
Abstract
This study aimed to investigate the relationship between the utilization of household water treatment devices (UHWTD) and both overall and cause-specific mortality, addressing the lack of comprehensive prospective research in this area. The study was a population-based prospective cohort study using data from the US National Health and Nutrition Examination Survey (NHANES 1999–2010). Among the 30,322 participants included in the study, the group without UHWTD (No UHWTD) was younger but reported worse baseline health compared to the UHWTD group. During an average follow-up period of 14.3 years, 6811 participants died. After adjusting for age, sex, and other covariates, No UHWTD was significantly associated with a higher risk of overall (adjusted hazard ratio [aHR]: 1.221, 95% Confidence Interval [CI]: 1.147–1.300), heart (aHR: 1.405, 95% CI: 1.241–1.589), cancer (aHR: 1.176, 95% CI: 1.003–1.379), Alzheimer’s disease (aHR: 1.404, 95% CI: 1.027–1.919), and nephrosis (aHR: 1.613, 95% CI: 1.026–2.537) mortality compared to UHWTD. Moreover, those main association almost remained after further adjustment for water source. Additionally, we observed a lower detection rate of bromoform, chloroform, bromodichloromethane, and dibromochloromethane in tap water when household water treatment devices was used compared to No UHWTD. The utilization of household water treatment devices in this prospective cohort was associated with modest reductions in the risk of overall, heart, cancer, Alzheimer’s disease, and nephrosis mortality. These findings suggest that the use of household water treatment devices may have the potential to influence health outcomes and extend life expectancy.
Similar content being viewed by others

Introduction
Access to clean and safe drinking water is not only essential for maintaining human health but also a basic human right recognized by the United Nations1. Inadequate access to clean water can lead to various waterborne diseases, particularly in developing countries where sanitation infrastructure is limited2. In developing countries, the transmission of bacteria, virus and other waterborne pathogens plays a crucial role in the health implications of drinking water3,4. In the absence of municipal and piped water supply conditions, household water treatment equipment plays a crucial role in preventing and controlling the spread of these diseases, as it helps remove pathogens, bacteria, and other contaminants from the water5. In low-income countries and regions, inappropriate waste disposal and high levels of pathogenicz microorganisms in water are major issues that affect water security6. Studies have observed the preventive effect of drinking water disinfection and household water treatment equipment on diarrhea, especially in children7,8. Recently published systematic reviews and meta- analyses have shown that the use of water disinfection and treatment equipment brings about substantial health and economic benefits in less developed areas9,10. This has significant importance in improving the risk of child mortality and addressing the challenges of water security in these regions11.
Even in developed countries, drinking water safety is still widely concerned, despite the presence of comprehensive municipal piped water supply and national standards for safe drinking water. While water treatment processes have been regulated to ensure compliance with drinking water standards, concerns have been raised about the potential health effects of certain chemicals and disinfection by-products that may persist in treated water. For example, chlorination, a commonly used disinfection method, can result in the formation of disinfection by-products such as trihalomethanes (THMs), which have been associated with adverse health effects, including an increased risk of cancer12. Additionally, emerging contaminants such as pharmaceuticals, pesticides, and personal care products have been detected in drinking water sources, raising concerns about their potential impacts on human health13,14. Despite undergoing standardized treatment, tap water or well water may still contain trace amounts of contaminants, including per- and polyfluoroalkyl substances (PFAS) and other persistent organic pollutants. PFAS are synthetic chemicals widely used in various industrial and consumer products, and their presence in drinking water has drawn significant attention due to potential adverse health effects15. In addition to these concerns, the excessive presence of heavy metals in water due to aging and corroded water supply pipes has become a significant public concern. A prominent example is the issue of lead contamination in water, which is prevalent in the United States due to deteriorating infrastructure and outdated housing with lead pipes16. This problem has had severe implications for public health, as demonstrated by cases like Flint, Michigan, and numerous other locations16,17.
Household water treatment equipment is the final stage of the water supply network, such as activated carbon filters and reverse osmosis systems, can effectively remove these contaminants, providing an additional layer of protection for consumers14. In the field of home water treatment equipment research and development, a plethora of emerging technologies and methods are being developed to address the crisis of water safety18,19,20. However, it is important to consider the potential trade-offs associated with water treatment. While the removal of contaminants is necessary for ensuring safe drinking water, the treatment process may also remove beneficial minerals that are essential for human health, such as calcium, magnesium, and potassium21. The loss of these minerals from treated water can have implications for overall mineral balance and potential health effects22. Therefore, finding a balance between effective contaminant removal and the preservation of essential minerals is crucial in the design and utilization of domestic water treatment equipment.
Although research in developing countries without municipal water supply suggests that the application of household water treatment devices has shown positive efficacy in improving reported cases of childhood diarrhea7,23, the self-reported incidence rate may not reflect long-term or more severe impacts. On the other hand, in the context of municipal and piped water supply, the long-term health effects of household water treatment devices are not sufficiently understood beyond infection and diarrhea. Given the complexity of these issues and the lack of conclusive evidence on the long-term health effects of domestic water treatment equipment, further research is needed. Compared to other measurement methods, reported mortality rates are considered less susceptible to bias and are regarded as the ultimate indicator of long-term health outcomes. This study aims to address this research gap by investigating the relationship between the utilization of household water treatment devices and both overall and cause-specific mortality. By analyzing a population-based prospective cohort, we aim to provide valuable insights into the potential impact of such equipment on long-term health outcomes.
Results
Baseline characteristics
Out of the 62,160 participants involved in NHANES (National Health and Nutrition Examination Survey) 1999–2010, a total of 30,322 participants, comprising 14,543 men (47.98%) and 15,779 women, fulfilled the inclusion criteria (Supplementary Fig. 1 in Supplementary Material). Their mean ages were 46.50 (95% CI: 46.07–46.94) years.
Among those, 7677 subjects reported utilizing household water treatment devices (UHWTD), while 22,645 did not. The adjusted utilization rate of household water treatment equipment among adults in the United States was 30.632%, showing significant variation across different races and education levels. Additionally, it is worth noting that the utilization rate of these devices has remained consistently stable over time (Supplementary Table 1 in Supplementary Material).
Table 1 presents the baseline characteristics of the study participants according to use of household water treatment devices or not. Compared to participants who did not use household water treatment devices (NO UHWTD), those in the UHWTD group were more likely to be elderly and engage in higher levels of alcohol consumption. Interestingly, they were with lower BMI, higher education, less likely to be current smokers, had better eating and exercise habits, a lower self-reported history of chronic disease, and better self-reported health.
Cohort characteristics by UHWTD and the source of tap water are presented in Supplementary Table 2 in Supplementary Material.
Relations of UHWTD with all-cause mortality
Among the 30,322 participants in NHANES 1999–2010, there were 6811 deaths during a mean follow-up of 14.3 years (391,638 person years). These deaths included 1745 from heart disease, 1501 from cancer, 389 from chronic lower respiratory diseases, 208 from injuries and accidents, 405 from cerebrovascular diseases, 278 from Alzheimer’s disease, 257 from diabetes mellitus, 156 from influenza and pneumonia, 167 from nephritis, nephrotic syndrome, and nephrosis, and 1705 from all other causes combined.
Table 2 provides a summary of the association between UHWTD and all-cause mortality. Participants in the NO UHWTD group had higher rates of all-cause mortality compared to those in the UHWTD group (adjusted hazard ratio [aHR]: 1.452, 95% confidence interval [CI]: 1.348–1.564). Even after adjusting for various factors, including age, sex, race/ethnicity, education, BMI, smoking, alcohol consumption, leisure time physical activity level, healthy eating index, family history of diabetes or heart attack, self-reported health, and self-reported history of chronic diseases, the associations remained significant for overall mortality (aHR: 1.221, 95% CI: 1.147–1.300).
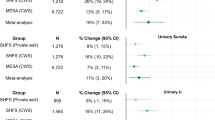
Further adjustment for the source of tap water did not affect our primary findings. When we further categorized the exposure based on UHWTD and the source of tap water, all other groups demonstrated a significant reduction in mortality rates compared to the “NO UHWTD & TAP from water company” group (Table 3). Among these groups, the “UHWTD & TAP from well” group exhibited the most substantial decrease in mortality rates (aHR: 0.756, 95% CI: 0.672–0.851).
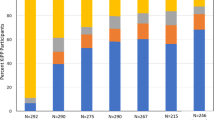
The association between UHWTD and all-cause mortality remained relatively consistent when analyzing the data stratified by sex, educational level, and smoking status (Fig. 1). However, age stratification may attenuate this link, especially among younger individuals.

All estimates accounted for complex survey designs and adjust for age (not when stratified by baseline age), sex (not when stratified by baseline sex), race/ethnicity, education (not when stratified by baseline education), BMI, smoking (not when stratified by baseline smoking status), alcohol consumption, leisure time physical activity level, healthy eating index, family history of diabetes or heart attack, self- reported health and self-reported chronic diseases. The error bar is defined as the 95% Cl of aHR.
The results were almost unchanged when we removed participants with missing values for covariates (Supplementary Table 3 in Supplementary Material), or excluded participants with prevalent diabetes, cardiovascular disease, or cancer (Supplementary Table 4 in Supplementary Material), or categorized participants based on different NHANES time periods (Supplementary Table 5 in Supplementary Material). When stratified by age at death to evaluate the effect on premature death, the associations were similar to our main results (Supplementary Table 6 in Supplementary Material).
Relations of UHWTD with cause--specific mortality
After comprehensive adjustment, participants in the NO UHWTD group exhibited higher rates of mortality from heart disease (aHR: 1.405, 95% CI: 1.241–1.589), cancer (aHR: 1.176, 95% CI: 1.003–1.379), Alzheimer’s disease (aHR: 1.404, 95% CI: 1.027–1.919), nephritis (aHR: 1.613, 95% CI: 1.026–2.537), and other causes (aHR: 1.231, 95% CI: 1.046–1.44) compared to those in the UHWTD group. In contrast, although participants in the NO UHWTD group showed higher rates of mortality from Chronic lower respiratory diseases, Cerebrovascular diseases, and Influenza and pneumonia compared to those in the UHWTD group in models adjusted for age, sex, and race, in fully adjusted models, this association was either not significant or only borderline significant.
Except for mortality related to Alzheimer’s disease and nephrosis, further considering the TAP water source did not weaken the strength of the association, as shown in Table 3. Consistent with the overall mortality trend, the “UHWTD & TAP from well” group exhibited the most substantial decrease in mortality rates from heart disease (aHR: 0.622, 95% CI: 0.478–0.811) and cancer (aHR: 0.791, 95% CI: 0.633–0.988).
UHWTD and volatile organic compounds in home tap water
A subset of participants underwent testing for volatile organic compounds (VOC) in their household tap water, with data provided in Supplementary Table 7 in Supplementary Material. In comparison to the non-UHWTD group, the UHWTD group exhibited significantly lower detection rates of Bromoform (P value:0.0120), Chloroform (P < 0.0001), Bromodichloromethane (P < 0.0001), and Dibromochloromethane (P < 0.0001). However, there was no significant difference in the detection rate of MTBE (methyl tertiary-butyl ether) (P value:0.7296) (Supplementary Fig. 2 in Supplementary Material).
UHWTD and lead exposure levels in NHANES
Although NHANES did not test for lead in tap water, some subjects were tested for lead levels in their blood and urine. In NHANES, subjects in the UHWTD group had significantly lower levels of lead in their blood and urine compared to those in the No UHWTD group (P < 0.0001). This trend still exists even after stratifying by age and gender. (Supplementary Fig. 3 in Supplementary Material).
Discussion
The long-term effects of household water treatment devices on health have not been adequately studied. In this context, we aim to investigate the relationship between the utilization of housing water treatment devices (UHWTD) and both overall and cause-specific mortality, in order to address the long-term impact of these devices on health.
Few prospective studies have examined the association between UHWTD and overall mortality. Our results indicate that individuals who did not utilize UHWTD (No UHWTD) had a higher risk of overall mortality, as well as mortality related to heart disease, cancer, Alzheimer’s disease, and nephrosis. These associations remained significant even after adjusting for potential confounding factors, including age, sex, and other covariates. These results are consistent with previous studies that have reported the potential benefits of water treatment devices in improving water quality and reducing health risks24. For instance, a population-based cohort study also reported a lower risk of gastrointestinal illness associated with the use of water treatment devices25. However, our study focuses on mortality outcomes and benefits from a longer follow-up period, providing valuable insights into the lasting impact of UHWTD utilization on overall and cause-specific mortality.
The link between drinking water and health originated from the recognition of pathogenic bacteria present in water. Water disinfection has played a crucial role in controlling the transmission of diarrheal and infectious diseases caused by these bacteria23,26. Furthermore, numerous previous studies have focused on examining the health effects of potentially harmful substances and disinfection by-products in water. For instance, the presence of aluminum and lithium in water has been associated with an increased risk of Alzheimer’s disease and mortality27,28, while the presence of arsenic in water may be linked to the development of ischemic heart disease and cancers29,30. Certain disinfection by-products like THMs have been identified as potential carcinogenic risks, and some PFAS have shown potential reproductive toxicity31. Additionally, emerging compounds found in water, such as microplastics and various novel organics, may have unknown health effects32,33. The utilization of the UHWTD can effectively reduce the presence of these toxic substances in both drinking water and household water, thereby making a significant contribution to overall health improvement. This observation partly explains why patients in the group without access to the UHWTD had poorer baseline health conditions.
Furthermore, our study uncovered a decreased detection rate of bromoform, chloroform, bromodichloromethane, and dibromochloromethane in tap water when UHWTD was employed, compared to No UHWTD. These chemicals are well-known disinfection by-products that can be found in water treated with chlorine or other disinfectants. The lower detection rate of these disinfection by-products in tap water when UHWTD was utilized suggests that these devices may effectively remove or reduce the levels of such contaminants, thus contributing to an overall improvement in water quality. These findings align with previous studies that have highlighted the potential benefits of water treatment devices in enhancing water quality and mitigating health risks. For instance, research has demonstrated that UHWTD can effectively eliminate or reduce contaminants like disinfection by-products, heavy metals, microplastics, and microbial pathogens from drinking water18,32,34,35,36. The lower detection rate of bromoform, chloroform, bromodichloromethane, and dibromochloromethane in tap water when UHWTD was utilized further supports the effectiveness of these devices in reducing the levels of disinfection by-products. We also examined the relationship between UHWTD and lead exposure. While NHANES did not specifically test for lead in tap water, certain individuals were tested for lead levels in their blood and urine. In the UHWTD group, lower levels of lead exposure were observed. This observation could potentially be attributed to the filtration of heavy metals, such as lead, in water by domestic water purification equipment.
The observed associations between UHWTD and reduced mortality risk may be attributed to several factors. Firstly, the use of UHWTD can help prevent exposure to potentially harmful contaminants present in the water supply. Disinfection by-products, for example, have been associated with adverse health effects such as increased cancer risk and reproductive issues12,37. By reducing the levels of these contaminants, UHWTD may contribute to improved health outcomes and reduced mortality. Furthermore, the utilization of UHWTD may also lead to improved water taste and odor, which can encourage individuals to consume more water. Adequate hydration is essential for maintaining overall health and preventing various health conditions38. Increased water consumption has been linked to a lower risk of cardiovascular disease, cancer, and kidney disease39,40. Therefore, the use of UHWTD may indirectly contribute to improved health outcomes through increased water intake.
Our research indicates that the utilization of domestic water treatment devices holds potential health benefits. These findings offer valuable insights and implications for integrating domestic water treatment equipment into policies for public health, sanitation, and water supply. Specifically, we have highlighted that home water treatment devices can offer additional health benefits beyond the prevention of diarrhea and infections, even in areas with reliable municipal water supply. This finding suggests that the evaluation of existing home water treatment devices should encompass a broader assessment of their hygienic and economic value, rather than solely focusing on the elimination of waterborne microorganisms. Furthermore, it is of utmost importance to emphasize the significance of adopting a health-focused approach to water resource management. After conducting a comprehensive evaluation of the economic value associated with household water treatment devices in terms of hygiene, governments may consider incorporating these devices into their public health strategies to better promote the health of their citizens.
Strengths and limitations of this study
The advantages of this study lie in its large sample size, national representativeness, high follow-up rate, and long-term mortality. Moreover, various potential confounding factors were adjusted or balanced to guarantee reliable results.
It is important to acknowledge some limitations of our study. Firstly, the utilization of household water treatment devices was self-reported, and we did not have detailed information on the specific types or quality of the devices used. This may introduce some measurement error and potential misclassification of exposure. Secondly, although we adjusted for several covariates, residual confounding cannot be completely ruled out. Other unmeasured factors or lifestyle variables may still influence the observed associations. Lastly, our study was conducted within the US population, and the generalizability of the findings to other populations or countries may be limited.
In conclusion, our study presents compelling evidence that the utilization of household water treatment devices significantly improved health outcomes. We observed a noteworthy reduction in the overall mortality risk, as well as mortality associated with specific causes such as heart disease, cancer, Alzheimer’s disease, and nephrosis. These findings emphasize the critical importance of considering water quality and highlight the potential benefits of incorporating household water treatment devices into public health strategies. However, further research is needed to validate these findings, unravel the underlying mechanisms, and assess the long-term effects on health. Collectively, our study contributes to the growing body of evidence supporting the potential of household water treatment devices in promoting public health and enhancing longevity. These findings offer valuable insights and have implications for future policies related to public health, sanitation, and family water supply.
Methods
Study population
The National Health and Nutrition Examination Survey (NHANES), conducted by the National Center for Health Statistics, is a comprehensive program aimed at assessing the health and nutritional status of individuals in the United States over a specific time period41. NHANES employs a complex, multistage, probability sampling method to gather nationally representative health-related data on the US population41. For the NHANES 1999–2010 survey, a total of 32,464 adults aged 20 and over participated. In this analysis, we excluded individuals who did not undergo a physical examination (n = 1712), those with missing information on housing water treatment devices (n = 359), and those with missing mortality data (n = 41). This resulted in a cohort of 30,322 participants for analysis (see Supplementary Fig. 1 in Supplementary Material). The mortality follow-up was a prospective study that assessed the vital status of all participants aged 20 and older until December 201942.
Ethical approval
Approval of the study from the National Center of Health and Statistics Research ethics review board was waived because the research relied on publicly used, de-identified secondary data. All participants signed informed consent forms before participated in NHANES.
Assessment of utilization of housing water treatment devices
All participants were asked whether they used any of the water treatment devices listed on the card (Supplementary Table 8 in Supplementary Material) in their homes. Additionally, they were asked to provide information about the source of tap water in their homes. Specifically, they were asked whether the water was supplied by a private or public water company, a private or public well, or another source.
Based on the utilization of household water treatment devices (UHWTD) and the source of tap water, we further categorized the exposure into four distinct categories: NO UHWTD & TAP from water company, NO UHWTD & TAP from well, UHWTD & TAP from water company, and UHWTD & TAP from well.
Definition of covariates
Baseline questionnaires were used to gather information on covariates, including age, sex, race/ethnicity, education level, smoking status, drinking habits, level of leisure time physical activity, and dietary intake. Additionally, family history of diabetes or heart attack, self-reported health status, and baseline history of diabetes, hypertension, cardiovascular disease, chronic obstructive pulmonary disease, and cancer were recorded in baseline questionnaires.
Volatile organic compounds in home tap water
Tap water samples collected from a subset of NHANES participants were analyzed to assess the levels of volatile organic compounds (VOCs). Specifically, the samples were tested for trihalomethanes (THMs) and the fuel additive methyl tertiary-butyl ether (MTBE). An automated analytical method employing headspace solid-phase microextraction coupled with capillary gas chromatography and mass spectrometry was utilized. This method enables the quantification of trace levels of THMs (including chloroform, bromodichloromethane, dibromochloromethane, and bromoform) and MTBE in tap water. For more comprehensive details regarding the testing methods, please visit the NHANES website41.
Lead exposure levels in blood and urine
Whole blood and Urine specimens are processed, stored, and shipped to the Division of Laboratory Sciences, National Center for Environmental Health, and Centers for Disease Control and Prevention for analysis. Whole blood lead concentrations and Urine lead concentration are determined using inductively coupled plasma mass spectrometry. For detailed testing details, please refer to NHANES website41.
Ascertainment of deaths
Baseline was defined as the time when participants underwent a physical examination, and our study examined two primary outcomes: all-cause mortality and cause-specific mortality from baseline until December 31st, 2019. To ascertain the death status of participants, we employed a unique study identifier and cross-referenced it with the National Death Index. For more detailed information regarding the matching method, please consult the resources provided by the National Center for Health Statistics43.
Statistical analysis
We accounted for the complex survey design factors of NHANES, including sample weights, clustering, and stratification, as specified in the instructions for utilizing NHANES data41. To compare baseline characteristics, we employed the Rao-Scott χ2 test for categorical variables and analysis of variance adjusted for sampling weights for continuous variables43.
Adjusted utilization rate estimates of a household water treatment devices were calculated for NHANES 1999–2010. The trend analysis was performed by combining data from three 4-year periods: 1999–2002, 2003–2006, and 2007–2010.
We defined baseline as the time when participants had their physical examinations. We counted person years from baseline to the date of death, loss to follow-up, or 31st December 2019, whichever came first. We used Cox proportional hazards models with time in study as the underlying time metric to calculate the hazard ratios and corresponding 95% confidence intervals for mortality in relation to UHWTD. In model 1, we included baseline age (continuous, in years), sex, and race/ethnicity (non-Hispanic white, non-Hispanic black, Mexican American, and others) as covariates. In model 2, we further incorporated education level (less than high school, high school or equivalent, and college or above), smoking status (never, former, and current smoker), drinking status (non-drinker, low to moderate drinker defined as <1 drink/day in women and <2 drinks/day in men, and heavy drinker defined as ≥1 drink/day in women and ≥2 drinks/day in men)44, family history of diabetes or heart attack, leisure time physical activity level (0, 1–2, or 3 times/week)45, dietary pattern represented by the healthy eating index scores (HEI-2015 in quarters)46, self-reported health status (very good to excellent, good, and poor to fair), as well as self-reported histories of diabetes, hypertension, cardiovascular disease, cancer (excluding skin cancer), and chronic obstructive pulmonary disease. The assumption of proportional hazards was assessed by creating a cross product of follow-up time and UHWTD patterns. Likelihood ratio tests comparing models with and without this variable did not yield statistically significant results, indicating no violation of the proportional hazards assumption.
Percentages of missing values of covariates were less than 5% except for drinking status (8.9%) and healthy eating index score (5.1%). We did multiple imputation for all missing values47. We also did stratified analyses and potential effect modifications by baseline age (<60 and ≥60 years), sex, educational level and smoking status.
To evaluate the effect on premature death, we examined the relations with deaths occurring before 65 years old, before 70 years old, before 75 years old, and before 80 years old among participants younger than 65 years old at baseline.
We conducted sensitivity analyses to assess the robustness of our results. Firstly, we performed complete case analyses by excluding participants with missing values for covariates. Additionally, we excluded patients with chronic diseases to account for the potential mediating effect of disease on the association between UHWTD utilization and mortality risk. Furthermore, we categorized participants based on different NHANES time periods to explore any potential variations over time.
We conducted all analyses using SAS 9.4, taking into account the complex sampling design. A two-tailed P value of <0.05 was considered statistically significant.
Data availability
The data that support the findings of this study are available from NHANES, [https://www.cdc.gov/nchs/nhanes]. Furthermore, the cleaned datasets that were analyzed in the current study are also available from the corresponding author upon reasonable request.
Code availability
The SAS code used in this article is available from the corresponding author.
References
United Nation, General comment no. 15 (2002), The right to water (arts. 11 and 12 of the International Covenant on Economic, Social and Cultural Rights). United Nation Agenda 11 (2002).
Bartram, J. & Cairncross, S. Hygiene, sanitation, and water: forgotten foundations of health. Plos Med. 7, e1000367 (2010).
Ashbolt, N. J. Microbial contamination of drinking water and disease outcomes in developing regions. Toxicology 198, 229–238 (2004).
Adelodun, B. et al. Assessment of socioeconomic inequality based on virus-contaminated water usage in developing countries: a review. Environ. Res. 192, 110309 (2021).
Sobsey, M. D. Managing water in the home: accelerated health gains from improved water supply. World Health 8, 1–83 (2004).
Kanbara, S. Nexus between water security framework and public health: a comprehensive scientific review. Water 13, 1365 (2021).
Clasen, T. Household water treatment and safe storage to prevent diarrheal disease in developing countries. Curr. Environ. Health Rep. 2, 69–74 (2015).
Gundry, S., Wright, J. & Conroy, R. A systematic review of the health outcomes related to household water quality in developing countries. J. Water Health 2, 1–13 (2004).
Luby, S. P. et al. Combining drinking water treatment and hand washing for diarrhoea prevention, a cluster randomised controlled trial. Trop. Med. Int. Health 11, 479–489 (2010).
Wolf, J. et al. Effectiveness of interventions to improve drinking water, sanitation, and handwashing with soap on risk of diarrhoeal disease in children in low-income and middle-income settings: a systematic review and meta-analysis. Lancet 400, 48–59 (2022).
Kremer, M., Luby, S., Maertens, R., Tan, B. & Wicek, W. Water Treatment and Child Mortality: A Meta-analysis and Cost-effectiveness Analysis. Social Science Electronic Publishing, https://doi.org/10.2139/ssrn.4071953 (2023).
Richardson, S. D., Plewa, MJ., Wagne, E. D., Schoeny, R. & DeMarini, DM. Occurrence, genotoxicity, and carcinogenicity of regulated and emerging disinfection by-products in drinking water: a review and roadmap for research. Mut. Res. 636, 178–242 (2007).
Schuebler, M. Pharmaceuticals in the environment: sources, fate, effects and risks. Clean 37, 514–514 (2009).
Chohan, A. et al. Per and polyfluoroalkyl substances scientific literature review: water exposure, impact on human health, and implications for regulatory reform. Revi. Environ. Health 36, 235–259 (2021).
Hu, X. C. et al. Detection of poly- and perfluoroalkyl substances (PFASs) in US drinking water linked to industrial sites, military fire training areas, and wastewater treatment plants. Environ. Sci. Tech. Lett. 3, 344–350 (2016).
Levallois, P., Barn, P., Valcke, M., Gauvin, D. & Kosatsky, T. Public health consequences of lead in drinking water. Curr. Environ. Health Rep. 5, 255–262 (2018).
Hanna-Attisha, M., LaChance, J., Sadler, R. C. & Champney Schnepp, A. Elevated blood lead levels in children associated with the flint drinking water crisis: a spatial analysis of risk and public health response. Am. J. Public Health 106, 283–290 (2016).
Qasem, N. A. A., Mohammed, R. H. & Lawal, D. U. Removal of heavy metal ions from wastewater: a comprehensive and critical review. npj Clean Water, https://doi.org/10.1038/s41545-021-00127-0 (2023).
Wang, J. et al. Novel RO membranes fabricated by grafting sulfonamide group: Improving water permeability, fouling resistance and chlorine resistant performance. J. Membr. Sci. 641, 119919 (2022).
Babu Ponnusami, A. et al. Advanced oxidation process (AOP) combined biological process for wastewater treatment: a review on advancements, feasibility and practicability of combined techniques. Environmental research 237, 116944 (2023).
Kozisek, F. Health risks from drinking demineralised water. Nutr. Drinking Water 1, 148–163 (2005).
World Health Organization. Calcium and Magnesium in Drinking-water: Public Health Significance. xi, 180 (Geneva, Switzerland: World Health Organization, 2009).
Mebrahtom, S., Worku, A. & Gage, D. J. The risk of water, sanitation and hygiene on diarrhea-related infant mortality in eastern Ethiopia: a population-based nested case-control. Bmc Public Health 22, 343 (2022).
Yang, H., Wang, J. B., Wang, X. K., Fan, J. H. & Qiao, Y. L. Association between type of drinking water and upper gastrointestinal cancer incidence in the Linxian General Population. BMC cancer 23, 397 (2023).
Tornevi, A., Simonsson, M., Forsberg, B., Save-Soderbergh, M. & Toljander, J. Efficacy of water treatment processes and endemic gastrointestinal illness - A multi-city study in Sweden. Water Res. 102, 263–270 (2016).
Crump, J. A. et al. Household based treatment of drinking water with flocculant-disinfectant for preventing diarrhoea in areas with turbid source water in rural western Kenya: cluster randomised controlled trial. BMJ 331, 478 (2005).
Fajardo, V. A., Fajardo, V. A., LeBlanc, P. J. & MacPherson, R. E. K. Examining the relationship between trace lithium in drinking water and the rising rates of age-adjusted Alzheimer’s disease mortality in Texas. J. Alzheimers Dis. 61, 425–434 (2018).
Huicho, L. et al. Drivers of the progress achieved by Peru in reducing childhood diarrhoea mortality: a country case study. J. Glob. Health 9, 020805 (2019).
Marshall, G. et al. Fifty-year study of lung and bladder canceir mortality in Chile related to arsenic in drinking water. J. Natl Cancer Institute 99, 920–928 (2007).
Greco, S. L., Belova, A., Haskell, J., & Backer, L. Estimated burden of disease from arsenic in drinking water supplied by domestic wells in the United States. J. Water Health 17, 801–812 (2019).
Winchell, L. J. et al. Per- and polyfluoroalkyl substances presence, pathways, and cycling through drinking water and wastewater treatment. J. Environ. Eng. 148, 03121003 (2022).
Kasprzyk-Hordern, B., Dinsdale, R. M. & Guwy, A. J. The removal of pharmaceuticals, personal care products, endocrine disruptors and illicit drugs during wastewater treatment and its impact on the quality of receiving waters. Water Res. 43, 363–380 (2009).
Simate, G. S., Iyuke, S. E., Ndlovu, S., Heydenrych, M. & Walubita, L. F. Human health effects of residual carbon nanotubes and traditional water treatment chemicals in drinking water. Environ. Int. 39, 38–49 (2012).
Moustafa, T. M. Removal of pathogenic bacteria from wastewater using silver nanoparticles synthesized by two fungal species. Water Sci. 31, 164–176 (2017).
Krueger et al. Drinking water source and human Toxoplasma gondii infection in the United States: a cross-sectional analysis of NHANES data. BMC Public Health 14, 711 (2014).
Shen, M., Song, B., Zhu, Y., Zeng, G. & Yi, H. Removal of microplastics via drinking water treatment: current knowledge and future directions. Chemosphere 251, 126612 (2020).
Villanueva, C. M. Meta-analysis of studies on individual consumption of chlorinated drinking water and bladder cancer. J Epidemiol. Community Health 57, 166 (2003).
Popkin, B. M., D’Anci, K. E. & Rosenberg, I. H. Water, hydration, and health. Nutri. Rev. 68, 439–458 (2010).
Jacqueline, C., Knutsen, S. F., Blix, G. G., Lee, J. W. & Fraser, G. E. Water, Other Fluids, and Fatal Coronary Heart Disease The Adventist Health Study. Am. J. Epidemiol. 155, 827–833 (2002).
Matsushita, K. Association of estimated glomerular filtration rate and albuminuria with all-cause and cardiovascular mortality in general population cohorts : a collaborative meta-analysis. Lancet 375, 2073–81 (2010).
Centers for Disease Control and Prevention. About the National Health and Nutrition Examination Survey, https://www.cdc.gov/nchs/nhanes/about_nhanes.htm (2023).
National Center for Health Statistics. 2019 Public-Use Linked Mortality Files, https://www.cdc.gov/nchs/data-linkage/mortality-public.htm (2023).
Rao, J. N. K. & Scott, A. J. On chi-squared tests for multiway contingency tables with cell proportions estimated from survey data. Ann. Stat. 12, 46–60 (1984).
Chen, F. et al. Association among dietary supplement use, nutrient intake, and mortality among U.S. adults: a cohort study. Ann. Intern. Med. 170, 604–613 (2019).
Piercy, K. L. et al. The physical activity guidelines for Americans. JAMA 320, 2020–2028, (2018).
National Cancer Institute. Developing the Healthy Eating Index, https://epi.grants.cancer.gov/hei/developing.html (2023).
Yuan, Y. Multiple imputation using SAS software. J. Stat. Softw. 45, 1–25 (2011).
Acknowledgements
We thank Chen Chen (Department of Epidemiology, School of Public Health, University of Michigan, Ann Arbor, MI, USA), for providing the Statistical consultation for this research work. This work was supported by the National Natural Science Foundation of China (Grants 82370700,82170701, 82370699 and 81974086) to R.Z. and Y.Y. The funder had no influence on study design, data collection and analysis, decision to publish or preparation of the manuscript.
Author information
Authors and Affiliations
Contributions
Study concept and design: S.W. Huang, H.L. Zhou, R. Zeng, Y. Yao; Acquisition of data: S.W. Huang, H.L. Zhou, R. Zeng, Y. Yao; Analysis and interpretation of data: S.W. Huang, H.L. Zhou, R. Zeng, Y. Yao; Drafting of the manuscript: S.W. Huang, R. Zeng; Critical revision of the manuscript for important intellectual content: S.W. Huang, H.L. Zhou, R. Zeng, Y. Yao. All authors contributed to subsequent editing and revising of the study manuscript. S.W. Huang and H.L. Zhou have contributed equally and are joint first authors. Y. Yao is the study guarantor and attests that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Huang, SW., Zhou, HL., Zeng, R. et al. Associations of the utilization of household water treatment devices with mortality. npj Clean Water 7, 5 (2024). https://doi.org/10.1038/s41545-024-00300-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41545-024-00300-1
