
Abstract
The United Nations’ Sustainable Development Goal (SDG) 3.9 calls for a substantial reduction in deaths attributable to PM2.5 pollution (DAPP). However, DAPP projections vary greatly and the likelihood of meeting SDG3.9 depends on complex interactions among environmental, socio-economic, and healthcare parameters. We project potential future trends in global DAPP considering the joint effects of each driver (PM2.5 concentration, death rate of diseases, population size, and age structure) and assess the likelihood of achieving SDG3.9 under the Shared Socioeconomic Pathways (SSPs) as quantified by the Scenario Model Intercomparison Project (ScenarioMIP) framework with simulated PM2.5 concentrations from 11 models. We find that a substantial reduction in DAPP would not be achieved under all but the most optimistic scenario settings. Even the development aligned with the Sustainability scenario (SSP1-2.6), in which DAPP was reduced by 19%, still falls just short of achieving a substantial (≥20%) reduction by 2030. Meeting SDG3.9 calls for additional efforts in air pollution control and healthcare to more aggressively reduce DAPP.
Similar content being viewed by others

Introduction
PM2.5 pollution—particulate matter smaller than 2.5 μm in diameter suspended in the air—is one of the largest environmental risk factors for public health and has been implicated in various respiratory and cardiovascular diseases1,2. Deaths caused by exposure to ambient PM2.5 pollution, termed deaths attributable to PM2.5 pollution (DAPP)3,4, numbered more than 4 million in 2019 worldwide5, more than double the total reported deaths (~2 million) from COVID-19 in 20206. Against this backdrop, the United Nations’ Sustainable Development Goal (SDG) 3.9 obliges signatories to “by 2030, substantially reduce the number of deaths and illnesses from hazardous chemicals and air, water and soil pollution and contamination1,7”. Within the total deaths related to air pollution (generally considered PM2.5 and ozone), DAPP accounts for more than 95%8,9. Hence, understanding future trends in DAPP and the relative influence of key drivers is of great importance for environmental policy and public health management.
DAPP is jointly driven by interactions between atmospheric PM2.5 concentration, population size, population age structure, and the healthcare (presented as death rate of diseases), which in turn, are affected by socioeconomic development and climate change (Fig. 1). Specifically, socioeconomic development directly influences the total population, age structure, and healthcare standards10,11, and has an indirect effect on PM2.5 concentration via the emission of airborne pollutants from the manufacturing, energy, and transport sectors12,13. Climate change can also affect PM2.5 concentration by influencing wind, precipitation, and other parameters which determine the transport and evolution of pollutants14,15. Socioeconomic development and climate change are also complexly interrelated16.

Socioeconomic development pathways can lead to changes in population, age structure, death rate of diseases, and PM2.5 concentration. Note that PM2.5 concentration is jointly determined by emissions and climatic conditions which are both a product of complex interactions between socioeconomic development and climate change.
While a few studies have projected future DAPP, estimates vary widely, with some studies showing opposite trends (Table S1). For instance, Lelieveld et al. 17 and Rafaj et al. 18 projected future increases in DAPP, while West et al. 19 and Silva et al. 15 projected declines. These studies have mainly focused on the effects of changes in PM2.5 concentration on DAPP, while other influential factors have either been held constant or estimated via projections from bespoke scenario frameworks. For example, some studies have assumed a constant death rate of diseases or age structure to isolate the effect of future air quality change on DAPP17,20, while other studies used projected PM2.5 concentration based on climate scenarios but assumed trends in demographic factors or death rate of diseases from ad hoc projections15,21. This lack of internal consistency in scenario assumptions cannot reliably capture relative effects of or the interactions between driving factors15,19,22 and can lead to inconsistent and even contrasting results. Furthermore, Yang et al. 23 projected DAPP under an integrated scenario framework which simulated PM2.5 concentration from a single atmospheric model (GFDL-ESM4.1), hence the results are limited in capturing the range of variation in PM2.5 concentration and the corresponding DAPP under climate change15. With less than 7 years to go to achieve the SDGs, a comprehensive projection of global DAPP at high spatial resolution, using multiple models and considering each driving factor and the inherent uncertainty in a coherent and internally consistent way is both essential and urgent.
In this study, we aimed to produce an integrated, comprehensive, and coherent suite of projections of future DAPP by using future PM2.5 concentration based on 11 available models (see details in Methods) and CMIP6 (Coupled Model Intercomparison Project Phase 6) climate change projections under the latest Scenario Model Intercomparison Project (ScenarioMIP) framework (Table 1). We considered four integrated scenarios represented as SSP x–y (i.e., Sustainability (SSP1-2.6); Middle of the Road (SSP2-4.5); Regional Rivalry (SSP3-7.0), and Fossil-fueled Development (SSP5-8.5)) in exploring the potential to achieve SDG3.9 by substantially reducing DAPP for 154 countries worldwide (Figure S1), where x represents societal conditions described by Shared Socioeconomic Pathway (SSP) and y represents the degree of climate forcing under the Representative Concentration Pathway that is consistent with SSP emissions24. First, we projected global DAPP from 2015 (adoption of the UN Agenda 2030) to 2050 by combining an epidemiological model with all driving factors under the ScenarioMIP framework (Figure S2) and assessed the attainment of SDG3.9 at three levels of ambition (10, 20, and 30% reduction compared to 2015 levels). We then identified the relative contributions of changes in PM2.5 concentration, population size, age structure, and death rate of diseases on DAPP using the decomposition method (Figure S18). Lastly, we explored alternative pathways to meet SDG3.9 by leveraging additional effort in air pollution control (20% lower PM2.5 concentration) and healthcare improvement (20% lower death rate of diseases) (see details in Methods). The results are crucial for informing national-level investment and policy for teaming climate change mitigation, air pollution control, and healthcare to substantially reduce global DAPP.
Results
Trends in DAPP under different scenarios and the attainment of SDG3.9
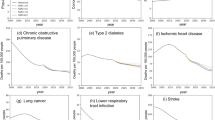
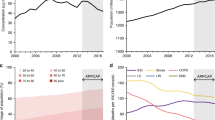
The multi-model average results indicate that global DAPP was substantially reduced only under those scenarios with the most ambitious assumptions around continuing growth and aging in the global population and declines in death rates of diseases (Figure S15). Thus, achieving SDG3.9 remains a great challenge. The SSP1-2.6 scenario saw the largest decrease, with average DAPP projected to almost meet the moderate target (i.e., a 20% reduction compared to 2015 levels) by 2030 (−19%) and exceed the target by 2050 (−24%). Under all other scenarios, the moderate target of SDG3.9 was not achieved. Average DAPP also declined (−11% by 2030 and −7% by 2050) under the SSP5-8.5 scenario, but remained stable under the SSP2-4.5 scenario (−1% by 2030 and +2% by 2050). In the worst case, average DAPP grew 14% by 2030 and 32% by 2050 under SSP3-7.0 (Fig. 2a). Among different age groups, the share of DAPP for older people (65 + ) accounted for almost 65% in 2015 and rose to 70% under all scenarios by 2030 because older adults have a higher baseline death rate and are more vulnerable to almost all types of health risk (Figure S5).

a Changes in DAPP at the global scale, b–f regional scale. Solid lines represent the average estimates and shading indicates the 95% confidence interval derived from uncertainty in future PM2.5 concentration (derived from 11 climate and earth system models) and the death rate of diseases (derived from the statistic model). See details in Supplementary Notes 2-4. The abbreviation is defined as ASIA Asian with the exception of the Middle East, Japan, and Former Soviet Union states. MAF Middle East and Africa. LAM Latin America and the Caribbean. OECD Organization for Economic Co-operation and Development and new European Union and candidates. REF reforming economies of Eastern Europe and the former Soviet Union.
Middle East and Africa (MAF) and Latin America and the Caribbean (LAM) were hotspots of future growth in DAPP, increasing between 11% (SSP1-2.6) and 101% (SSP3-7.0) by 2030, and between 13% (SSP1-2.6) and 105% (SSP3-7.0) by 2050, respectively. SDG3.9 achievement in these regions is not expected in the future (Fig. 2c, e). In contrast, DAPP in the member states of the Organization for Economic Co-operation and Development and new European Union and candidates (OECD) and the reforming economies of Eastern Europe and the Former Soviet Union (REF) tended to decrease under most scenarios. The OECD met the moderate SDG3.9 target under SSP1-2.6 by 2030 and 2050 while REF even achieved the ambitious target (30% reduction) (Fig. 2d, f).
Future trends in PM2.5 concentrations among different CMIP6 general circulation models differed in both magnitude and sign because of their differences in natural emissions, chemical mechanisms, and processes. The multi-model average DAPP was estimated based on all available models to provide a general trend (see details in Methods). To further encompass the uncertainties among the 11 models, we also calculated the model-specific trend in DAPP (Figure S9) and found that most models yielded results similar to the average estimates (calculated based on all available models). Although some models (e.g., MIROC-ES2L, INM-CM5-0) displayed a steeper decline in DAPP, the moderate SDG3.9 target was not achieved by 2030 for any scenario except SSP1-2.6 (Figure S4; Table 2). Considering some models were scenario-specific, to ensure consistency, we also presented the average results calculated based on the eight models with estimates for all scenarios, which was highly in line with average results from all available models.
Achieving the moderate SDG3.9 target was also a challenge at national scale. According to the multi-model average DAPP, more than two-thirds of the world’s nations (107/154) did not meet the moderate target by 2030 under any scenario (Fig. 3), including over 80% of countries in LAM and MAF, and more than 70% of countries in ASIA (Table S2). Even by 2050, although the number of countries achieving the moderate SDG3.9 target varied slightly over time, substantially reducing DAPP remained a challenge for most countries (Fig. 3). When loosening the definition of a “substantial reduction” to a 10% reduction (i.e., the weak target), the challenge to meet SDG3.9 remained with over 50% of nations (87/154) failing to meet SDG3.9 by 2030 under any scenario, and when tightening (30%) the target (i.e., the ambitious target), 80% of nations (127/154) failed (Fig. 3).

The colors indicate percentages of countries that can meet SDG3.9 under 0, 1, 3, 2, and 4 possible scenarios assessed with, weak, moderate, and ambitious settings for SDG3.9 represented as 10%, 20%, and 30% reduction in DAPP relative to 2015, respectively. Only 8 models that were available for all the 4 scenarios were included in the model-specific analysis.
While considering the variation among different models, the finding many countries cannot achieve SDG3.9 under any scenario was robust. Even when considering the relatively loose standard for SDG3.9 (i.e., a 10% reduction) and the model with the most aggressive PM2.5 pollution reduction (MIROC-ES2L), more than one-third of nations failed to achieve a substantial reduction in DAPP. This proportion rose to 55% and 69% when tightening the target to moderate (i.e., 20%) and ambitious (i.e., 30%).
Within regions, substantial spatial heterogeneity occurred (Fig. 4), with global concentrations in DAPP coinciding with the major global urban centers where dense populations co-exist with the major sources of PM2.5 pollution (i.e., traffic networks, power generation, heavy industry). For example, under the Middle of the Road scenario (SSP2-4.5), northern India had the largest growth in DAPP which included the megacities of Delhi and Kolkata. Similarly, the largest city in South America—Sao Paulo in Brazil—also saw a large growth in DAPP.

Effects of individual factors on the attainment of SDG3.9
Trends of DAPP can be disentangled into the net effects of changes in PM2.5 concentration which reflects the risk factor itself, and population, age structure, and death rate of diseases which alter the size and vulnerability via decomposition analysis (see Methods for details). Population aging was the dominant factor under all scenarios in driving growth in DAPP, causing an increase of 34% (SSP3-7.0) to 41% (SSP5-8.5) by 2030. Conversely, healthcare improvement was the strongest factor driving down DAPP, leading to a decline of 36% (SSP3-7.0) to 44% (SSP5-8.5). As socioeconomic development reduced the death rate of diseases and exacerbated population aging simultaneously, these two drivers tended to offset each other, resulting in a relatively minor net decrease of around 1 to 3% (Fig. 5). This counteracting effect also influenced the age distribution of DAPP. The share of DAPP amongst older people (65 + ) increased from almost 65% in 2015 to around 70% under all scenarios by 2030 due to the increase in older adults and better healthcare (Figure S5). Population growth led to a minor increase in DAPP of around 6% (SSP1-2.6) to 14% (SSP3-7.0).

a–d the cumulative effect of four factors: population, age structure, death rate, and PM2.5 concentration, under SSP1-2.6, SSP2-4.5, SSP3-7.0, and SSP5-8.5, respectively. Data represents the mean value and error bars represent the projections based on the 95% confidence intervals of future PM2.5 concentration (derived from 11 climate and earth system models) and the death rate of diseases (derived from a statistical model). See details in Supplementary Notes 2-4.
Compared with other driving factors, the effect of PM2.5 concentration was more variable across scenarios. For instance, DAPP in 2030 was projected to decrease by 24% relative to 2015 because of the decline in PM2.5 concentration alone under SSP1-2.6, led by the effort in climate mitigation and strong air pollution control. Similarly, air quality improvement was responsible for a decline of 15% and 8% in DAPP under SSP5-8.5 (strong air pollution control and high energy demand) and SSP2-4.5 (moderate air pollution control and moderate energy demand), respectively. Under the worst scenario for air pollution (SSP3-7.0) which assumes a weak air pollution control with slow socioeconomic development, DAPP was projected to increase by 2% due to a 12% increase in PM2.5 concentration relative to 2015 (Fig. 5; Figure S15). As the relationship between PM2.5 concentration and health effects represented by exposure-response curves is non-linear, DAPP tended to show a steeper increase at lower concentrations and leveled off at higher concentrations (Figure S3). Hence, a lower level of PM2.5 concentration in the future would substantially reduce DAPP. For example, under SSP1-2.6 a decrease in PM2.5 concentration of 31% led to a 24% decrease in DAPP from 2015 to 2030; whereas under SSP5-8.5, a growth of 12% in PM2.5 concentration led to a 2% increase in DAPP (Fig. 5).
Similar patterns in driving factors occurred beyond 2030 at the global scale. Aging and healthcare improvement remained the dominant driving factors affecting DAPP and the attainment of SDG3.9 while the effect of PM2.5 concentration varied among scenarios. The effect of population growth between 2030 and 2050 was smaller relative to that from 2015 to 2030 because population growth was slower.
Detailed region- and country-specific decomposition were also conducted (Figure S19-20). For most countries, changes in aging and healthcare were the main contributors to DAPP but the interaction of other driving factors also had an influence. For instance, DAPP in China declined over time and met moderate or ambitious SDG3.9 targets under all scenarios except SSP3-7.0 because of low population growth and decreasing PM2.5 concentration. Conversely, DAPP in India tended to increase in most scenarios driven by population growth and relatively modest and slow air quality improvement.
Meeting SDG3.9 via additional pollution control and healthcare advances
Amongst the four driving factors that shape DAPP, PM2.5 concentration and death rate of diseases are more readily modified via policy measures such as incentives, regulation, and investment in technology research, development, and implementation. Hence, we conducted a sensitivity analysis to explore the ability to meet SDG3.9 via additional efforts in air pollution control and healthcare (see details in Methods).
The results indicate that advances in air pollution control and healthcare can make important contributions towards achieving a substantial reduction in DAPP. When PM2.5 concentration was set at 20% lower (i.e., moderate SDG3.9 target) than the projected value under different scenarios, a substantial reduction (-29%) in global DAPP was achieved under SSP1-2.6 by 2030. Under SSP5-8.5, a decrease in DAPP of 21% was achieved. When the death rate of diseases was set at 20% lower than the projected value, the moderate SDG3.9 target was met under most scenarios except SSP3-7.0. With both measures in place (i.e., a 20% lower PM2.5 concentration and a 20% lower death rate of diseases), large reductions in DAPP were achieved (Fig. 6a).

a, b Relative change in deaths attributable to PM2.5 pollution from 2015 to 2030 and 2050. c, d Percentage of countries meeting moderate SDG3.9 by 2030 and 2050 (calculated based on 154 countries). Colors in the legends indicate a 20% lower PM2.5 concentration (green) and death rate of diseases (blue) relative to the projected value because of additional improvements in air pollution control and healthcare. The data represent the mean value and error bars represent 95% confidence intervals, calculated based on the upper and lower intervals of future PM2.5 concentration (derived from 11 climate and earth system models) and the death rate of diseases (derived from statistic model). See details in Supplementary Notes 3-4. A similar reduction was also adopted to the upper and lower intervals when considering the additional improvement.
Thus, the challenge to substantially reduce DAPP for countries requires substantial advances in both healthcare and air pollution control which can boost the reduction of DAPP for countries that did not meet SDG3.9 under the original ScenarioMIP scenarios. By combining PM2.5 concentrations and the death rate of diseases at 20% lower than the projected values, the number of countries that met SDG3.9 more than doubled relative to the original projections, and almost 90% of the world’s nations can achieve the moderate SDG3.9 target under SSP1-2.6 by 2030 (Fig. 6c). Details of the potential pathways for each country to meet the moderate SDG3.9 target by considering additional improvement in healthcare and air pollution control can be found in Figure S21.
Discussion
Several studies have assessed the trends in DAPP including dynamic PM2.5 concentration levels, population structure and aging, and death rates of diseases based on various scenarios (including SSP-RCP scenarios) (Table S1). However, a lack of internally consistent, comprehensive scenario analyses has led to wide variations in future projections of DAPP which differ not only in magnitude but also in sign, potentially resulting in divergent interpretations and policy responses. As a response, a major contribution of this study is providing a comprehensive long-term projection of DAPP with all 11 available simulations from CMIP6 under the latest ScenarioMIP framework, which provides ensembles of integrated, internally consistent estimates for the drivers of DAPP (population, age structure, death rate of diseases, and air quality)25. Thus, our projections used internally consistent assumptions around driving factors15 to improve the accuracy and robustness of projections. Compared with another study23 that did project DAPP using coherent and internally consistent assumptions for each relevant factor under the ScenarioMIP framework with PM2.5 concentration simulated by GFDL-ESM4.1, our study also provides all available CMIP6 general circulation models. In addition, estimation based on a well-established scenario framework also makes our results comparable with other studies under the SSPs and CMIP6 framework and estimates the trends in DAPP under different climate change and socioeconomic pathways. This can further support integrated decision-making by jointly considering the results from multiple fields26,27.
This work also attempted to assess potential future progress and development pathways towards SDG3.9 and does so on multiple scales: global, regional, national, and by grid cell at a spatial resolution of 1 degree. The results shed light on guiding future air pollution control policy and healthcare improvement and provide the robust projections required to support the management of health impacts caused by PM2.5 pollution for the scientific community and stakeholders.
Achieving SDG3.9 requires additional efforts in air pollution mitigation and healthcare beyond the SSP storylines. Global DAPP will not be substantially reduced under all but the most ambitious scenarios (SSP1-2.6) because of the overwhelming effect of population aging (Fig. 3). However, there are complex interactions between drivers under different scenarios which must be considered in terms of the net overall effect on DAPP. For instance, with socioeconomic development, the death rate of diseases declines reduces population vulnerability, but population aging simultaneously increases the size of vulnerable populations11,28. Hence, while scenarios with high population aging (SSP1-2.6 and SSP5-8.5) counterintuitively showed a greater reduction in DAPP, this was driven by the effect of population aging being offset by improvement in healthcare in these scenarios. Besides the improvement in healthcare, change in PM2.5 concentration is also a key driver of reducing DAPP. SSP1-2.6 had the largest reduction because of the underlying assumption of a cleaner energy mix and strong air pollution control. However, PM2.5 concentration is also expected to reduce in SSP5-8.5. That is because of the strong air pollution control led by the adoption of the current best available technology (especially end-of-pipe control) and strong socio-economic development based on high energy demand and fossil fuel dominated energy mix. Hence, socioeconomic transformation towards a more sustainable future aligned with SSP1-2.6 with stronger air quality control and less fossil fuel dependence is the better pathway for reducing DAPP (Fig. 5, Figure S9) as it has positive co-benefits for many other SDGs that are not assessed in this study.
In addition, the interaction between different drivers varied by region. For instance, besides population aging, population growth in MAF also played a considerable role under all scenarios because the region’s population is relatively young and growing fast. While in LAM and ASIA, aging is the dominant driver of growth in DAPP (Figure S19). Different countries also exhibited heterogeneity in mechanisms driving DAPP. For instance, China is likely to achieve SDG3.9 under most scenarios because of the reversal of population growth and the declining trend of PM2.5 pollution, as well as healthcare improvement. While for India, DAPP tended to increase under three scenarios (all bar SSP1-2.6) mainly because of the joint effect of air quality deterioration and demographic change.
With the challenge in the reduction of DAPP, meeting SDG3.9 needs strong additional policies and investment in air pollution control and healthcare. While considering the additional improvement in air quality and healthcare alone, weak and moderate SDG3.9 targets can be achieved under SSP2-4.5, and while combining both 20% lower PM2.5 concentration and death rate of diseases, even an ambitious SDG3.9 target (i.e., a 30% reduction in DAPP) can almost be achieved. Under the most ideal settings combining SSP1-2.6, an additional 20% lower death rate of diseases, and 20% lower PM2.5 concentration, the more ambitious target for SDG3.9 can be exceeded by 2030 with a decrease in DAPP of 43%.
ScenarioMIP provided an ensemble description of feasible futures with integrated transitions across multiple sectors including pollution control, energy structure, emissions reduction, technology innovation, and socioeconomic development (Table 1). Beyond the measures incorporated in the SSP-based narratives, extra efforts to control air pollution need to be implemented if SDG3.9 is to be achieved, such as promoting end-of-pipe devices, replacing fossil fuel with renewable electricity, and improving efficiency via technology upgrade29,30,31. An additional decrease in the death rate of disease can be achieved by measures such as strengthening the investment in the health system, building a health monitoring system for older people, and increasing medical accessibility through financial support and allied services provision32,33,34.
Due to the heterogeneity in pathways to reduce air pollution and improve healthcare, countries also need different strategies to meet SDG3.9 (Figure S21). For countries like China where it is feasible to meet SDG3.9 by following the basic scenarios, future development aligned with less fossil fuel dependency and with more stringent pollution controls (i.e., SSP1-2.6) is needed. In countries like India that cannot meet SDG3.9 under any of the basic scenarios, more investment in emissions reduction and healthcare improvement are needed. Moreover, many developing countries in MAF and LAM face great challenges to meeting SDG3.9 under most scenarios even with additional improvements in healthcare and air pollution control. These countries will need more assistance from developed countries (such as high-income countries identified by the World Bank) in technology, medicine, and finance. Finally, even for the countries that meet SDG3.9 under most scenarios, efforts in air quality control and emissions abatement can be helpful to boost the well-being of residents and offset potential medical expenditure34,35,36,37. Cost-effectiveness and technological feasibility should also be considered. Strategies like pricing carbon and pollutant emissions using market-based policy could be a feasible way to help developing countries encourage innovation38.
Stronger efforts in air pollution control and healthcare are also co-beneficial for achieving several other SDGs. Efforts in air pollution control are in line with mitigation and adaptation commitments in SDG13 (Climate Action)39,40 and promote progress toward many other aspects of sustainability. Hence, comprehensive policies that team up air pollution control and public health with climate change mitigation efforts, technological innovation, and energy system overhaul could help meet multiple SDGs41,42,43.
A few key limitations and uncertainties remain in our study. Firstly, in estimating DAPP, although we used the latest method from GBD 20195, the epidemiological model cannot differentiate the interactive effects between PM2.5 pollution and other closely related risk factors (e.g., climate change-induced heatwaves, ozone pollution) and consideration of these effects is required in future analyses44,45. As our model reflected the long-term effects of PM2.5, and estimated DAPP based on annual PM2.5 concentration, the short-term effects associated with acute cardiovascular and respiratory diseases were not considered46. Further estimations of DAPP considering short-term epidemiological studies are needed in the future47. In addition, because of a lack of indoor PM2.5 data, our study did not differentiate the interaction between ambient and indoor PM2.548, but this limitation does not influence our major findings or conclusions.
Secondly, the choice of data sources for quantifying the driving factors and the exposure-response curve used both introduce uncertainty into DAPP projection49. Regarding PM2.5 concentration, there are several potential explanations for the discrepancy between the 11 CMIP6 models, including differences in the treatment of aerosols and their components (e.g., organic aerosols and emission of biogenic volatile organic compounds) as well as the effect of climate change (i.e., temperature and precipitation) simulated by models and its impact on natural aerosol emissions50. To account for this variation, we presented model-specific (Figure S9) as well as multi-model average results with ranges (Figure S15-16) reflecting uncertainty in future PM2.5 concentration. Regarding the exposure-response function, we used the Bayesian, regularized, trimmed (MR-BRT) model following GBD2019 (see details in Methods), and presented the results derived from the middle value, and the upper and lower estimates was also conducted to quantify the range of uncertainty (Figure S7-8, Figure S22). Some studies also found a potential shortcoming of the MR-BRT model in that the saturation of relative risk at high PM2.5 tends to be more pronounced. More comprehensive sensitivity analyses considering other exposure-response functions (e.g., Global Exposure Mortality Model and Fusion model) are needed in the future to more thoroughly explore the influence of this modeling choice51. Considering the availability of data, projections of death rate of diseases and age structure in this study were conducted at the national level, which generalizes the heterogeneity within countries, an effect which may be critical especially in large and populous countries (e.g., United States, China, India). While we do not provide a detailed exploration of the results at the national-level here, further analyses of trends and driving mechanism for individual countries may be undertaken based on the Supplementary Information provided to support decision-making of communities and stakeholders at regional and local scales52,53,54.
Thirdly, our projections were conducted under the ScenarioMIP framework, which reflected possible future socioeconomic and climate trajectories. The results should be treated as projections based on interactions among different driving factors, rather than as forecasts. Our study cannot reflect the effects caused by abrupt socioeconomic, geopolitical, or environmental changes (such as war or pandemic disease)55,56,57 or specific emissions control actions (such as China’s Air Pollution Control Policy implemented in 2013) on DAPP58. In the future, strategies to meet SDG3.9 can be explored by considering specific policy implementations29,38 and using detailed emissions inventories17,35,59.
Finally, we set a series of standards for all countries (i.e., 10, 20, and 30%) to reflect the challenges of meeting SDG3.9 globally. Although they are uniform in proportion, the absolute numbers of DAPP are country-specific. Similar to the air quality targets proposed by WHO (2021)60, countries can further specify their own targets of SDG3.9 based on our analyses to suit their socioeconomic development stage. When analyzing the additional improvement in healthcare and air pollution control, we used simple scenarios which generalize the complex interactions among socioeconomic development, healthcare, and aging. Policy efforts towards lowering PM2.5 concentrations and improving baseline mortality rates are far more achievable via policymaking than other measures for reducing DAPP such as lowering population aging and hence, these intervention scenarios can provide general insights into the scale of response of DAPP required to meet SDG3.9. This simplification should be interpreted as a sensitivity analysis and may underestimate DAPP. More specific target setting and exploration of pathways by country considering emissions, energy structure, socioeconomic development, and political factors are needed38,61.
Methods
Scenario framework
Part of the Coupled Model Intercomparison Project Phase 6 (CMIP6), ScenarioMIP is a new, widely accepted scenario framework62,63 which provides integrated, internally consistent ensemble simulations of driving factors suitable for research across multiple scientific fields (Table 1). ScenarioMIP represents a matrix of possible integration of multiple SSPs and forcing outcomes driven by a set of emissions and land use scenarios, produced with integrated assessment models (IAMs)64. Compared with previous RCPs derived from earlier emissions and land use scenarios65, ScenarioMIP scenarios provided a related but updated simulation.
In ScenarioMIP, eight representative scenarios were provided to describe possible futures, which can be further divided into Tier 1 and Tier 2 based on relative priority62. Considering the accessibility of data, we used the four Tier 1 scenarios: Sustainability (SSP1-2.6), representing sustainable development in both socioeconomic and environmental aspects; Middle of the Road (SSP2-4.5), representing the continuation of recent global trends; Regional Rivalry (SSP3-7.0), representing a world of high inequality in human and economic opportunities, and Fossil-fueled Development (SSP5-8.5), representing a future with prosperous socioeconomic development embodied with improved air quality control at the expense of climate, with high energy demand66.
Under this framework, studies have projected the corresponding socioeconomic factors and concentration of pollutants50,67,68, with stricter air pollution controls tied to higher levels of economic development66. Hence, weak air pollution controls occur in SSP3-7.0, with medium controls in SSP2-4.5, and strong air pollution controls in SSP1-2.6 and SSP5-8.525. These studies provided a quantitative and systematic foundation for the robust and internally consistent projection of future trajectories of global DAPP. The corresponding data under ScenarioMIP includes surface concentration of pollutants (SO4, black carbon, organic aerosol, dust, sea salt), age-specific population, and socioeconomic data (fertility, GDP per capita, and average years of education)67,68 (Supplementary Note 1).
Estimating deaths attributable to PM2.5 pollution
Historical (2000–2015) DAPP can be estimated based on total population, population age structure, measured annual average PM2.5 concentration, as well as the death rate of diseases (details in Supplementary Note 1). The equation is given as follows4,5:
where DAPP is the deaths attributable to PM2.5 pollution; PAFa,d is the proportion of deaths attributed to PM2.5 pollution caused by disease d in a population with age a; POP refers to the total population; Ratea,d is the death rate of disease d for people with age a, and AgePa is the percentage of the total population of age a. In our formulation, 15 age groups were included in the equation, i.e., 25–30, 30–35, …, 90–95, and 95+ years old. Six diseases related to PM2.5 pollution were considered in this study, including lung cancer, chronic obstructive pulmonary disease, lower respiratory infection, ischemic heart disease, stroke, and diabetes mellitus type 2. Evidence linking these diseases with exposure to ambient air pollution was judged to be consistent with a causal relationship on the basis of criteria specified for Global Burden of Disease (GBD) risk factors, including meta-analysis, cohort study, and biologically plausible relationship5. Although PM2.5 pollution is also related to other adverse birth outcomes including low birth weight and short gestation, these 6 diseases represent around 95% of total deaths related to PM2.5 pollution from all causes based on the estimation of GBD 20195. We did not consider differences by gender to reduce the complexity of our projections.
PAFa,d refers to the proposition that a given disease proportion of deaths attributed to PM2.5 pollution caused by disease d in a population with age a, which can be calculated as below69.
where RRa,d is the relative risk for the population with age a of acquiring disease d. This refers to the ratio of incidence for an exposed population compared to an unexposed population. Relative risk can be quantified based on a non-linear exposure-response function which usually shows a steeper increase at lower concentrations with more modest increases at higher concentrations. In this study, we used the latest meta-regression (i.e., MR-BRT) exposure-response functions updated by GBD 20195 (Figure S3). For ischemic heart disease and stroke, we used age-specific exposure-response functions because the epidemiological evidence suggests that the relative risks for these diseases change by age4,49. For the other four diseases, the exposure-response functions are uniform for all age groups. Details of the calculation and validation of DAPP can be found in Supplementary Note 2.
Projecting future deaths attributable to PM2.5 pollution
We projected DAPP under different scenarios from 2015 to 2050 by introducing the corresponding driving factors from the ScenarioMIP framework into the above-mentioned epidemiological model. Among the driving factors used for the projection of DAPP, the total population and age structure were derived from existing projections in the SSPs database, consistent with the ScenarioMIP framework68 Future PM2.5 concentration and the death rate of diseases were both estimated in this study.
We used data from 11 climate and earth system models in the CMIP6 database to estimate future PM2.5 concentrations. Eight models are available for all four scenarios. In addition, one model (GFDL-CM4) provided data for SSP2-4.5 and 5-8.5 only, and two models (BCC-ESM1 and CNRM-ESM2-1) were only available for SSP3-7.0 (Table S3). Under a given scenario, these models use consistent anthropogenic and biomass-burning emissions from the same dataset25,66, but differ in other natural emissions (e.g., dust, biogenic volatile organic compounds, and others.) and aerosol scheme50. For example, only GISS-E2-1-G and GFDL-ESM4 provide ammonium and nitrate mass mixing ratios. For the CNRM-ESM2-1 model, anomalously large concentrations were obtained from sea salt mass mixing ratios. To ensure consistency, we calculated PM2.5 concentration offline with surface concentration of pollutants via the below equation:
where BC is black carbon; OA is organic aerosols (primary and secondary) and SS is sea salt. The concentration of NH4 is not estimated in all CMIP6 models so we estimated it as NH4 = (36 × SO4)/96 assuming that NH4 is only present as ammonium sulfate20. The factors 0.25 and 0.1 were intended to approximate the fractions of sea salt and dust in the PM2.5 size range. As one component of PM2.5, nitrate was only reported by two models from CMIP6, therefore, following Silva et al. 70 and Silva et al. 71, we omitted it from the PM2.5 concentration formula to avoid inconsistencies with other CMIP6 models. Where models included multiple ensembles, a mean was taken using all available members for each model.
Because the PM2.5 concentration from the CMIP6 models and historical estimation was not comparable, we further calibrated PM2.5 concentration based on the trend in simulated PM2.5 concentration relative to historical PM2.5 concentration measurements for the base year 2015. Please see Supplementary Note 3 and Figs. S5–6 for the details of PM2.5 concentration projection, validation, and uncertainty analysis.
We estimated future death rate of diseases based on the historical death rate of diseases and future socioeconomic development indicators using the model developed by Foreman et al. 11. This model assumed the cause-specific death rate would change with socioeconomic development following the formulae:
where ln(m) refers to the natural logarithm of the cause-specific death rate, which can be determined by \(\hat{y}\) (representing the effects of the long-term trend, socioeconomic development, and risk factors) and \(\hat{\epsilon }\) (representing the residuals that cannot be explained by these factors). In the equation to calculate \(\hat{y}\), β1 and β2 represent the global coefficients of the Socio-Demographic Index (SDI) when its value is less or more than 0.8. θa refers to an age-specific secular trend, and t represents time. αla is the region and age-specific intercept, and ln(R) represents a scalar that captures the effects of risk factors. SDI is calculated by combining the logarithm of income per person, educational attainment, and total fertility rate under 25 years. \(\hat{\epsilon }\) can be derived using historical data based on the autoregressive integrated moving average model (ARIMA). The detailed projection, validation, and uncertainty analysis for the future death rates of diseases can be found in Supplementary Note 4 and Figures S7-8. The global and regional long-term trends of underlying drivers used to project DAPP are presented in Figures S9-10.
We then quantified the uncertainty in the projection of DAPP. The driving factors and the epidemiological model both introduce uncertainty into DAPP projection. We considered the range of uncertainty in future PM2.5 concentration and the death rate of diseases, and calculated the possible range in DAPP based on these uncertainty intervals. Regarding the epidemiological model, uncertainty mainly comes from the choice of the exposure-response function. We present the results derived from the medium MR-BRT function, and conducted a similar uncertainty analysis based on the upper (97.5th) and lower (2.5th) estimates of MR-BRT to validate the robustness. Detail of the uncertainty in DAPP projections can be found in Supplementary Note 2.
Measuring the attainment of SDG3.9
SDG3.9 commits countries to a substantial reduction in the number of deaths and illnesses from hazardous chemicals and air, water, and soil pollution and contamination7. However, the term substantial reduction is subjective and not clearly defined in SDG3.9. Previously, GBD2017 SDG Collaborators (2018)72 used the top 10th percentile of performance among country-level rates of change before 2015 as the annualized change rate of indicators between 2015 and 2030 required by 25 SDG targets. Hence, targets which are not quantitatively defined can be specified by assuming their progress is keeping pace with defined indicators. We set quantitative targets for SDG3.9 based on the 10th percentile reduction in DAPP at the national scale during 2000–2015, and the estimated value is around 30%. In addition, to acknowledge the different levels of target setting and the uncertainty of pathways, following Moallemi et al. 27, we roughly defined the substantial reduction in terms of three levels of ambition in DAPP reduction targets under SDG3.9, where weak, moderate, and ambitious targets are represented by a 10%, 20%, and 30% reduction compared to 2015 levels, respectively.
Quantifying the effect of different driving factors on the attainment of SDG3.9
DAPP is a function of the nonlinear interaction (Eq. 1) of different driving factors (population size, PM2.5 concentration, age structure, and death rate of diseases). Hence, a decomposition method4,73 was taken to dissect the contributions of these factors to the change in DAPP. The decomposition method estimates the contribution of factors by sequentially introducing each factor into the DAPP equation. The difference between each consecutive step represents the relative contribution of the corresponding factor. As the sequence of adding factors also influences the results, we estimated the results under all 24 possible sequences of the four factors. The final estimation of contributions from different factors is the average value of the results for each factor. Detailed equations and processes are shown in Figure S18.
Exploring pathways to meet SDG3.9 via additional improvements in air pollution control and healthcare
Based on ScenarioMIP projection, we also considered the potential of additional efforts to reduce DAPP. Among the four components influencing DAPP, demographic factors (population and age structure) cannot be effectively altered by policy intervention in the short term, but PM2.5 concentration and death rate of diseases can more readily be changed via additional efforts in air pollution control (e.g., stricter air quality standards, technological innovation, and cleaner energy mix)38,61 and healthcare (e.g., investment in medical research, scientific breakthroughs, health system improvements, and better accessibility)11,74. We considered three possible conditions, including additional air quality improvement (20% lower PM2.5 concentration + No change in death rate of diseases); additional healthcare improvement (No change in PM2.5 concentration + 20% lower death rate of diseases), and both measures (20% lower PM2.5 concentration + 20% lower death rate of diseases). The value of 20% was selected subjectively to represent a substantial and plausible improvement resulting from concerted government attention. With these assumptions, we conducted a sensitivity analysis to assess the response of additional air quality and healthcare interventions towards SDG3.9.
Reporting summary
Further information on research design is available in the Nature Portfolio Reporting Summary linked to this article.
Data availability
All the data generated in this study have been deposited in the GitHub repository https://github.com/yuehuanbi/attainment-of-SDG3.9. Other specific data are available from the corresponding author upon reasonable request.
Code availability
We used the integrated exposure-response function updated in the Global Burden of Disease 2019 to estimate the relative risk caused by PM2.5 exposure. The detailed function is accessible to all users at https://ghdx.healthdata.org/record/global-burden-disease-study-2019-gbd-2019-air-pollution-exposure-estimates-1990-2019. Other data processing in this study are conducted using ArcGIS and Microsoft Excel, see details in Supplementary Note 2-4.
References
World Health Organization. Ambient air pollution: A global assessment of exposure and burden of disease, http://www.who.int/phe/publications/air-pollution-global-assessment/en/ (2016).
International Organization for Standardization. ISO 4225:2020 Air quality—General aspects—Vocabulary, https://www.iso.org/standard/10025.html (2020).
Kaiser, J. Mounting evidence indicts fine-particle pollution. Science 307, 1858–1861 (2005).
Cohen, A. et al. Estimates and 25-year trends of the global burden of disease attributable to ambient air pollution: an analysis of data from the Global Burden of Diseases Study 2015. Lancet 389, 1907–1918 (2017).
GBD 2019 Risk Factors Collaborators. Global burden of 87 risk factors in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet 396, 1223–1249 (2020).
World Health Organization. World Health Statistics 2022: Monitoring health for the SDGs, https://www.who.int/data/gho/publications/world-health-statistics (2022).
United Nations. Sustainable Development Goals, https://sustainabledevelopment.un.org/ (2015).
Wang, Y. et al. Health Burden and economic impacts attributed to PM2.5 and O3 in China from 2010 to 2050 under different representative concentration pathway scenarios. Resour. Conserv. Recycling 173, 105731 (2021).
Conibear, L. et al. The contribution of emission sources to the future air pollution disease burden in China. Environ. Res. Lett. 17, 064027 (2022).
Myrskylä, M., Kohler, H.-P. & Billari, F. C. Advances in development reverse fertility declines. Nature 460, 741 (2009).
Foreman, K. J. et al. Forecasting life expectancy, years of life lost, and all-cause and cause-specific mortality for 250 causes of death: reference and alternative scenarios for 2016-40 for 195 countries and territories. Lancet 392, 2052–2090 (2018).
Guan, D. et al. The socioeconomic drivers of China’s primary PM 2.5 emissions. Environ. Res. Lett. 9, 024010 (2014).
Geng, G. et al. Drivers of PM2.5 air pollution deaths in China 2002–2017. Nat. Geosci. 14, 645–650 (2021).
Cai, W., Li, K., Liao, H., Wang, H. & Wu, L. Weather conditions conducive to Beijing severe haze more frequent under climate change. Nat. Clim. Change 7, 257–262 (2017).
Silva, R. et al. Future global mortality from changes in air pollution attributable to climate change. Nat. Clim. Change 7, 647–651 (2017).
Moss, R. H. et al. The next generation of scenarios for climate change research and assessment. Nature 463, 747–756 (2010).
Lelieveld, J., Evans, J., Fnais, M., Giannadaki, D. & Pozzer, A. The contribution of outdoor air pollution sources to premature mortality on a global scale. Nature 525, 367–371 (2015).
Rafaj, P. et al. Outlook for clean air in the context of sustainable development goals. Glob. Environ. Change 53, 1–11 (2018).
West, J. J. et al. Co-benefits of mitigating global greenhouse gas emissions for future air quality and human health. Nat. Clim. Change 3, 885–889 (2013).
Hong, C. et al. Impacts of climate change on future air quality and human health in China. Proc. Natl Acad. Sci. USA 116, 17193–17200 (2019).
Markandya, A. et al. Public health benefits of strategies to reduce greenhouse-gas emissions: low-carbon electricity generation. Lancet 374, 2006–2015 (2009).
Chowdhury, S., Dey, S. & Smith, K. R. Ambient PM2.5 exposure and expected premature mortality to 2100 in India under climate change scenarios. Nat. Commun. 9, 318 (2018).
Yang, H., Huang, X., Westervelt, D. M., Horowitz, L. & Peng, W. Socio-demographic factors shaping the future global health burden from air pollution. Nat. Sustain. https://doi.org/10.1038/s41893-022-00976-8 (2022).
O’Neill, B. C. et al. Achievements and needs for the climate change scenario framework. Nat. Clim. Change 10, 1074–1084 (2020).
Gidden, M. J. et al. Global emissions pathways under different socioeconomic scenarios for use in CMIP6: a dataset of harmonized emissions trajectories through the end of the century. Geosci. Model Dev. 2018, 1–42 (2018).
Hess, J. J. et al. Guidelines for modeling and reporting health effects of climate change mitigation actions. Environ. Health Perspect. 128, 115001 (2020).
Moallemi, E. A. et al. Early systems change necessary for catalyzing long-term sustainability in a post-2030 agenda. One Earth 5, 792–811 (2022).
KC, S. & Lutz, W. The human core of the shared socioeconomic pathways: Population scenarios by age, sex and level of education for all countries to 2100. Global Environmental Change, https://doi.org/10.1016/j.gloenvcha.2014.06.004 (2014).
Zhang, Q. et al. Drivers of improved PM2.5 air quality in China from 2013 to 2017. Proc. Natl Acad. Sci. USA 116, 24463–24469 (2019).
Wang, H. et al. Health benefits of on-road transportation pollution control programs in China. Proc. Natl Acad. Sci. USA 117, 25370 (2020).
Hill, J. et al. Air-quality-related health damages of maize. Nat. Sustain. 2, 397–403 (2019).
Yin, H. et al. Population ageing and deaths attributable to ambient PM2.5 pollution: a global analysis of economic cost. Lancet Planet. Health 5, e356–e367 (2021).
GBD 2019 Diseases and Injuries Collaborators. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet 396, 1204–1222 (2020).
World Health Organization. Global Expenditure on Health: Public Spending on the Rise?, https://apps.who.int/iris/bitstream/handle/10665/350560/9789240041219-eng.pdf (2022).
Lacey, F. G. et al. Improving present day and future estimates of anthropogenic sectoral emissions and the resulting air quality impacts in Africa. Faraday Discuss. 200, 397–412 (2017).
Dimitrova, A. et al. Health impacts of fine particles under climate change mitigation, air quality control, and demographic change in India. Environ. Res. Lett. 16, 054025 (2021).
Vohra, K. et al. Rapid rise in premature mortality due to anthropogenic air pollution in fast-growing tropical cities from 2005 to 2018. Sci. Adv. 8, eabm4435 (2022).
Huang, X., Srikrishnan, V., Lamontagne, J., Keller, K. & Peng, W. Effects of global climate mitigation on regional air quality and health. Nat. Sustain. 6, 1054–1066 (2023).
Cifuentes, L., Borja-Aburto, V. H., Gouveia, N., Thurston, G. & Davis, D. L. Climate change: Hidden health benefits of greenhouse gas mitigation. Science 293, 1257–1259 (2001).
Sandalow, D. Guide to Chinese Climate Policy 2019, https://energypolicy.columbia.edu/research/report/guide-chinese-climate-policy (2019).
Qian, H. et al. Air pollution reduction and climate co-benefits in China’s industries. Nat. Sustain. 4, 417–425 (2021).
Soergel, B. et al. A sustainable development pathway for climate action within the UN 2030 Agenda. Nat. Clim. Change 11, 656–664 (2021).
The State Council of China. Fighting the Tough Battle of Pollution Prevention and Control, http://www.gov.cn/zhengce/2021-11/07/content_5649656.htm (2021).
Li, K. et al. A two-pollutant strategy for improving ozone and particulate air quality in China. Nat. Geosci. 12, 906–910 (2019).
Patel, D. et al. Joint effects of heatwaves and air quality on ambulance services for vulnerable populations in Perth, western Australia. Environ. Pollut. 252, 532–542 (2019).
Kloog, I., Ridgway, B., Koutrakis, P., Coull, B. A. & Schwartz, J. D. Long- and short-term exposure to PM2.5 and mortality: using novel exposure models. Epidemiology 24, 555–561 (2013).
Liu, C. et al. Ambient particulate air pollution and daily mortality in 652 cities. N. Engl. J. Med. 381, 705–715 (2019).
Zhao, B. et al. Change in household fuels dominates the decrease in PM2.5 exposure and premature mortality in China in 2005–2015. Proc. Natl Acad. Sci. USA 115, 12401 (2018).
Burnett, R. & Cohen, A. Relative risk functions for estimating excess mortality attributable to outdoor PM2.5 air pollution: evolution and state-of-the-art. Atmosphere 11, 589 (2020).
Turnock, S. T. et al. Historical and future changes in air pollutants from CMIP6 models. Atmos. Chem. Phys. 2020, 1–40 (2020).
Burnett, R. T., Spadaro, J. V., Garcia, G. R. & Pope, C. A. Designing health impact functions to assess marginal changes in outdoor fine particulate matter. Environ. Res. 204, 112245 (2022).
Shen, H. et al. Urbanization-induced population migration has reduced ambient PM2.5 concentrations in China. Sci. Adv. 3, e1700300 (2017).
Liu, Y. et al. Role of climate goals and clean-air policies on reducing future air pollution deaths in China: a modelling study. Lancet Planet. Health 6, e92–e99 (2022).
Xu, F. et al. The challenge of population aging for mitigating deaths from PM2.5 air pollution in China. Nat. Commun. 14, 5222 (2023).
He, G., Pan, Y. & Tanaka, T. The short-term impacts of COVID-19 lockdown on urban air pollution in China. Nat. Sustain. 3, 1005–1011 (2020).
Bertram, C. et al. COVID-19-induced low power demand and market forces starkly reduce CO2 emissions. Nat. Clim. Change 11, 193–196 (2021).
Shi, Z. et al. Abrupt but smaller than expected changes in surface air quality attributable to COVID-19 lockdowns. Sci. Adv. 7, eabd6696 (2021).
Yue, H., He, C., Huang, Q., Yin, D. & Bryan, B. A. Stronger policy required to substantially reduce deaths from PM2.5 pollution in China. Nat. Commun. 11, 1462 (2020).
Cheng, J. et al. Pathways of China’s PM2.5 air quality 2015–2060 in the context of carbon neutrality. Natl Sci. Rev. 8, nwab078 (2021).
World Health Organization. WHO global air quality guidelines: particulate matter (PM2.5 and PM10), ozone, nitrogen dioxide, sulfur dioxide and carbon monoxide, https://www.who.int/publications/i/item/9789240034228 (2021).
Cheng, J. et al. A synergistic approach to air pollution control and carbon neutrality in China can avoid millions of premature deaths annually by 2060. One Earth 6, 978–989 (2023).
O’Neill, B. C. et al. The Scenario Model Intercomparison Project (ScenarioMIP) for CMIP6. Geosci. Model Dev. 9, 3461–3482 (2016).
Eyring, V. et al. Overview of the Coupled Model Intercomparison Project Phase 6 (CMIP6) experimental design and organization. Geosci. Model Dev. 9, 1937–1958 (2016).
Riahi, K. et al. The Shared Socioeconomic Pathways and their energy, land use, and greenhouse gas emissions implications: an overview. Glob. Environ. Change 42, 153–168 (2017).
van Vuuren, D. P. et al. The representative concentration pathways: an overview. Clim. Change 109, 5 (2011).
Rao, S. et al. Future air pollution in the shared socio-economic pathways. Glob. Environ. Change 42, 346–358 (2017).
Dellink, R., Chateau, J., Lanzi, E. & Magné, B. Long-term economic growth projections in the shared socioeconomic pathways. Glob. Environ. Change 42, 200–214 (2017).
Lutz, W., Anne, G., Samir, K., Marcin, S. & Nikolaos, S. Demographic and Human Capital Scenarios for the 21st Century: 2018 assessment for 201 countries, http://www.who.int/phe/publications/air-pollution-global-assessment/en/ (2018).
Rockhill, B., Newman, B. & Weinberg, C. Use and misuse of population attributable fractions. Am. J. Public Health 88, 15–19 (1998).
Silva, R. et al. Global premature mortality due to anthropogenic outdoor air pollution and the contribution of past climate change. Environ. Res. Lett. 8, 034005 (2013).
Silva, R. A. et al. The effect of future ambient air pollution on human premature mortality to 2100 using output from the ACCMIP model ensemble. Atmos. Chem. Phys. 16, 9847–9862 (2016).
GBD 2017 SDG Collaborators. Measuring progress from 1990 to 2017 and projecting attainment to 2030 of the health-related Sustainable Development Goals for 195 countries and territories: a systematic analysis for the Global Burden of Disease Study 2017. Lancet 392, 2091–2138 (2018).
Li, C. et al. Reversal of trends in global fine particulate matter air pollution. Nat. Commun. 14, 5349–5349 (2023).
Girosi, F. & King, G. Demographic Forecasting, https://gking.harvard.edu/node/5502 (2008).
National Platform for Common Geospatial Information Services of China. World Map, https://www.tianditu.gov.cn/ (2023).
US National Geophysical Data Center. ETOPO1, Global 1 Arc-minute Ocean Depth and Land Elevation, https://rda.ucar.edu/datasets/ds759.4/ (2009).
Acknowledgements
We express our gratitude to the anonymous reviewers and editors for their professional comments and suggestions. We thank Prof. Samir K.C. (International Institute for Applied Systems Analysis, Laxenburg, Austria) and Dr. Steven T. Turnock (Met Office, Exeter, UK) for their generous sharing of data. We would like to thank the high-performance computing support from the Center for Geodata and Analysis, Faculty of Geographical Science, Beijing Normal University [http://gda.bnu.edu.cn/]. C.H. was funded by the National Natural Science Foundation of China (Grant No. 42371296) and BNU-FGS Global Environmental Change Program (No. 2023-GC-ZYTS-08). H.Y. was supported by the Shandong Provincial Natural Science Foundation (ZR2022QD051). D.Z. received funding from the National Natural Science Foundation of China (Grant No. 42271314). Q.H. was supported by the and Beijing Nova Program (Grant No. 20220484163) and B.B. was supported by Deakin University, Australia.
Author information
Authors and Affiliations
Contributions
H.Y., C.H., Q.H. and B.B. designed the study and developed the analysis plan. H.Y., B.B., Y.Y., X.Q. and D.Z. prepared the basic data and did the data analysis and visualization. H.Y., Q.H., B.B., Q.M., E.M. and D.Z. drafted the manuscript. Q.H., F.X. and P.S. verified the underlying data. All authors contributed to the interpretation of findings, provided revisions to the manuscript, and approved the final manuscript.
Corresponding authors
Ethics declarations
Competing interests
We declare no competing interests.
Peer review
Peer review information
Nature Communications thanks Yilin Chen, Eric Lavigne, Jon Sampedro, and the other, anonymous, reviewer(s) for their contribution to the peer review of this work. A peer review file is available.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Yue, H., He, C., Huang, Q. et al. Substantially reducing global PM2.5-related deaths under SDG3.9 requires better air pollution control and healthcare. Nat Commun 15, 2729 (2024). https://doi.org/10.1038/s41467-024-46969-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41467-024-46969-3
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
