
Abstract
The American Urological Association and Endocrine Society published guidelines for the management of testosterone deficiency in 2018. Testosterone prescription patterns have varied widely recently, owing to increased public interest and emerging data on the safety of testosterone therapy. The effect of guideline publication on testosterone prescribing is unknown. Thus, we aimed to assess testosterone prescription trends using Medicare prescriber data. Specialties with over 100 testosterone prescribers from 2016–2019 were analyzed. Nine specialties were included (in order of descending prescription frequency): family practice, internal medicine, urology, endocrinology, nurse practitioners, physician assistants, general practice, infectious disease, and emergency medicine. The number of prescribers grew by a mean of 8.8% annually. There was a significant increase in average claims per provider from 2016 to 2019 (26.4 to 28.7, p < 0.0001), with the steepest increase occurring between 2017 and 2018 when the guidelines were released (27.2 to 28.1, p = 0.015). The largest increase in claims per provider was among urologists. Advanced practice providers comprised 7.5% of Medicare testosterone claims in 2016 and 11.6% in 2019. While no causation can be established, these results suggest that professional society guidelines are associated with increasing numbers of testosterone claims per provider, especially among urologists. The changing demographics of prescribers justifies targeted education and further research.
Similar content being viewed by others
Introduction
Testosterone deficiency (TD) is a common condition affecting men with increasing prevalence as they age [1, 2]. Patients with TD present with a varied constellation of signs and symptoms, including muscle wasting, fatigue, osteoporosis, oligospermia, and obesity. Sexual dysfunction, such as erectile dysfunction and decreased libido, also represents a hallmark of the condition [3]. Testosterone therapy (TTh) is an increasingly common treatment for men diagnosed with TD.
As more clinicians recognize and diagnose TD among their patients, the use of TTh has increased in tandem. TTh use in the United States (US) increased by over 350% from 2001 to 2011. From 2007 to 2014, TTh prescriptions among patients insured with Medicare increased by 15.5% on average each year [4].
National trends in testosterone prescribing have fluctuated based on guidance from professional and regulatory organizations. In 2015, the US Food and Drug Administration issued a warning regarding increased cardiovascular risk in men over 65 receiving TTh. Not surprisingly, this was followed by a decrease in TTh prescriptions [5]. However, further research concluded that there was insufficient data to show a significant increase cardiovascular risk with use of TTh [6]. Following this determination, prescriptions for TTh have increased through 2017 [7].
In March of 2018, the Endocrine Society (ES) also released guidelines regarding TD, updating their prior guidelines from 2010 [8]. In August of the same year, the American Urological Association (AUA) released its inaugural guidelines regarding the evaluation and management of men with TD [9]. It is unknown how the release of these guidelines has affected testosterone prescribing patterns. The objective of this study was to evaluate TTh prescription trends before and after the release of the 2018 professional society guidelines. We hypothesized that there would be a significant increase in the average number of testosterone claims per provider with the release of new society guidelines.
Methods
Data was extracted from the Centers for Medicare and Medicaid Services (CMS) Part D Prescriber Public Use File, spanning the years 2016 to 2019. The CMS datasets report claim data for each Medicare prescriber over the course of the calendar year. The datasets were queried for providers who prescribed any modality of testosterone during the years analyzed.
We collected prescription information including year of prescription, testosterone claim count, and days of testosterone prescribed. Providers report their primary specialty when registering with CMS, and reported specialty was extracted from the National Provider Identifier (NPI) taxonomy data in CMS data. Specialties with fewer than 100 providers were excluded from the analysis.
Statistical analysis and creation of figures was performed using R (version 4.1.2). As the number of claims are non-normally distributed, the data was analyzed via generalized linear models. Both a Poisson and negative binomial model were fit, including specialty and year as predictors. The negative binomial model provided better fit to the data, as determined via a likelihood ratio test (χ2(1) = 1,186,779, p < 0.001). To assess overall change between 2016 and 2019, marginal estimates of the average number of prescriptions per prescriber were calculated. Pairwise comparisons of these estimates were calculated with the Tukey adjustment for multiple comparisons.
Results
In 2016 there were 20,532 total testosterone prescribers in the CMS dataset. This grew to 26,405 prescribers in 2019 (28.6% increase). Prescribers had 542,040 claims, representing a total of 23,722,979 days of testosterone supplied in 2016. In 2019, there were 751,976 claims (54.6% increase) for testosterone representing 33,004,554 days supplied (52% increase).
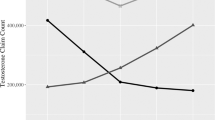
Nine specialties with over 100 TTh prescribers were identified for analysis (listed in order of descending number of prescribers): family practice, internal medicine, urology, endocrinology, nurse practitioners (NPs), physician assistants (PAs), general practice, infectious disease, and emergency medicine (Table 1). These nine specialties represented 96.5% of testosterone prescribers in 2016 and 96.8% of prescribers in 2019. From 2016 to 2019, each specialty had an increase in the number of testosterone prescribers, except for emergency medicine which had a 4% decline. NPs had the largest relative increase in prescribers (118%), followed by PAs (78%) and family practice (31%). Urology and endocrinology prescribers increased by 18% and 25% respectively (Fig. 1).

Total number of testosterone prescribers grouped by specialty plotted from 2016 to 2019.
The average number of claims per provider increased each year from 26.4 claims in 2016 to 28.1 in 2019 (p < 0.0001). Between 2016 and 2017 the average number of prescriptions increased by 0.62 from 26.38 to 27.00. If that same pace carried on, the expected rate would be 27.62 prescriptions in 2018 but was instead 28.1 (an increase of 1.1 prescriptions per provider). Between 2018 and 2019 there was an increase of 0.47 to 28.58. Focusing on consecutive years, only 2017 to 2018 demonstrated statistically significant differences in mean testosterone claims per provider (p = 0.015; 2016 to 2017, p = 0.33; 2018 to 2019, p = 0.60) (Fig. 2). Urologists had the largest increase in mean annual claims, from 37.8 in 2016 to 44.7 in 2019. During the same period, endocrinologist mean annual claims grew from 33.9 to 38.6 (Fig. 3).

Average number of testosterone claims per prescriber from 2016 to 2019 estimated from negative binomial regression model. Error bars represent 95% confidence intervals.

Violin plots showing the average number of testosterone claims per prescribers of each specialty from 2016 to 2019. Note the y-axis has been log transformed to better show the distribution.
NPs and PAs accounted for an increased share of testosterone claims from 2016 to 2019, growing from 4.1% to 6.6% and 3.4% to 5.0% respectively. Collectively, advanced practice providers (APP) were responsible for 7.5% of CMS testosterone claims in 2016 and 11.6% in 2019 (Fig. 4).

Stacked column chart showing the cumulative growth in total testosterone claims overall and of each specialty.
Discussion
We demonstrate a significant increase in testosterone prescriptions coinciding with the release of new TD management guidelines by the AUA and ES in 2018. This trend of rising testosterone prescriptions in CMS between 2016 to 2019 is consistent with years prior [7]. Our analysis highlights the statistically significant increase in the average annual claims per provider in 2018, the year of AUA and ES guideline publication, compared to the year prior, suggesting that the new guidelines are associated with higher prescriptions rates. This result is similar to a study on guideline effectiveness in pain management. After the CDC released the “Guideline for Prescribing Opioids for Chronic Pain” in 2016, there were fewer new prescriptions for opiates and the prescriptions were for shorter durations, effectively reversing the trends from years prior [10]. Our results suggest that the guidelines can function as an effective tool for changing practice patterns and educating providers.
Our study found the increase in claims was most pronounced in urologists, possibly because the guidelines were viewed more by urologists or are more trusted by urologists compared to other specialties. The ES guidelines appear to be more conservative than the AUA guidelines with a lower cut off for defining TD (264 ng/dL vs 300 ng/dL) and additional contraindications for TTh possibly explaining the higher number of claims per provider in urology compared to endocrinology [11].
The baseline annual increase in testosterone is likely in part from reasons unrelated to the guidelines. For one, the population of adults in the US over 65-year-old is increasing [12], and the incidence of low testosterone increases with age from a prevalence of 20% in men over 60, and 50% in men over 80 years of age [13]. At the same time, marketing for TTh, especially by direct-to-consumer (DTC) providers, has increased aggressively over recent years which may have increased disease awareness and demand for TTh [14]. Finally, several new modalities for exogenous testosterone administration had emerge during the years analyzed which may have further increased intertest among both prescribers and patients [15]. Guidelines can quickly become outdated in the setting of innovation. Societies must continuously evaluate the validity of guidelines as 1 in 5 recommendations become outdated within 3 years [16].
The proportion of APPs, such as NPs and PAs, in the urology workforce is projected to almost double between 2015 and 2035. Meanwhile, the number of full-time urologists is projected to decrease over time [17]. This changing landscape creates more opportunities for APPs to assume roles in which they are responsible for prescribing TTh, whether it be supervised in a physician’s office, independent practice, or in a DTC model. This trend is reflected in our study with an increasing proportion of TTh claims coming from APPs over the study period. Professional societies should recognize the increasing role of APPs and tailor guidelines and education as appropriate.
Infectious disease and emergency medicine make up a relatively small proportion of the total prescribers, however their inclusion is notable. The AUA recommends testing for TD in HIV men [9] and the ES recommends consideration of TTh for certain HIV men to reduce weight loss [8]. Infectious disease physicians are likely to be managing much of the care for these patients. There has been interest of emergency medicine physicians in evaluating for TD and prescribing TTh with recent articles promoting TD management in the urgent care setting [18] and online classes on TTh being led by emergency medicine physicians (https://nealrouzier.com/). Future study will be needed to see how the prescription practices of these two specialties evolve.
Further research is also needed to determine the trend of testosterone prescription claims during the COVID-19 pandemic, the growth of telehealth, and the increasing number of DTC websites offering TTh. Indeed, several companies are now providing DTC TTh such as TRT Nation (trtnation.com) and Regenx Health (https://www.regenxhealth.com). Prior studies have shown high variability in the degree to which these companies follow AUA guidelines regarding testing and treatment of TD [19]. Several companies prescribe testosterone for patients testing well above the established AUA and ES laboratory cut-offs for TD [20]. These companies represent a new avenue for patients to receive TTh without formal consultation with a trained provider leading to increased access to therapy but also the potential for substandard management.
While our study is strengthened by the use of national prescriber data, it is limited to information contained within CMS and thus does not capture commercial insurance claims, prescriptions from compounding pharmacies, or those paid with cash. In addition, the AUA guidelines recommended that “Commercially manufactured testosterone products should be prescribed rather than compounded testosterone, when possible,” which may have had a large effect on use of compounded formulations. Unfortunately, the large proportion of prescriptions where the specific formulation or modality of testosterone was unspecified in the CMS dataset prohibits analysis of modality prescribed without significant bias. While trends in testosterone modality usage are beyond the scope of this investigation, past studies have shown that there is significant variation between specialties [7]. Finally, our study focused on the guidelines’ association with prescription rates, we were not able to elucidate if providers actual adhered to the recommendations.
Conclusion
One thing remains clear: as the landscape of testosterone therapy continues to evolve, it becomes more complex with more stakeholders involved. Here we demonstrate an increase in the number of testosterone related claims to CMS. We also show an increased number of providers prescribing TTh and changing demographics of these providers coinciding with the release of AUA and ES TD guidelines published in 2018. Our results suggest the society guidelines educated testosterone providers and are associated with changing practice patterns, but further study to characterize the effect of the guidelines beyond TTh prescribing is warranted.
Data availability
Data used in this study was extracted from the CMS Part D Prescriber Public Use File which is publicly available at https://data.cms.gov/.
References
Harman SM, Metter EJ, Tobin JD, Pearson J, Blackman MR. Aging BLSo. Longitudinal effects of aging on serum total and free testosterone levels in healthy men. Baltimore Longitudinal Study of Aging. J Clin Endocrinol Metab. 2001;86:724–31.
Auerbach JM, Moghalu OI, Das R, Horns J, Campbell A, Hotaling J, et al. Evaluating incidence, prevalence, and treatment trends in adult men with hypogonadism in the United States. Int J Impot Res. 2021;34:762–8. https://doi.org/10.1038/s41443-021-00471-2.
Kumar P, Kumar N, Thakur DS, Patidar A. Male hypogonadism: symptoms and treatment. J Adv Pharm Technol Res. 2010;1:297–301.
Zhou CK, Advani S, Chaloux M, Gibson JT, Yu M, Bradley M, et al. Trends and patterns of testosterone therapy among U.S. male medicare beneficiaries, 1999 to 2014. J Urol. 2020;203:1184–90.
Baillargeon J, Kuo YF, Westra JR, Urban RJ, Goodwin JS. Testosterone prescribing in the United States, 2002–2016. JAMA. 2018;320:200–2.
Corona G, Rastrelli G, Di Pasquale G, Sforza A, Mannucci E, Maggi M. Testosterone and cardiovascular risk: meta-analysis of interventional studies. J Sex Med. 2018;15:820–38.
Carter IV, Callegari MJ, Jella TK, Mahran A, Cwalina TB, Muncey W, et al. Trends in testosterone prescription amongst medical specialties: a 5-year CMS data analysis. Int J Impot Res. 2022. https://doi.org/10.1038/s41443-021-00497-6.
Bhasin S, Brito JP, Cunningham GR, Hayes FJ, Hodis HN, Matsumoto AM, et al. Testosterone therapy in men with hypogonadism: an endocrine society clinical practice guideline. J Clin Endocrinol Metab. 2018;103:1715–44.
Mulhall JP, Trost LW, Brannigan RE, Kurtz EG, Redmon JB, Chiles KA, et al. Evaluation and management of testosterone deficiency: AUA guideline. J Urol. 2018;200:423–32.
Goldstick JE, Guy GP, Losby JL, Baldwin G, Myers M, Bohnert AS. Changes in initial opioid prescribing practices after the 2016 release of the CDC guideline for prescribing opioids for chronic pain. JAMA Netw Open. 2021;4:e2116860.
Zucker IJ, Masterson TA. Comparison of American Urological Association and Endocrine Society guidelines on testosterone replacement. Int J Impot Res. 2022;34:626–9. https://doi.org/10.1038/s41443-021-00477-w.
Colby SL, Ortman JM. Projections of the Size and Composition of the U.S. Population: 2014 to 2060. Population Estimates and Projections. Current Population Reports. P25-1143 [Internet]. US Census Bureau; 2015 [cited 2023 Mar 27]. Available from: https://eric.ed.gov/?id=ED578934.
Harman SM, Metter EJ, Tobin JD, Pearson J, Blackman MR. Longitudinal effects of aging on serum total and free testosterone levels in healthy men. J Clin Endocrinol Metab. 2001;86:724–31. https://doi.org/10.1210/jcem.86.2.7219.
Bandari J, Ayyash OM, Emery SL, Wessel CB, Davies BJ. Marketing and testosterone treatment in the USA: a systematic review. Eur Urol Focus. 2017;3:395–402.
Kresch E, Patel M, Lima TF, Ramasamy R. An update on the available and emerging pharmacotherapy for adults with testosterone deficiency available in the USA. Expert Opin Pharmacother. 2021;22:1761–71.
García LM, Sanabria AJ, Álvarez EG, Trujillo-Martín MM, Etxeandia-Ikobaltzeta I, Kotzeva A, et al. The validity of recommendations from clinical guidelines: a survival analysis. CMAJ. 2014;186:1211–9.
McKibben MJ, Kirby EW, Langston J, Raynor MC, Nielsen ME, Smith AB, et al. Projecting the urology workforce over the next 20 years. Urology. 2016;98:21–6.
Iyeke LO, Richman MJ. Evaluating decreased libido: the lowdown on low T. J Urgent Care Med. 2021;16:33–4.
Jesse E, Sellke N, Rivero MJ, Muncey W, Ghayda RA, Loeb A, et al. Practice comparison and cost analysis of direct-to-consumer telemedicine platforms offering testosterone therapy. J Sex Med. 2022;19:1608–15.
Dubin JM, Jesse E, Fantus RJ, Bennett NE, Brannigan RE, Thirumavalavan N, et al. Guideline-discordant care among direct-to-consumer testosterone therapy platforms. JAMA Intern Med. 2022;182:1321–3.
Author information
Authors and Affiliations
Contributions
All authors meet all four criteria for authorship, including. (1) Conceived and/or designed the work that led to the submission, acquired data, and/or played an important role in interpreting the results. (2) Drafted or revised the manuscript. (3) Approved the final version. (4) Agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Sellke, N., Omil-Lima, D., Sun, H.H. et al. Trends in testosterone prescription during the release of society guidelines. Int J Impot Res (2023). https://doi.org/10.1038/s41443-023-00709-1
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41443-023-00709-1
