
Abstract
Conventional dual antiplatelet therapy (DAPT) for patients with acute coronary syndromes undergoing percutaneous coronary intervention comprises aspirin with a potent P2Y purinoceptor 12 (P2Y12) inhibitor (prasugrel or ticagrelor) for 12 months. Although this approach reduces ischaemic risk, patients are exposed to a substantial risk of bleeding. Strategies to reduce bleeding include de-escalation of DAPT intensity (downgrading from potent P2Y12 inhibitor at conventional doses to either clopidogrel or reduced-dose prasugrel) or abbreviation of DAPT duration. Either strategy requires assessment of the ischaemic and bleeding risks of each individual. De-escalation of DAPT intensity can reduce bleeding without increasing ischaemic events and can be guided by platelet function testing or genotyping. Abbreviation of DAPT duration after 1–6 months, followed by monotherapy with aspirin or a P2Y12 inhibitor, reduces bleeding without an increase in ischaemic events in patients at high bleeding risk, particularly those without high ischaemic risk. However, these two strategies have not yet been compared in a head-to-head clinical trial. In this Consensus Statement, we summarize the evidence base for these treatment approaches, provide guidance on the assessment of ischaemic and bleeding risks, and provide consensus statements from an international panel of experts to help clinicians to optimize these DAPT approaches for individual patients to improve outcomes.
Similar content being viewed by others


Introduction
Antiplatelet therapy is central to the management of acute coronary syndromes (ACS) in patients undergoing percutaneous coronary intervention (PCI). The current ‘standard-of-care’ dual antiplatelet therapy (DAPT) for patients with ACS undergoing PCI, according to international guidelines, comprises aspirin combined with a potent P2Y purinoceptor 12 (P2Y12) inhibitor, namely prasugrel or ticagrelor1,2,3,4,5,6. Although DAPT reduces the risk of ischaemic events after ACS, it substantially increases the risk of bleeding7,8. Increased awareness of the prognostic importance of bleeding has prompted the investigation of strategies to de-escalate DAPT and identify a strategy balancing thrombotic and bleeding risks.
The existing European and North American guidelines on the management of ST-segment elevation myocardial infarction (STEMI)2,4, non-ST-segment elevation ACS1,5 and PCI3,6 only loosely cover options for antithrombotic therapy. To date, no position documents or guidelines have been published that summarize the available options for abbreviation or de-escalation of DAPT nor the evidence base supporting the various strategies. Therefore, we convened an international panel of experts to produce a Consensus Statement to guide clinicians when identifying patients who are suitable for abbreviation or de-escalation of DAPT and to improve clinical outcomes by maintaining efficacy while reducing bleeding.
In this Consensus Statement, we refer to shortening of DAPT duration (also known as abbreviation of DAPT), in which DAPT is curtailed before the standard 12 months and treatment is continued with a single antiplatelet agent, either aspirin or a P2Y12 inhibitor (clopidogrel, prasugrel or ticagrelor), and to de-escalation of DAPT intensity, in which treatment is switched from conventional doses of the more potent P2Y12 inhibitors (prasugrel or ticagrelor) to either clopidogrel or reduced-dose prasugrel. We summarize the evidence base for these two approaches to treatment, provide guidance on the assessment of ischaemic and bleeding risks, and make recommendations to help clinicians to optimize these approaches to DAPT for individual patients (Box 1). We also identify current gaps in the evidence, which represent areas for future research (Box 2). Our recommendations do not apply to patients who require oral anticoagulation after ACS because they represent a very specific cohort for whom the evidence base for abbreviation or de-escalation of DAPT is not robust and different medications are required when these strategies are attempted.
Methods for consensus recommendations
We conducted a search of the literature to identify clinical trials of de-escalation of DAPT intensity or abbreviation of DAPT duration in patients with ACS treated with PCI. The PubMed, Embase and Cochrane Library databases were searched for papers published up to November 2022, with no restriction on language. Reference lists of selected papers were also checked for additional relevant papers. The authors worked on allocated sections of this Consensus Statement in pairs. All the authors reviewed all sections of the manuscript and participated in a series of ‘rounds’, in which the manuscript was shared with all other authors and the comments made were used to inform and evolve the manuscript in the next round. Video discussions between the authors were also conducted. All the authors judged the available evidence, leading to the consensus recommendations.
Risk of bleeding in clinical trials
In clinical trials of DAPT, the incidence of major bleeding in the 12 months after PCI among patients with ACS is 1–10% depending on the definition of ‘bleeding’, the type and dose of P2Y12 inhibitor used9,10,11, and the ethnicity and bleeding risk category of the patient12,13. In observational studies, the reported incidence of major bleeding is 2.8–11.0%11,14. Major bleeding in patients with ACS increases mortality by nearly threefold in the first 12 months after hospital discharge14 and increases the adjusted hazard ratio for death or myocardial infarction (MI) at 30 days by up to fivefold, with risk increasing in proportion to the severity of the bleeding15.
The risk of bleeding with DAPT relates not only to the combined effects of aspirin and the P2Y12 inhibitor on haemostasis but also to the potency of the P2Y12 inhibitor used (prasugrel and ticagrelor are more potent than clopidogrel). In a systematic review of 53 studies (36 observational studies and 17 randomized clinical trials; n = 714,458 patients with ACS) focusing on the period after discharge from hospital, the 12-month incidence of bleeding ranged from 0.2% to 37.5% in observational studies and from 0.96% to 39.4% in randomized trials, varying with the classification of bleeding used14. The risk of bleeding seems to be fairly consistent over time (despite being most common during the first month), whereas thrombotic risk is highest early after an ACS event14,16,17.
In clinical trials, bruising is the most commonly reported bleeding event, followed by gastrointestinal bleeding and epistaxis, whereas intracranial bleeding is relatively rare16. Nuisance bleeding (Bleeding Academic Research Consortium (BARC) type 1) is very common in the first year after ACS (up to 37.5%)18 and can lead to DAPT discontinuation, worsening quality of life, repeat hospitalization and an increased risk of subsequent serious bleeding18. In addition, the degree of platelet inhibition achieved by the P2Y12 inhibitor, as measured by platelet function testing (PFT), is directly related to the risk of mild bleeding (BARC type 1 or 2)19,20 and likelihood of DAPT discontinuation.
Clinical risk factors for bleeding
Older age (a continuum rather than a threshold age), previous bleeding and chronic kidney disease (CKD) are well-established risk factors for bleeding in patients with ACS undergoing PCI but other clinical factors also contribute (Table 1). Bleeding risk is usually based on the interaction between non-modifiable and modifiable risk factors. Multiple clinical scores have been developed to predict the risk of bleeding in patients receiving antiplatelet therapy7,21,22. The PRECISE-DAPT Risk Calculator was developed to predict the risk of bleeding in patients who undergo coronary stent implantation and receive subsequent DAPT7. The score includes five criteria (age, creatinine clearance, haemoglobin level, white blood cell count and previous spontaneous bleeding) and predicts the risk of out-of-hospital bleeding during DAPT.
In 2019, the Academic Research Consortium for High Bleeding Risk (ARC-HBR) developed a consensus definition of patients at high risk of bleeding focusing on those undergoing PCI23. Twenty clinical criteria were identified as major or minor, supported by published evidence. Patients were considered to be at high risk of bleeding (BARC type 3–5 bleeding, annual rate of ≥4%) if at least one major or two minor criteria were present.
Although the ARC-HBR criteria and the PRECISE-DAPT Risk Calculator can be adequately applied to real-world cohorts, several important clinical risk factors for bleeding are not covered by these scores (such as low body weight, frailty, heart failure and peripheral artery disease) and, therefore, risk of bleeding might be underestimated in these patients24.
Differences between antiplatelet agents
The differences in bleeding risk between the various oral P2Y12 inhibitors largely reflect the extent of platelet P2Y12 inhibition achieved. Approved regimens of prasugrel and ticagrelor achieve a higher mean level of platelet inhibition than clopidogrel25,26,27 and are associated with higher rates of minor and major bleeding9,10,28,29,30 (Table 2). Consistently high levels of P2Y12 inhibition with standard doses of prasugrel (10 mg daily) and ticagrelor (90 mg twice daily) translate to similar rates of bleeding for each agent29,31. However, the wide interindividual pharmacodynamic response to clopidogrel is associated with variation in individual bleeding risk, such that patients with greater P2Y12 inhibition have higher rates of bleeding31,32. The risk of bleeding related to surgery (either cardiac or non-cardiac) depends on the timing of P2Y12 inhibitor cessation before surgery, the mean level of platelet P2Y12 inhibition during treatment, and whether the inhibitory effect is reversible (ticagrelor) or irreversible (clopidogrel and prasugrel)33.
Aspirin, even at low daily maintenance doses of ≤100 mg, achieves consistently high levels of platelet cyclooxygenase 1 inhibition, resulting in a predictable compromise between haemostasis and increased bleeding risk with standard regimens34, either as monotherapy or as part of DAPT30 (Table 2). However, aspirin is associated with a dose-dependent increase in the risk of gastroduodenal erosion or ulceration, which increases the risk of gastrointestinal haemorrhage beyond the risk attributable to platelet inhibition35. Indeed, aspirin per se is not benign from the bleeding perspective; the risk of major and intracranial bleeding with aspirin is broadly similar to that of warfarin when stratified by the HAS-BLED score in patients with atrial fibrillation36. The assessment and mitigation of bleeding risk in patients with atrial fibrillation and venous thromboembolism and ethnic variation in bleeding risk associated with antithrombotic drugs have been the topic of consensus documents published in the past 2 years37,38.
Clinical risk factors for recurrent ischaemic events
Patients with ACS undergoing PCI are at risk of subsequent ischaemic events, with an incidence of nearly 5% in the first year after the index event, increasing to 15% by the fourth year39. The definition of high ischaemic risk has undergone several changes over time (Table 1), with the current definition based on the 2020 ESC guidelines for the management of ACS in patients presenting without persistent ST-segment elevation1. Clinical risk factors associated with recurrent ischaemic events include older age, frailty, diabetes mellitus, polyvascular disease, complex coronary artery disease and CKD40,41 (Table 1). Technical aspects of PCI that increase ischaemic risk include implantation of at least three stents, treatment of at least three lesions, total stent length >60 mm, bifurcation with two stents implanted, history of complex revascularization (such as left main stem or chronic total occlusion) and history of stent thrombosis with antiplatelet therapy1,42,43.
In patients with ACS undergoing PCI, definite or probable stent thrombosis occurs in 0.4–1.8% of patients in the first year44,45 and is more frequent than in patients with chronic coronary syndromes (CCS), especially in the first 6 months46. The major risk with premature discontinuation of DAPT is stent thrombosis, for which mortality is 20–45%47, being highest with acute (<24 h) and subacute (1–30 days) stent thrombosis. In a real-world registry of patients with non-ST-segment elevation ACS (patients with STEMI were excluded) receiving drug-eluting stents (DES), the incidence of stent thrombosis at 9 months was 1.3%, which is substantially higher than rates reported in major clinical trials (0.4–0.6%)48. Stent thrombosis occurred in 29% of patients who prematurely discontinued DAPT, with a case-fatality rate of 45%48. In another large registry, among patients with MI (either STEMI or non-STEMI) receiving DES, those who stopped thienopyridine therapy by 30 days had a ninefold increased risk of death over the next 11 months (7.5% versus 0.7%; P < 0.0001)49. In the PARIS registry46, among patients with ACS, the rate of stent thrombosis increased threefold after premature cessation of DAPT. Furthermore, in a subanalysis of the Dutch ST Registry50,51, the rate of stent thrombosis was threefold higher when clopidogrel was discontinued within the first month compared with discontinuation between 1 and 6 months. However, the findings of a systematic review and meta-analysis suggest that the increased risk of stent thrombosis with abbreviated DAPT might be attenuated with the use of second-generation DES compared with first-generation DES52.
Balancing ischaemic and bleeding risks
The principle of balancing ischaemic risk and bleeding risk is important when reducing the intensity or duration of DAPT. Bleeding risk can be assessed using the ARC-HBR criteria3 or the PRECISE-DAPT, CRUSADE or ACUITY risk scores53. However, PRECISE-DAPT is the only score validated for the selection of DAPT duration. The use of risk scores to assess bleeding risk is gaining popularity. However, risk scores for ischaemia and bleeding often have overlapping clinical features and depend on the same variables, particularly in elderly patients.
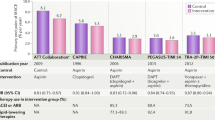
In a systematic review and meta-analysis of studies validating the DAPT score (88,563 patients undergoing PCI electively or for ACS), the DAPT score could be used to separate the risk of ischaemia from that of bleeding54. Patients with a DAPT score of ≥2 were at higher ischaemic risk and lower bleeding risk than patients with a DAPT score of <2, who were at higher bleeding risk and lower ischaemic risk. Therefore, application of the DAPT score could help to identify patients who might benefit from standard or prolonged DAPT. In 2022, a paper reporting on the long-term outcomes of patients enrolled in the PEGASUS-TIMI 54 trial indicated that a single factor defining increased ischaemic risk is insufficient to recommend prolonged DAPT55. The investigators concluded that two or more risk factors should be used to define patients who are truly at high ischaemic risk55. On the whole, patients with a high risk of bleeding do not derive a clear ischaemic benefit from prolonged DAPT; therefore, ischaemic risk should guide more prolonged DAPT regimens, mainly in patients without a high risk of bleeding12,56.
Timing of ischaemic risk versus bleeding risk
The incidence of ischaemic events is highest during the first month after PCI and tends to decrease thereafter57. In two large registries (BleeMACS and RENAMI; 19,826 unselected patients with ACS undergoing PCI), the ischaemic risk exceeded the bleeding risk in the first 2 weeks after PCI, especially in patients with STEMI and those with incomplete revascularization58. Thereafter, the risk of ischaemia was generally similar to the risk of bleeding up to 1 year58. Data from another registry (ADAPT-DES; 19,826 patients with ACS treated with PCI) also suggest that ischaemic risk is highest in the first 30 days, especially the first 2 weeks after ACS59. This acute increase in ischaemic risk could be stent-related (such as stent thrombosis) due to the progression or destabilization of non-culprit lesions (such as new MI) or vascular events in other areas affected by atherosclerotic disease (such as stroke)59.
By contrast, the risk of bleeding with DAPT, despite being relatively high in the first few days after PCI due to the use of an arterial access site and periprocedural antithrombotic therapy, does not diminish over time when antiplatelet therapy is continued42,57. Therefore, the net benefit of DAPT might diminish over time, depending on the clinical circumstances of the patient57. Hence, the rationale for de-escalation of DAPT in the setting of ACS lies in the concept that ischaemic risk clusters in the first months, whereas bleeding risk remains stable and might exceed ischaemic risk beyond the first few months after ACS.
Selection of patients for DAPT abbreviation or de-escalation
Multiple strategies that vary the intensity or duration of DAPT, or both, have been investigated in an effort to mitigate bleeding risk without a trade-off in ischaemic risk (Fig. 1). The decision to abbreviate or de-escalate DAPT depends on individual clinical judgement, driven by the perceived balance between the risks of ischaemia and bleeding, adverse events, comorbidities, co-medications, and the availability of the respective drugs.

ACS, acute coronary syndrome; DAPT, dual antiplatelet therapy; HBR, high bleeding risk; P2Y12, P2Y purinoceptor 12; RCT, randomized controlled trial; SAPT, single antiplatelet therapy. aPotent P2Y12 inhibitors are prasugrel or ticagrelor.
DAPT de-escalation can be tailored to the risk profile (which can be dynamic, requiring reassessment as circumstances change), PFT or genetics of a patient. Overall, many patients with ACS undergoing PCI, especially those at high risk of bleeding, could be suitable for de-escalation. Consensus-based criteria and statistical tools can assist in guiding clinical judgement and decision-making to implement this strategy. Both the ARC-HBR classification23 and the PRECISE-DAPT score (≥25) can help to identify patients at high risk of bleeding7,60; however, at least one additional risk factor should be considered if age is the only underlying factor used in the PRECISE-DAPT score.
De-escalation can be either unguided, based purely on clinical judgement, or based on clinical judgement and guided either by PFT or CYP2C19 genotyping, depending on the risk profile and availability of assays (ESC class IIb recommendation, level of evidence A)1. PFT allows direct determination of the degree of platelet inhibition, which can subsequently identify patients at increased thrombotic risk (high on-treatment platelet reactivity) or bleeding risk (low on-treatment platelet reactivity). This information can be used to inform the modulation of P2Y12 therapy to achieve the desired platelet response. The benefit of genetic testing over PFT is that the results remain unchanged, whereas the results of PFT are subject to intraindividual and interindividual variability. However, genetic data should be integrated with knowledge of clinical phenotypes that impair antithrombotic efficacy such as obesity, high BMI, diabetes and kidney dysfunction. Two meta-analyses published in the past year showed that either guided or unguided DAPT de-escalation were associated with a reduction in bleeding without an increase in ischaemic events61,62.
Clinical trial evidence for abbreviation of DAPT duration
The risks and benefits of ≤6-month DAPT regimens followed by aspirin monotherapy versus standard 12-month DAPT have been investigated in several studies of patients undergoing PCI with DES implantation12,63,64,65,66,67,68,69,70,71,72,73,74 (Table 3). Among the few trials that focused on patients with ACS, substantial heterogeneity was present in the type of DES used. Some studies mandated biodegradable polymer DES and other studies mandated durable polymer DES, and a variety of drugs were eluted (biolimus, everolimus, sirolimus, tacrolimus or zotarolimus). In some studies, patients received one type of stent, whereas other studies included patients with three or more types of DES. Therefore, on the whole, we believe that the data can be extrapolated to daily clinical practice with most modern types of stent.
In the SMART DATE trial66, 1,357 patients with ACS were assigned to the 6-month DAPT group and 1,355 to the ≥12-month DAPT group. The trial showed non-inferiority of the 6-month DAPT regimen for the composite of all-cause death, MI and stroke. However, MI occurred more frequently with 6 months of DAPT than with ≥12 months of DAPT. No significant difference in BARC type 2–5 bleeding was reported66. A subsequent individual patient-level analysis of 14,963 patients from eight randomized trials comparing 3–6 months of DAPT followed by aspirin with ≥12 months of DAPT showed that patients with ACS who were not at high risk of bleeding benefited from prolonged DAPT with a reduction in ischaemic events, whereas those at high risk of bleeding (PRECISE-DAPT score ≥25) did not benefit from the longer duration of DAPT irrespective of their ischaemic risk56.
The effectiveness and safety of abbreviated DAPT followed by P2Y12 inhibitor (rather than aspirin) monotherapy have been compared with standard DAPT regimens in six studies (Table 3). Earlier aggregate data from direct or network meta-analyses did not conclusively quantify the risks and benefits of aspirin withdrawal in comparison with DAPT after PCI. The inclusion of events occurring during the initial DAPT phase, which was identical in both experimental and control regimens, might have biased treatment estimates towards the null, thereby underestimating the potential benefit of aspirin withdrawal.
The Single Versus Dual Antiplatelet Therapy (SIDNEY) Collaboration initially gathered individual patient data from two studies of ticagrelor monotherapy75 and, in a second iteration, from six studies assessing either clopidogrel or ticagrelor after 1–3 months of DAPT compared with DAPT continuation76. The rate of the primary outcome of all-cause death, MI and stroke was similar in patients with P2Y12 inhibitor monotherapy (mainly ticagrelor) and in patients receiving DAPT, with P2Y12 inhibitor monotherapy meeting the criteria for non-inferiority to DAPT. The treatment effect was consistent with the use of either clopidogrel or ticagrelor and in patients with or without a high risk of bleeding or ACS. In addition, the P2Y12 inhibitor monotherapy strategy was associated with reduced major bleeding76.
Subsequently, in the STOPDAPT-2 ACS extension study74, 3,008 patients with ACS undergoing PCI were randomly assigned to 1–2 months of DAPT followed by clopidogrel monotherapy or to standard DAPT, comprising aspirin and clopidogrel, for 12 months. The data were analysed in combination with the previous 1,161 patients with ACS included in the earlier STOPDAPT-2 trial77. Clopidogrel monotherapy after 1–2 months of DAPT did not meet the criteria for non-inferiority to conventional DAPT for net clinical benefit and was associated with a substantial increase in the rate of MI. Therefore, the use of clopidogrel monotherapy might be best reserved for patients with ACS in whom bleeding risk outweighs ischaemic risk.
In the MASTER DAPT trial12, patients with a high risk of bleeding undergoing PCI (for either CCS or ACS) were enrolled. Among those without the need for oral anticoagulation (64% of patients), a 1-month DAPT regimen followed by antiplatelet monotherapy (either aspirin or, in two-thirds of patients, a P2Y12 inhibitor) was compared with standard DAPT for ≥6 months. The trial demonstrated the non-inferiority of 1-month DAPT regimens, both for net adverse events and major adverse cardiac and cerebral events, together with a reduced rate of bleeding, with consistent results in patients with ACS, including those undergoing complex interventions78,79.
Clinical trial evidence for de-escalation of DAPT intensity
Unguided de-escalation
Three randomized trials testing an unguided approach to DAPT de-escalation after ACS have been conducted80,81,82,83,84,85 (Table 4). In the TOPIC trial80, patients with ACS were randomly assigned to clopidogrel-based DAPT versus standard DAPT. All patients were pre-treated with either prasugrel or ticagrelor for 1 month before randomization. The primary composite end point of cardiovascular death, urgent revascularization, stroke and BARC bleeding grade ≥2 at 1 year after ACS was significantly lower in the de-escalation group than in the standard DAPT group. These findings were driven by a reduction in BARC ≥2 bleeding, whereas the incidence of ischaemic events was similar in the two groups80.
The non-inferiority of a prasugrel dose-reduction strategy (from 10 mg to 5 mg), compared with continuation of the 10 mg dose, 1 month after ACS was tested in East Asian patients in the HOST-REDUCE-POLYTECH-ACS randomized trial81. The incidence of the primary end point — the rate of net adverse clinical events (all-cause death, non-fatal MI, stent thrombosis, repeat revascularization, stroke and BARC ≥2 bleeding) — was lower with the dose de-escalation strategy, driven by a reduction in minor bleeding without an increase in ischaemia81, irrespective of PCI complexity86.
In the TALOS-AMI study82, an open-label, non-inferiority randomized trial, 2,697 East Asian patients were assigned to clopidogrel-based DAPT or continuation of ticagrelor-based DAPT for 1 month after ACS. The clopidogrel-based de-escalation strategy met the criteria for non-inferiority for the primary composite end point of cardiovascular death, MI, stroke or BARC ≥2 bleeding. These results were primarily driven by a reduction in BARC ≥2 bleeding events in the de-escalation group82.
Guided de-escalation
The response of individuals to some drugs can be variable due to genetic variation and other characteristics such as body weight and the presence of comorbidities, including CKD and diabetes87. Of the antiplatelet drugs, only clopidogrel is subject to large interindividual variability in its antiplatelet effect partly due to polymorphism of the CYP2C19 gene, resulting in an inadequate response to treatment in approximately 30% of patients88. To reduce the risk of bleeding in patients with ACS receiving prasugrel or ticagrelor as part of DAPT, de-escalation to clopidogrel based on genetic testing could be a useful strategy.
The ABCD-GENE risk score comprises four clinical variables (age, BMI, CKD status and diabetes status) and one genetic variable (CYP2C19 loss-of-function alleles) and can help clinicians to identify patients who are most likely to have high on-treatment platelet reactivity with clopidogrel87. This genotype-guided de-escalation strategy was tested in the POPular Genetics trial85, involving 2,488 patients with STEMI undergoing primary PCI. All patients received aspirin and were randomly assigned within 48 h of PCI to a genotype-guided P2Y12 inhibitor strategy or to a standard-of-care P2Y12 inhibitor strategy. In the genotype-guided group, carriers of loss-of-function CYP2C19 alleles (39%) were treated with prasugrel or ticagrelor, whereas non-carriers (61%) received clopidogrel. Genotype-guided P2Y12 inhibitor treatment resulted in a lower rate of bleeding compared with standard treatment (9.8% versus 12.5%; HR 0.78, 95% CI 0.61–0.98; P = 0.04) without an increase in ischaemic events87.
The antiplatelet effect of oral P2Y12 inhibitors can be assessed in vitro by PFT89. Studies have consistently shown that patients treated with PCI and with high on-treatment platelet reactivity are at increased risk of ischaemic events, including stent thrombosis, whereas bleeding risk is higher in patients with low on-treatment platelet reactivity89. These observations led to the concept of a therapeutic window for platelet inhibition32, which could enable tailoring of antiplatelet treatment, including guiding DAPT de-escalation after PCI in patients with ACS.
The TROPICAL-ACS trial84 of 2,610 patients with ACS undergoing PCI showed that PFT-guided DAPT de-escalation met the criteria for non-inferiority, compared with standard prasugrel treatment, for a net clinical benefit end point. A similar rate of ischaemic events occurred in the two treatment groups, with a trend towards less bleeding with PFT-guided treatment. The net clinical benefit from the guided treatment approach was also seen in specific subgroups (such as younger patients)90. A meta-analysis (19,855 patients with ACS or CCS; 11 randomized trials and 3 observational studies) published in 2021 showed that guided (genotyping or PFT) DAPT de-escalation led to a reduction in bleeding events (risk ratio 0.81, 95% CI 0.68–0.96) compared with standard DAPT91.
Although both genetic tests and PFT have been used in clinical trials to guide DAPT de-escalation, access to these tests is not uniform across all practice settings. Many clinicians do not have access to either test and, even when available, results might not be obtainable within a suitable time frame to guide clinical decision-making during the hospital admission for ACS. Nonetheless, reflecting the available evidence, the latest European guidelines1,3 include a class IIb (level of evidence A) recommendation for a DAPT de-escalation strategy (including but not restricted to a PFT-guided approach), which can be considered for patients with ACS deemed unsuitable for 12 months of potent platelet inhibition.
Abbreviation versus de-escalation of DAPT
The number of patients enrolled in trials assessing the abbreviation of DAPT duration (n = 41,093) is threefold higher than the number of patients enrolled in trials assessing de-escalation of DAPT intensity (n = 12,707). Although no head-to-head comparisons of the two strategies have been performed, a network meta-analysis of 29 trials in patients with ACS undergoing PCI showed that there was no significant difference in all-cause death between abbreviated DAPT and de-escalation of DAPT intensity92. Abbreviated DAPT reduced the occurrence of major bleeding, whereas de-escalation of DAPT intensity reduced the rate of net adverse cardiovascular events92. Furthermore, although patients at high risk of bleeding have been specifically enrolled in several studies of DAPT abbreviation, the same cannot be said about trials assessing de-escalation of DAPT intensity. Therefore, less evidence exists to support the use of DAPT intensity de-escalation in patients with a high bleeding risk.
Optimal timing of abbreviation or de-escalation
DAPT abbreviation or de-escalation strategies can be initiated at different time points. De-escalation of DAPT intensity can be instituted 1 week after PCI if guided by PFT or genotyping42 and 1 month after PCI if unguided80,81,82. In most studies of DAPT abbreviation, the switch to aspirin monotherapy was made at 6 months but, in the RESET64 and the REDUCE69 trials, DAPT was abbreviated after 3 months and showed non-inferiority compared with 12 months of DAPT for the primary composite end point of ischaemic and bleeding events. By contrast, in most trials of DAPT abbreviated to P2Y12 inhibitor monotherapy, the switch occurred earlier, at 1–3 months. On the basis of the available evidence, abbreviation of DAPT duration can be considered after 1–3 months if switching to monotherapy with clopidogrel or ticagrelor, or after 3–6 months if switching to aspirin monotherapy. The 2020 ESC guidelines on the treatment of patients with ACS without STEMI recommend the use of ticagrelor monotherapy after 3 months of standard DAPT as an alternative to standard 12-month DAPT1.
As mentioned earlier, some procedural characteristics, such as double stenting of coronary bifurcations, stenting of chronic total occlusions or long lesions requiring multiple stents, are associated with an increased risk of ischaemic events1,42,43. In these patients, standard 12-month DAPT with prasugrel or ticagrelor, or even prolongation of antiplatelet therapy beyond 12 months, should be considered for those at low risk of bleeding, for whom low-dose ticagrelor would be the agent of choice93. Overall, the duration and intensity of DAPT should be tailored to the risk of ischaemia and bleeding of individual patients (Fig. 2).

ACS, acute coronary syndrome; ARC-HBR, Academic Research Consortium for High Bleeding Risk; DAPT, dual antiplatelet therapy; P2Y12, P2Y purinoceptor 12; PCI, percutaneous coronary intervention; SAPT, single antiplatelet therapy. aClopidogrel is the most studied P2Y12 inhibitor in this setting. bTicagrelor is the most studied P2Y12 inhibitor in this setting.
DAPT abbreviation or de-escalation in specific populations
Older patients
Older patients are conventionally regarded as those aged ≥75 years and represent over one-third of the population with ACS94,95. These patients are at higher ischaemic and bleeding risk than younger individuals owing to increased frailty and associated comorbidities95. Few randomized trials have been conducted to test DAPT abbreviation or de-escalation strategies in older patients with ACS. Acute, periprocedural and long-term antithrombotic therapy in older patients was addressed in a 2023 consensus paper from the ESC Working Group on Thrombosis96.
The GLOBAL LEADERS trial70 compared 1 month of DAPT followed by 23 months of ticagrelor monotherapy with 12 months of DAPT followed by 12 months of aspirin monotherapy. In a prespecified analysis of older patients (aged >75 years) enrolled in this trial (n = 2,565), there were no significant differences between the two strategies with respect to the primary end point of all-cause death or new Q-wave MI97. Among the >7,000 patients with ACS enrolled in the TWILIGHT trial30, 3 months of DAPT followed by ticagrelor monotherapy was associated with a lower incidence of clinically relevant bleeding than ticagrelor plus aspirin, without an increased risk of death, MI or stroke. These results were confirmed when restricted to older patients (aged ≥65 years)30. By contrast, in the STOPDAPT-2 ACS study of >4,000 patients (29% ≥75 years), clopidogrel monotherapy after 1–2 months of DAPT did not achieve non-inferiority to 12 months of DAPT in terms of net clinical benefit, with a numerical increase in cardiovascular events74. No treatment interaction by age was observed.
In a prespecified analysis of the TROPICAL-ACS study, no significant differences in net clinical outcome were found between PFT-guided de-escalation (DAPT with 1 week of prasugrel followed by 1 week of clopidogrel, then maintenance therapy with clopidogrel or prasugrel) and the control group (12 months of prasugrel) in patients aged >70 years90. In the TALOS-AMI trial82 of unguided de-escalation in patients with ACS, only 12% of patients were aged ≥75 years. However, the hazard ratios for the primary end point were consistent across the prespecified age subgroups (<75 years or ≥75 years), showing a significant reduction in net clinical events for the unguided de-escalation strategy82. Other studies of de-escalation from potent P2Y12 inhibitors to clopidogrel have included very few older patients. An alternative strategy was assessed in the ANTARCTIC trial83, in which older patients (aged ≥75 years) with ACS were randomly assigned to prasugrel 5 mg daily with dose or drug adjustment in the event of inadequate response (including up-titration to 10 mg or downgrading to clopidogrel according to PFT results) or oral prasugrel 5 mg daily with no monitoring. The study showed similar results with either strategy83.
Patients with renal impairment
Renal impairment is an important risk factor for the development of complex coronary artery disease. Although patients with CKD were historically less likely to undergo coronary angiography and PCI, advances over the past two decades have led to an upward trend in the rate of interventions performed in these patients98. Patients with CKD tend to have a greater coronary calcification burden and a higher prevalence of cardiovascular risk factors, such as hypertension, hyperlipidaemia and diabetes, than those without this disease, presenting substantial challenges for PCI. Those with CKD are also at increased risk of in-hospital complications, including death and bleeding after PCI, especially if transfemoral access is used99,100. Importantly, CKD is a risk factor for both long-term ischaemic and bleeding events after PCI.
The ESC guidelines include baseline CKD (estimated glomerular filtration rate (eGFR) 15–59 ml/min/1.73 m2) as a criterion for DAPT extension beyond 1 year to reduce the risk of ischaemic events1. However, CKD is also a major (eGFR <30 ml/min/1.73 m2) or minor (eGFR 30–59 ml/min/1.73 m2) criterion for abbreviation or de-escalation of DAPT according to the ARC-HBR score1. Trials of DAPT abbreviation101 that provide a subgroup analysis for baseline CKD have shown the benefit of reduced DAPT duration or intensity in patients with CKD12,30,85 as well as the safety and efficacy of this approach in those who also have a high risk of bleeding79,102.
East Asian patients
East Asian patients are considered to be at lower ischaemic risk and higher bleeding risk (including intracranial haemorrhage) with DAPT than non-East Asian patients owing to enhanced pharmacokinetic and pharmacodynamic profiles with ticagrelor and prasugrel despite CYP2C19 loss-of-function alleles being more frequent in those with East Asian ancestry38. This phenomenon is referred to as the ‘East Asian paradox’. Therefore, lower-than-conventional doses of prasugrel are prescribed in some East Asian countries such as Japan and Taiwan.
Importantly, the majority of trials of de-escalation or abbreviation of DAPT have been conducted in East Asian patients103. A systematic review and meta-analysis published in 2023 specifically assessed the safety and effectiveness of DAPT de-escalation strategies in East Asian versus non-East Asian patients with ACS undergoing PCI103. The net benefit and safety of reduction in either intensity or duration of DAPT seem to be greater in East Asian than in non-East Asian patients. The 2020 (ref. 104) and 2021 (ref. 105) Asian Pacific Society of Cardiology consensus recommendations on the use of P2Y12 antagonists in the Asia Pacific region indicate that, after a period of DAPT, use of ticagrelor monotherapy seems to be reasonable in patients with high ischaemic risk and low bleeding risk. Conversely, clopidogrel monotherapy can be used for patients with low ischaemic risk or patients with a high risk of both ischaemia and bleeding. The recommendations also support the use of abbreviated DAPT in older patients at high risk of bleeding or in patients with CKD receiving dialysis. For patients with diabetes undergoing complex PCI who are at high risk of bleeding, ticagrelor monotherapy can be considered after 3 months of DAPT105.
Several studies have been conducted to investigate DAPT abbreviation or de-escalation strategies in East Asian populations. The TICO trial73, conducted in South Korea, showed that 3 months of DAPT followed by ticagrelor monotherapy had clinical benefit in patients with ACS compared with 12 months of DAPT, which was mostly driven by a reduction in major bleeding. These data are supported by the findings from two other randomized clinical trials from East Asia: SMART-CHOICE67 (Korea) and STOPDAPT-2 (ref. 102) (Japan). In these studies, compared with 12 months of DAPT, the use of P2Y12 inhibitor monotherapy after an initial 1–3 months of DAPT was shown to reduce the risk of clinically serious bleeding in East Asian patients undergoing PCI71,77. The HOST-REDUCE-POLYTECH-ACS trial86 from South Korea showed that, in patients with ACS treated with DAPT, including 10 mg prasugrel for 1 month, the subsequent reduction to 5 mg of prasugrel significantly reduced the risk of bleeding (HR 0.48, 95% CI 0.32–0.73; P = 0.0007) without increasing ischaemic risk (HR 0.76, 95% CI 0.40–1.45; P = 0.40) compared with continuation of the conventional dose of 10 mg.
The Korea Acute Myocardial Infarction Registry–National Institutes of Health study combined ischaemic and bleeding models to establish a simple clinical prediction score for the use of DAPT. Patients with a high score (≥3 points) showed an overall benefit from potent P2Y12 inhibitor versus clopidogrel in reducing ischaemic events at 1 year without a significant increase in bleeding whereas, in patients with a low score (<3), the bleeding risk with potent P2Y12 inhibitors exceeded the ischaemic benefit106.
Conclusions
The duration and intensity of DAPT should be tailored to the risks of ischaemia and bleeding of individual patients. The risk of both types of event is highest in the early period following ACS, after which the bleeding risk falls and then stays constant over the duration of DAPT. Strategies to reduce the risk of bleeding include de-escalation of DAPT intensity, with dose reduction or a switch to a less-potent P2Y12 inhibitor, or abbreviation of DAPT duration with continuation of treatment using a single antiplatelet agent. Trials have shown that de-escalation of DAPT intensity can reduce bleeding without an increase in ischaemic events in patients without high long-term ischaemic risk and can be guided by PFT or genotyping. Abbreviation of DAPT after 1–6 months reduces bleeding without an increase in ischaemic events in patients with a high risk of bleeding and without high long-term ischaemic risk. The two approaches to reducing DAPT have not been compared in head-to-head randomized trials. Our consensus statements (Box 1) should guide clinicians to tailor these approaches to DAPT abbreviation and de-escalation for individual patients to improve outcomes.
References
Collet, J. P. et al. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur. Heart J. 42, 1289–1367 (2021).
Ibanez, B. et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur. Heart J. 39, 119–177 (2018).
Neumann, F. J. et al. 2018 ESC/EACTS guidelines on myocardial revascularization. Eur. Heart J. 40, 87–165 (2019).
O’Gara, P. T. et al. 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation 127, e362–e425 (2013).
Amsterdam, E. A. et al. 2014 AHA/ACC guideline for the management of patients with non-ST-elevation acute coronary syndromes: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation 130, e344–e426 (2014).
Lawton, J. S. et al. 2021 ACC/AHA/SCAI guideline for coronary artery revascularization: executive summary: a report of the American College of Cardiology/American Heart Association Joint Committee on clinical practice guidelines. Circulation 145, e4–e17 (2022).
Costa, F. et al. Derivation and validation of the predicting bleeding complications in patients undergoing stent implantation and subsequent dual antiplatelet therapy (PRECISE-DAPT) score: a pooled analysis of individual-patient datasets from clinical trials. Lancet 389, 1025–1034 (2017).
Navarese, E. P. et al. Optimal duration of dual antiplatelet therapy after percutaneous coronary intervention with drug eluting stents: meta-analysis of randomised controlled trials. BMJ 350, h1618 (2015).
Wallentin, L. et al. Ticagrelor versus clopidogrel in patients with acute coronary syndromes. N. Engl. J. Med. 361, 1045–1057 (2009).
Wiviott, S. D. et al. Prasugrel versus clopidogrel in patients with acute coronary syndromes. N. Engl. J. Med. 357, 2001–2015 (2007).
Pufulete, M. et al. Real-world bleeding in patients with acute coronary syndrome (ACS) undergoing percutaneous coronary intervention (PCI) and prescribed different combinations of dual antiplatelet therapy (DAPT) in England: a population-based cohort study emulating a ‘target trial’.Open Heart 9, e001999 (2022).
Valgimigli, M. et al. Dual antiplatelet therapy after PCI in patients at high bleeding risk. N. Engl. J. Med. 385, 1643–1655 (2021).
Kang, J. et al. Racial differences in ischaemia/bleeding risk trade-off during anti-platelet therapy: individual patient level landmark meta-analysis from seven RCTs. Thromb. Haemost. 119, 149–162 (2019).
Ismail, N. et al. Incidence and prognostic impact of post discharge bleeding post acute coronary syndrome within an outpatient setting: a systematic review. BMJ Open. 9, e023337 (2019).
Eikelboom, J. W. et al. Adverse impact of bleeding on prognosis in patients with acute coronary syndromes. Circulation 114, 774–782 (2006).
Ismail, N. et al. Bleeding after hospital discharge following acute coronary syndrome: incidence, types, timing, and predictors. J. Am. Heart Assoc. 8, e013679 (2019).
Crimi, G. et al. Time course of ischemic and bleeding burden in elderly patients with acute coronary syndromes randomized to low-dose prasugrel or clopidogrel. J. Am. Heart Assoc. 8, e010956 (2019).
Amin, A. P. et al. Nuisance bleeding with prolonged dual antiplatelet therapy after acute myocardial infarction and its impact on health status. J. Am. Coll. Cardiol. 61, 2130–2138 (2013).
Jeong, Y. H. et al. Pharmacodynamic profile and prevalence of bleeding episode in East Asian patients with acute coronary syndromes treated with prasugrel standard-dose versus de-escalation strategy: a randomized A-MATCH trial. Thromb. Haemost. 121, 1376–1386 (2021).
Aradi, D. et al. Platelet reactivity and clinical outcomes in acute coronary syndrome patients treated with prasugrel and clopidogrel: a pre-specified exploratory analysis from the TROPICAL-ACS trial. Eur. Heart J. 40, 1942–1951 (2019).
Baber, U. et al. Coronary thrombosis and major bleeding after PCI with drug-eluting stents: risk scores from PARIS. J. Am. Coll. Cardiol. 67, 2224–2234 (2016).
Yeh, R. W. et al. Development and validation of a prediction rule for benefit and harm of dual antiplatelet therapy beyond 1 year after percutaneous coronary intervention. JAMA 315, 1735–1749 (2016).
Urban, P. et al. Defining high bleeding risk in patients undergoing percutaneous coronary intervention: a consensus document from the Academic Research Consortium for High Bleeding Risk. Eur. Heart J. 40, 2632–2653 (2019).
Nakamura, M. et al. JCS 2020 guideline focused update on antithrombotic therapy in patients with coronary artery disease. Circ. J. 84, 831–865 (2020).
Wiviott, S. D. et al. Prasugrel compared with high loading- and maintenance-dose clopidogrel in patients with planned percutaneous coronary intervention: the Prasugrel in Comparison to Clopidogrel for Inhibition of Platelet Activation and Aggregation-Thrombolysis in Myocardial Infarction 44 trial. Circulation 116, 2923–2932 (2007).
Storey, R. F. et al. Inhibitory effects of ticagrelor compared with clopidogrel on platelet function in patients with acute coronary syndromes: the PLATO (PLATelet inhibition and patient Outcomes) PLATELET substudy. J. Am. Coll. Cardiol. 56, 1456–1462 (2010).
Orme, R. C. et al. Study of two dose regimens of ticagrelor compared with clopidogrel in patients undergoing percutaneous coronary intervention for stable coronary artery disease. Circulation 138, 1290–1300 (2018).
Yusuf, S. et al. Effects of clopidogrel in addition to aspirin in patients with acute coronary syndromes without ST-segment elevation. N. Engl. J. Med. 345, 494–502 (2001).
Schupke, S. et al. Ticagrelor or prasugrel in patients with acute coronary syndromes. N. Engl. J. Med. 381, 1524–1534 (2019).
Mehran, R. et al. Ticagrelor with or without aspirin in high-risk patients after PCI. N. Engl. J. Med. 381, 2032–2042 (2019).
Kang, M. G. et al. Prevalence of adverse events during ticagrelor versus clopidogrel treatment and its association with premature discontinuation of dual antiplatelet therapy in East Asian patients with acute coronary syndrome. Front. Cardiovasc. Med. 9, 1053867 (2022).
Sibbing, D., Steinhubl, S. R., Schulz, S., Schomig, A. & Kastrati, A. Platelet aggregation and its association with stent thrombosis and bleeding in clopidogrel-treated patients: initial evidence of a therapeutic window. J. Am. Coll. Cardiol. 56, 317–318 (2010).
Sousa-Uva, M. et al. Expert position paper on the management of antiplatelet therapy in patients undergoing coronary artery bypass graft surgery. Eur. Heart J. 35, 1510–1514 (2014).
Jones, W. S. et al. Comparative effectiveness of aspirin dosing in cardiovascular disease. N. Engl. J. Med. 384, 1981–1990 (2021).
CURRENT-OASIS 7 Investigators et al. Dose comparisons of clopidogrel and aspirin in acute coronary syndromes. N. Engl. J. Med. 363, 930–942 (2010).
Friberg, L., Rosenqvist, M. & Lip, G. Y. Evaluation of risk stratification schemes for ischaemic stroke and bleeding in 182 678 patients with atrial fibrillation: the Swedish Atrial Fibrillation cohort study. Eur. Heart J. 33, 1500–1510 (2012).
Gorog, D. A. et al. Assessment and mitigation of bleeding risk in atrial fibrillation and venous thromboembolism: executive summary of a European and Asia-Pacific expert consensus paper. Thromb. Haemost. 122, 1625–1652 (2022).
Kim, H. K. et al. The East Asian paradox: an updated position statement on the challenges to the current antithrombotic strategy in patients with cardiovascular disease. Thromb. Haemost. 121, 422–432 (2021).
Abtan, J. et al. Residual ischemic risk and its determinants in patients with previous myocardial infarction and without prior stroke or TIA: insights from the REACH registry. Clin. Cardiol. 39, 670–677 (2016).
Lafitte, M. et al. After acute coronary syndrome, diabetic patients with peripheral vascular disease remain at high risk of cardiovascular events despite secondary prevention measures. Arch. Cardiovasc. Dis. 103, 97–105 (2010).
Leonardi, S. et al. Optimised care of elderly patients with acute coronary syndrome. Eur. Heart J. Acute Cardiovasc. Care 7, 287–295 (2018).
Galli, M. & Angiolillo, D. J. De-escalation of antiplatelet therapy in acute coronary syndromes: why, how and when. Front. Cardiovasc. Med. 9, 975969 (2022).
Giustino, G. et al. Efficacy and safety of dual antiplatelet therapy after complex PCI. J. Am. Coll. Cardiol. 68, 1851–1864 (2016).
D’Ascenzo, F. et al. Incidence and predictors of coronary stent thrombosis: evidence from an international collaborative meta-analysis including 30 studies, 221,066 patients, and 4276 thromboses. Int. J. Cardiol. 167, 575–584 (2013).
Gosling, R. et al. Comparison of P2Y(12) inhibitors for mortality and stent thrombosis in patients with acute coronary syndromes: single center study of 10 793 consecutive ‘real-world’ patients. Platelets 28, 767–773 (2017).
Palmerini, T. et al. Three, six, or twelve months of dual antiplatelet therapy after DES implantation in patients with or without acute coronary syndromes: an individual patient data pairwise and network meta-analysis of six randomized trials and 11 473 patients. Eur. Heart J. 38, 1034–1043 (2017).
Grines, C. L. et al. Prevention of premature discontinuation of dual antiplatelet therapy in patients with coronary artery stents: a science advisory from the American Heart Association, American College of Cardiology, Society for Cardiovascular Angiography and Interventions, American College of Surgeons, and American Dental Association, with representation from the American College of Physicians. Circulation 115, 813–818 (2007).
Iakovou, I. et al. Incidence, predictors, and outcome of thrombosis after successful implantation of drug-eluting stents. JAMA 293, 2126–2130 (2005).
Spertus, J. A. et al. Prevalence, predictors, and outcomes of premature discontinuation of thienopyridine therapy after drug-eluting stent placement: results from the PREMIER registry. Circulation 113, 2803–2809 (2006).
Zwart, B., Godschalk, T. C., Kelder, J. C. & Ten Berg, J. M. High risk of stent thrombosis in the first 6 months after coronary stenting: do not discontinue clopidogrel early after ACS. J. Interv. Cardiol. 30, 421–426 (2017).
Schoos, M. et al. Patterns and impact of dual antiplatelet cessation on cardiovascular risk after percutaneous coronary intervention in patients with acute coronary syndromes. Am. J. Cardiol. 123, 709–716 (2019).
Giustino, G. et al. Duration of dual antiplatelet therapy after drug-eluting stent implantation: a systematic review and meta-analysis of randomized controlled trials. J. Am. Coll. Cardiol. 65, 1298–1310 (2015).
Kawashima, H. et al. Comparative assessment of predictive performance of PRECISE-DAPT, CRUSADE, and ACUITY scores in risk stratifying 30-day bleeding events. Thromb. Haemost. 120, 1087–1095 (2020).
Mihatov, N. et al. Utility of the dual antiplatelet therapy score to guide antiplatelet therapy: a systematic review and meta-analysis. Catheter. Cardiovasc. Interv. 97, 569–578 (2021).
Bonaca, M. P. et al. Patient selection for long-term secondary prevention with ticagrelor: insights from PEGASUS-TIMI 54. Eur. Heart J. 43, 5037–5044 (2022).
Costa, F. et al. Dual antiplatelet therapy duration based on ischemic and bleeding risks after coronary stenting. J. Am. Coll. Cardiol. 73, 741–754 (2019).
Angiolillo, D. J., Galli, M., Collet, J. P., Kastrati, A. & O’Donoghue, M. L. Antiplatelet therapy after percutaneous coronary intervention. EuroIntervention 17, e1371–e1396 (2022).
D’Ascenzo, F. et al. Average daily ischemic versus bleeding risk in patients with ACS undergoing PCI: insights from the BleeMACS and RENAMI registries. Am. Heart J. 220, 108–115 (2020).
Chau, K. H. et al. Stent thrombosis risk over time on the basis of clinical presentation and platelet reactivity: analysis from ADAPT-DES. JACC Cardiovasc. Interv. 14, 417–427 (2021).
Costa, F. et al. A 4-item PRECISE-DAPT score for dual antiplatelet therapy duration decision-making. Am. Heart J. 223, 44–47 (2020).
Tavenier, A. H. et al. Guided and unguided de-escalation from potent P2Y12 inhibitors among patients with acute coronary syndrome: a meta-analysis. Eur. Heart J. Cardiovasc. Pharmacother. 8, 492–502 (2022).
Kang, J. et al. Dual antiplatelet therapy de-escalation in acute coronary syndrome: an individual patient meta-analysis. Eur. Heart J. 44, 1360–1370 (2023).
Gwon, H. C. et al. Six-month versus 12-month dual antiplatelet therapy after implantation of drug-eluting stents: the Efficacy of Xience/Promus Versus Cypher to Reduce Late Loss After Stenting (EXCELLENT) randomized, multicenter study. Circulation 125, 505–513 (2012).
Kim, B. K. et al. A new strategy for discontinuation of dual antiplatelet therapy: the RESET Trial (REal Safety and Efficacy of 3-month dual antiplatelet Therapy following endeavor zotarolimus-eluting stent implantation). J. Am. Coll. Cardiol. 60, 1340–1348 (2012).
Han, Y. et al. Six versus 12 months of dual antiplatelet therapy after implantation of biodegradable polymer sirolimus-eluting stent: randomized substudy of the I-LOVE-IT 2 trial. Circ. Cardiovasc. Interv. 9, e003145 (2016).
Hahn, J. Y. et al. 6-month versus 12-month or longer dual antiplatelet therapy after percutaneous coronary intervention in patients with acute coronary syndrome (SMART-DATE): a randomised, open-label, non-inferiority trial. Lancet 391, 1274–1284 (2018).
Kedhi, E. et al. Six months versus 12 months dual antiplatelet therapy after drug-eluting stent implantation in ST-elevation myocardial infarction (DAPT-STEMI): randomised, multicentre, non-inferiority trial. BMJ 363, k3793 (2018).
Lee, B. K. et al. Safety of six-month dual antiplatelet therapy after second-generation drug-eluting stent implantation: OPTIMA-C randomised clinical trial and OCT substudy. EuroIntervention 13, 1923–1930 (2018).
De Luca, G. et al. Final results of the randomised evaluation of short-term dual antiplatelet therapy in patients with acute coronary syndrome treated with a new-generation stent (REDUCE trial). EuroIntervention 15, e990–e998 (2019).
Vranckx, P. et al. Ticagrelor plus aspirin for 1 month, followed by ticagrelor monotherapy for 23 months vs aspirin plus clopidogrel or ticagrelor for 12 months, followed by aspirin monotherapy for 12 months after implantation of a drug-eluting stent: a multicentre, open-label, randomised superiority trial. Lancet 392, 940–949 (2018).
Hahn, J. Y. et al. Effect of P2Y12 inhibitor monotherapy vs dual antiplatelet therapy on cardiovascular events in patients undergoing percutaneous coronary intervention: the SMART-CHOICE randomized clinical trial. JAMA 321, 2428–2437 (2019).
Baber, U. et al. Ticagrelor alone vs. ticagrelor plus aspirin following percutaneous coronary intervention in patients with non-ST-segment elevation acute coronary syndromes: TWILIGHT-ACS. Eur. Heart J. 41, 3533–3545 (2020).
Kim, B. K. et al. Effect of ticagrelor monotherapy vs ticagrelor with aspirin on major bleeding and cardiovascular events in patients with acute coronary syndrome: the TICO randomized clinical trial. JAMA 323, 2407–2416 (2020).
Watanabe, H. et al. Comparison of clopidogrel monotherapy after 1 to 2 months of dual antiplatelet therapy with 12 months of dual antiplatelet therapy in patients with acute coronary syndrome: the STOPDAPT-2 ACS randomized clinical trial. JAMA Cardiol. 7, 407–417 (2022).
Valgimigli, M. et al. Ticagrelor monotherapy versus dual-antiplatelet therapy after PCI: an individual patient-level meta-analysis. JACC Cardiovasc. Interv. 14, 444–456 (2021).
Valgimigli, M. et al. P2Y12 inhibitor monotherapy or dual antiplatelet therapy after coronary revascularisation: individual patient level meta-analysis of randomised controlled trials. BMJ 373, n1332 (2021).
Watanabe, H. et al. Effect of 1-month dual antiplatelet therapy followed by clopidogrel vs 12-month dual antiplatelet therapy on cardiovascular and bleeding events in patients receiving PCI: the STOPDAPT-2 randomized clinical trial. JAMA 321, 2414–2427 (2019).
Smits, P. C. et al. Abbreviated antiplatelet therapy after coronary stenting in patients with myocardial infarction at high bleeding risk. J. Am. Coll. Cardiol. 80, 1220–1237 (2022).
Valgimigli, M. et al. Duration of antiplatelet therapy after complex percutaneous coronary intervention in patients at high bleeding risk: a MASTER DAPT trial sub-analysis. Eur. Heart J. 43, 3100–3114 (2022).
Cuisset, T. et al. Benefit of switching dual antiplatelet therapy after acute coronary syndrome: the TOPIC (timing of platelet inhibition after acute coronary syndrome) randomized study. Eur. Heart J. 38, 3070–3078 (2017).
Kim, H. S. et al. Prasugrel-based de-escalation of dual antiplatelet therapy after percutaneous coronary intervention in patients with acute coronary syndrome (HOST-REDUCE-POLYTECH-ACS): an open-label, multicentre, non-inferiority randomised trial. Lancet 396, 1079–1089 (2020).
Kim, C. J. et al. Unguided de-escalation from ticagrelor to clopidogrel in stabilised patients with acute myocardial infarction undergoing percutaneous coronary intervention (TALOS-AMI): an investigator-initiated, open-label, multicentre, non-inferiority, randomised trial. Lancet 398, 1305–1316 (2021).
Cayla, G. et al. Platelet function monitoring to adjust antiplatelet therapy in elderly patients stented for an acute coronary syndrome (ANTARCTIC): an open-label, blinded-endpoint, randomised controlled superiority trial. Lancet 388, 2015–2022 (2016).
Sibbing, D. et al. Guided de-escalation of antiplatelet treatment in patients with acute coronary syndrome undergoing percutaneous coronary intervention (TROPICAL-ACS): a randomised, open-label, multicentre trial. Lancet 390, 1747–1757 (2017).
Claassens, D. M. F. et al. A genotype-guided strategy for oral P2Y12 inhibitors in primary PCI. N. Engl. J. Med. 381, 1621–1631 (2019).
Hwang, D. et al. Prasugrel dose de-escalation therapy after complex percutaneous coronary intervention in patients with acute coronary syndrome: a post hoc analysis from the HOST-REDUCE-POLYTECH-ACS trial. JAMA Cardiol. 7, 418–426 (2022).
Angiolillo, D. J. et al. Derivation, validation, and prognostic utility of a prediction rule for nonresponse to clopidogrel: the ABCD-GENE score. JACC Cardiovasc. Interv. 13, 606–617 (2020).
Roberts, J. D. et al. Point-of-care genetic testing for personalisation of antiplatelet treatment (RAPID GENE): a prospective, randomised, proof-of-concept trial. Lancet 379, 1705–1711 (2012).
Sibbing, D. et al. Updated expert consensus statement on platelet function and genetic testing for guiding P2Y(12) receptor inhibitor treatment in percutaneous coronary intervention. JACC Cardiovasc. Interv. 12, 1521–1537 (2019).
Sibbing, D. et al. Age and outcomes following guided de-escalation of antiplatelet treatment in acute coronary syndrome patients undergoing percutaneous coronary intervention: results from the randomized TROPICAL-ACS trial. Eur. Heart J. 39, 2749–2758 (2018).
Galli, M. et al. Guided versus standard antiplatelet therapy in patients undergoing percutaneous coronary intervention: a systematic review and meta-analysis. Lancet 397, 1470–1483 (2021).
Laudani, C. et al. Short duration of DAPT versus de-escalation after percutaneous coronary intervention for acute coronary syndromes. JACC Cardiovasc. Interv. 15, 268–277 (2022).
Bonaca, M. P. et al. Long-term use of ticagrelor in patients with prior myocardial infarction. N. Engl. J. Med. 372, 1791–1800 (2015).
Garcia-Blas, S. et al. Acute coronary syndrome in the older patient. J. Clin. Med. 10, 4132 (2021).
Kayani, W. T., Khan, M. R., Deshotels, M. R. & Jneid, H. Challenges and controversies in the management of ACS in elderly patients. Curr. Cardiol. Rep. 22, 51 (2020).
Andreotti, F. et al. Acute, periprocedural and longterm antithrombotic therapy in older adults. Eur. Heart J. 44, 262–279 (2023).
Tomaniak, M. et al. Ticagrelor monotherapy beyond one month after PCI in ACS or stable CAD in elderly patients: a pre-specified analysis of the GLOBAL LEADERS trial. EuroIntervention 15, e1605–e1614 (2020).
Patel, B., Shah, M., Dusaj, R., Maynard, S. & Patel, N. Percutaneous coronary intervention and inpatient mortality in patients with advanced chronic kidney disease presenting with acute coronary syndrome. Proc. (Bayl. Univ. Med. Cent.) 30, 400–403 (2017).
Gupta, T. et al. Association of chronic renal insufficiency with in-hospital outcomes after percutaneous coronary intervention. J. Am. Heart Assoc. 4, e002069 (2015).
Latif, A. et al. Meta-analysis of transradial versus transfemoral access for percutaneous coronary intervention in patients with chronic kidney disease. Am. J. Cardiol. 157, 8–14 (2021).
Gelbenegger, G. et al. Optimal duration and combination of antiplatelet therapies following percutaneous coronary intervention: a meta-analysis. Vasc. Pharmacol. 138, 106858 (2021).
Dangas, G. et al. Ticagrelor with or without aspirin after complex PCI. J. Am. Coll. Cardiol. 75, 2414–2424 (2020).
Gorog, D. A. et al. Comparison of de-escalation of DAPT intensity or duration in East Asian and Western patients with ACS undergoing PCI: a systematic review and meta-analysis. Thromb. Haemost. https://doi.org/10.1055/s-0043-57030 (2023).
Tan, J. W. et al. 2020 Asian Pacific Society of Cardiology consensus recommendations on the use of P2Y12 receptor antagonists in the Asia-Pacific region. Eur. Cardiol. 16, e02 (2021).
Tan, J. W. C. et al. 2021 Asian Pacific Society of Cardiology consensus recommendations on the use of P2Y12 receptor antagonists in the Asia-Pacific region: special populations. Eur. Cardiol. 16, e43 (2021).
Lee, S. H. et al. Practical guidance for P2Y12 inhibitors in acute myocardial infarction undergoing percutaneous coronary intervention. Eur. Heart J. Cardiovasc. Pharmacother. 7, 112–124 (2021).
van der Sangen, N. M. R. et al. Single antiplatelet therapy directly after percutaneous coronary intervention in non-ST-segment elevation acute coronary syndrome patients: the OPTICA study. EuroIntervention 19, 63–72 (2023).
Author information
Authors and Affiliations
Contributions
The authors contributed substantially to all aspects of the article.
Corresponding author
Ethics declarations
Competing interests
D.A.G. reports institutional research grants from Alpha MD, AstraZeneca, Bayer, Medtronic and Werfen, and speaker fees from AstraZeneca. J.L.F. reports speaker fees from Abbott, AstraZeneca, Boehringer Ingelheim, Bristol Myers Squibb, Daiichi Sankyo, Eli Lilly, Ferrer, Pfizer, Roche Diagnostics, Rovi and Terumo; consulting fees from AstraZeneca, Biotronik, Boehringer Ingelheim, Boston Scientific, Bristol Myers Squibb, Daiichi Sankyo, Eli Lilly, Ferrer and Pfizer; and a research grant from AstraZeneca. J.A. reports speaking honoraria from AstraZeneca, Bayer and Daiichi Sankyo. T.G. reports speaker and consultant fees or research grants from AstraZeneca, Bayer, BMS/Pfizer, Boehringer Ingelheim, Daiichi Sankyo, Edwards Lifescience, Ferrer/Chiesi and Medtronic. S.H. reports speaker fees from AstraZeneca, BMS/Pfizer, Novartis and Sanofi. No fees were received personally. Y.H.J. reports speaker fees from Daiichi Sankyo, Han-mi Pharmaceutical, JW Pharmaceutical, and Sanofi Aventis and research grants from Biotronik, Han-mi Pharmaceuticals, Sam-jin Pharmaceuticals, U&I Corporation and Yuhan Pharmaceuticals. E.P.N. reports research grants from Abbott and Amgen and lecture fees/honoraria from Amgen, AstraZeneca, Bayer, Pfizer and Sanofi-Regeneron. D.S. reports speaker fees and fees for advisory board activities from Bayer and Sanofi Aventis. J.M.S.-M. reports speaker or consultant fees from Biosensors, Boehringer Ingelheim, Boston Scientific, Chiesi, Daiichi Sankyo and P&F. R.F.S. reports institutional research grants/support from AstraZeneca, Cytosorbents, GlyCardial Diagnostics and Thromboserin, and personal fees from Alnylam, AstraZeneca, Bayer, Bristol Myers Squibb/Pfizer, Chiesi, CSL Behring, Cytosorbents, Daiichi Sankyo, GlyCardial Diagnostics, Hengrui, Idorsia, Intas Pharmaceuticals, Medscape, Novartis, PhaseBio, Sanofi Aventis and Thromboserin. J.W.C.T. reports honoraria from Abbott Vascular, Alvimedica, Amgen, AstraZeneca, Bayer, Biosensors, Boehringer Ingelheim, Medtronic and Pfizer; research and educational grants from Abbott Vascular, Amgen, AstraZeneca, Biosensors, Biotronik, Medtronic, Otsuka, Philips, Roche and Terumo; and consulting fees from CSL Behring and Elixir. J.M.t.B. reports advisory/consulting/speakers fees from AstraZeneca, Bayer, BMS, Boehringer Ingelheim, CeleCOR Daiichi Sankyo, Eli Lilly, Ferrer, and Pfizer and institutional research grants from AstraZeneca, Daiichi Sankyo and ZonMw (Dutch Government). M.V. reports grants from Terumo and personal fees from Abbott Vascular, Alvimedica/CID, AstraZeneca, Bayer, Biotronik, Boston Scientific, Bristol Myers Squibb SA, Chiesi, CoreFLOW, Daiichi Sankyo, ECRI, IDORSIA Pharmaceuticals, Medscape, Medtronic, Novartis, PhaseBio, Terumo, Universität Basel, Dept. Klinische Forschung, Vesalio and Vifor. C.V. reports speaker fees from Bayer, Boehringer Ingelheim and Daiichi Sankyo. G.Y.H.L. reports consultant and speaker activities for Anthos, BMS/Pfizer, Boehringer Ingelheim and Daiichi Sankyo. No fees were received personally. The other authors declare no competing interests.
Peer review
Peer review information
Nature Reviews Cardiology thanks Usman Baber, José María de la Torre Hernández and João Morais for their contribution to the peer review of this work.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Gorog, D.A., Ferreiro, J.L., Ahrens, I. et al. De-escalation or abbreviation of dual antiplatelet therapy in acute coronary syndromes and percutaneous coronary intervention: a Consensus Statement from an international expert panel on coronary thrombosis. Nat Rev Cardiol 20, 830–844 (2023). https://doi.org/10.1038/s41569-023-00901-2
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41569-023-00901-2
This article is cited by
-
Randomized evaluation of 5-month Ticagrelor monotherapy after 1-month dual-antiplatelet therapy in patients with acute coronary syndrome treated with drug-coated balloons: REC-CAGEFREE II trial rationale and design
BMC Cardiovascular Disorders (2024)
-
Author’s Reply to Kow et al.: “Comparison of Clinical Outcomes between Ticagrelor and Clopidogrel in East-Asian Patients with Acute Coronary Syndrome: Large Cohort Study”
American Journal of Cardiovascular Drugs (2024)
-
De-escalation of antithrombotic treatment after acute coronary syndrome, a new paradigm
Internal and Emergency Medicine (2024)
-
Role of Brain-Derived Neurotrophic Factor in Anxiety or Depression After Percutaneous Coronary Intervention
Molecular Neurobiology (2023)
