenotype compared with control fibroblasts, suggesting some (as-yet uncharacterized) permanent change in their behaviour109.
Diagnosis, screening and prevention
Diagnosis
Trachoma is diagnosed through clinical examination. This requires a trained examiner, a calm examinee, magnification (generally ×2.5 binocular magnifying loupes), and a means for the examiner to prevent iatrogenic transmission of infection from one examinee to the next (alcohol-based hand gel, disposable examination gloves, or soap and water). Diagnosis is often (but not always) done in the field. Illumination is also important; a torch is optimal when looking for TT, whereas bright sunlight is generally adequate for examining the conjunctiva.
Most individuals with active trachoma have minimal or no symptoms. Some report eye irritation or a small amount of discharge. Individuals with TT often report a history of eye pain, blepharospasm (involuntary closure of both eyelids), light intolerance or reduced vision110. Many epilate their in-turned eyelashes using home-made forceps, clam shells or tree resin111. Poor vision may be reported even in the absence of corneal opacity. Quality of life may be severely impaired9,112,113.
A comprehensive trachoma examination routine is ideal but, in some contexts (in particular, routine surveys conducted by public health programmes to estimate prevalence), not all of its elements are required. The examination should be guided by its purpose and context.
The comprehensive examination comprises several steps. Visual acuity is measured (for each eye separately) where possible. To reduce the risk of transposing findings in the record, routinely examining the right eye, then the left eye, is recommended. Upper and lower eyelids are inspected for entropion, trichiasis and evidence of recent epilation; the latter includes broken or re-growing eyelashes or empty eyelash follicles. The cicatricial complications of trachoma characteristically affect the upper eyelid; in ~10% of patients, they also affect the lower eyelid but rarely in the absence of upper eyelid disease114. The cornea and limbus (border between cornea and sclera) are inspected for opacities, upper pole pannus (ingrowth of fibrovascular tissue from the limbus into the cornea) and Herbert pits (rounded depressions at the limbus resulting from regression of lymphoid follicles). If fluorescein and a slit lamp are available, superficial punctate keratitis might be detectable in some individuals with active trachoma. The upper eyelid is everted and the tarsal conjunctiva examined for central follicles, inflammatory thickening due to a papillary response, and scarring110,115. If follicles are present in the central part of the upper tarsal conjunctiva, only those with a diameter ≥0.5 mm should be regarded as being of pathological significance; follicle size guides116 fixed to the examiner’s thumbnails can assist in accurately assessing follicle diameter. Particularly when examining children, having an assistant to reassure and support the examinee can be invaluable117.
Other causes of conjunctival inflammation, conjunctival scarring, trichiasis, entropion and corneal opacity can have clinical signs that resemble those produced by trachoma. For example, inclusion conjunctivitis looks like active trachoma but is a self-limited inflammatory condition caused by infection of the conjunctiva with urogenital Ct118. Its prevalence has not been determined for any trachoma-endemic population but could be high in places where urogenital Ct is very common and access to water and sanitation is very poor. Non-chlamydial bacterial or viral infection may also drive follicular inflammation of the conjuctiva81,119.
The interpretation of clinical signs and their classification as being attributable (or not attributable) to trachoma can be influenced by a range of contextual impressions. For trachoma, these include the relative poverty of the patient and family, the examiner’s impression of the patient’s personal and family hygiene, and the trachoma endemicity of the patient’s community. However, community-level endemicity status is often unknown or not known with certainty. The examiner’s view on whether trachoma is endemic in a community influences the clinical interpretation of the patient, which can then (potentially inappropriately) confirm, in a circular fashion, the examiner’s classification of the community120. This possible confirmation bias is important in both the diagnosis of active trachoma and in differentiating upper eyelid trichiasis that is trachomatous from that caused by other pathological processes.
To help maximize the objectivity of assessment, particularly for estimates of trachoma prevalence at the population level, WHO developed trachoma grading systems that have subsequently evolved over decades110. Two systems are in current use. The modified WHO grading system (or FPC system, for follicles (F), papillary hypertrophy (P), cicatriciae (C)) is a specialist scale that was last updated in 1981 (ref.121) and is used principally in research studies. The simplified WHO grading system, intended for non-specialist personnel, was first published in 1987 (ref.122) and updated in 2020 (ref.115) (Table 1). It is in widespread use for screening and population-level assessment. The five signs are signs, not stages, and more than one can be simultaneously present in an eye. In the simplified grading system, the presence of trachomatous inflammation — follicular (TF) and/or trachomatous inflammation — intense (TI) in either eye constitutes active trachoma (Fig. 4).

The World Health Organization (WHO) simplified trachoma grading system defines five signs that are indicative of trachoma. The shaded area indicates the area of the conjunctiva to be examined for follicles. Follicles found outside this area may be normal122. Trachomatous inflammation — follicular and trachomatous inflammation — intense are signs of active trachoma122. Adapted from ref.115, CC BY 4.0 (https://creativecommons.org/licenses/by/4.0/).
The simplified system includes acknowledged imperfections115. For example, not all epilation is undertaken for trichiasis123; when epilated eyelashes have not fully regrown, it is hard to determine whether they were touching the eyeball before removal; and not all upper eyelid trichiasis is due to trachoma124.
Since 2012, standardization of grader training, grader certification and fieldwork procedures116,125,126,127,128 have further contributed to comparability and confidence in trachoma prevalence data generated by national programmes. However, when assessing an individual patient, rigid adherence to grading systems and standard operating procedures may not be appropriate. This represents a fundamental difference between the diagnostic approaches needed for clinical (Box 2) and epidemiological (Box 3) purposes.
Screening
In June 2021, 136 million people worldwide lived in areas in which active trachoma was thought to represent a public health problem17. Individually screening large populations for active trachoma is problematic because examining millions of people requires many examiners, and examiners without adequate training provide assessments with predictive values that are too low to be epidemiologically or programmatically useful129. Even physicians working in endemic areas may produce inaccurate screening assessments if they are not well trained130,131. Of note, the frequency of asymptomatic Ct infection and ease of reinfection after treatment mean that characterization and management of the population as a whole are crucial for controlling active trachoma; individual screening for the purposes of individual-level management would be unhelpful for achieving public health targets132.
For TT, active case-finding, including through mass population screening, is a recognized strategy for linking individuals who have TT with surgical services, thereby achieving agreed public health targets133. Various screening approaches are used, including centralized village-level screening conducted by eye workers and door-to-door screening by TT case finders. The limited data available suggest that the sensitivity and specificity of TT case finders are highly variable134,135,136. Properly training134 and equipping137 case finders is likely to be important.
Population-level assessment
A key concept in trachoma epidemiology is ‘elimination as a public health problem’, which is defined only for countries as a whole. It has three criteria: first, a prevalence of TT ‘unknown to the health system’ (that is, excluding individuals with post-surgical TT, individuals with TT who have refused surgery for it, and individuals with TT who have a surgical date set in the future) of <0.2% in those aged 15 years or more, in each formerly endemic district; second, a prevalence of TF of <5% in those aged 1–9 years, in each formerly endemic district; and, third, written evidence that the health system can identify and manage incident TT cases138.
Although validation of elimination as a public health problem can only be undertaken for a country as a whole, district-level data are needed to substantiate the claim that the first two criteria have been satisfied. Here, the term ‘district’ means the normal administrative unit for health-care management, generally a population unit of 100,000–250,000 people138. To avoid confusion with local administrative units designated as districts that may have populations outside the 100,000–250,000 range, trachoma programmes often use the term ‘evaluation units’ instead. WHO has published recommendations on estimating the prevalence of TT and TF at the level of evaluation units32,139. Although rigorous surveys undertaken according to those recommendations were determined to cost a median of US$8,298 (in 2017) per evaluation unit140, the alternative approaches of simply continuing interventions without checking that they continue to be justified, or not eliminating trachoma at all, are likely to be considerably more expensive10,141.
Since 2012, the Global Trachoma Mapping Project (GTMP)142 and its successor, Tropical Data143 (Table 2), have together supported health ministries in 50 countries to conduct population-based trachoma prevalence surveys consistent with WHO recommendations, generating globally comparable, epidemiologically robust data125. Data from all GTMP and Tropical Data surveys are owned by the relevant health ministries, with automated linkages made available to display evaluation unit-level prevalence categories on the open-access Trachoma Atlas and provide the most current information to decision-makers at all levels144.
Tests for Ct infection
Sensitive molecular approaches for pathogen detection, including qualitative and quantitative nucleic acid amplification-based tests, are available110,145. In trachoma, they are generally used for research purposes and not for programmatic decision-making. However, they might find more widespread use in the future as TF prevalence is not a perfect marker in this context, for several reasons146.
First, the sign TF is reasonably specific but not particularly sensitive for conjunctival Ct infection. In cross-sectional surveys, a relatively high proportion of individuals who are positive in nucleic acid amplification-based tests for conjunctival Ct do not have TF147. The prevalence of Ct tends to be higher in those with TI than in those with TF, and higher in those with TF than in those with less florid signs of trachoma54,83,104. Some of this discrepancy is due to variation between the natural history of infection and the natural history of disease in the individual3,110. In particular, Ct infection is present for days to weeks before TF or TI develops, and is cleared days to weeks before TF or TI resolves.
Second, the specificity of TF for conjunctival Ct infection varies between contexts. In trachoma-endemic populations, less than half of those with TF are PCR-positive for Ct147. Again, some of this discrepancy will be due to the natural history of infection versus that of disease in the indvidual110, including the effect of frequent reinfection in accelerating Ct clearance after each infection episode3. In addition, other processes also cause follicular conjunctivitis. Although in antibiotic MDA-naive communities in Africa, the prevalence of TF (or TI) tends to reflect the underlying prevalence of conjunctival Ct147, this relationship weakens after antibiotic MDA, presumably because reductions in the prevalence of Ct infection give other causes of follicular and intense conjunctival inflammation greater relative importance, and/or because of reduced sensitivity of tests for Ct where Ct bacterial loads are lower147. In some countries in the Western Pacific, even before antibiotic MDA, children have moderately high prevalences of TF despite the extremely low prevalence of or absent conjunctival Ct infection148,149,150,151,152.
Third, falling TF prevalences globally make the appropriate training of graders both more difficult and more important. High-quality photographs and centralized photograph grading153,154 might help but would not solve the problem of the mismatch between the natural histories of disease and infection.
An appropriately designed155 diagnostic test for current conjunctival Ct infection, deployed to help estimate infection at the evaluation unit level, could avoid misclassification from all three of these issues. Efforts have been made to develop rapid point-of-care diagnostics for the detection of current conjunctival Ct infection156,157,158. However, the principal programmatic use case is to determine whether or not interventions are indicated at the population level; therefore, high-quality tests for infection do not need to be performed next to the individuals recruited to participate in a survey. Alternatively, although open to misinterpretation in the assessment of a single individual, anti-Ct antibody data, based in particular on the presence of antibodies to the Ct antigen Pgp3, can be used to generate age–seroprevalence curves and seroconversion rates that are likely to be informative at the population level. This holds considerable promise for programmes159.
Prevention
Ct vaccine research is an important topic for basic and translational research160. From 2016 to 2017, a phase I, first-in-human, randomized, placebo-controlled trial was undertaken of recombinant Ct protein CTH522, adjuvanted with either CAF01 liposomes or aluminium hydroxide, as a potential vaccine against urogenital Ct infection. Both preparations seemed to be safe and immunogenic, with CTH522:CAF01 showing particular promise161. Currently, however, no vaccine is commercially available that protects against conjunctival or urogenital Ct infection. Therefore, preventing blindness from trachoma relies on interventions intended to limit Ct transmission, treat Ct infection and re-shape eyelids with TT so that eyelashes no longer touch the eyeball. These interventions are designed to achieve primary, secondary and tertiary prevention of trachomatous visual impairment.
Management
Interventions against trachoma are grouped together as the SAFE strategy: surgery (S) for TT, antibiotics (A) to clear infection, and facial (F) cleanliness and environmental (E) improvement to reduce transmission162. The components of the SAFE strategy are delivered at different scales: surgery is offered to individuals, while antibiotics, facial cleanliness and environmental improvement are generally offered to whole evaluation units of 100,000–250,000 people. However, ‘surgery’ conceptualized as a public health-level intervention entails measures, sometimes including painstaking house-to-house case searches, to reduce the evaluation unit-level prevalence of TT to below the threshold for elimination as a public health problem. Equally, it is critical that, while delivering the A, F and E components, the principles of non-maleficence and autonomy for every individual are respected; as Addiss has written so powerfully for another global health programme, we must continue to “see both the faces and the numbers”163 of the people that we serve.
Surgery
The S of SAFE comes first not just because it makes a good acronym. Individuals with TT are at continuous risk of progressive visual impairment and are often in considerable pain9. Management to interrupt contact between eyelashes and the eyeball is urgent.
Many different surgical procedures have been used to correct TT, with varying success164. The two procedures recommended by WHO165 are the bilamellar tarsal rotation procedure (BLTR) and the posterior lamellar tarsal rotation procedure (PLTR or modified Trabut). Both involve an incision across the upper eyelid, parallel to the eyelid margin, to release the trachomatous scarring-induced tension in the tarsus that draws eyelashes inwards, followed by placement of sutures to rotate the eyelashes outwards towards their normal anatomical position. Long-term surgical success is principally evaluated by assessing the cumulative incidence of post-operative TT (PTT), which is caused by either immediate surgical failure or longer-term disease progression resulting in eyelashes touching the eyeball again. Other adverse surgical outcomes include pyogenic granulomata and eyelid contour abnormalities166. A pyogenic granuloma is a small, round, highly vascularized growth on the conjunctival surface of the eyelid that develops as a result of injury or to protect against a foreign body such as a suture fragment left in the eyelid. Eyelid contour abnormalities are defined as any deviation >1 mm from the normal curvature of the eyelid. These can range in severity from a slight change in the contour to substantial deviation in the form of a gap between the eye and eyelid, which can often lead to the development of a pyogenic granuloma.
PTT rates vary by procedure, geographical location and type of study, with a cumulative incidence at 1 year after surgery ranging from below 10% to above 40%167. Surgeon skill level is an important predictor of outcome168 but non-physician surgeons can be as successful as ophthalmologists169. A head-to-head trial showed that PLTR was superior to BLTR in reducing the cumulative incidence of PTT, both in the short term and 3 years after surgery170,171. This trial included surgeons originally trained in PLTR who then converted to deliver BLTR, which could have influenced outcomes. Work to investigate whether BLTR-experienced surgeons should convert to PLTR is ongoing172. Currently, WHO recommends that new surgeons should be trained in PLTR173, but existing surgeons trained in BLTR may continue to employ that procedure. Use of absorbable sutures and the TT clamp, which enables a single, safe, guided incision in the eyelid, have both been shown to reduce the incidence of pyogenic granuloma formation174,175. The TT clamp is also successful at reducing eyelid contour abnormalities175. In settings where surgeons are highly skilled, a single dose of azithromycin reduces PTT incidence by about one-third176; however, this effect is diminished in settings with increased rates of PTT177. Doxycycline does not reduce the incidence of PTT178. TT severity can range from a single eyelash touching the eye to the entire eyelid having cicatricial entropion with all eyelashes in contact with the eye. The number of trichiatic eyelashes present pre-operatively and surgeon skill are the most consistent predictors of PTT, with more trichiatic eyelashes increasing the risk of developing PTT168,179. An analysis of multiple clinical trials also showed that peripheral trichiatic eyelashes were a risk factor for PTT regardless of the surgical procedure used180. The evidence on best approaches for the management of TT at first presentation is relatively clear but very little is known about how best to manage PTT. Individualized management by highly skilled surgeons is probably required181.
Since 2013, training programmes for TT surgery have evolved to maximize the skill levels of new surgeons. WHO now recommends that surgical simulation should be included in both new and refresher training programmes and that periodic monitoring of surgical quality after training is advisable124. Standard checklists are available to evaluate the skills required for each of the main surgical procedures165.
In trachoma-endemic communities, surgery is typically provided free of charge, either through outreach campaigns or static services. Uptake of surgical services varies both within and between countries. Patients’ understanding of what the surgery involves, distance to the location at which surgery is available and access to domestic help after surgery all affect uptake182,183. Surgical productivity is also affected by surgeons’ access to surgical supplies and a supervisor184.
The removal of eyelashes with forceps is referred to as epilation, and this provides temporary pain relief. Cross-sectional studies suggest that eyes with evidence of previous epilation have a lower prevalence of corneal opacity185,186. Epilation is widely used in trachoma-endemic communities by individuals who have TT or their caregivers (with caregiver involvement being particularly important for individuals with TT and impaired vision). A trial evaluating epilation versus surgery for eyelids with ≤5 trichiatic eyelashes showed that epilation was non-inferior for vision outcomes but less successful at preventing eyelashes from touching the eye187. Epilation using high-quality forceps and with regular follow-up is recommended where an individual with TT either declines surgery or has no immediate access to it124. Some countries have been reluctant to incorporate advice to epilate into their trachoma programmes based on concerns that it might further reduce surgical uptake. Evidence from Ethiopia suggests that programmatic support for epilation does not adversely affect the willingness of patients to consider future surgical management for TT188.
Although surgery is expected to primarily limit further loss of vision owing to ongoing corneal opacification, high-quality surgery can actually improve visual acuity compared with the pre-operative baseline177,189, presumably by reducing corneal oedema and tearing. TT surgery leads to marked decreases in pain, discharge and photophobia, improving both self-reported physical functioning and quality of life190,191, even in the absence of an improvement in visual acuity. Most PTT occurs within the first 12 months after surgery and subsequent incidence is low, suggesting that the longer-term prognosis for patients who have good outcomes at 1 year is relatively positive171,192.
Antibiotics
Antibiotics are used to clear conjunctival Ct. Two alternative antibiotic regimens are recommended by WHO: 1% tetracycline eye ointment, instilled into the lower conjunctival sac of both eyes twice daily for 6 weeks, or a single oral dose of 20 mg azithromycin/kg body weight, to a maximum of 1 g (ref.117). Evidence for the effect of oral azithromycin is stronger than that for topical tetracycline193. Topical tetracycline treatment also has several disadvantages that limit adherence, including a prolonged treatment course, which cannot be completely directly observed by health-care workers. In addition, instillation into the conjunctival sac is difficult, and the ointment stings slightly on application and briefly blurs the vision after each administration. Oral therapy has the additional benefit of treating extra-ocular Ct infections that might otherwise be reservoirs for conjunctival recurrence68. Tetracycline eye ointment remains on the recommended list because it is very cheap, used in children aged <6 months of age, and is nearly universally available, whereas azithromycin is comparatively expensive if it is not donated.
The high intracellular concentration and long half-life of azithromycin are beneficial for single-dose treatment of Ct, which can only replicate intracellularly. Initial trials showed that oral azithromycin was at least as effective as topical tetracycline for clearing infection in individuals194,195. Efficacy in a single dose and the excellent safety profile enabled consideration of its use in MDA. The Azithromycin in Control of Trachoma trial in Egypt, Gambia and the United Republic of Tanzania demonstrated that azithromycin MDA led to greater reductions in Ct prevalence than topical tetracycline MDA84. This finding was supported by cohort studies demonstrating dramatic reductions in the prevalence and load of conjunctival Ct following azithromycin MDA29,196,197,198.
The goal of the A component is to clear infection from as much of the community as possible, rather than merely treating individuals with clinically apparent active trachoma. Annual199 MDA is employed, with a target of ≥80% coverage of the population at each treatment round117. Azithromycin (specifically Zithromax, Pfizer, NY, USA) is donated to trachoma-endemic countries through the International Trachoma Initiative200 and is offered as tablets to individuals who are both ≥120 cm tall and aged ≥7 years. Azithromycin suspension is given to children aged ≥6 months and <7 years and individuals <120 cm tall; suspension can also be taken by those older and taller than these thresholds if they have difficulty swallowing tablets201. The 20 mg/kg body weight dose of azithromycin is approximated using a dosing pole, up to the adult dose of 1 g (refs129,201,202). Children aged <6 months are offered tetracycline eye ointment.
Determination by trachoma programmes of the need for antibiotic MDA is based on evaluation unit-level prevalence of TF in those aged 1–9 years. If prevalence is ≥30%, the evaluation unit is offered five annual rounds of antibiotics and then re-evaluated with a repeat population-based survey undertaken at least 6 months after the last round. If prevalence is 10–29.9%, the evaluation unit is offered three annual rounds, and if prevalence is 5.0–9.9%, a single round. Antibiotic MDA should be discontinued in evaluation units in which the TF prevalence, estimated through adequately powered prevalence surveys, is <5%.
The incidence of adverse events, such as local irritation or skin reactions, with the use of tetracycline eye ointment is extremely low. Azithromycin is also very well tolerated. In MDA programmes, the overall incidence of reported adverse events following single-dose azithromycin treatment is <10%203,204. Most symptoms are minor and gastrointestinal, including abdominal pain, nausea, vomiting and diarrhoea18,19. In general, the incidence of adverse events increases with increasing age; in children aged <6 months participating in a study of azithromycin MDA for prevention of mortality, the prevalence of adverse events did not significantly differ between children receiving azithromycin or placebo205. Azithromycin MDA may have additional benefits for children, including reducing all-cause mortality (by 13.5% in the largest cluster-randomized trial206) and the burden of some specific pathogens beyond Ct, including Streptococcus pneumoniae, Campylobacter spp., Treponema pallidum subsp. pertenue (the causative agent of yaws) and Plasmodium spp.206,207,208,209,210,211,212,213,214,215,216. Although observational studies have suggested a relationship between azithromycin use and risk of cardiovascular death in adults in the USA217, a randomized study of MDA in Ethiopia found no increase in adult mortality in communities receiving azithromycin compared with those receiving placebo, nor did it find a difference in mortality between individuals aged ≥30 years who took azithromycin and those who did not218.
To date, substantial macrolide resistance in Ct has not been documented following azithromycin MDA for trachoma219,220,221. Some evidence of selection for resistance in non-target organisms exists193,222. In nasopharyngeal Streptococcus pneumoniae collected from population-based samples of children, an increase in macrolide resistance has been found following azithromycin MDA, followed by a reduction in resistance when MDA was discontinued, removing selection pressure223,224. Selection for resistance in other potentially pathogenic organisms, including Escherichia coli and Staphylococcus aureus, has also been documented224,225,226,227,228.
Facial cleanliness and environmental improvement
The goal of the F and E components of the SAFE strategy is to reduce the transmission of conjunctival Ct. For F, the ‘theory of change’ holds that clean faces reduce the amount of infected eye and nose discharge available for transfer to fingers, fomites and flies, and reduce the attractiveness to female M. sorbens of both infected and uninfected eyes. Like the disappearance of trachoma from Europe and North America12, the elimination of trachoma as a public health problem in the Islamic Republic of Iran has been attributed to improvements in hygiene and environmental health229. Multiple cross-sectional studies consistently show an association between a lack of facial cleanliness and the increased probability of having active trachoma57,58,59. However, these studies are limited both in temporality and by the potential for unmeasured confounding.
The evidence base for the efficacy of interventions to improve facial cleanliness is not strong. A pair-matched, community randomized trial in the United Republic of Tanzania found no significant evidence that a hygiene promotion intervention designed to improve face washing among children reduced TF prevalence230. In this trial, the hygiene promotion intervention did reduce the prevalence of a marker of very severe active trachoma, the key driver to scarring, and having a clean face on multiple visits was protective against active trachoma. There is potential for reverse causality or unmeasured confounding between sustained facial cleanliness and active trachoma outcomes. A more recent cluster-randomized trial in Ethiopia found no evidence of an effect of hygiene promotion on the prevalence of conjunctival Ct infection in young children231. Interventions promoting facial cleanliness may be limited by difficulties in achieving sustained behaviour change, which is unlikely to be achieved using the approaches employed by most contemporary trachoma programmes232,233. Because evidence of efficacy for any particular intervention is weak, it is difficult to offer programmes an evidence-based recommendation to alter their approach; instead, it is only possible to observe that current approaches are not in accordance with established theory on behaviour change234.
Environmental improvement interventions attempt to increase access to water and the means to safely dispose of human faeces. Theoretically, increased water access could improve personal hygiene, including face and hand cleanliness, and thereby decrease transmission, while improved sanitation could reduce the abundance of M. sorbens, which lays eggs on human faeces left exposed on soil70. The water used for personal hygiene does not necessarily have to be potable: seawater, for example, would (at least in theory) also be effective. Unfortunately, community randomized trials in Ethiopia and the Gambia have not provided evidence that the provision of latrines reduces the prevalence of active trachoma or conjunctival Ct infection235,236,237. Similarly, evidence for the effectiveness of improving access to water on trachoma markers is inconclusive, lacking support from community randomized trials231,237.
Although a firm evidence base for the F and E components of SAFE is lacking237,238, access to water and sanitation is thought to be important for the management of many other neglected tropical diseases239 as well as being a fundamental human right. A rights-based approach mandates us to continue to promote the F and E components of SAFE while simultaneously encouraging further research on specific interventions designed to reduce transmission of conjunctival Ct.
Quality of life
Active trachoma does not impair vision. Individuals with active trachoma tend to report mild eye irritation, perhaps accompanied by a small amount of eye discharge that may cause eyelash crusting. Because these symptoms are common in trachoma-endemic populations and because the peak prevalence of active trachoma is in young children, these symptoms often go unremarked110.
Conjunctival scarring causes progressive drying of the eyes240,241. This is associated with pervasive eye discomfort and fluctuating visual disturbances that can affect daily activities. Paradoxically, scarring of the lacrimal canaliculi can also lead to epiphora (apparent excessive watering of the eyes), as the normal drainage of the conjunctival sac is impaired and tear fluid escapes onto the cheeks242. Either dry eye or epiphora can have a considerable negative impact on quality of life243,244.
TT is painful to the point of being debilitating, even without objective loss of visual acuity. It has profoundly negative effects on quality of life, psychological health, productivity and social standing9,112,113 that persist for as long as TT is present. For example, when assessed using WHO-recommended instruments, individuals with TT in Amhara Region, Ethiopia, had a substantially lower overall quality of life (mean 34.5 versus 64.6; P < 0.0001) and health satisfaction (mean 38.2 versus 71.7; P < 0.0001) compared with control individuals matched for age, gender and location. These associations are present even in subgroups of patients and control individuals with normal visual acuity112. Surgery for TT improves the quality of life regardless of whether it improves vision9,113,191.
Outlook
Progress against trachoma to date
From 2002 to 2021, the estimated number of people with trichiasis worldwide fell from 7.6 million to 1.8 million, a decrease of 77%. In the same period, the estimated number of people living in areas that warranted treatment with the A, F and E components of the SAFE strategy for trachoma elimination purposes fell from 1.5 billion people to 136 million, a decrease of 91%17,245. Of the 2021 total, 116 million lived in the WHO African region. Ethiopia was the most affected country, where 67 million people were at risk of trachomatous blindness. As of March 2022, WHO had validated 12 countries as having eliminated trachoma as a public health problem: Cambodia, China, Gambia, Ghana, the Islamic Republic of Iran, Lao People’s Democratic Republic, Mexico, Morocco, Myanmar, Nepal, Oman and Saudi Arabia17,246 (Fig. 5). Despite this undoubtedly encouraging progress, it is important to acknowledge that the December 2020 deadline for the global elimination of trachoma as a public health problem, agreed in 1996 (ref.247), was missed; the target date has now been reset to 2030 (ref.1). Of note, progress has been heterogeneous and elimination has proven difficult to achieve in some areas. This is further discussed below.

As of March 2022, 44 countries were known to require interventions to eliminate trachoma as a public health problem, 7 required investigation to determine whether interventions are required, 3 claimed to have eliminated trachoma as a public health problem, and 12 had been validated as having eliminated trachoma as a public health problem. The boundaries and names shown and the designations used on this map do not imply the expression of any opinion whatsoever on the part of the authors or the institutions with which they are affiliated concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Adapted with permission from ref.291, World Health Organization (WHO).
Future progress against trachoma
Elimination as a public health problem is a considerably more modest public health goal than eradication, which requires the permanent reduction to zero of the worldwide incidence of an infection248. At an international meeting in 2019, most of the trachoma stakeholders who were present and surveyed believed trachoma could actually be eradicated at some future date249. Others believe that setting such a goal would not be in the best overall interest of global health, since the opportunity cost might be considerably greater than the immediate public health benefit250. This issue (like all other issues related to future progress against trachoma) will benefit from continuing input from all relevant stakeholders, particularly national programme managers. If eradiation was to be targeted, improvements in surveillance systems, increased funding, enhanced community engagement and the absence of emergent antibiotic resistance (or development of an infection-blocking vaccine) may be pre-requisites249.
An effective Ct vaccine would certainly change the landscape for trachoma. Although 100 years of work on chlamydial vaccines have not yet generated an effective product, encouraging data have emerged from a phase I trial of a recombinant protein subunit vaccine targeting the major outer membrane protein of Ct161. The lack of established immunological correlates of protection161 and the relative difficulty of determining disease-related outcomes in the urogenital tract suggest that future partnership of vaccine developers with trachoma programmes may be rewarding: the protection offered by an effective vaccine will be easier to observe in the conjunctivae.
In addition to the further efforts to develop and make available an efficacious future vaccine, weaknesses of current programmes need attention, as several types of measurement error put further progress at risk.
The imperfect predictive power of TF prevalence as a marker for Ct infection at the population level hampers progress; evaluation of indicators of conjunctival Ct transmission intensity other than TF prevalence is an area of growing interest. Serological indicators may have an application in monitoring for recrudescence after antibiotic MDA has been discontinued, including in post-validation surveillance251,252,253. Programmes need guidance on optimal strategies to detect possible recrudescence but evidence on which to base this guidance is currently limited. Serosurveys would be one possible approach. However, currently assayed anti-Ct antibodies are not specific for trachoma Ct strains; thus, serosurveillance approaches using these antibodies would need to be driven primarily by data from children who have cleared maternal antibodies and not yet reached the age of sexual debut and would need to accept the contribution of inclusion conjunctivitis to population-level seropositivity. Identification of an anti-Ct antibody specific to trachoma strains would be a major step forward in the utility of serosurveillance.
Another measurement issue arises from the difficulty of estimating the prevalence of a rare condition. Despite assiduous attention to epidemiological principles in survey design and implementation of quality control and quality assurance tools126, prevalence estimates generated by surveys remain estimates, subject to error. This becomes particularly important when public health decisions are made against fine margins as is inevitably the case when measuring progress against the elimination prevalence threshold (0.2%) for TT. The use of a geospatial rather than traditional frequentist statistical approach enables the harnessing of spatial correlation in prevalence data and may therefore improve the accuracy of TT prevalence estimates254.
In addition, important questions about each component of the SAFE strategy remain to be answered. For the S component, data on the best approaches for managing PTT are needed as, even in the best hands, at least 10% of individuals who receive surgery for TT will commonly develop PTT167. Based on available global data, at least 180,000 individuals who had TT in June 2021 (ref.17) will need further surgical management after their primary operations. In most settings, patients with PTT are currently managed with the same procedure that they initially received to manage their TT. Two surgical approaches for correcting PTT are currently being investigated in a clinical trial255, PLTR and the Bevel-Rotation Advancement Procedure (B-RAP)256. PLTR involves a partial-thickness incision followed by rotation of the distal fragment to return eyelashes to their normal anatomical position. In doing so, the distal and proximal tarsal fragments are overlapped, creating a thicker tarsus, which may be more likely to result in an eyelid contour abnormality. B-RAP is a new procedure designed to overcome this issue by creating a bevelled incision of the tarsus, dissecting between the anterior and posterior lamellae and removing scar tissue. This approach enables the marginal rotation to be combined with a posterior lamellar advancement and a reduction in eyelid thickness. Additionally, some countries are beginning to recommend epilation as a definitive management strategy for PTT in which just one or two eyelashes touch the sclera temporal or nasal to the cornea257.
For countries to clear their TT surgery backlogs, efficient case-finding strategies are needed. The use of machine learning to develop image recognition software for TT identification is currently under way, which has the potential to improve broad-scale screening for TT. Similar programmes are also being developed for the identification of active trachoma258. As TT becomes less common, strategies for ensuring access to high-quality surgery for all who need it will continue to be important. This will require surgeons to maintain their skills through regular practise on simulators, and potentially other creative solutions for delivering integrated, people-centred services259 to a progressively more scattered population in need.
For the A component, research priorities depend on local epidemiology. In areas where Ct transmission persists despite years of implementation of A, F and E, such as some areas of Ethiopia260, new strategies (within the A, F or E components) for reducing community transmission of conjunctival Ct are needed18. In these areas, multiple rounds of annual azithromycin MDA may have produced a new equilibrium wherein transmission continues but at lower levels than at baseline. Although increased antibiotic pressure, such as through more frequent MDA or a higher target antibiotic coverage, could hypothetically reduce infection prevalence, community randomized trials in Ethiopia and Niger have not consistently found empirical support for this theory261,262,263,264,265. However, in one trial in Ethiopia, quarterly treatment offered only to those aged 1–10 years achieved lower conjunctival Ct prevalence than annual MDA to people of all ages266, and evidence of a herd protection effect was noted with reduced Ct prevalence in untreated older children and adults267. This is likely to be a demonstration of a ‘core group’ effect in local transmission dynamics, in which suppression of transmission from and between children prevents infection from sustaining an equilibrium level in the population as a whole268. Further studies are needed.
Work is also required to determine how to identify where (or even whether) antibiotic MDA is needed in evaluation units in which the TF prevalence is around the 5% elimination threshold. In communities in the United Republic of Tanzania with a baseline TF prevalence of 5.0–9.9% randomized to a single round of antibiotic MDA or no treatment, no difference in TF prevalence after 12 months was observed between study arms269. Longer-term study of the need for antibiotics in evaluation units where trachoma is disappearing or where the prevalence of TF seems to be rising again after antibiotic MDA discontinuation would provide greater insight into where and how antibiotics should be used for trachoma270. Tests for Ct infection need further exploration as potential guides for decision-making271.
For the F and E components, a better understanding of Ct transmission and reliable markers of sustained facial cleanliness would help in the testing of candidate interventions and assessment of programme effectiveness272,273,274. A community randomized trial of combined facial cleanliness and environmental improvement interventions did not prevent recrudescence in conjunctival Ct infection prevalence after antibiotic MDA was discontinued in a trachoma hyperendemic population231,275, but it is important to note that coverage of interventions fell short of the 80–90% that models indicate might be a threshold for effectiveness65. Randomized controlled trials of WASH interventions are challenging to undertake, both logistically and in terms of achieving the transformative change in WASH access and use that is probably important276. However, such trials are essential to evaluate how best to deliver the F and E components to achieve sustained progress against trachoma. When washing the face, the use of soap may be important277.
The SAFE strategy is a combination of measures intended to prevent visual impairment from trachoma at multiple levels. Prevention of iatrogenic harm is also important and can be achieved through maintaining high-quality surgery and exercising good antibiotic stewardship. Surgical quality should be maximized through improvements in training, support, supervision and audit184,278,279 of surgeons as well as consideration of who to operate on188. Good antibiotic stewardship involves avoidance of unnecessary antibiotic distribution280. Minimization of pressure driving the development of antimicrobial resistance222 is growing in importance. Developing better tools for characterizing the population-level need for anti-Ct antibiotics for trachoma elimination purposes should help. Greater attention to visual rehabilitation and disability inclusion for those whose sight has already been affected by trachoma281 also needs to be built into programmes. The effects of COVID-19-related interruptions to community-based work on trachoma have yet to be empirically determined; models suggest that these may be considerable282,283.
Beyond trachoma
In January 2021, WHO published the road map for neglected tropical diseases 2021–2030 (ref.1). A neglected tropical disease research and development blueprint, to be published as a companion document, is being prepared. Research needs for trachoma, including some of the questions identified above, will form part of this. A common issue for all neglected tropical diseases will be how best to integrate what have often been relatively disease-specific programmes to achieve maximum efficiency, and how to further combine those efforts into a whole-of-health-system approach in collaboration with other sectors284,285,286,287. It is our hope that further characterizing the research needs of trachoma in this way, and then fulfilling those needs, will lead to a 2030 world in which trachoma is no longer a public health problem.
References
World Health Organization. Ending the Neglect to Attain the Sustainable Development Goals: a Road Map for Neglected Tropical Diseases 2021–2030 (World Health Organization, 2020).
Flaxman, S. R. et al. Global causes of blindness and distance vision impairment 1990–2020: a systematic review and meta-analysis. Lancet Glob. Health 5, e1221–e1234 (2017).
Taylor, H. R. et al. An animal model of trachoma II. The importance of repeated reinfection. Invest. Ophthalmol. Vis. Sci. 23, 507–515 (1982).
Grayston, J. T., Wang, S. P., Yeh, L. J. & Kuo, C. C. Importance of reinfection in the pathogenesis of trachoma. Rev. Infect. Dis. 7, 717–725 (1985).
Hadfield, J. et al. Comprehensive global genome dynamics of Chlamydia trachomatis show ancient diversification followed by contemporary mixing and recent lineage expansion. Genome Res. 27, 1220–1229 (2017).
West, S. K., Munoz, B., Mkocha, H., Hsieh, Y. H. & Lynch, M. C. Progression of active trachoma to scarring in a cohort of Tanzanian children. Ophthalmic Epidemiol. 8, 137–144 (2001).
Wolle, M. A., Munoz, B. E., Mkocha, H. & West, S. K. Constant ocular infection with Chlamydia trachomatis predicts risk of scarring in children in Tanzania. Ophthalmology 116, 243–247 (2009).
Rajak, S. N. et al. The clinical phenotype of trachomatous trichiasis in Ethiopia: not all trichiasis is due to entropion. Invest. Ophthalmol. Vis. Sci. 52, 7974–7980 (2011).
Palmer, S. L. et al. ‘A living death’: a qualitative assessment of quality of life among women with trichiasis in rural Niger. Int. Health 6, 291–297 (2014).
Frick, K. D., Hanson, C. L. & Jacobson, G. A. Global burden of trachoma and economics of the disease. Am. J. Trop. Med. Hyg. 69, 1–10 (2003).
Habtamu, E. et al. Trachoma and relative poverty: a case-control study. PLoS Negl. Trop. Dis. 9, e0004228 (2015).
Taylor, H. R. Trachoma: a Blinding Scourge from the Bronze Age to the Twenty-First Century (Centre for Eye Research Australia, 2008).
Dolin, P. J. et al. Reduction of trachoma in a sub-Saharan village in absence of a disease control programme. Lancet 349, 1511–1512 (1997).
Hoechsmann, A. et al. Reduction of trachoma in the absence of antibiotic treatment: evidence from a population-based survey in Malawi. Ophthalmic Epidemiol. 8, 145–153 (2001).
Jha, H. et al. Disappearance of trachoma from Western Nepal. Clin. Infect. Dis. 35, 765–768 (2002).
Flueckiger, R. M. et al. The global burden of trichiasis in 2016. PLoS Negl. Trop. Dis. 13, e0007835 (2019).
World Health Organization. WHO Alliance for the Global Elimination of Trachoma by 2020: progress report on elimination of trachoma, 2020. Wkly Epidemiol. Rec. 96, 353–364 (2021). The most recent annual progress report from WHO on global trachoma elimination.
Sata, E. et al. Twelve-year longitudinal trends in trachoma prevalence among children aged 1–9 years in Amhara, Ethiopia, 2007–2019. Am. J. Trop. Med. Hyg. https://doi.org/10.4269/ajtmh.20-1365 (2021).
Duke-Elder, W. S. Textbook of Ophthalmology. Volume II: Clinical Methods of Examination, Congenital and Developmental Anomalies, General Pathological and Therapeutic Considerations, Diseases of the Outer Eye (Henry Kimpton, 1937).
Dunn, F. L. Sociomedical contributions to trachoma research and intervention. Rev. Infect. Dis. 7, 783–786 (1985).
Taylor, H. R. Trachoma in Australia. Med. J. Aust. 175, 371–372 (2001).
Mabey, D. C., Bailey, R. L., Ward, M. E. & Whittle, H. C. A longitudinal study of trachoma in a Gambian village: implications concerning the pathogenesis of chlamydial infection. Epidemiol. Infect. 108, 343–351 (1992).
Taylor, H. R. & Anjou, M. D. Trachoma in Australia: an update. Clin. Exp. Ophthalmol. 41, 508–512 (2013).
Smith, J. L. et al. The geographical distribution and burden of trachoma in Africa. PLoS Negl. Trop. Dis. 7, e2359 (2013).
Tafida, A. et al. Poverty and blindness in Nigeria: results from the National Survey of Blindness and Visual Impairment. Ophthalmic Epidemiol. 22, 333–341 (2015).
Solomon, A. W. et al. Strategies for control of trachoma: observational study with quantitative PCR. Lancet 362, 198–204 (2003).
Taylor, H. R., Siler, J. A., Mkocha, H. A., Munoz, B. & West, S. The natural history of endemic trachoma: a longitudinal study. Am. J. Trop. Med. Hyg. 46, 552–559 (1992).
Burton, M. J. et al. Re-emergence of Chlamydia trachomatis infection after mass antibiotic treatment of a trachoma-endemic Gambian community: a longitudinal study. Lancet 365, 1321–1328 (2005).
Solomon, A. W. et al. Mass treatment with single-dose azithromycin for trachoma. N. Engl. J. Med. 351, 1962–1971 (2004).
West, E. S. et al. Mass treatment and the effect on the load of Chlamydia trachomatis infection in a trachoma-hyperendemic community. Invest. Ophthalmol. Vis. Sci. 46, 83–87 (2005).
Last, A. et al. Spatial clustering of high load ocular Chlamydia trachomatis infection in trachoma: a cross-sectional population-based study. Pathog. Dis. 75, 1–10 (2017).
World Health Organization Strategic and Technical Advisory Group on Neglected Tropical Diseases. Design and Validation of a Trachomatous Trichiasis-Only Survey WHO/HTM/NTD/PCT/2017.08 (World Health Organization, 2018).
Bero, B. et al. Prevalence of and risk factors for trachoma in Oromia Regional State of Ethiopia: results of 79 population-based prevalence surveys conducted with the Global Trachoma Mapping Project. Ophthalmic Epidemiol. 23, 392–405 (2016).
Adera, T. H. et al. Prevalence of and risk factors for trachoma in southern nations, nationalities, and peoples’ region, ethiopia: results of 40 population-based prevalence surveys carried out with the global trachoma mapping project. Ophthalmic Epidemiol. 23, 84–93 (2016).
Cromwell, E. A. et al. The excess burden of trachomatous trichiasis in women: a systematic review and meta-analysis. Trans. R. Soc. Trop. Med. Hyg. 103, 985–992 (2009).
Wondimu, A. & Bejiga, A. Prevalence of trachomatous trichiasis in the community of Alaba District, Southern Ethiopia. East. Afr. Med. J. 80, 365–368 (2003).
Courtright, P. & West, S. K. Contribution of sex-linked biology and gender roles to disparities with trachoma. Emerg. Infect. Dis. 10, 2012–2016 (2004).
Berry, A. & Hall, J. V. The complexity of interactions between female sex hormones and Chlamydia trachomatis infections. Curr. Clin. Microbiol. Rep. 6, 67–75 (2019).
Wang, S. P. & Grayston, J. T. Immunologic relationship between genital TRIC, lymphogranuloma venereum, and related organisms in a new microtiter indirect immunofluorescence test. Am. J. Ophthalmol. 70, 367–374 (1970).
Elwell, C., Mirrashidi, K. & Engel, J. Chlamydia cell biology and pathogenesis. Nat. Rev. Microbiol. 14, 385–400 (2016).
Gitsels, A., Sanders, N. & Vanrompay, D. Chlamydial infection from outside to inside. Front. Microbiol. 10, 2329 (2019).
Caldwell, H. D., Kromhout, J. & Schachter, J. Purification and partial characterization of the major outer membrane protein of Chlamydia trachomatis. Infect. Immun. 31, 1161–1176 (1981).
Harris, S. R. et al. Whole-genome analysis of diverse Chlamydia trachomatis strains identifies phylogenetic relationships masked by current clinical typing. Nat. Genet. 44, 413–419 (2012).
Caldwell, H. D. et al. Polymorphisms in Chlamydia trachomatis tryptophan synthase genes differentiate between genital and ocular isolates. J. Clin. Invest. 111, 1757–1769 (2003).
Puck, A., Liappis, N. & Hildenbrand, G. Ion exchange column chromatographic investigation of free amino acids in tears of healthy adults. Ophthalmic Res. 16, 284–288 (1984).
Belland, R. J. et al. Genomic transcriptional profiling of the developmental cycle of Chlamydia trachomatis. Proc. Natl Acad. Sci. USA 100, 8478–8483 (2003).
Ohashi, K., Burkart, V., Flohé, S. & Kolb, H. Cutting edge: heat shock protein 60 is a putative endogenous ligand of the Toll-like receptor-4 complex. J. Immunol. 164, 558–561 (2000).
Bailey, R., Osmond, C., Mabey, D. C., Whittle, H. C. & Ward, M. E. Analysis of the household distribution of trachoma in a Gambian village using a Monte Carlo simulation procedure. Int. J. Epidemiol. 18, 944–951 (1989).
West, S. K., Munoz, B., Turner, V. M., Mmbaga, B. B. & Taylor, H. R. The epidemiology of trachoma in central Tanzania. Int. J. Epidemiol. 20, 1088–1092 (1991).
Blake, I. M. et al. Estimating household and community transmission of ocular Chlamydia trachomatis. PLoS Negl. Trop. Dis. 3, e401 (2009).
Polack, S. R. et al. The household distribution of trachoma in a Tanzanian village: an application of GIS to the study of trachoma. Trans. R. Soc. Trop. Med. Hyg. 99, 218–225 (2005).
Bailey, R. L. et al. Molecular epidemiology of trachoma in a Gambian village. Br. J. Ophthalmol. 78, 813–817 (1994).
Hägi, M. et al. Active trachoma among children in Mali: Clustering and environmental risk factors. PLoS Negl. Trop. Dis. 4, e583 (2010).
Burton, M. J. et al. Which members of a community need antibiotics to control trachoma? Conjunctival Chlamydia trachomatis infection load in Gambian villages. Invest. Ophthalmol. Vis. Sci. 44, 4215–4222 (2003).
Last, A. et al. Detecting extra-ocular Chlamydia trachomatis in a trachoma-endemic community in Ethiopia: identifying potential routes of transmission. PLoS Negl. Trop. Dis. 14, e0008120 (2020).
Broman, A. T., Shum, K., Munoz, B., Duncan, D. D. & West, S. K. Spatial clustering of ocular chlamydial infection over time following treatment, among households in a village in Tanzania. Invest. Ophthalmol. Vis. Sci. 47, 99–104 (2006).
Schemann, J. F. et al. Risk factors for trachoma in Mali. Int. J. Epidemiol. 31, 194–201 (2002).
Taylor, H. R. et al. Hygiene factors and increased risk of trachoma in central Tanzania. Arch. Ophthalmol. 107, 1821–1825 (1989).
West, S. et al. Water availability and trachoma. Bull. World Health Organ. 67, 71–75 (1989).
Golovaty, I. et al. Access to water source, latrine facilities and other risk factors of active trachoma in Ankober, Ethiopia. PLoS ONE 4, e6702 (2009).
Amza, A. et al. Community risk factors for ocular Chlamydia infection in Niger: pre-treatment results from a cluster-randomized trachoma trial. PLoS Negl. Trop. Dis. 6, e1586 (2012).
Harding-Esch, E. M. et al. Trachoma prevalence and associated risk factors in The Gambia and Tanzania: baseline results of a cluster randomised controlled trial. PLoS Negl. Trop. Dis. 4, e861 (2010).
Katz, J. et al. Prevalence and risk factors for trachoma in Sarlahi district, Nepal. Br. J. Ophthalmol. 80, 1037–1041 (1996).
Hsieh, Y. H., Bobo, L. D., Quinn, T. O. & West, S. K. Risk factors for trachoma: 6-year follow-up of children aged 1 and 2 years. Am. J. Epidemiol. 152, 204–211 (2000).
Garn, J. V. et al. Sanitation and water supply coverage thresholds associated with active trachoma: modeling cross-sectional data from 13 countries. PLoS Negl. Trop. Dis. 12, e0006110 (2018). Secondary analysis of cross-sectional data from 13 countries showing that community-level sanitation coverage exceeding 80% is associated with herd protection against active trachoma in children.
Baggaley, R. F. et al. Distance to water source and altitude in relation to active trachoma in Rombo district, Tanzania. Trop. Med. Int. Health 11, 220–227 (2006).
Collier, L. H., Duke-Elder, S. & Jones, B. R. Experimental trachoma produced by cultured virus. Br. J. Ophthalmol. 42, 705–720 (1958).
West, S. et al. Nonocular Chlamydia infection and risk of ocular reinfection after mass treatment in a trachoma hyperendemic area. Invest. Ophthalmol. Vis. Sci. 34, 3194–3198 (1993).
Gower, E. W. et al. Chlamydial positivity of nasal discharge at baseline is associated with ocular chlamydial positivity 2 months following azithromycin treatment. Invest. Ophthalmol. Vis. Sci. 47, 4767–4771 (2006).
Emerson, P. M., Bailey, R. L., Mahdi, O. S., Walraven, G. E. & Lindsay, S. W. Transmission ecology of the fly Musca sorbens, a putative vector of trachoma. Trans. R. Soc. Trop. Med. Hyg. 94, 28–32 (2000).
Brewer, N. et al. Persistence and significance of Chlamydia trachomatis in the housefly, Musca domestica L. Vector Borne Zoonotic Dis. https://doi.org/10.1089/vbz.2021.0021 (2021).
Miller, K. et al. Pesky trachoma suspect finally caught. Br. J. Ophthalmol. 88, 750–751 (2004).
Lee, S. et al. Chlamydia on children and flies after mass antibiotic treatment for trachoma. Am. J. Trop. Med. Hyg. 76, 129–131 (2007).
Emerson, P. M. et al. Effect of fly control on trachoma and diarrhoea. Lancet 353, 1401–1403 (1999).
Versteeg, B. et al. Viability PCR shows that non-ocular surfaces could contribute to transmission of Chlamydia trachomatis infection in trachoma. PLoS Negl. Trop. Dis. 14, e0008449 (2020). Experimental study demonstrating that Ct can remain viable on plastic, cotton cloth and skin for over 24 hours, firmly establishing the potential for fomite transmission.
Gambhir, M. et al. The development of an age-structured model for trachoma transmission dynamics, pathogenesis and control. PLoS Negl. Trop. Dis. 3, e462 (2009). Mathematical model of transmission of conjunctival Ct and development of cicatricial disease, predicting, amongst other things, that more than 100 infections during an individual’s lifetime are needed to generate trachomatous scarring and more than 150 infections are needed to develop TT.
Bailey, R., Duong, T., Carpenter, R., Whittle, H. & Mabey, D. The duration of human ocular Chlamydia trachomatis infection is age dependent. Epidemiol. Infect. 123, 479–486 (1999).
Jawetz, E., Rose, L., Hanna, L. & Thygeson, P. Experimental inclusion conjunctivitis in man: measurements of infectivity and resistance. JAMA 194, 150–162 (1965).
Grassly, N. C., Ward, M. E., Ferris, S., Mabey, D. C. & Bailey, R. L. The natural history of trachoma infection and disease in a Gambian cohort with frequent follow-up. PLoS Negl. Trop. Dis. 2, e341 (2008).
Hu, V. H., Holland, M. J. & Burton, M. J. Trachoma: protective and pathogenic ocular immune responses to Chlamydia trachomatis. PLoS Negl. Trop. Dis. 7, e2020 (2013).
Baral, K. et al. Reliability of clinical diagnosis in identifying infectious trachoma in a low-prevalence area of Nepal. Bull. World Health Organ. 77, 461–466 (1999).
Bird, M. et al. Does the diagnosis of trachoma adequately identify ocular chlamydial infection in trachoma-endemic areas? J. Infect. Dis. 187, 1669–1673 (2003).
Michel, C. E., Roper, K. G., Divena, M. A., Lee, H. H. & Taylor, H. R. Correlation of clinical trachoma and infection in Aboriginal communities. PLoS Negl. Trop. Dis. 5, e986 (2011).
Schachter, J. et al. Azithromycin in control of trachoma. Lancet 354, 630–635 (1999). Community randomized trial demonstrating that MDA of azithromycin reduces the prevalence of Ct infection and active trachoma.
Ramadhani, A. M., Derrick, T., Holland, M. J. & Burton, M. J. Blinding trachoma: systematic review of rates and risk factors for progressive disease. PLoS Negl. Trop. Dis. 10, e0004859 (2016).
Dawson, C. R., Marx, R., Daghfous, T., Juster, R. & Schachter, J. in Chlamydial Infections: Proceedings of the Seventh International Symposium on Human Chlamydial Infections (eds Bowie, W. R. et al.) 271–278 (Cambridge University Press, 1990).
Wolle, M. A., Munoz, B., Mkocha, H. & West, S. K. Age, sex, and cohort effects in a longitudinal study of trachomatous scarring. Invest. Ophthalmol. Vis. Sci. 50, 592–596 (2009).
Ramadhani, A. M. et al. Progression of scarring trachoma in Tanzanian children: a four-year cohort study. PLoS Negl. Trop. Dis. 13, e0007638 (2019). Cohort study establishing the strong association between repeated episodes of papillary conjunctival inflammation and trachomatous scarring, building on earlier work.
Burton, M. J. et al. Pathogenesis of progressive scarring trachoma in Ethiopia and Tanzania and its implications for disease control: two cohort studies. PLoS Negl. Trop. Dis. 9, e0003763 (2015).
Flueckiger, R. M. et al. Understanding the spatial distribution of trichiasis and its association with trachomatous inflammation — follicular. BMC Infect. Dis. 19, 364 (2019).
Hu, V. H. et al. Non-chlamydial bacterial infection and progression of conjunctival scarring in trachoma. Invest. Ophthalmol. Vis. Sci. 59, 2339–2344 (2018).
Taylor, H. R., Prendergast, R. A., Dawson, C. R., Schachter, J. & Silverstein, A. M. An animal model for cicatrizing trachoma. Invest. Ophthalmol. Vis. Sci. 21, 422–433 (1981).
Taylor, H. R., Johnson, S. L., Schachter, J. & Prendergast, R. A. An animal model of trachoma: IV. The failure of local immunosuppression to reveal inapparent infection. Invest. Ophthalmol. Vis. Sci. 24, 647–650 (1983).
Taylor, H. R., Johnson, S. L., Schachter, J., Caldwell, H. D. & Prendergast, R. A. Pathogenesis of trachoma: the stimulus for inflammation. J. Immunol. 138, 3023–3027 (1987).
el-Asrar, A. M. et al. Immunopathology of trachomatous conjunctivitis. Br. J. Ophthalmol. 73, 276–282 (1989).
Hu, V. H. et al. In vivo confocal microscopy of trachoma in relation to normal tarsal conjunctiva. Ophthalmology 118, 747–754 (2011).
Hu, V. H. et al. In vivo confocal microscopy and histopathology of the conjunctiva in trachomatous scarring and normal tissue: a systematic comparison. Br. J. Ophthalmol. 97, 1333–1337 (2013).
Hu, V. H. et al. Immunohistochemical analysis of scarring trachoma indicates infiltration by natural killer and undefined CD45 negative cells. PLoS Negl. Trop. Dis. 10, e0004734 (2016).
Derrick, T. et al. Increased epithelial expression of CTGF and S100A7 with elevated subepithelial expression of IL-1beta in trachomatous trichiasis. PLoS Negl. Trop. Dis. 10, e0004752 (2016).
Rasmussen, S. J. et al. Secretion of proinflammatory cytokines by epithelial cells in response to Chlamydia infection suggests a central role for epithelial cells in chlamydial pathogenesis. J. Clin. Invest. 99, 77–87 (1997).
Darville, T. & Hiltke, T. J. Pathogenesis of genital tract disease due to Chlamydia trachomatis. J. Infect. Dis. 201, S114–S125 (2010).
Burton, M. J., Bailey, R. L., Jeffries, D., Mabey, D. C. & Holland, M. J. Cytokine and fibrogenic gene expression in the conjunctivas of subjects from a Gambian community where trachoma is endemic. Infect. Immun. 72, 7352–7356 (2004).
Natividad, A. et al. Human conjunctival transcriptome analysis reveals the prominence of innate defense in Chlamydia trachomatis infection. Infect. Immun. 78, 4895–4911 (2010).
Ramadhani, A. M. et al. Immunofibrogenic gene expression patterns in Tanzanian children with ocular chlamydia trachomatis infection, active trachoma and scarring: baseline results of a 4-year longitudinal study. Front. Cell Infect. Microbiol. 7, 406 (2017).
Derrick, T. et al. Immunopathogenesis of progressive scarring trachoma: results of a 4-year longitudinal study in Tanzanian children. Infect. Immun. 88, e00629-19 (2020).
Stephens, R. S. The cellular paradigm of chlamydial pathogenesis. Trends Microbiol. 11, 44–51 (2003).
Vicetti Miguel, R. D., Quispe Calla, N. E., Pavelko, S. D. & Cherpes, T. L. Intravaginal Chlamydia trachomatis challenge infection elicits TH1 and TH17 immune responses in mice that promote pathogen clearance and genital tract damage. PLoS ONE 11, e0162445 (2016).
Hu, V. H. et al. Innate immune responses and modified extracellular matrix regulation characterize bacterial infection and cellular/connective tissue changes in scarring trachoma. Infect. Immun. 80, 121–130 (2012).
Kechagia, J. Z., Ezra, D. G., Burton, M. J. & Bailly, M. Fibroblasts profiling in scarring trachoma identifies IL-6 as a functional component of a fibroblast-macrophage pro-fibrotic and pro-inflammatory feedback loop. Sci. Rep. 6, 28261 (2016).
Solomon, A. W., Peeling, R. W., Foster, A. & Mabey, D. C. Diagnosis and assessment of trachoma. Clin. Microbiol. Rev. 17, 982–1011 (2004).
Talero, S. L., Munoz, B. & West, S. K. Potential effect of epilation on the outcome of surgery for trachomatous trichiasis. Transl. Vis. Sci. Technol. 8, 30 (2019).
Habtamu, E. et al. The impact of trachomatous trichiasis on quality of life: a case control study. PLoS Negl. Trop. Dis. 9, e0004254 (2015).
Dhaliwal, U., Nagpal, G. & Bhatia, M. S. Health-related quality of life in patients with trachomatous trichiasis or entropion. Ophthalmic Epidemiol. 13, 59–66 (2006).
World Health Organization. Report of the 4th Global Scientific Meeting on Trachoma, Geneva. WHO/CDS/NTD/PCT/2019.03 27–29 (World Health Organization, 2019).
Solomon, A. W. et al. The simplified trachoma grading system, amended. Bull. World Health Organ. 98, 698–705 (2020). Defines and discusses the WHO simplified trachoma grading system, intended for use by non-specialist personnel working at community level, and now the basis for determining whether trachoma is a public health problem at the population level.
Solomon, A. W., Le Mesurier, R. T. & Williams, W. J. A diagnostic instrument to help field graders evaluate active trachoma. Ophthalmic Epidemiol. 25, 399–402 (2018).
Solomon, A. W. et al. Trachoma Control: a Guide for Programme Managers (World Health Organization, 2006).
Tullo, A. B., Richmond, S. J. & Easty, D. L. The presentation and incidence of paratrachoma in adults. J. Hyg. 87, 63–69 (1981).
Burr, S. E. et al. Association between ocular bacterial carriage and follicular trachoma following mass azithromycin distribution in The Gambia. PLoS Negl. Trop. Dis. 7, e2347 (2013).
Elston, D. M. Confirmation bias in medical decision-making. J. Am. Acad. Dermatol. 82, 572 (2020).
Dawson, C. R., Jones, B. R. & Tarizzo, M. L. Guide to Trachoma Control in Programmes for the Prevention of Blindness (World Health Organization, 1981).
Thylefors, B., Dawson, C. R., Jones, B. R., West, S. K. & Taylor, H. R. A simple system for the assessment of trachoma and its complications. Bull. World Health Organ. 65, 477–483 (1987).
Macleod, C. et al. Eyelash epilation in the absence of trichiasis: results of a population-based prevalence survey in the western division of Fiji. PLoS Negl. Trop. Dis. 11, e0005277 (2017).
World Health Organization. Second Global Scientific Meeting on Trachomatous Trichiasis. Cape Town, 4-6 November 2015 WHO/HTM/NTD/2016.5 (World Health Organization, 2016).
Solomon, A. W. et al. The Global Trachoma Mapping Project: methodology of a 34-country population-based study. Ophthalmic Epidemiol. 22, 214–225 (2015).
Solomon, A. W. et al. Quality assurance and quality control in the global trachoma mapping project. Am. J. Trop. Med. Hyg. 99, 858–863 (2018).
Courtright, P., Flueckiger, R., Harding-Esch, E. M., Lewallen, S. & Solomon, A. W. Tropical Data: Trichiasis Surveys-Training for Mapping of Trachomatous Trichiasis (version 1.1) (International Coalition for Trachoma Control, 2018).
Courtright, P. et al. Tropical Data: Training System for Trachoma Prevalence Surveys (version 3) (International Coalition for Trachoma Control, 2019).
Solomon, A. W. et al. Pilot study of the use of community volunteers to distribute azithromcyin for trachoma control in Ghana. Bull. World Health Organ. 79, 8–14 (2001).
de Oliveira Alves, A., Ferreira, V. S. & Bernardes Filho, F. Young boy with roughening in the inner eyelids. Ann. Emerg. Med. 71, e13–e14 (2018).
Talero, S. L., Resnikoff, S., Saboya-Diaz, M. I. & Solomon, A. W. Giant papillae versus lymphoid follicles of the conjunctiva. Ann. Emerg. Med. 73, 694–695 (2019).
Blake, I. M. et al. Targeting antibiotics to households for trachoma control. PLoS Negl. Trop. Dis. 4, e862 (2010).
Senyonjo, L. et al. Operational adaptations of the trachoma pre-validation surveillance strategy employed in Ghana: a qualitative assessment of successes and challenges. Infect. Dis. Poverty 8, 78 (2019).
Greene, G. S., West, S. K., Mkocha, H., Munoz, B. & Merbs, S. L. Assessment of a novel approach to identify trichiasis cases using community treatment assistants in Tanzania. PLoS Negl. Trop. Dis. 9, e0004270 (2015).
Sanders, A. M., Adam, M., Aziz, N., Callahan, E. K. & Elshafie, B. E. Piloting a trachomatous trichiasis patient case-searching approach in two localities of Sudan. Trans. R. Soc. Trop. Med. Hyg. 114, 561–565 (2020).
Kabona, G., Flueckiger, R. M., Ngondi, J., Mwingira, U. & Simon, A. Trachomatous Trichiasis Management in Tanzania: Investigation of the Productivity of Case Finding and Referral of Patients to Trichiasis Surgery Services (RTI International, 2019).
Mpyet, C., Ramyil, A., Dami, N. & Courtright, P. Use of an inexpensive magnifier with light source in the diagnosis of trichiasis among community-based case finders in Nigeria. Ophthalmic Epidemiol. 25, 138–142 (2018).
World Health Organization. Validation of Elimination of Trachoma as a Public Health Problem WHO/HTM/NTD/2016.8 (World Health Organization, 2016).
World Health Organization Strategic and Technical Advisory Group on Neglected Tropical Diseases. Design Parameters for Population-Based Trachoma Prevalence Surveys WHO/HTM/NTD/PCT/2018.07 (World Health Organization, 2018).
Stelmach, R. D. et al. The costs of monitoring trachoma elimination: evaluating the costs of trachoma impact, surveillance, and trachomatous trichiasis (TT)-only surveys. PLoS Negl. Trop. Dis. 13, e0007605 (2019).
Solomon, A. W. et al. The importance of failure: how doing impact surveys that fail saves trachoma programs money. Am. J. Trop. Med. Hyg. 103, 2481–2487 (2020).
Solomon, A. W. & Kurylo, E. The global trachoma mapping project. Commun. Eye Health 27, 18 (2014).
West, S. K. Milestones in the fight to eliminate trachoma. Ophthalmic Physiol. Opt. 40, 66–74 (2020).
Courtright, P. et al. Strengthening the links between mapping, planning and global engagement for disease elimination: lessons learnt from trachoma. Br. J. Ophthalmol. 102, 1324–1327 (2018).
Roberts, C. H. et al. Development and evaluation of a next-generation digital PCR diagnostic assay for ocular Chlamydia trachomatis infections. J. Clin. Microbiol. 51, 2195–2203 (2013).
World Health Organization Strategic and Technical Advisory Group for Neglected Tropical Diseases. Trachoma Alternative Indicators Study Data review, 31 August - 1 September 2016, Geneva, Switzerland WHO/HTM/NTD/PCT/2017.10 (World Health Organization, 2017).
Ramadhani, A. M., Derrick, T., Macleod, D., Holland, M. J. & Burton, M. J. The relationship between active trachoma and ocular chlamydia trachomatis infection before and after mass antibiotic treatment. PLoS Negl. Trop. Dis. 10, e0005080 (2016).
Butcher, R. M. et al. Low prevalence of conjunctival infection with chlamydia trachomatis in a treatment-naive trachoma-endemic region of the Solomon Islands. PLoS Negl. Trop. Dis. 10, e0004863 (2016).
Macleod, C. K. et al. Low prevalence of ocular chlamydia trachomatis infection and active trachoma in the western division of Fiji. PLoS Negl. Trop. Dis. 10, e0004798 (2016).
Butcher, R. et al. Clinical signs of trachoma are prevalent among Solomon Islanders who have no persistent markers of prior infection with Chlamydia trachomatis. Wellcome Open. Res. 3, 14 (2018).
Butcher, R. et al. Ocular Chlamydia trachomatis infection, anti-Pgp3 antibodies and conjunctival scarring in Vanuatu and Tarawa, Kiribati before antibiotic treatment for trachoma. J. Infect. 80, 454–461 (2020).
Macleod, C. K. et al. Trachoma, anti-Pgp3 serology and ocular Chlamydia trachomatis infection in Papua New Guinea. Clin. Infect. Dis. 72, 423–430 (2021).
Nesemann, J. M. et al. Comparison of smartphone photography, single-lens reflex photography, and field-grading for trachoma. Am. J. Trop. Med. Hyg. https://doi.org/10.4269/ajtmh.20-0386 (2020).
Snyder, B. M. et al. Smartphone photography as a possible method of post-validation trachoma surveillance in resource-limited settings. Int. Health 11, 613–615 (2019).
Kosack, C. S., Page, A. L. & Klatser, P. R. A guide to aid the selection of diagnostic tests. Bull. World Health Organ. 95, 639–645 (2017).
Michel, C. E. et al. Field evaluation of a rapid point-of-care assay for targeting antibiotic treatment for trachoma control: a comparative study. Lancet 367, 1585–1590 (2006).
Harding-Esch, E. M. et al. Diagnostic accuracy of a prototype point-of-care test for ocular Chlamydia trachomatis under field conditions in The Gambia and Senegal. PLoS Negl. Trop. Dis. 5, e1234 (2011).
Derrick, T. R. et al. DjinniChip: evaluation of a novel molecular rapid diagnostic device for the detection of Chlamydia trachomatis in trachoma-endemic areas. Parasit. Vectors 13, 533 (2020).
Martin, D. L. et al. The use of serology for trachoma surveillance: current status and priorities for future investigation. PLoS Negl. Trop. Dis. 14, e0008316 (2020). Reviews the use of serology as a future programmatic tool for trachoma surveillance.
Poston, T. B., Gottlieb, S. L. & Darville, T. Status of vaccine research and development of vaccines for Chlamydia trachomatis infection. Vaccine 37, 7289–7294 (2017).
Abraham, S. et al. Safety and immunogenicity of the chlamydia vaccine candidate CTH522 adjuvanted with CAF01 liposomes or aluminium hydroxide: a first-in-human, randomised, double-blind, placebo-controlled, phase 1 trial. Lancet Infect. Dis. 19, 1091–1100 (2019).
Francis, V. & Turner, V. Achieving Community Support for Trachoma Control WHO/PBL/93.36 (World Health Organization, 1993).
Addiss, D. G. Global elimination of lymphatic filariasis: a “mass uprising of compassion”. PLoS Negl. Trop. Dis. 7, e2264 (2013).
Burton, M., Habtamu, E., Ho, D. & Gower, E. W. Interventions for trachoma trichiasis. Cochrane Database Syst. Rev. 2015, CD004008 (2015).
Merbs, S. et al. Trichiasis Surgery for Trachoma 2nd edn (World Health Organization, 2015).
Gower, E. W. et al. Definitions and standardization of a new grading scheme for eyelid contour abnormalities after trichiasis surgery. PLoS Negl. Trop. Dis. 6, e1713 (2012).
Mwangi, G., Courtright, P. & Solomon, A. W. Systematic review of the incidence of post-operative trichiasis in Africa. BMC Ophthalmol. 20, 451 (2020).
Habtamu, E. et al. Predictors of trachomatous trichiasis surgery outcome. Ophthalmology https://doi.org/10.1016/j.ophtha.2017.03.016 (2017).
Alemayehu, W. et al. Surgery for trichiasis by ophthalmologists versus integrated eye care workers: a randomized trial. Ophthalmology 111, 578–584 (2004). Randomized trial demonstrating that ophthalmologists and integrated eye care workers trained as TT surgeons generate similar outcomes for patients with TT, enabling expanded access to surgery in trachoma-endemic areas.
Habtamu, E. et al. Posterior versus bilamellar tarsal rotation surgery for trachomatous trichiasis in Ethiopia: a randomised controlled trial. Lancet Glob. Health 4, e175–e184 (2016). Randomized controlled, single-masked clinical trial demonstrating a reduced cumulative incidence of recurrent trichiasis at 12 months in patients randomized to posterior lamellar tarsal rotation than those randomized to bilamellar tarsal rotation.
Habtamu, E. et al. Posterior lamellar versus bilamellar tarsal rotation surgery for trachomatous trichiasis: long-term outcomes from a randomised controlled trial. EClinicalMedicine 17, 100202 (2019).
Bayissasse, B. et al. Maximising trichiasis surgery success (MTSS) trial: rationale and design of a randomised controlled trial to improve trachomatous trichiasis surgical outcomes. BMJ Open 10, e036327 (2020).
Solomon, A. W. Optimising the management of trachomatous trichiasis. Lancet Glob. Health 4, e140–e141 (2016).
Rajak, S. N. et al. Absorbable versus silk sutures for surgical treatment of trachomatous trichiasis in Ethiopia: a randomised controlled trial. PLoS Med. 8, e1001137 (2011).
Gower, E. W. et al. Trachomatous trichiasis clamp vs standard bilamellar tarsal rotation instrumentation for trichiasis surgery: results of a randomized clinical trial. JAMA Ophthalmol. 131, 294–301 (2013).
West, S. K. et al. Single-dose azithromycin prevents trichiasis recurrence following surgery: randomized trial in Ethiopia. Arch. Ophthalmol. 124, 309–314 (2006).
Burton, M. J. et al. A randomised controlled trial of azithromycin following surgery for trachomatous trichiasis in the Gambia. Br. J. Ophthalmol. 89, 1282–1288 (2005).
Habtamu, E. et al. Oral doxycycline for the prevention of postoperative trachomatous trichiasis in Ethiopia: a randomised, double-blind, placebo-controlled trial. Lancet Glob. Health 6, e579–e592 (2018).
Rajak, S. N. et al. The outcome of trachomatous trichiasis surgery in Ethiopia: risk factors for recurrence. PLoS Negl. Trop. Dis. 7, e2392 (2013).
Gower, E. W. et al. Pre-operative trichiatic eyelash pattern predicts post-operative trachomatous trichiasis. PLoS Negl. Trop. Dis. 13, e0007637 (2019).
Kreis, A. J. et al. Challenges in addressing post-operative trachomatous trichiasis. Eye 34, 2131–2132 (2020).
Gupta, K. M., Harding, J. C., Othman, M. S., Merbs, S. L. & Gower, E. W. Why do patients refuse trichiasis surgery? Lessons and an education initiative from Mtwara Region, Tanzania. PLoS Negl. Trop. Dis. 12, e0006464 (2018).
Bickley, R. J., Mkocha, H., Munoz, B. & West, S. Identifying patient perceived barriers to trichiasis surgery in Kongwa District, Tanzania. PLoS Negl. Trop. Dis. 11, e0005211 (2017).
Lewallen, S., Mahande, M., Tharaney, M., Katala, S. & Courtright, P. Surgery for trachomatous trichiasis: findings from a survey of trichiasis surgeons in Tanzania. Br. J. Ophthalmol. 91, 143–145 (2007).
West, E. S. et al. The association between epilation and corneal opacity among eyes with trachomatous trichiasis. Br. J. Ophthalmol. 90, 171–174 (2006).
Rajak, S. N. et al. Epilation for trachomatous trichiasis and the risk of corneal opacification. Ophthalmology 119, 84–89 (2012).
Habtamu, E. et al. Epilation for minor trachomatous trichiasis: four-year results of a randomised controlled trial. PLoS Negl. Trop. Dis. 9, e0003558 (2015).
Habtamu, E. et al. Effect of repeated epilation for minor trachomatous trichiasis on lash burden, phenotype and surgical management willingness: a cohort study. PLoS Negl. Trop. Dis. 14, e0008882 (2020).
Woreta, T. A., Munoz, B. E., Gower, E. W., Alemayehu, W. & West, S. K. Effect of trichiasis surgery on visual acuity outcomes in Ethiopia. Arch. Ophthalmol. 127, 1505–1510 (2009).
Oktavec, K. C. et al. Patients’ perceptions of trichiasis surgery: results from the Partnership for Rapid Elimination of Trachoma (PRET) surgery clinical trial. Ophthalmic Epidemiol. 22, 153–161 (2015).
Habtamu, E. et al. Impact of trichiasis surgery on quality of life: a longitudinal study in ethiopia. PLoS Negl. Trop. Dis. 10, e0004627 (2016).
Woreta, F., Munoz, B., Gower, E., Alemayehu, W. & West, S. K. Three-year outcomes of the surgery for trichiasis, antibiotics to prevent recurrence trial. Arch. Ophthalmol. 130, 427–431 (2012).
Evans, J. R. et al. Antibiotics for trachoma. Cochrane Database Syst. Rev. 2019, CD001860 (2019).
Bailey, R. L., Arullendran, P., Whittle, H. C. & Mabey, D. C. Randomised controlled trial of single-dose azithromycin in treatment of trachoma. Lancet 342, 453–456 (1993).
Bowman, R. J. et al. Operational comparison of single-dose azithromycin and topical tetracycline for trachoma. Invest. Ophthalmol. Vis. Sci. 41, 4074–4079 (2000).
Solomon, A. W. et al. Two doses of azithromycin to eliminate trachoma in a Tanzanian community. N. Engl. J. Med. 358, 1870–1871 (2008).
Burton, M. J. et al. Profound and sustained reduction in Chlamydia trachomatis in The Gambia: a five-year longitudinal study of trachoma endemic communities. PLoS Negl. Trop. Dis. 4, e835 (2010).
Chidambaram, J. D. et al. Effect of a single mass antibiotic distribution on the prevalence of infectious trachoma. JAMA 295, 1142–1146 (2006).
Lietman, T., Porco, T., Dawson, C. & Blower, S. Global elimination of trachoma: how frequently should we administer mass chemotherapy? Nat. Med. 5, 572–576 (1999). Mathematical model suggesting that, where <35% of children have active trachoma, annual antibiotic MDA may be sufficient to eliminate trachoma, while biannual MDA may be needed where >50% of children have active trachoma.
Emerson, P. M., Hooper, P. J. & Sarah, V. Progress and projections in the program to eliminate trachoma. PLoS Negl. Trop. Dis. 11, e0005402 (2017).
International Trachoma Initiative. Zithromax Management Guide 2019: How to Successfully Apply for, Administer and Manage the Zithromax Donation for Trachoma Elimination (International Trachoma Initiative, 2019).
Munoz, B. et al. Antibiotic dosage in trachoma control programs: height as a surrogate for weight in children. Invest. Ophthalmol. Vis. Sci. 44, 1464–1469 (2003).
Ayele, B. et al. Adverse events after mass azithromycin treatments for trachoma in Ethiopia. Am. J. Trop. Med. Hyg. 85, 291–294 (2011).
World Health Organization. Ending the Neglect to Attain the Sustainable Development Goals: A Global Strategy on Water, Sanitation and Hygiene to Combat Neglected Tropical Diseases 2021–2030 (World Health Organization, 2021).
Oldenburg, C. E. et al. Safety of azithromycin in infants under six months of age in Niger: a community randomized trial. PLoS Negl. Trop. Dis. 12, e0006950 (2018).
Keenan, J. D. et al. Azithromycin to reduce childhood mortality in sub-Saharan Africa. N. Engl. J. Med. 378, 1583–1592 (2018). Cluster randomized, placebo-controlled trial that showed a 13.5% reduction in all-cause mortality in children aged 1–59 months living in communities receiving biannual azithromycin MDA compared with those receiving placebo MDA.
Porco, T. C. et al. Effect of mass distribution of azithromycin for trachoma control on overall mortality in Ethiopian children: a randomized trial. JAMA 302, 962–968 (2009).
Oldenburg, C. E. et al. Mass azithromycin distribution to prevent childhood mortality: a pooled analysis of cluster-randomized trials. Am. J. Trop. Med. Hyg. https://doi.org/10.4269/ajtmh.18-0846 (2019).
Fry, A. M. et al. Adverse and beneficial secondary effects of mass treatment with azithromycin to eliminate blindness due to trachoma in Nepal. Clin. Infect. Dis. 35, 395–402 (2002).
Coles, C. L. et al. Association of mass treatment with azithromycin in trachoma-endemic communities with short-term reduced risk of diarrhea in young children. Am. J. Trop. Med. Hyg. 85, 691–696 (2011).
Schachterle, S. E. et al. Short-term malaria reduction by single-dose azithromycin during mass drug administration for trachoma, Tanzania. Emerg. Infect. Dis. 20, 941–949 (2014).
Hinterwirth, A. et al. Rapid reduction of Campylobacter species in the gut microbiome of preschool children after oral azithromycin: a randomized controlled trial. Am. J. Trop. Med. Hyg. 103, 1266–1269 (2020).
Ghinai, R. et al. A cross-sectional study of ‘yaws’ in districts of Ghana which have previously undertaken azithromycin mass drug administration for trachoma control. PLoS Negl. Trop. Dis. 9, e0003496 (2015).
Marks, M. et al. Prevalence of active and latent yaws in the Solomon Islands 18 months after azithromycin mass drug administration for trachoma. PLoS Negl. Trop. Dis. 10, e0004927 (2016).
Marks, M. et al. Impact of community mass treatment with azithromycin for trachoma elimination on the prevalence of yaws. PLoS Negl. Trop. Dis. 9, e0003988 (2015).
Solomon, A. W. et al. Trachoma and yaws: common ground? PLoS Negl. Trop. Dis. 9, e0004071 (2015).
Ray, W. A., Murray, K. T., Hall, K., Arbogast, P. G. & Stein, C. M. Azithromycin and the risk of cardiovascular death. N. Engl. J. Med. 366, 1881–1890 (2012).
Keenan, J. D., Emerson, P. M., Gaynor, B. D., Porco, T. C. & Lietman, T. M. Adult mortality in a randomized trial of mass azithromycin for trachoma. JAMA Intern. Med. 173, 821–823 (2013).
Solomon, A. W. et al. Impact of mass distribution of azithromycin on the antibiotic susceptibilities of ocular Chlamydia trachomatis. Antimicrob. Agents Chemother. 49, 4804–4806 (2005).
Hong, K. C. et al. Lack of macrolide resistance in Chlamydia trachomatis after mass azithromycin distributions for trachoma. Emerg. Infect. Dis. 15, 1088–1090 (2009).
West, S. K. et al. Is there evidence for resistance of ocular Chlamydia trachomatis to azithromycin after mass treatment for trachoma control? J. Infect. Dis. 210, 65–71 (2014).
O’Brien, K. S. et al. Antimicrobial resistance following mass azithromycin distribution for trachoma: a systematic review. Lancet Infect. Dis. 19, e14–e25 (2019). Systematic review of antimicrobial resistance associated with azithromycin MDA, demonstrating selection of resistance in some potentially pathogenic bystander organisms but no evidence of resistance in conjunctival Ct.
Skalet, A. H. et al. Antibiotic selection pressure and macrolide resistance in nasopharyngeal Streptococcus pneumoniae: a cluster-randomized clinical trial. PLoS Med. 7, e1000377 (2010).
Haug, S. et al. The decline of pneumococcal resistance after cessation of mass antibiotic distributions for trachoma. Clin. Infect. Dis. 51, 571–574 (2010).
Seidman, J. C. et al. Increased carriage of macrolide-resistant fecal E. coli following mass distribution of azithromycin for trachoma control. Int. J. Epidemiol. 43, 1105–1113 (2014).
Bloch, E. M. et al. Antibiotic resistance in young children in Kilosa district, Tanzania 4 years after mass distribution of azithromycin for trachoma control. Am. J. Trop. Med. Hyg. 97, 815–818 (2017).
Seidman, J. C. et al. Longitudinal comparison of antibiotic resistance in diarrheagenic and non-pathogenic Escherichia coli from young Tanzanian children. Front. Microbiol. 7, 1420 (2016).
Bojang, A. et al. Prevalence and risk factors for Staphylococcus aureus nasopharyngeal carriage during a PCV trial. BMC Infect. Dis. 17, 588 (2017).
Ministry of Health and Medical Education. Elimination of Trachoma, Iran (Ministry of Health and Medical Education, 2018).
West, S. et al. Impact of face-washing on trachoma in Kongwa, Tanzania. Lancet 345, 155–158 (1995).
Aragie, S. et al. Water, sanitation, and hygiene for control of trachoma in Ethiopia (WUHA): a two-arm, parallel-group, cluster-randomised trial. Lancet Glob. Health 10, e87–e95 (2022).
Delea, M. G., Solomon, H., Solomon, A. W. & Freeman, M. C. Interventions to maximize facial cleanliness and achieve environmental improvement for trachoma elimination: a review of the grey literature. PLoS Negl. Trop. Dis. 12, e0006178 (2018).
Chen, X., Munoz, B., Mkocha, H., Wolle, M. A. & West, S. K. Children as messengers of health knowledge? Impact of health promotion and water infrastructure in schools on facial cleanliness and trachoma in the community. PLoS Negl. Trop. Dis. 15, e0009119 (2021).
Dodson, S. et al. Behavioural change interventions for sustained trachoma elimination. Bull. World Health Organ. 96, 723–725 (2018).
Emerson, P. M. et al. Role of flies and provision of latrines in trachoma control: cluster-randomised controlled trial. Lancet 363, 1093–1098 (2004).
Stoller, N. E. et al. Efficacy of latrine promotion on emergence of infection with ocular Chlamydia trachomatis after mass antibiotic treatment: a cluster-randomized trial. Int. Health 3, 75–84 (2011).
Rabiu, M., Alhassan, M. B., Ejere, H. O. & Evans, J. R. Environmental sanitary interventions for preventing active trachoma. Cochrane Database Syst. Rev. 2012, CD004003 (2012).
Ejere, H. O., Alhassan, M. B. & Rabiu, M. Face washing promotion for preventing active trachoma. Cochrane Database Syst. Rev. 2015, CD003659 (2015).
Boisson, S. et al. Water, sanitation and hygiene for accelerating and sustaining progress on neglected tropical diseases: a new Global Strategy 2015-20. Int. Health 8, i19–i21 (2016).
Blodi, B. A., Byrne, K. A. & Tabbara, K. F. Goblet cell population among patients with inactive trachoma. Int. Ophthalmol. 12, 41–45 (1988).
Guzey, M., Satici, A. & Karadede, S. Corneal thickness in trachomatous dry eye. Eur. J. Ophthalmol. 12, 18–23 (2002).
Tabbara, K. F. & Bobb, A. A. Lacrimal system complications in trachoma. Ophthalmology 87, 298–301 (1980).
Juri Mandić, J. et al. Quality of life and depression level in patients with watery eye. Psychiatr. Danubina 30, 471–477 (2018).
Uchino, M. & Schaumberg, D. A. Dry eye disease: impact on quality of life and vision. Curr. Ophthalmol. Rep. 1, 51–57 (2013).
World Health Organization. WHO Alliance for the Global Elimination of Trachoma by 2020: progress report, 2019. Wkly Epidemiol. Rec. 30, 349–360 (2020).
World Health Organization. WHO Validates Saudi Arabia for Eliminating Trachoma as a Public Health Problem (World Health Organization, 2022).
World Health Organization. Future Approaches to Trachoma Control: Report of a Global Scientific Meeting, Geneva, 17–20 June 1996 WHO/PBL/96.56 (World Health Organization, 1997).
Dowdle, W. R. The principles of disease elimination and eradication. Bull. World Health Organ. 76, 22–25 (1998).
Oldenburg, C. E. et al. Can we eradicate trachoma? A survey of stakeholders. Br. J. Ophthalmol. 105, 1059–1062 (2020).
Gebre, T. Rethinking disease eradication: putting countries first. Int. Health 13, 215–221 (2021).
Pinsent, A. et al. The utility of serology for elimination surveillance of trachoma. Nat. Commun. 9, 5444 (2018).
Kim, J. S. et al. Community-level chlamydial serology for assessing trachoma elimination in trachoma-endemic Niger. PLoS Negl. Trop. Dis. 13, e0007127 (2019).
Senyonjo, L. G. et al. Serological and PCR-based markers of ocular Chlamydia trachomatis transmission in northern Ghana after elimination of trachoma as a public health problem. PLoS Negl. Trop. Dis. 12, e0007027 (2018).
Amoah, B. et al. Model-based geostatistics enables more precise estimates of neglected tropical-disease prevalence in elimination settings: mapping trachoma prevalence in Ethiopia. Int. J. Epidemiol. https://doi.org/10.1093/ije/dyab227 (2021).
US National Library of Medicine. ClinicalTrials.gov https://clinicaltrials.gov/ct2/show/NCT03886519 (2022).
Merbs, S. L. et al. A new surgical technique for postoperative trachomatous trichiasis. Ophthalmic Plast. Reconstr. Surg. https://doi.org/10.1097/iop.0000000000002055 (2021).
Rajak, S. N., Collin, J. R. & Burton, M. J. Trachomatous trichiasis and its management in endemic countries. Surv. Ophthalmol. 57, 105–135 (2012).
Kim, M. C. et al. Sensitivity and specificity of computer vision classification of eyelid photographs for programmatic trachoma assessment. PLoS ONE 14, e0210463 (2019).
Burton, M. J. et al. The Lancet global health commission on global eye health: vision beyond 2020. Lancet Glob. Health 9, e489–e551 (2021).
Nash, S. D. et al. Ocular chlamydia trachomatis infection under the surgery, antibiotics, facial cleanliness, and environmental improvement strategy in Amhara, Ethiopia, 2011–2015. Clin. Infect. Dis. 67, 1840–1846 (2018). Epidemiology of ocular Ct in the presence of ongoing implementation of the SAFE strategy in a population with persistently hyperendemic trachoma.
Gebre, T. et al. Comparison of annual versus twice-yearly mass azithromycin treatment for hyperendemic trachoma in Ethiopia: a cluster-randomised trial. Lancet 379, 143–151 (2012). Community randomized trial that failed to find evidence of a difference between the effects of biannual and annual azithromycin MDA in a population hyperendemic for trachoma.
Amza, A. et al. Effectiveness of expanding annual mass azithromycin distribution treatment coverage for trachoma in Niger: a cluster randomised trial. Br. J. Ophthalmol. 102, 680–686 (2017).
Melese, M. et al. Comparison of annual and biannual mass antibiotic administration for elimination of infectious trachoma. JAMA 299, 778–784 (2008).
Oldenburg, C. E. et al. Comparison of mass azithromycin coverage targets of children in Niger: a cluster-randomized trachoma trial. Am. J. Trop. Med. Hyg. https://doi.org/10.4269/ajtmh.17-0501 (2017).
Melo, J. S. et al. Targeted antibiotics for trachoma: a cluster-randomized trial. Clin. Infect. Dis. https://doi.org/10.1093/cid/ciab193 (2021).
Lietman, T. M. et al. Frequency of mass azithromycin distribution for ocular chlamydia in a trachoma endemic region of Ethiopia: a cluster randomized trial. Am. J. Ophthalmol. 214, 143–150 (2020).
House, J. I. et al. Assessment of herd protection against trachoma due to repeated mass antibiotic distributions: a cluster-randomised trial. Lancet 373, 1111–1118 (2009).
Lietman, T. M. et al. Identifying a sufficient core group for trachoma transmission. PLoS Negl. Trop. Dis. 12, e0006478 (2018).
Wilson, N. et al. Evaluation of a single dose of azithromycin for trachoma in low-prevalence communities. Ophthalmic Epidemiol. 26, 1–6 (2019).
Amza, A. et al. Azithromycin Reduction to Reach Elimination of Trachoma (ARRET): study protocol for a cluster randomized trial of stopping mass azithromycin distribution for trachoma. BMC Ophthalmol. 21, 15 (2021).
Harding-Esch, E. M. et al. Mass treatment with azithromycin for trachoma: when is one round enough? Results from the PRET Trial in the Gambia. PLoS Negl. Trop. Dis. 7, e2115 (2013).
King, J. D. et al. Randomised trial of face-washing to develop a standard definition of a clean face for monitoring trachoma control programmes. Trans. R. Soc. Trop. Med. Hyg. 105, 7–16 (2011).
Delea, M. G. et al. Development and reliability of a quantitative personal hygiene assessment tool. Int. J. Hyg. Env. Health 227, 113521 (2020).
Harding-Esch, E. M. et al. Facial cleanliness indicators by time of day: results of a cross-sectional trachoma prevalence survey in Senegal. Parasit. Vectors 13, 556 (2020).
Wittberg, D. M. et al. WASH Upgrades for Health in Amhara (WUHA): study protocol for a cluster-randomised trial in Ethiopia. BMJ Open 11, e039529 (2021).
Budge, S., Ambelu, A., Bartram, J., Brown, J. & Hutchings, P. Environmental sanitation and the evolution of water, sanitation and hygiene. Bull. World Health Organ. 100, 286–288 (2022).
Czerniewska, A. et al. Comparison of face washing and face wiping methods for trachoma control: a pilot study. Am. J. Trop. Med. Hyg. 102, 740–743 (2020).
Mwangi, G., Courtright, P. & Solomon, A. W. National approaches to trichiasis surgical follow-up, outcome assessment and surgeon audit in trachoma-endemic countries in Africa. Br. J. Ophthalmol. https://doi.org/10.1136/bjophthalmol-2019-315777 (2020).
Djore, D. et al. Pilot audit of trichiasis surgery outcomes using a mobile app in the republic of Chad. Middle East. Afr. J. Ophthalmol. 27, 14–21 (2020).
Butcher, R. et al. Conjunctival scarring, corneal pannus and Herbert’s pits in adolescent children in trachoma-endemic populations of the Solomon Islands and Vanuatu. Clin. Infect. Dis. https://doi.org/10.1093/cid/ciaa1151 (2020).
The Lancet Global Health. Unlocking human potential with universal eye health. Lancet Glob. Health 9, e372 (2021).
Borlase, A. et al. Modelling trachoma post-2020: opportunities for mitigating the impact of COVID-19 and accelerating progress towards elimination. Trans. R. Soc. Trop. Med. Hyg. 115, 213–221 (2021).
Blumberg, S. et al. Implications of the COVID-19 pandemic in eliminating trachoma as a public health problem. Trans. R. Soc. Trop. Med. Hyg. 115, 222–228 (2021).
Harding-Esch, E. M. et al. Lessons from the field: integrated survey methodologies for neglected tropical diseases. Trans. R. Soc. Trop. Med. Hyg. 115, 124–126 (2021).
Morice, A., Taleo, F., Barogui, Y., A, C. S. & Marks, M. Lessons from the field: integrated programmes for neglected tropical diseases. Trans. R. Soc. Trop. Med. Hyg. 115, 127–128 (2021).
Boisson, S. et al. Building on a decade of progress in water, sanitation and hygiene to control, eliminate and eradicate neglected tropical diseases. Trans. R. Soc. Trop. Med. Hyg. 115, 185–187 (2021).
Laing, G. et al. One Health for neglected tropical diseases. Trans. R. Soc. Trop. Med. Hyg. 115, 182–184 (2021).
World Health Organization. Report of the 3rd Global Scientific Meeting on Trachoma, Johns Hopkins University WHO/PBD/2.10 (World Health Organization, 2010).
Hoffman, J. J. et al. 3D images as a field grader training tool for trachomatous trichiasis: a diagnostic accuracy study in Ethiopia. PLoS Negl. Trop. Dis. 13, e0007104 (2019).
Courtright, P., Flueckiger, R., Harding-Esch, E. M., Lewallen, S. & Solomon, A. W. Tropical Data: Training System for Trachomatous Trichiasis Population-Based Prevalence Surveys (version 2) (International Coalition for Trachoma Control, 2019).
World Health Organization. Status of elimination of trachoma as a public health problem, 2021. WHO https://www.who.int/images/default-source/maps/trachoma_2021_status.png?sfvrsn=91211dd5_3 (2021).
Solomon, A. W. & Mabey, D. C. W. in International Encyclopaedia of Public Health (2nd ed) (ed Quah, S.) (Elsevier, 2016).
Chandra, N. L. et al. Detection of Chlamydia trachomatis in rectal specimens in women and its association with anal intercourse: a systematic review and meta-analysis. Sex. Transm. Infect. 94, 320–326 (2018).
Howe, S. E., Shillova, N. & Konjufca, V. Dissemination of Chlamydia from the reproductive tract to the gastro-intestinal tract occurs in stages and relies on Chlamydia transport by host cells. PLoS Pathog. 15, e1008207 (2019).
Acknowledgements
A.W.S. is a staff member of the World Health Organization. M.J.B. is supported by the Wellcome Trust (207472/Z/17/Z). E.W.G. is supported by the National Eye Institute (UG1EY025992). E.M.H.-E. is Chief Scientist to Tropical Data; she receives salary support from the International Trachoma Initiative. Additional core Tropical Data funding is provided by the International Trachoma Initiative, Sightsavers and RTI International through the United States Agency for International Development (USAID) Act to End NTDs | East program. C.E.O. is supported by a Research to Prevent Blindness Career Development Award and the National Eye Institute (UG1EY028088 and UG1EY030833). None of our funders had any role in the conception, design or interpretation of data in this Review, in decisions on where, how or when to publish in the peer-reviewed press, or in preparation of the manuscript.
Author information
Authors and Affiliations
Contributions
Introduction (C.E.O.); Epidemiology (E.M.H.-E.); Mechanisms/pathophysiology (M.J.B. and H.R.T.); Diagnosis, screening and prevention (A.W.S. and L.T.); Management (E.W.G.); Quality of life (E.W.G.); Outlook (C.E.O.); Overview of Primer (A.W.S.).
Corresponding author
Ethics declarations
Competing interests
E.M.H.-E. receives salary support from the International Trachoma Initiative, which receives an operating budget and research funds from Pfizer Inc., the manufacturer of Zithromax (azithromycin). M.J.B. and C.E.O. each lead research programmes on trachoma that have received donated azithromycin (and, for C.E.O., placebo) for research studies from the International Trachoma Initiative/Pfizer Inc. A.W.S. is a staff member of the World Health Organization. All other authors declare no competing interests.
Peer review
Peer review information
Nature Reviews Disease Primers thanks T. Gebre, M. Hammerschalg and the other, anonymous, reviewer(s) for their contribution to the peer review of this work.
Additional information
We dedicate this article to the memory of Professor Julius Schachter, pioneering chlamydiologist, colleague, collaborator, mentor, teacher, friend; sadly lost to COVID-19 in December 2020. The world wouldn’t have made it this far against trachoma without you, Julie.
Disclaimer
A.W.S. is a staff member of the World Health Organization. The authors alone are responsible for the views expressed in this article and they do not necessarily represent the views, decisions or policies of the institutions with which they are affiliated.
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Related links
International Trachoma Initiative: https://www.trachoma.org/
Trachoma Atlas: https://atlas.trachomadata.org/
WHO Global Health Observatory: https://apps.who.int/gho/data/node.main.A1644?lang=en
Rights and permissions
About this article

Cite this article
Solomon, A.W., Burton, M.J., Gower, E.W. et al. Trachoma. Nat Rev Dis Primers 8, 32 (2022). https://doi.org/10.1038/s41572-022-00359-5
Accepted:
Published:
DOI: https://doi.org/10.1038/s41572-022-00359-5

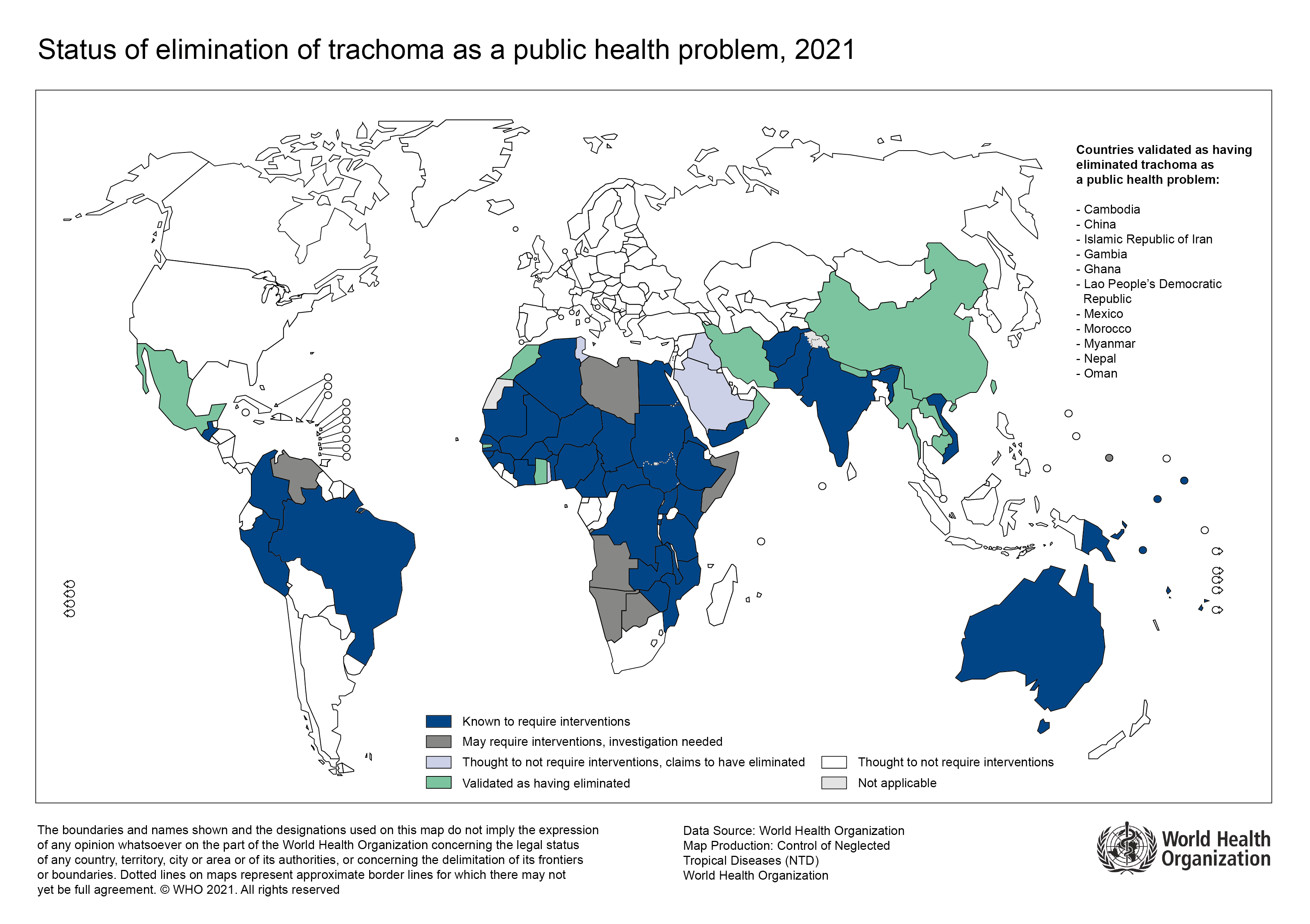{kind=link}