
Abstract
Preterm birth is currently the leading cause of neonatal morbidity and mortality. Genetic, immunological and infectious causes are suspected. Preterm infants have a higher risk of severe bacterial neonatal infections, most of which are caused by Escherichia coli an in particular E. coli K1strains. Women with history of preterm delivery have a high risk of recurrence and therefore constitute a target population for the development of vaccine against E. coli neonatal infections. Here, we characterize the immunological, microbiological and protective properties of a live attenuated vaccine candidate in adult female mice and their pups against after a challenge by K1 and non-K1 strains of E. coli. Our results show that the E. coli K1 E11 ∆aroA vaccine induces strong immunity, driven by polyclonal bactericidal antibodies. In our model of meningitis, mothers immunized prior to mating transfer maternal antibodies to pups, which protect newborn mice against various K1 and non-K1 strains of E. coli. Given the very high mortality rate and the neurological sequalae associated with neonatal E. coli K1 meningitis, our results constitute preclinical proof of concept for the development of a live attenuated vaccine against severe E. coli infections in women at risk of preterm delivery.
Similar content being viewed by others
Introduction
Preterm delivery (<37 weeks of gestation) is the leading cause of neonatal morbidity and mortality1. Each year, approximately 15 million babies worldwide are born prematurely; this corresponds to 11% of all births. 90% of preterm deliveries take place in low-income/resource-poor countries2,3. With 35% of all deaths among newborns due to prematurity, prematurity which also accounts for 18% of all deaths among children aged under 5 years is a true public health problem worldwide2,3. The etiology of preterm delivery is multifactorial, and genetic, infectious and immunological factors have been described4,5. Researchers have found that women with a previous preterm delivery are significantly more likely to have a subsequent preterm delivery5. Furthermore, infections are at least six times more frequent in preterm infants than in term infants6, due to immaturity of the immune system7. Indeed, preterm infants have functional impairments in innate immunity (as evidenced by abnormally low levels of cytokines, chemokines, antimicrobial proteins, and antimicrobial peptides), cellular immunity, and the complement system7,8,9,10. Escherichia coli an in particular E. coli K1 strains among the most common pathogens in newborns and constitutes the leading cause of neonatal bacterial meningitis in preterm infants11,12,13. Infants born to women with a previous preterm delivery have an elevated risk of neonatal E. coli K1 meningitis; hence, vaccine-based prevention in these women might significantly reduce the incidence of neonatal meningitis. Scientific and technological progress has enabled the development of a vaccine against E. coli K1 bacterial meningitis. Although a candidate vaccine against E. coli K1 (based on the OmpA protein) has shown efficacy in mice14,15,16, it has not been approved to date for use in clinical practice.
Live attenuated vaccines reportedly confer the high levels of rapid, sustained, full immunity required for protection of the mother and her infant17,18. However, the use of these vaccines is not recommended in certain high-risk populations, such as pregnant women and immunocompromised individuals19,20. Nevertheless, the administration of a live vaccine is not contraindicated prior to pregnancy in women of childbearing age or in those at risk of preterm delivery20,21,22.
By using a combination of saturated transposon mutagenesis and high-throughput sequencing (TnSeq, a powerful tool to study host-pathogen interactions), we recently identified the aroA gene as a virulence factor in E. coli K123. aroA encodes 5-enolpyruvylshikimate-3-phosphate synthase which is involved in the biosynthesis of aromatic amino acids24 and several iron capture systems25. Therefore, we decided to build a ∆aroA E. coli K1 mutant and evaluate it potential as a live attenuated vaccine against severe neonatal infections caused by E. coli. Although our TnSeq experiments had revealed other E. coli K1 virulence factors, AroA was selected for live vaccine attenuation because deletion of the aroA gene have been shown to provide strong protection in other settings (such as Pseudomonas aeruginosa or Salmonella sp. Infections)26,27. Furthermore, it has also been reported that an E. coli O78 vaccine attenuated by deletion of the aroA gene was efficacious against avian diseases28. One of the main reason aroA is a good mutated background for vaccine strains is that it makes strains auxotrophic for aromatic amino acids and so cannot replicate properly in certain niches in the host26,29,30.
In the present study, we first confirmed the results of the Tnseq data experiments and showed that the virulence of E. coli K1 E11 ∆aroA was indeed attenuated both in vitro and in vivo probably through the significant decreased of the expression of the genes encoding for the type 1 fimbriae, a major E. coli K1 virulence factor31,32 in the ∆aroA mutant strains. We then characterized the immunological and microbiological properties of a live attenuated E. coli K1 E11 ∆aroA vaccine candidate after injection into adult female mice. Lastly, we demonstrated the very strong degree of protection afforded to offspring born to mothers having received with the attenuated vaccine before mating. Our results constitute preclinical proof of concept of a new strategy for the development of a vaccine against E. coli K1 infections in women at risk of preterm delivery.
Results
Characterization of the attenuation of E. coli K1 E11∆aroA
Using the methods described by Datsenko33, we built a ∆aroA mutant by deleting the gene aroA from a clinical strain of E. coli K1 E1123. The absence of the aroA gene in the mutant strain was confirmed by a PCR analysis and control experiments. Clones resistant to 100 µg/mL kanamycin were obtained and then tested (using PCR) to check the insertion of the kanamycin cassette and the deletion of the aroA gene (Supplementary Fig. 1).
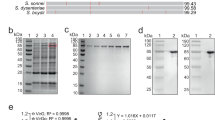
After seven hours of culture in liquid lysogeny broth (LB) and Dulbecco’s Modified Eagle Medium (DMEM) medium, the growth rate of the aroA-deleted strain was similar to that of the wild type (WT) E. coli E11 strain in LB medium, While a non-significant reduction (P > 0.05) was found in DMEM, the culture medium used in the cell experiments conducted in this project (Fig. 1A) when carrying out an auxotrophicity test for amino acids in the minimal M9 medium, we observed a difference in growth between E. coli K1 E11 WT and ΔaroA in M9 minimal medium not supplemented with amino acid: the mutant strain was not able to grow in minimal medium unless supplemented with amino acids (Supplementary Fig. 1B).

A: Growth curves for E. coli E11 WT and ΔaroA strains in LB and DMEM medium. After 7 h of culture, the difference in the growth rate between the two strains was not significant (p > 0.05) (n = 3). B, C Adhesion to (B) (n = 6) and invasion (C) (n = 4) of Hela cells by E. coli E11 ΔaroA were significantly lower than for the WT strain E. coli E11 (p < 0.05) data are presented as mean values SD. D RNAseq analysis of E. coli E11 WT and E. coli E11 ΔaroA grown in LB: genes encoding for the genes fimABCDEFGHI (red dots) are annotated in a volcano plot: a scatterplot showing statistical significance (P-values, Y-axis) versus magnitude of change (fold change, X axis) (n = 3). E Expression of the FimH gene by RTqPCR in the E11 WT vs ΔaroA strain in LB. Significantly decreased expression of the FimH is found in E11 ΔaroA (p = 0,02) (n = 6). F–H Evaluation of the in vivo (n = 4) mortality of the mutant strain vs. the virulent WT E. coli K1 E11, S88, RS218 (F-G) and two non-K1(H) E. coli strains. The WT strains were 100 times more virulent than the mutant strain (F). The lethal dose was 107 CFU for E. coli K1 E11 WT and S88, 106 CFU for RS218, 108 CFU for S242 (no-K1), 107 CFU for S510 (no-K1) and over 109 CFU for the mutant strain. Error bars represent standard deviations (SD). (A): p-value values indicate significant differences in an ordinary One-way ANOVA, Dunnett’s multiple comparisons test, with a single pooled variance. (B, C, and E) p-value values indicate significant differences in a two-tailed Mann–Whitney non-parametric test (B, C, and E), (D): one-way ANOVA using Bonferroni’s multiple comparisons test and a Mantel–Haenszel log-rank test (F–H). Source data are provided as a Source Data file.
Then, we found that the adhesion and invasion capacities of E. coli K1 E11 ΔaroA were significantly reduced compared to those of the WT strain (p = 0.002 and p = 0.02 respectively) (Fig. 1B, C) without any bias that could have been caused by a growth defect of the AroA mutant (no difference between the two strains at T0 of the experiment as shown in Supplementary Fig. 1C–E).
While part of this finding could be due to the growth defect of the E. coli E11 ΔaroA strain found in DMEM (Fig. 1A), we decided to further explore the phenotype of the aroA mutant, in particular with regard to any changes in expression of the main E. coli K1 virulence determinants. Therefore, we performed a comprehensive investigation on the impact on the transcriptome of the deletion of the aroA gene by conducting RNAseq experiments in LB and DMEM of E. coli E11 WT and ΔaroA.
As shown (Fig. 1D) and (Supplemental Table 1), genes encoding for type 1 fimbriae were among the top ten genes with the most decreased expression in the E. coli E11 ΔaroA compared to E11 WT when both strains were grown in LB. This decreased expression was confirmed by qRT-PCR (Fig. 1E) and also found in DMEM (Supplemental Fig. 5). When looking at the top ten percent genes with the most decreased expression in E. coli E11 ΔaroA compared to E11 WT in LB and the top ten percent genes with the most decreased expression in E. coli E11 ΔaroA compared to E11 WT in DMEM, we found 39 genes in common (Supplemental Table 2). Among these 39 genes, we found all the genes encoding for the Type 1 Fimbriae except the regulator genes fimB and E34. The role of the Type 1 Fimbriae in the adhesion on epithelial cells has long been described in E. coli, further explaining the results presented Fig. 1B–C. However, the Type 1 Fimbriae also constitutes a major virulence factor in E. coli K131,32. Therefore, we next evaluated the in vivo attenuation of E. coli K1 E11∆aroA compared to E. coli K1 E11 WT.
Using a mouse model of systemic dissemination after intraperitoneal injection, we compared the mortality rates resulting from infections by the mutant strain E. coli K1 E11 ∆aroA vs. the WT strain (Fig. 1F). We also tested two E. coli K1 strains (E. coli S8835 and RS21836) and two non-K1 E. coli meningitis strains (E. coli S510 and E. coli S242) responsible for severe neonatal infections (Fig. 1G, H). All the E. coli K1 strains were 100 to 1000 times more virulent than the E. coli K1 E11 ∆aroA mutant, while the E. coli non-K1 strains were 10–100 times more virulent than the ∆aroA mutant. Indeed, the lethal doses were 107 colony forming units (CFU) for E. coli E11 WT and E. coli S88, 106 CFU for E. coli RS218, 107 CFU for E. coli S510 (non-K1), 108 CFU for E. coli S242, and >109 CFU for the mutant strain E. coli E11 ∆aroA (Fig. 1F–H). Our data showed that E. coli E11 ∆aroA could be used safely as a live attenuated vaccine in our project—even at doses that would be lethal if non-mutant strains were used. The significant reduction in the expression of genes coding for type 1 fimbriae found in this study probably add significantly to the safety of the live attenuated E. coli E11 ∆aroA vaccine.
Evaluation of the humoral immune response after immunization
After having confirmed the safety of our live attenuated vaccine, we evaluated its immunogenicity in an immunization regimen (Fig. 2A) with intraperitoneal (IP) and/or subcutaneous (SC) injection of a 105 CFU suspension of E. coli E11 ∆aroA in adult female mice once a week for 3 weeks.

A The immunization regimen for BALB/c female mice with 105 CFU of E. coli K1 E11 ΔaroA or NaCl (n = 4) by intraperitoneal (IP) and subcutaneous routes (SC). B IgG response to three E. coli K1 strains initially selected for the study (E11 WT, S88 and RS218, responsible for neonatal meningitis) after each immunization by IP route (n = 4). C IgG response to E. coli K1 E11 WT and RS218 strains, after immunization with 3 doses by IP and SC route (n = 4). D Antibody titers after immunization with 3 doses (IP route on top, SC route in the bottom) (n = 4). E Detection of IgG1, Ig2a, IgG2b and IgG3 antibody isotypes after subcutaneous immunization in 3 doses (n = 4). E p-value values indicate significant differences in an ordinary one-way ANOVA. Error bars represent standard deviations (SD). Source data are provided as a Source Data file.
Vaccinated female mice were sampled to test their humoral response against whole-bacterial cells. Levels of specific antibodies against three E. coli K1 strains (E. coli E11 WT, S88 and RS218) initially selected for the study were detected (using an ELISA) in the sera of immunized mice by IP route (Fig. 2B). Levels of specific antibodies against E. coli K1 strains (E. coli E11 WT and RS218) were also detected (using ELISA) in the serum of subcutaneously immunized mice (Fig. 2C). The kinetics of antibody titers after immunization with 3 doses by the IP and SC routes were also observed. High antibody levels were detected up to 35 days after immunization (Fig. 2D) and more that 100 days after immunization by IP route (Supplementary Fig. 2A). We also detected isotype levels of IgG1, IgG2a, IgG2b and IgG3 in the serum of immunized mice. The IgG2 level was the highest in the serum tested (Fig. 2E). In the sera of immunized mice, we also found an elevated titer of antibodies against other E. coli K1 and E. coli non-K1 strains including strains responsible for severe neonatal infections (provided by the French National Reference Center) (Supplementary Fig. 2B, C). To confirm that our live attenuated vaccine induced a specific, polyclonal immune response, we next performed SDS PAGE gel experiments using E. coli K1 strains and Western blot experiments with three E. coli K1 strains and a E. coli non-K1 strain. We were able to visualize the proteins in all of these bacteria (Supplementary Fig. 2D) and we detected polyclonal antibodies against several bacterial antigens (Supplementary Fig. 2E, F), including several antigens from the E. coli non-K1 S510 strain. (Supplementary Fig. 2G). Furthermore, we compared the immunogenicity of the live attenuated strain to the inactivated strain, and found that the live attenuated strain was significantly more immunogenic compared to the inactivated strain (Supplementary Fig. 2J). Taken as a whole, these results show that immunization with the ∆aroA mutant E. coli K1 strain induced a strong humoral immune response and triggered the production of polyclonal antibodies capable of binding to a range of antigens from both K1 and non-K1 strains of E. coli.
Evaluation of the cellular immune response after immunization
We next evaluated the cellular immune response in BALB/c female mice (n = 4) immunized with three doses of the E. coli E11 K1 ∆aroA suspension. Mice were sacrificed 7 days after the third dose of immunization; each animal’s spleen was collected, and the splenocytes were isolated and analyzed. Our results showed that there were no significant differences between vaccinated and nonvaccinated groups of mice with regard to the expression of T cell (Fig. 3A), B cell (Fig. 3B), CD4 and CD8 T cell populations (Fig. 3C, D) and regulatory T cells (Fig. 3E). However, a trend towards a greater regulatory T cell count was observed in the spleen samples from vaccinated mice but with no significant difference (Fig. 3F, G). Furthermore, we assessed the cellular response at the systemic level by quantifying serum levels of cytokines associated with Th1, Th2 and Th17 responses. The production of TNFα (Fig. 3H) and IL-10 (Fig. 3I) was induced more strongly in the vaccinated mice than in the nonvaccinated mice, even though the levels of these cytokines were very low in absolute terms. Our results indicate that vaccination with the E. coli K1 E11 ∆aroA strain did not induce a robust cellular immune response.

A–E Comparison of the expression of T cells (A), B cells (B), T cells CD4+ (C), T cells CD8+ (D) and regulatory T cells (E) among the hematopoietic splenocytes in the groups of vaccinated and non-vaccinated mice (n = 4). There were no significant intergroup differences in the various cell populations (p > 0.05). F-G Comparison of regulatory T cell expression (F) (n = 4) and FOXP3 expression by the T cell DC4+ population (G) (n = 4). The regulatory T cell count was higher in the vaccinated group of mice, but the difference was not significant (p > 0.05). The samples could be almost perfect superposed. H–I (n = 4): The concentration of TNF (H) and IL-10 (I) 7 days after the third dose was significantly higher in the sera of vaccinated mice than in nonvaccinated mice (p < 0.05). IL-2, IL4, IFN gamma and IL-17A were absent in the sera of the vaccinated and nonvaccinated groups. P-value values indicate significant and non-significant differences in a two-tailed Mann-Whitney non-parametric test (A–I). Error bars represent standard deviations (SD). Source data are provided as a Source Data file.
Evaluation of the protection of vaccinated female mice
To evaluate the in vitro protection afforded by the polyclonal antibodies generated after vaccination, we performed serum bactericidal assays against three strains of E. coli K1 (E11 WT, S88 and RS218). In the presence of baby rabbit complement, we detected strong bactericidal activities against the three E. coli K1 strains in the serum of immunized mice, up to a serum dilution of 1:100 (Fig. 4A). We detected bactericidal activity against two other K1 strains of E. coli (S524 and S395) in the serum of immunized mice at a serum dilution of 1:2 (Supplementary Fig. 3A). However, the K1 capsule is known for its high resistance to the action of the complement37 and other strains could be more or totally resistant if tested in this assay38,39. To confirm the specificity of the observed bactericidal activity, we tested other pathogenic Gram-negative bacteria (Klebsiella pneumoniae and Pseudomonas aeruginosa PA14, previously used in killing experiments) as controls. The absence of bactericidal activity against these two control species confirmed the specificity of our assays (Fig. 4B).

A Percentage of bacterial activity obtained with various dilutions (1:2, 1:20 and 1:100) of sera from immunized and non-immunized mice (Normal Mice Serum, NMS), (n = 4) with the E. coli strains E11, S88 and RS218, using 3–4 week-old baby rabbit complement. B Percentage of activity obtained with sera from immunized mice or non-immunized mice with Pseudomonas aeruginosa PA14 and Klebsiella pneumoniae, using 3–4 week-old baby rabbit complement (n = 4). Bactericidal activity is considered potentially significant in vivo if in vitro killing is >30%. C–I On day 7 post-vaccination by the IP route, groups of vaccinated female BALB/c mice (n = 4 per group) were challenged with lethal doses of 107 CFU (C) and 108 CFU (D) of E. coli K1 E11 WT, 107 CFU (E) 108 CFU (F) of E. coli K1 S88, 107 CFU (G) 108 CFU (H) of E. coli K1 RS218 and on day 7 post-vaccination by IP, groups of vaccinated female BALB/c mice (n = 4 per group) were challenged with lethal doses of 107 CFU (I) of E. coli non-K1 S510. group of mice challenged with the S510 strain were immunized by IP. P-value indicate significant differences in a Mantel–Haenszel log-rank test. Error bars represent standard deviations (SD). Source data are provided as a Source Data file.
To further evaluate the protection conferred by our vaccine candidate against E. coli K1 infections, adult female mice immunized by IP route were challenged with two lethal doses (107 and 108 CFU/mouse) of three E. coli K1 strains (E11 WT, S88 and RS218). We also assessed the protection conferred by our vaccine against a E. coli non-K1 S510 (lethal dose: 107 CFU/mouse). All the vaccinated mice challenged with the three E. coli K1 strains and E. coli non-K1 S510 survived, up to 35 days after the infection. Conversely, we observed a 100% mortality rate within 24 h after nonvaccinated control mice were challenged with the same E. coli K1 strains (Fig. 4C–H). Mortality rates of 75% and 100% were observed at 48 and 72 h, respectively, in the nonvaccinated group infected with the E. coli non-K1 S510 strain (Fig. 4I). A 100% protection was also observed in adult challenged mice 60 days after immunization with E. coli strains K1 E11 WT, S88 and RS218 (Supplementary Fig. 3B–D).
Adult female mice immunized by the SC route were infected with a lethal dose 107 CFU/mouse by three strains of E. coli K1 (E11 WT, S88 and RS218). All the vaccinated mice challenged with the three E. coli K1 strains survived, up to 35 days after the infection. Conversely, we observed a 100% mortality rate within 24 h after nonvaccinated control mice were challenged with the same E. coli K1 strains (Supplementary Fig. 4A–C).
Taken as a whole, these results indicate that vaccination of a mouse model with the attenuated vaccine E. coli K1 E11 ∆aroA induced a strong polyclonal antibody-mediated humoral response and led to significant protection. In vitro, the vaccine-induced antibodies mediated the killing of E. coli K1. In vivo, our vaccine candidate protected adult mice against severe infections caused by E. coli K1 (E11 WT, S88 and RS218) and E. coli non-K1 (S510).
Evaluation of the presence of maternal antibodies in mouse pups
To assess the vertical transfer of maternal antibodies to mouse pups, female mice were immunized with three doses of our vaccine and then mated with male mice with the same BALB/c genetic background (Fig. 5A). The resulting pups were sacrificed at the age of 7 days. Blood samples were collected, and titers of E. coli K1-specific antibody were quantified in a whole-bacterial cell ELISA. We found antibodies able to bind to several strains of E. coli K1 in the sera of pups born to immunized mothers but not in the sera of pups born to nonvaccinated mothers (Fig. 5B). Western blot experiments confirmed that the maternal antibodies found in the sera of pups born to immunized mothers were specific and polyclonal (Supplementary Fig. 2H). Conversely, no specific, polyclonal antibodies were found in the serum of pups born to nonvaccinated mothers (Supplementary Fig. 2I). Taken as a whole, these results evidenced the vertical transfer of maternal antibodies to the pups.

A Seven days after the last vaccination dose, immunized and non-immunized BALB/c female mice were mated with BALC/c males. Newborn mice born to immunized and non-immunized mothers were sacrificed at Day 7 (n = 4) and their sera collected for (B) evaluation of the presence of maternal antibodies titers specific to E. coli K1 E11 WT, S88 and RS218 by whole-bacterial cell ELISA. Error bars represent standard deviations (SD). Source data are provided as a Source Data file.
The effect of maternal vaccination on the protection of the pups
The protection of pups born to vaccinated mothers by IP and SC route was evaluated at three and 7 days of life.
Three-day-old pups born to mothers immunized by IP were challenged with 105 CFU of E. coli K1 S88 (Fig. 6A), 105 CFU of E. coli RS218 (Fig. 6B), and 105 CFU of E. coli E11(Fig. 6C). Three-day-old pups from mothers immunized by SC were challenged with 105 CFU of E. coli K1 S88, 105 CFU of E. coli RS218, and 105 CFU of E. coli E11(Supplementary Fig. 4D–F) Very strong protection was observed against all these K1 strains, with 24 h mortality rates of 0% (0 out of 4) in pups born to vaccinated mothers versus 100% (4 out of 4) in pups born to nonvaccinated mothers.

A–C Three days after delivery, groups of four pups born to immunized by IP and non-immunized female mice were injected intraperitoneally with 105 CFU of E. coli K1 S88 (A), 105 CFU of E. coli K1 RS218 (B), and 105 CFU E. coli K1 E11 WT (C). Protection was assessed for 24 h. D–F Seven days after delivery, groups of four pups born to immunized by IP and non-immunized females were also given 106 CFU E. coli K1 E11 WT (D), 106 CFU E. coli K1 S88 (E) and 107 E. coli K1 RS218 (F). Seven days after delivery, groups of four pups born to immunized and non-immunized by IP females were also given 107 E. coli non-K1 S242 (G), and 107 E. coli non-K1 S510 (H). I The CFU count in the brain 24 h after infection with 106 CFU of E. coli K1 E11 WT bacteria in 7 day-old mouse pups. P-value values indicate significant and non-significant differences a Mantel–Haenszel log-rank test. Error bars represent standard deviations (SD). Source data are provided as a Source Data file.
In 7 day-old pups born to mothers immunized with IP and challenged with three K1 strains (106 CFU of E. coli E11 WT, 106 CFU of E. coli S88 and 106 CFU of E. coli RS218 strains), we also observed strong protection with 24 h mortality rates of 0% (0 out of 4) in pups born to vaccinated mothers versus 100% (4 out of 4) pups born to nonvaccinated mothers (Fig. 6D–F). The same complete protection was found for pups born to subcutaneously vaccinated mothers compared to pups born to unvaccinated mothers (Supplementary Fig. 4G–I). We also showed that the attenuated vaccine E. coli K1 E11 ∆aroA conferred the protection against two E. coli non-K1 strains (S242 and S510, 107 CFU) infecting 7 day-old pups: survival rates of 100% were observed in pups born to immunized mothers. In contrast, the 24 h mortality rates in mouse pups born to non-immunized dams were 75% (3 out of 4) for E. coli S242 infections and 40% (2 out of 5) for S510 infections (Fig. 6G, H). While we had previously reported a high level of bacteria in the brains of pups after an intraperitoneal injection of the WT E. coli K1 E1123, no bacteria were detected in the brains of the 7 day-old pups born to immunized mothers 24 h after the intraperitoneal injection (Fig. 6I).
Two weeks and 4 weeks old mice born to immunized mothers (IP route) were still completely protected against a lethal infection by E. coli K1 (Supplemental Fig. 3E, F).
Three-day-old pups mice born to mothers and immunized either with IP (Supplementary Fig. 3G, H) or SC (Supplementary Fig. 4J, K) were challenged by gavage with E. coli K1 strains. A 100% protection was found while a 50% mortality rate was observed in pups born from non-immunized mothers.
Taken as a whole, these in vivo results indicate that vertically transferred maternal antibodies can effectively protect newborns against severe infections caused by various E. coli K1and non-K1 strains.
Discussion
Antibiotic-resistant E. coli strains have been found in premature infants and in women who have given birth prematurely40,41. The effectiveness of advanced antibiotic therapy for E. coli K1 meningitis is limited by the emergence of antibiotic resistance in some E. coli K1 strains16,42,43. A recent study in France found that 37% of the E. coli K1 strains causing meningitis produced an extended-spectrum beta lactamase and were resistant to third-generation cephalosporins6. Even when meningitis is caused by E. coli strains susceptible to antibiotics, the post-treatment mortality and sequalae rates are high44,45. In view of these ongoing issues, a vaccine would be a rapid, effective, preventive option. The effectiveness of a vaccine is driven by its safety and its immunogenicity. It is known that attenuated vaccines induce rapid, long-lasting, effective immunity17,18,46,47. Although live attenuated vaccines are not recommended during pregnancy, they can be considered in women planning to conceive so that an immune response can be transferred to the infant. The results of our study indicate that the E. coli K1 E11 ∆aroA strain is a good candidate for an attenuated vaccine with high levels of immunogenicity and strong preclinical in vitro and in vivo protection. We selected E. coli E11 K1 ∆aroA as the basis for our attenuated vaccine candidate because (i) we previously found that aroA is a virulence factor for E. coli K1, and (ii) this approach has been successful with other pathogens26,27.
The specific immunity of newborns (including premature newborns) against pathogens relies mainly on maternal antibodies48,49. In contrast, maternal T cells are not involved because of maternal-fetal differences in tissue antigens (HLA in particular)48. We showed in vitro and in vivo the attenuation of the strain by deletion of the aorA gene. This attenuation is probably mediated for a significant part by the reduced expression of genes such as FimH encoding for the Type 1 fimbriae which is a well-recognized virulence factor for E. coli K131,32. The role of the fimbriae probably play an important role in the results found in the adherence and invasion assays, however, we also have to take into account that type 1 fimbriae expression is controlled by a genetic switch that can easily been turned off or on50. Our present results showed that vaccination with ∆aroA E. coli E11 K1 induced a very strong humoral immune response and produced a very high level of bactericidal activity. We detected a higher level of IgG2 isotype after vaccination. Of note, IgG2 has a high capacity to bind to a novel gamma chain-dependent IgG activating Fc receptor, FcgammaRIV, and has high protective and pathogenic properties51. Our results also showed that the antibodies induced by immunization with this vaccine candidate fully protected female mice against various lethal doses of E. coli K1 and non-K1 strains. Other studies have shown that maternal antibodies are transferred to their offspring via the placenta and breast milk49 and that these antibodies alone are enough to provide protection against perinatal infections16.
In the present study, we showed that pups born to immunized mothers contained maternal polyclonal antibodies that were specific for E. coli K1. This antibody response was specific to the K1 and non-K1 E. coli strains responsible for meningitis. The fact that the female mice were vaccinated prior to mating demonstrated the efficacious, long-lasting immune protection induced by the aroA mutant E. coli K1 vaccine candidate.
Furthermore, our results indicated that pups born to vaccinated mothers were efficaciously protected, since both 3 day-old pups52 and 7 day-old pups45,53 were protected against lethal doses of various virulent E. coli strains causing meningitis. Furthermore, no bacteria were detected in the brains of pups born to vaccinated mothers. No detectable T cell responses were found in vaccinated mothers, but this did not influence the degree of protection observed in the pups.
Maternal antibodies can access fetal neural tissue through the developing blood-brain barrier and can thus prevent infection by vertically transmitted pathogens32. Indeed, the K1 and non-K1 E. coli strains responsible for meningitis are able to cross the blood-brain barrier and multiply in the cerebrospinal fluid54.
Vaccination before or during pregnancy is useful in protecting newborn babies and pregnant women from serious infections55. The maternal antibodies induced by the vaccine can be transferred to the fetus and newborn via the placenta and breastfeeding, where they offer protection against specific micro-organisms. Maternal vaccination against the micro-organisms responsible for congenital and neonatal infections has therefore gain a major public health interest. Transplacental transfer of antibodies is a more natural, safer, more effective and less costly method of increasing neonatal antibody levels than administering immunoglobulin preparations to the infant55,56. However, the nature of the antigens and the type of vaccine administered during pregnancy also influence the effectiveness of antibody transfer to the fetus or newborn. Higher antibody titers have been observed in infants born to mothers immunized with conjugate vaccines compared with polysaccharide vaccines during pregnancy56,57.
It has also been shown that asymptomatic carriage of E. coli K1 strains in the maternal gut microbiota is positively correlated with the risk of vertical transmission to the infant at birth58,59. Eliminating E. coli K1 strains from the maternal microbiota could also be a solution. Celine et al have shown that strains can be eliminated using specific phages58. Since bacteremia is a primordial stage in the pathophysiology of E. coli K1 meningitis60,61, maternal vaccination induced by the transfer of specific IgG to newborns would be an excellent strategy for protecting newborns against neonatal E. coli K1 meningitis. Maternal vaccination could be an excellent way of better protecting offspring against neonatal E. coli K1 meningitis.
Our study shows that preconceptional vaccination with the E. coli K1 E11 ∆aroA vaccine induces strong immunity, driven by polyclonal bactericidal antibodies and protects not only mothers from infections during pregnancy, but also protects their offspring through vertical transmission of maternal immune effectors55. Maternal vaccination could be an excellent way of better protecting offspring against neonatal E. coli K1 infection and especially meningitis.
A limitation of our study is related to the transplacental transfer of IgG to the human fetus that occurs mainly during the last trimester of pregnancy and only reaches around 50% between 28- and 32 weeks’ gestation62. Therefore, while late preterm and at term neonates could potentially benefit greatly from the strategy described in this work, extremely preterm neonates born after <28 weeks gestation would probably benefit only to a limited extent from these protective maternal antibodies.
Another limitation of our study is the lack of evidence that prematurely born mice would be adequately be protected against severe E. coli infections. Further follow-up studies in larger preterm mammals, beyond the scope of this current work, may be able to prove this concept in the future.
However, despite these limitations, our study provides an excellent preclinical proof of concept that maternal immunization with our attenuated live vaccine can protect neonates against severe E. coli infections.
Given the very high mortality rate and the neurological sequalae associated with neonatal E. coli K1 meningitis in preterm infants, our results constitute preclinical proof of concept for the development of a live attenuated vaccine against severe E. coli infections in women at risk of preterm delivery. The strategy we suggest, would be to vaccinate women at high risk of preterm delivery and more particularly those with a history of preterm delivery who envisage a new pregnancy. The benefits of such vaccination could be multiple. They mainly concern the newborns through passive protection against E. coli K1 infections, but potentially also by reducing preterm delivery related to maternal infection. Finally, our approach could also protect the mothers from E. coli sepsis during pregnancy.
Given that (i) women having already given birth prematurely have a very high risk of a subsequent preterm delivery (in turn associated with a greater risk of severe neonatal infections), (ii) the most common severe neonatal infection of this type is bacterial meningitis, and (iii) E. coli in general and E. coli K1 strains in particular constitute the most frequent cause of neonatal meningitis in this population, our results constitute strong preclinical proof-of-concept for the development of a preconceptionally administered attenuated vaccine in this target population.
Methods
Ethical statement
The animal experiments were carried out at the Institut Imagine animal facility in Paris in compliance with current regulations (Directive 2010/63/EU of 22 September 2010 and Decree no. 2013-118 of 1 February 2013 on the protection of animals used for scientific purposes). The protocol was approved by an animal experimentation ethics committee approved by the French Ministry of Higher Education and Research (APAFIS number: 2020011519022360). Every effort has been made to minimize animal suffering. The animals come from an approved supplier and have SPF health status. SPF status considers the main pathogens in rodents and therefore makes it possible to establish a health status for “healthy” animals that are free from the main pathogens. On arrival, they are placed in a cage rack in an infectious A2 zone in cages containing nesting material and gnawing sticks. We also pay attention to social enrichment by limiting the isolation of our animals and we respect a 7 day acclamation period to allow the animals to recover from transport. The animals are also monitored every day, with appropriate limit points set up.
Bacteria and cells
The E. coli K1 and E. coli non-K1 strains were provided by Professor Stéphane Bonacorci, head of the French national reference center for E. coli (Table 1). The Hela CRM-CCL-2™ cell line was provided by the ATCC and maintained at 37 °C with 5% CO2 in Dulbecco’s high glucose modified Eagle’s medium (DMEM, Invitrogen, Carlsbad, CA, USA) with 10% fetal bovine serum (Dominique Dutscher, France).
Construction of the aroA mutant
The 1284-nucleotide aroA gene is present in the E. coli K1 E11 strain. The methodology used to delete the aroA gene in this strain was described by Datsenko in 200033. The technique is based on recombination between homologous sequences in the vicinity of the gene to be deleted and a previously generated DNA cassette. Recombination was facilitated by the Reda/Redb proteins encoded by the pRed plasmid. We used primers containing sequences (20 nucleotides) with homology to the kanamycin resistance cassette (1737 bp) contained in the genomic DNA of E. coli E11 ∆csga that we wished to amplify. These primers also contain 50-nucleotide sequences homologous to adjacent sequences to the aroA gene in E. coli E11 (Table 2). PCRs were used to generate a DNA product containing the kanamycin resistance cassette (1.7 kb), which was subsequently column-purified. The primer sequences are summarized in Table 2. The pRed plasmid was transferred into our E. coli strain by electroporation. Next, the strain was grown overnight on solid LB medium containing 100 µg/ml ticarcillin, in order to select bacteria containing the pRed plasmid. The resulting colonies were then re-isolated on LB agar plates containing 100 µg/ml ticarcillin and tested in a PCR assay with primers homologous to the ampicillin resistance gene contained in pRed. The proteins required for homologous recombination were induced by culturing E. coli plus pREd with L-arabinose. Next, the kanamycin resistance cassette with homology to sequences adjacent to the aroA gene was transferred into E. coli plus pRed by electroporation; the pRed plasmid is lost during this step following culture in liquid medium at 37 °C. Lastly, the bacteria were grown overnight on LB medium containing 20, 50 and 100 µg/ml kanamycin, in order to select mutants having received the kanamycin resistance cassette and lost the aroA gene through homologous recombination.
Bacterial growth curve
The WT and ∆aroA E. coli strains were grown at 37 °C in LB liquid and DMEM medium. During this period, bacterial growth was measured in terms of the optical density (OD) every hour for 8 h. The WT and ∆aroA E. coli K1 E11 strains were grown under the same conditions.
Growth in minimal medium M9
Wild type and ∆aroA Escherichia coli K1 E11 strains were grown for 48 h at 37 °C on M9 minimum medium (Sigma, France) with or without the addition of 40 µg/ml tryptophan, 40 µg/ml tyrosine, 40 µg/ml phenylalanine. A third condition with the addition of 2 times the amino acids was added. During this period, bacterial growth was measured by Optical Density.
Bacterial adhesion assays with epithelial cells
The two strains of E. coli K1 E11 (WT and ΔaroA) were cultured in LB liquid medium at 37 °C overnight. On the following day, the bacterial culture was diluted to obtain an OD600 of 0.05 and then incubated at 37 °C until an OD600 of between 0.6 and 0.7 was reached (corresponding to exponential growth). The strains were then pelleted by centrifugation at 5000 × g for 10 min at 4 °C. The resulting supernatant was discarded, and the pellet was washed twice with PBS and resuspended in DMEM without antibiotics (Invitrogen, Carlsbad, CA, USA). In parallel, Hela epithelial cells were grown in 24-well plates at 37 °C in a 5% CO2 humidified atmosphere for infection assays. The cells were then washed and incubated with the bacteria contained in the medium. The plates with infected Hela cells were placed at 37 °C in a humidified atmosphere at 5% CO2 and washed five times with PBS, to eliminate non-adherent bacteria. The adherent bacteria present at the bottom of the wells were lysed with 500 μL of 0.2% Triton X-100 for 10 min on ice. The cell suspension was then serially diluted 10-fold with PBS and plated on LB agar plates to determine the adhesion frequency. For the invasion test, the content of each plate with the Hela epithelial cells was washed after 1 h of infection and then cultured in medium containing 100 μg/mL of gentamicin at 37 °C for 3 h. Next, we washed the plates five times with PBS, to eliminate non-adherent bacteria. The adherent cells present at the bottom of the wells were lysed with 500 μL of 0.2% Triton X-100 for 10 min on ice. The cell suspension was then serially diluted 10-fold with PBS and plated on LB agar plates to determine the invasion frequency.
RNA-Seq analysis
E. coli K1 E11 strains WT and ∆aroA were grown in LB broth at 37 °C overnight. The following day, bacterial cultures of the 2 strains were grown from OD = 0.08 to exponential phage. At OD = 0.600, the bacteria were harvested and washed by centrifugation, then recovered in lysis buffer from the RNA extraction kit, Bioanalysis (Valencienner, Germany) reference 740955.50. Total RNA from both strains was extracted using this kit according to the manufacturer’s instructions. RNA concentration was quantified using a spectrophotometer (Nanodrop Technologies). RNA-Seq analysis was carried out by the Genotyping/Sequencing Platform of the Brain Institute—ICM, France. mRNA library preparation was realized following manufacturer’s recommendations (Stranded Total RNA Prep with Ribo-Zero Plus Kit from ILLUMINA). Final samples pooled library prep were sequenced on Nextseq 2000 ILLUMINA P2-200 cartridge (2x400Millions of 100 bases reads) corresponding to 2x14Millions of reads per sample after demultiplexing. RNA-Seq analysis was carried out by the Genotyping/Sequencing Platform of the Institut du Cerveau/Paris Brain Institute—ICM, France. Analysis of RNA sequencing data using CLC Genomics.
RNA extraction and q-RTPCR
E. coli K1 E11 strains WT and ∆aroA were grown in LB broth at 37 °C overnight and in DMEM. The following day, bacterial cultures of the 2 strains were grown from OD = 0.08 to exponential phage. At OD = 0.600, the bacteria were harvested and washed by centrifugation, then recovered in lysis buffer from the RNA extraction kit, Bioanalysis (Valencienner, Germany) reference 740955.50. Total RNA from both strains was extracted using this kit according to the manufacturer’s instructions. RNA concentration was quantified using a spectrophotometer (Nanodrop Technologies). For host gene expression, reverse transcription was performed using SuperScript™ III Platinum™ one-step RT-PCR (Life Technologies) and oligo(dT) primers. qPCR was performed using the Smart SYBRGreen fast Master kit (Roche Diagnostics) and specific primers targeting the FimH gene (Table 2) in a CFX Touch detection system (Bio-Rad). Thermal cycling was performed at 55 °C for 10 min for RT, followed by 95 °C for 3 min, then 45 cycles at 95 °C for 15 s and 58 °C for 30 s. Measurement of quantified gene expression was expressed as cycle threshold (Ct) values normalized against the bacterial housekeeping gene DnaE (Table 2) and expressed as relative quantification (RQ) = 2 -ΔCt with ΔCt = Ct Target -Ct DnaE.
Determination of the virulence of the WT and ΔaroA mutant strains
To assess the virulence of the WT and ΔaroA E. coli K1 E11 strains, we first determined the lethal dose by infecting 6 week-old female mice with different inoculums. For each strain, 20 mice were divided into five groups of four mice. The bacterial strains were grown in LB liquid medium up to an OD600 of 0.6-0.8. Next, the bacteria were washed twice with sterile phosphate buffered saline (PBS) and resuspended in NaCl. Mice in each group received an intraperitoneal injection of 1 × 109, 1 × 108, 1 × 107, 1 × 106 or 1 × 105, CFU of bacteria in 200 µl of NaCl. The mortality rate was observed over a 1 week period.
The antibody response of BALB/C female mice
To assess the immunogenicity of our E. coli K1 E11 ΔaroA strain against different clinical K1 and non-K1 E. coli strains, we performed a whole-bacterial-cell ELISA. First, we vaccinated a group of 6 week-old female mice with the mutant strain by the intraperitoneal (IP) and subcutaneous routes (SC) (Fig. 2A). In parallel, we administrated a placebo (NaCl) to a control group. Blood samples were taken from the retroorbital sinus 7 and 28 days after the last dose of vaccine or placebo. Antibody titers were assessed with the whole-bacterial-cell ELISA, according to standard methods63. To obtain heat-stable antigens from the various strains, bacteria were inactivated for 60 min in a water bath at 70 °C after an overnight culture in LB liquid at 37 °C. The culture media were then centrifuged at 20,000 × g for 10 min in a microcentrifuge. The pellets were resuspended in PBS and diluted to an OD600 of 0.1. Next, 100 µl of the different bacterial suspension were coated onto 96-well ELISA plates, which were incubated overnight at 37 °C. On the next day, 100 µl of bovine serum albumin (BSA) 1% were added to each well and incubated for 90 min at 37 °C. After washing with a mixture of PBS and Tween® 20 (Sigma-Aldrich, St. Louis, MO, USA), 100 µL of mice sera were added to each well and incubated for 2 h at 37 °C. Next, 100 µL of a 1:10000 dilution of anti-mouse secondary antibodies (rabbit anti-mouse IgG H&L, Abcam, Paris, France) coupled to horseradish peroxidase were added. A substrate was then used to reveal the reaction (TMB Liquid Substrate, TONBObioscience, San Diego, CA, USA).
Furthermore, we also inactivated the strain deleted from the aorA gene using a temperature of 70 °C for an hour, then immunized a group of mice with this strain and also evaluated their immunogenicity.
SDS-PAGE gel electrophoresis and Western blots
The three E. coli K1 strains (E11 WT, S88 and RS218) and the two non-K1 strains (S242 and S510) were cultured at 37 °C until an OD600 of 1.00 was reached. The culture media were centrifuged to collect the bacteria, which were then resuspended in 1 mL of RIPA lysis buffer (Sigma-Aldrich, St, Louis, MO, USA). Lysed samples were centrifuged, and 10 μL of the supernatant were electrophoresed in a 4–15% SDS-polyacrylamide gel (SDS-PAGE, BioRad, Marnes-la-Coquette, France). Proteins from gels not stained with Coomassie Blue reagent were transferred to nitrocellulose membranes using the Wet/Tank Blotting System and the Western Blotting Transfer System (BioRad, Marnes-la-Coquette, France), according to the manufacturer’s instructions. Next, mouse sera were pooled according to their immunized and non-immunized status and placed in contact with the nitrocellulose membranes overnight at 4 °C. On the next day, anti-mouse secondary antibodies (rabbit anti-mouse IgG H&L (ab6709), Abcam, Paris, France) coupled to horseradish peroxidase were diluted (1:5000 in PBS) and used to detect primary antibodies. A chemiluminescent substrate (ECL Revel-Blot®, Ozyme, Saint-Cyr-l’Ecole, France) was used to reveal the presence of specific, polyclonal antibodies against bacteria proteins.
Spleen cell phenotype analysis
Seven days after full immunization, BALB/c mice were sacrificed, and the spleens were collected for the flow cytometry analysis of lymphocytes. Red blood cells were removed from spleen cell suspensions by lysis with ammonium chloride buffer. The remaining cells were then incubated with LIVE/DEAD™ Fixable Aqua Dead Cell Stain Kit (Invitrogen L34957, Thermo Scientific Inc., Branchburg, NJ, USA) (Table 3) in PBS, according to the manufacturer’s instructions. Next, cells were surface-stained with anti-CD45 PerCP-Cy5.5 (BioLegend, France), anti-CD19 APCeF780 (eBioscience 47-0193-80, France) (Table 3), anti-TCRb AF700 (BioLegend 109224, France), anti-CD8 BV605 (BD Horizon 563152), and anti-CD4 PB (100534) (Table 3) in cold PBS containing 0.5% BSA. The cells were then fixed and permeabilized with True-Nuclear™ Transcription Factor Buffer Set (BioLegend 424401, France), according to the manufacturer’s instructions, and then stained with anti-FOXP3 allophycocyanin conjugate (Invitrogen 17-5773-82, Thermo Scientific Inc., Branchburg, NJ, USA) (Table 3) diluted in permeabilization buffer. Cells were then washed and resuspended in cold PBS containing 2% FCS. A Fortessa flow cytometer (BD Biosciences, San Jose, CA, USA) was used to analyze 105 stained cells. Doublets were excluded from the analysis by using appropriate forward scatter/side scatter gates. Each immune subpopulation was defined as follows: B cells = CD45+ TCRb- CD19 + , T cells = CD45 + CD19- TCRb + , CD4 T cells = CD45 + CD19- TCRb+ CD8- CD4 + , CD8 T cells = CD45 + CDs19- TCRb+ CD4- CD8 + , and regulatory T cells = CD45 + CD19- TCRb + CD8- CD4 + FOXP3 + . Data were analyzed with Flowjo software. The cell count for a selected population was expressed as a percentage of the total hematopoietic cell count.
A gating strategy example is provided in Supplemental Fig. 6.
Cytokine assays
Mouse cytokines (IL-10, IFN-γ, TNF-α, IL-4, IL-6, IL-2 and IL-17) in serum from immunized and non-immunized mice were assayed using the cytometric bead array (CBA) method (Becton Dickinson, Le Pont-de-Claix, France), according to the manufacturer’s instructions. The CBA data were acquired with a BD AccuriTM cytometer (Becton Dickinson, Le Pont-de-Claix, France) and analyzed using HEC software. The results of the cytokine assays were expressed in pg/mL, as determined from a standard curve.
The bactericidal activity assay
Serum bactericidal activity assays were performed to determine the activity of sera from immunized or non-immunized mice sera against three strains of E. coli K1 (E11 WT, S88, and RS218), according to methods described previously64,65. Briefly, the strains were grown overnight at 37 °C in LB liquid media and then diluted to an OD600 of 0.05. The dilutions were then incubated at 37 °C until an exponential growth was achieved (OD600 ~ 0.7). An appropriate volume of the culture medium was sampled to obtain 103 CFU. The bacteria were then washed twice and resuspended in PBS, without additional Mg2+ or Ca2+. Next, 10 μl of the bacterial suspensions were added to 10 μl of heat-inactivated immunized sera, 10 μl of 3–4 week-old baby rabbit complement (Pel-Freez® Biologicals, AR, Rogers, USA), and 10 μl of PBS in a 96-well plate, and incubated at 37 °C. After a 1 h incubation, serial dilutions in PBS enabled us to determine the amounts of viable bacteria in each reaction mixture, with plating on solid LB medium overnight at 37 °C. In parallel, the initial bacterial concentration was determined by serial dilution. Bacterial killing was calculated by comparing the concentration of viable E. coli at the beginning of the assay with that at the end of the assay. As negative controls, assays were performed with heat-inactivated sera from non-immunized mice. Bactericidal activity >30% in two or more dilutions was considered as a positive assay.
Evaluation of the protection conferred by the attenuated E. coli K1 E11 ΔaroA vaccine
To evaluate the degree of protection conferred by our live attenuated E. coli K1 E11 ΔaroA vaccine, several groups of 6 week-old female BALB/c mice were vaccinated (Fig. 2A). The vaccination schedule consisted of an intraperitoneal injection of a bacterial suspension (105 CFU of E. coli E11 ∆aroA in 200 µl of NaCl per adult female mouse) once a week for 3 weeks. One week after the third dose, the groups of mice received lethal doses (107 or 108 CFU) of different E. coli K1 and non-K1 strains responsible for neonatal meningitis. Outcomes were monitored for 35 days.
Evaluation of maternal vaccine antibody transfer and the protection of pups born to vaccinated mothers
To assess the protection of pup mice born to vaccinated mothers, groups of 6 week-old female BALB/c mice were immunized according to our vaccination schedule (Fig. 2A). In parallel, we administrated a same volume of a placebo (NaCl) to control mice. The different groups of female mice were matched with male mice. Three and 7 days after birth, two groups of four baby mice born to the vaccinated or nonvaccinated mothers as well as their mothers were sacrificed and their blood was collected to detect and quantify specific E. coli antibodies by whole-bacterial-cell ELISA and Western blots, respectively. Furthermore, groups of four pups (aged three and 7 days) from vaccinated or non-vaccinated mothers were given various doses of E. coli strains. The pups’ survival at 24 h was evaluated.
Data analysis
All data were analyzed using GraphPad Prism software (v9, GraphPad Software LLC, San Diego, CA, USA). Data are expressed as the mean ± standard deviation (SD). Groups were compared in a Mann-Whitney bilateral test, one-way ANOVA with correction for multiple comparisons or a Mantel–Haenszel log-rank test. The threshold for statistical significance was set to p < 0.05.
Reporting summary
Further information on research design is available in the Nature Portfolio Reporting Summary linked to this article.
Data availability
The authors declare that the data supporting the findings of this study are available within the article and its Supplementary Information files or are available from the authors upon request. Source data are provided with this paper. The RNAseq data have been deposited in NCBI. https://www.ncbi.nlm.nih.gov/geo/query/acc.cgi?acc=GSE252194. Source data are provided with this paper.
References
Vogel, J. P. et al. The global epidemiology of preterm birth. Best. Pract. Res. Clin. Obstet. Gynaecol. 52, 3–12 (2018).
Blencowe, H. et al. National, regional, and worldwide estimates of preterm birth rates in the year 2010 with time trends since 1990 for selected countries: a systematic analysis and implications. Lancet 379, 2162–2172 (2012).
Walani, S. R. Global burden of preterm birth. Int. J. Gynecol. Obstet. 150, 31–33 (2020).
Goldenberg, R. L., Culhane, J. F., Iams, J. D. & Romero, R. Epidemiology and causes of preterm birth. Lancet 371, 75–84 (2008).
Romero, R. et al. The preterm parturition syndrome. BJOG 113, 17–42 (2006).
Sikias, P. et al. Early-onset neonatal sepsis in the Paris area: a population-based surveillance study from 2019 to 2021. Arch. Dis. Child Fetal Neonatal Ed. 108, 114–120 (2023).
Collins, A., Weitkamp, J.-H. & Wynn, J. L. Why are preterm newborns at increased risk of infection? Arch. Dis. Child Fetal Neonatal Ed. 103, F391–F394 (2018).
Pammi, M. & Brocklehurst, P. Granulocyte transfusions for neonates with confirmed or suspected sepsis and neutropenia. Cochrane Database Syst. Rev. 2011, CD003956 (2011).
Bae, Y. M. et al. Effect of exogenous surfactant therapy on levels of pulmonary surfactant proteins A and D in preterm infants with respiratory distress syndrome. J. Perinat. Med 37, 561–564 (2009).
McGreal, E. P., Hearne, K. & Spiller, O. B. Off to a slow start: under-development of the complement system in term newborns is more substantial following premature birth. Immunobiology 217, 176–186 (2012).
Stoll, B. J. et al. Early-Onset Neonatal Sepsis 2015 to 2017, the Rise of Escherichia coli, and the Need for Novel Prevention Strategies. JAMA Pediatr. 174, e200593 (2020).
Dawson, K. G., Emerson, J. C. & Burns, J. L. Fifteen years of experience with bacterial meningitis. Pediatr. Infect. Dis. J. 18, 816–822 (1999).
Gaschignard, J., Levy, C., Bingen, E. & Cohen, R. Épidémiologie des méningites néonatales à Escherichia coli. Arch. de. Pédiatrie 19, S129–S134 (2012).
Krohn, M. A., Thwin, S. S., Rabe, L. K., Brown, Z. & Hillier, S. L. Vaginal colonization by Escherichia coli as a risk factor for very low birth weight delivery and other perinatal complications. J. Infect. Dis. 175, 606–610 (1997).
Gu, H. et al. Rational design and evaluation of an artificial Escherichia coli K1 protein vaccine candidate based on the structure of ompA. Front. Cell Infect. Microbiol. 8, 172 (2018).
Zhang, J. et al. Development of a chitosan‐modified PLGA nanoparticle vaccine for protection against Escherichia coli K1 caused meningitis in mice. J. Nanobiotechnol. 19, 69 (2021).
Patel, C. D. et al. Maternal immunization confers protection against neonatal herpes simplex mortality and behavioral morbidity. Sci. Transl. Med. 11, eaau6039 (2019).
Shan, C. et al. Maternal vaccination and protective immunity against Zika virus vertical transmission. Nat. Commun. 10, 5677 (2019).
Locht, C. & Mielcarek, N. Live attenuated vaccines against pertussis. Expert Rev. Vaccines 13, 1147–1158 (2014).
Gruslin, A. et al. Immunization in pregnancy. J. Obstet. Gynaecol. Can. 31, 1085–1101 (2009).
MPH, I. T. G. Vaccines For Women: Before Conception, During Pregnancy, And After a Birth. https://www.health.harvard.edu/blog/vaccines-for-women-before-conception-during-pregnancy-and-after-a-birth-2020011018649 (2020).
Ministry of Health, State of Israel. Vaccines for Women Before Pregnancy, During Pregnancy and After Childbirth. https://www.health.gov.il/English/Topics/Pregnancy/during/Pages/vaccine_pregnant.aspx (2024).
Pons, S. et al. A high-throughput sequencing approach identifies immunotherapeutic targets for bacterial meningitis in neonates. EBioMedicine 88, 104439 (2023).
Xing, X.-J. et al. Functional characterization of 5-enopyruvylshikimate-3-phosphate synthase from alkaliphilus metalliredigens in transgenic Arabidopsis. J. Microbiol. Biotechnol. 24, 1421–1426 (2014).
Lemaître, C. et al. The ssbL gene harbored by the ColV plasmid of an Escherichia coli neonatal meningitis strain is an auxiliary virulence factor boosting the production of siderophores through the shikimate pathway. J. Bacteriol. 196, 1343–1349 (2014).
Felgner, S. et al. aroA-deficient salmonella enterica serovar typhimurium is more than a metabolically attenuated mutant. mBio 7, e01220–16 (2016).
Priebe, G. P. et al. Construction and characterization of a live, attenuated aroA deletion mutant of pseudomonas aeruginosa as a candidate intranasal vaccine. Infect. Immun. 70, 1507–1517 (2002).
Galal, H. M., Abdrabou, M. I., Faraag, A. H. I., Mah, C. K. & Tawfek, A. M. Evaluation of commercially available aroA delated gene E. coli O78 vaccine in commercial broiler chickens under middle east simulating field conditions. Sci. Rep. 11, 1938 (2021).
Sebkova, A., Karasova, D., Crhanova, M., Budinska, E. & Rychlik, I. aro Mutations in salmonella enterica cause defects in cell wall and outer membrane integrity. J. Bacteriol. 190, 3155–3160 (2008).
Barbagelata, M. S. et al. Auxotrophic mutant of staphylococcus aureus interferes with nasal colonization by the wild type. Microbes Infect. 13, 1081–1090 (2011).
Liu, R. et al. CD48 and α7 nicotinic acetylcholine receptor synergistically regulate FimH-mediated escherichia coli K1 penetration and neutrophil transmigration across human brain microvascular endothelial cells. J. Infect. Dis. 219, 470–479 (2019).
Khan, N. A., Kim, Y., Shin, S. & Kim, K. S. FimH-mediated escherichia coli K1 invasion of human brain microvascular endothelial cells. Cell. Microbiol. 9, 169–178 (2007).
Datsenko, K. A. & Wanner, B. L. One-step inactivation of chromosomal genes in Escherichia coli K-12 using PCR products. Proc. Natl Acad. Sci. USA 97, 6640–6645 (2000).
Klemm, P. Two regulatory fim genes, fimB and fimE, control the phase variation of type 1 fimbriae in Escherichia coli. EMBO J. 5, 1389–1393 (1986).
Lemaître, C., Bidet, P., Bingen, E. & Bonacorsi, S. Transcriptional analysis of the Escherichia coli ColV-Ia plasmid pS88 during growth in human serum and urine. BMC Microbiol 12, 115 (2012).
Wijetunge, D. S. S. et al. Characterizing the pathotype of neonatal meningitis causing Escherichia coli (NMEC). BMC Microbiol 15, 211 (2015).
Pluschke, G., Mayden, J., Achtman, M. & Levine, R. P. Role of the capsule and the O antigen in resistance of O18:K1 Escherichia coli to complement-mediated killing. Infect. Immun. 42, 907–913 (1983).
Weiss, J., Victor, M., Cross, A. S. & Elsbach, P. Sensitivity of K1-encapsulated Escherichia coli to killing by the bactericidal/permeability-increasing protein of rabbit and human neutrophils. Infect. Immun. 38, 1149–1153 (1982).
Arredondo-Alonso, S. et al. Evolutionary and functional history of the Escherichia coli K1 capsule. Nat. Commun. 14, 3294 (2023).
Zhu, M. et al. Multi-drug resistant Escherichia coli causing early-onset neonatal sepsis—a single center experience from China. Infect. Drug Resist. 12, 3695–3702 (2019).
Li, Y. Y., Kong, C. W. & To, W. W. K. Pathogens in preterm prelabour rupture of membranes and erythromycin for antibiotic prophylaxis: a retrospective analysis. Hong. Kong Med J. 25, 287–294 (2019).
Yamamoto, T. et al. Electron microscopic structures, serum resistance, and plasmid restructuring of New Delhi metallo-β-lactamase-1 (NDM-1)-producing ST42 Klebsiella pneumoniae emerging in Japan. J. Infect. Chemother. 19, 118–127 (2013).
Blanco, J. et al. National survey of Escherichia coli causing extraintestinal infections reveals the spread of drug-resistant clonal groups O25b:H4-B2-ST131, O15:H1-D-ST393 and CGA-D-ST69 with high virulence gene content in Spain. J. Antimicrob. Chemother. 66, 2011–2021 (2011)
Liu, Y. et al. Escherichia coli causing neonatal meningitis during 2001–2020: a study in eastern China. Int J. Gen. Med 14, 3007–3016 (2021).
Basmaci, R. et al. Escherichia coli meningitis features in 325 children from 2001 to 2013 in France. Clin. Infect. Dis. 61, 779–786 (2015).
Shan, C. et al. A single-dose live-attenuated vaccine prevents Zika virus pregnancy transmission and testis damage. Nat. Commun. 8, 676 (2017).
Griffin, D. E. Measles vaccine. Viral Immunol. 31, 86–95 (2018).
Zinkernagel, R. M. Maternal antibodies, childhood infections, and autoimmune diseases. N. Engl. J. Med. 345, 1331–1335 (2001).
Hurley, W. L. & Theil, P. K. Perspectives on immunoglobulins in colostrum and milk. Nutrients 3, 442–474 (2011).
Stentebjerg-Olesen, B., Chakraborty, T. & Klemm, P. Type 1 fimbriation and phase switching in a natural Escherichia coli fimB null strain, nissle 1917. J. Bacteriol. 181, 7470–7478 (1999).
Nimmerjahn, F., Bruhns, P., Horiuchi, K. & Ravetch, J. V. FcgammaRIV: a novel FcR with distinct IgG subclass specificity. Immunity 23, 41–51 (2005).
Mendoza-Palomar, N. et al. Escherichia coli early-onset sepsis: trends over two decades. Eur. J. Pediatr. 176, 1227–1234 (2017).
Xu, M. et al. Etiology and clinical features of full-term neonatal bacterial meningitis: a multicenter retrospective cohort study. Front. Pediatr. 7, 31 (2019).
Xie, Y., Kim, K. J. & Kim, K. S. Current concepts on Escherichia coli K1 translocation of the blood-brain barrier. FEMS Immunol. Med Microbiol. 42, 271–279 (2004).
Sereme, Y., Toumi, E., Saifi, E., Faury, H. & Skurnik, D. Maternal immune factors involved in the prevention or facilitation of neonatal bacterial infections. Cell. Immunol. 395-396, 104796 (2024).
Kachikis, A. & Englund, J. A. Maternal immunization: optimizing protection for the mother and infant. J. Infect. 72, S83–S90 (2016).
Englund, J. A. et al. Transplacental antibody transfer following maternal immunization with polysaccharide and conjugate haemophilus influenzae Type B vaccines. J. Infect. Dis. 171, 99–105 (1995).
Antoine, C. et al. Phage targeting neonatal meningitis E. coli K1 In Vitro in the intestinal microbiota of pregnant donors and impact on bacterial populations. Int J. Mol. Sci. 24, 10580 (2023).
Glode, M. P., Sutton, A., Moxon, E. R. & Robbins, J. B. Pathogenesis of neonatal Escherichia coli meningitis: induction of bacteremia and meningitis in infant rats fed E. coli K1. Infect. Immun. 16, 75–80 (1977).
Kim, K. S. Strategy of Escherichia coli for crossing the blood-brain barrier. J. Infect. Dis. 186, S220–S224 (2002).
Doran, K. S. et al. Host-pathogen interactions in bacterial meningitis. Acta Neuropathol. 131, 185–209 (2016).
Palmeira, P., Quinello, C., Silveira-Lessa, A. L., Zago, C. A. & Carneiro-Sampaio, M. IgG placental transfer in healthy and pathological pregnancies. Clin. Dev. Immunol. 2012, 985646 (2012).
Fleiszig, S. Lipopolysaccharide outer core is a ligand for corneal cell binding and ingestion of Pseudomonas aeruginosa. Invest. Ophthalmol. Vis. Sci. 37, 976–986 (1996).
Lu, X. et al. A Poly-N-Acetylglucosamine−shiga toxin broad-spectrum conjugate vaccine for shiga toxin-producing Escherichia coli. mBio 5, e00974–14 (2014).
Granoff, D. M. Relative importance of complement-mediated bactericidal and opsonic activity for protection against meningococcal disease. Vaccine 27, B117 (2009).
Acknowledgements
We thank all the staff in the INEM group 1 and the staff in the Imagine Institute’s animal house for their assistance. We also thank Samantha Schaeffer (INSERM UMRS 1138, “Functional genomics of solid tumors” group), Iris Delavaud stagaire student, Amaury Gensou (Janvier Labs—Faxility-Management, Paris, France) for their assistance and support. DS received an award from the ANR (AAPG2020-Seq-N-Vaq, France), and an award from the Charles H. Hood Foundation.
Author information
Authors and Affiliations
Contributions
Y.S., D.S. designed the experiments and interpreted the results. Y.S. lead all in vitro and in vivo experiments. C.S., H.F., M.A., E.L.W., Y.C.M., E.A., E.P., E.F., and F.B. carried out experiments and analyzed data. S.B. participated in the design of the study and provided bacterial strains. MC., VT., analyzed data and contributed to the drafting and revision of the manuscript. Y.S., D.S. wrote the first draft of the paper. All co-authors worked on iterations of the manuscript. D.S. provided the funding, developed the study concept and supervised the project.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Peer review
Peer review information
Nature Communications thanks Peter Taylor, Esther Speer and David Gally for their contribution to the peer review of this work. A peer review file is available.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Source data
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Sereme, Y., Schrimp, C., Faury, H. et al. A live attenuated vaccine to prevent severe neonatal Escherichia coli K1 infections. Nat Commun 15, 3021 (2024). https://doi.org/10.1038/s41467-024-46775-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41467-024-46775-x
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
