
Abstract
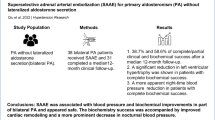
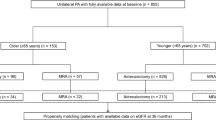
Superselective adrenal artery embolization (SAAE) is an effective treatment for patients with primary aldosteronism (PA). However, the impact of SAAE on renal function in the PA population remains uncertain. We investigated the estimated glomerular filtration rate (eGFR) and age, sex, body mass index, and diabetes-specific percentiles of eGFR residuals in 182 PA patients treated with SAAE in a prospective cohort from Nanchang SAAE in treating PA registry study. Data suggest that SAAE caused a significant decrease in eGFR from 91.9 ± 26.1 to 88.7 ± 24.1 ml/min/1.73 m2 (p < 0.05) after a median follow-up of 8 months in PA patients. Patients experienced a significant decrease in eGFR from 110.6 ± 18.9 to 103.8 ± 18.2 ml/min/1.73 m2 (p < 0.001) and a very slight increase from 71.1 ± 14.8 to 71.8 ± 17.8 ml/min/1.73 m2 (p = 0.770) with baseline eGFR ≥90 and <90 ml/min/1.73 m2, respectively. Patients with high eGFR residuals (glomerular hyperfiltration) experienced a significant decrease in their eGFR levels from 123.1 ± 22.6 to 105.0 ± 18.6 ml/min/1.73 m2 (p < 0.001). In contrast, there was no significant impact of SAAE on the eGFR of patients with normal or low eGFR residuals. The very early eGFR changes (24 h after SAAE) best predicted the effect of SAAE on eGFR changes after median of eight months in PA patients. On the whole, SAAE seems to have a beneficial impact on renal function in patients with PA, the results of which vary depending on the patient’s baseline eGFR and glomerular hyperfiltration status.

This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout



Similar content being viewed by others

References
Loh KC, Koay ES, Khaw MC, Emmanuel SC, Young WF Jr. Prevalence of primary aldosteronism among Asian hypertensive patients in Singapore. J Clin Endocrinol Metab. 2000;85:2854–9.
Monticone S, Burrello J, Tizzani D, Bertello C, Viola A, Buffolo F, et al. Prevalence and clinical manifestations of primary aldosteronism encountered in primary care practice. J Am Coll Cardiol. 2017;69:1811–20.
Rossi GP, Bernini G, Caliumi C, Desideri G, Fabris B, Ferri C, et al. A prospective study of the prevalence of primary aldosteronism in 1,125 hypertensive patients. J Am Coll Cardiol. 2006;48:2293–300.
Calhoun DA, Nishizaka MK, Zaman MA, Thakkar RB, Weissmann P. Hyperaldosteronism among black and white subjects with resistant hypertension. Hypertension. 2002;40:892–6.
Funder JW, Carey RM, Mantero F, Murad MH, Reincke M, Shibata H, et al. The management of primary aldosteronism: case detection, diagnosis, and treatment: an endocrine society clinical practice guideline. J Clin Endocrinol Metab. 2016;101:1889–916.
Rossi GP, Bernini G, Desideri G, Fabris B, Ferri C, Giacchetti G, et al. Renal damage in primary aldosteronism: results of the PAPY Study. Hypertension. 2006;48:232–8.
Sechi LA, Novello M, Lapenna R, Baroselli S, Nadalini E, Colussi GL, et al. Long-term renal outcomes in patients with primary aldosteronism. JAMA. 2006;295:2638–45.
Ribstein J, Du Cailar G, Fesler P, Mimran A. Relative glomerular hyperfiltration in primary aldosteronism. J Am Soc Nephrol. 2005;16:1320–5.
Stavropoulos K, Papadopoulos C, Koutsampasopoulos K, Lales G, Mitas C, Doumas M. Mineralocorticoid receptor antagonists in primary aldosteronism. Curr Pharm Des. 2018;24:5508–16.
Takeda M, Yamamoto K, Akasaka H, Rakugi H, Naruse M, Takeda Y, et al. Clinical characteristics and postoperative outcomes of primary aldosteronism in the elderly. J Clin Endocrinol Metab. 2018;103:3620–29.
Williams TA, Lenders JWM, Mulatero P, Burrello J, Rottenkolber M, Adolf C, et al. Outcomes after adrenalectomy for unilateral primary aldosteronism: an international consensus on outcome measures and analysis of remission rates in an international cohort. Lancet Diabetes Endocrinol. 2017;5:689–99.
Sam D, Kline GA, So B, Przybojewski SJ, Leung AA. Unilateral disease is common in patients with primary aldosteronism without adrenal nodules. Can J Cardiol. 2021;37:269–75.
Mulatero P, Stowasser M, Loh KC, Fardella CE, Gordon RD, Mosso L, et al. Increased diagnosis of primary aldosteronism, including surgically correctable forms, in centers from five continents. J Clin Endocrinol Metab. 2004;89:1045–50.
Hokotate H, Inoue H, Baba Y, Tsuchimochi S, Nakajo M. Aldosteronomas: experience with superselective adrenal arterial embolization in 33 cases. Radiology. 2003;227:401–6.
Sacks BA, Sacks AC, Faintuch S. Radiofrequency ablation treatment for aldosterone-producing adenomas. Curr Opin Endocrinol Diabetes Obes. 2017;24:169–73.
Fowler AM, Burda JF, Kim SK. Adrenal artery embolization: anatomy, indications, and technical considerations. AJR Am J Roentgenol. 2013;201:190–201.
Dong H, Zou Y, He J, Deng Y, Chen Y, Song L, et al. Superselective adrenal arterial embolization for idiopathic hyperaldosteronism: 12-month results from a proof-of-principle trial. Catheter Cardiovas Interv. 2021;97:976–81.
Qiu J, Li N, Xiong HL, Yang J, Li YD, Hu CK, et al. Superselective adrenal arterial embolization for primary aldosteronism without lateralized aldosterone secretion: an efficacy and safety, proof-of-principle study. Hypertens Res. 2023;46:1297–310.
Reincke M, Rump LC, Quinkler M, Hahner S, Diederich S, Lorenz R, et al. Risk factors associated with a low glomerular filtration rate in primary aldosteronism. J Clin Endocrinol Metab. 2009;94:869–75.
Sechi LA, Di Fabio A, Bazzocchi M, Uzzau A, Catena C. Intrarenal hemodynamics in primary aldosteronism before and after treatment. J Clin Endocrinol Metab. 2009;94:1191–7.
Iwakura Y, Morimoto R, Kudo M, Ono Y, Takase K, Seiji K, et al. Predictors of decreasing glomerular filtration rate and prevalence of chronic kidney disease after treatment of primary aldosteronism: renal outcome of 213 cases. J Clin Endocrinol Metab. 2014;99:1593–8.
Rossi GP, Auchus RJ, Brown M, Lenders JW, Naruse M, Plouin PF, et al. An expert consensus statement on use of adrenal vein sampling for the subtyping of primary aldosteronism. Hypertension. 2014;63:151–60.
Zhu JR, Gao RL, Zhao SP, Lu GP, Zhao D, Li JJ, et al. Guidelines for prevention and treatment of dyslipidemia in Chinese adults (2016 version). Chinese Circulation Journal. 2016;31:937–53, (in chinese).
Mellitus CCGftPaTosd. Clinical Guidelines for Prevention and Treatment of Type 2 Diabetes Mellitus in the Elderly in China (2022 Edition). Chinese Journal of Diabetes. 2022;30:2–51.
Levey AS, Coresh J, Balk E, Kausz AT, Levin A, Steffes MW, et al. National kidney foundation practice guidelines for chronic kidney disease: evaluation, classification, and stratification. Ann Intern Med. 2003;139:137–47.
Rowe C, Sitch AJ, Barratt J, Brettell EA, Cockwell P, Dalton RN, et al. Biological variation of measured and estimated glomerular filtration rate in patients with chronic kidney disease. Kidney Int. 2019;96:429–35.
Coresh J, Turin TC, Matsushita K, Sang Y, Ballew SH, Appel LJ, et al. Decline in estimated glomerular filtration rate and subsequent risk of end-stage renal disease and mortality. JAMA. 2014;311:2518–31.
Kwon SS, Lee H, Park BW, Kwon SH, Bang DW, Jeon JS, et al. Association of glomerular hyperfiltration with carotid artery plaque in the general population. Atherosclerosis. 2023;369:30–36.
Moriconi D, Sacchetta L, Chiriaco M, Nesti L, Forotti G, Natali A, et al. Glomerular hyperfiltration predicts kidney function decline and mortality in Type 1 and Type 2 diabetes: a 21-year longitudinal study. Diabetes Care. 2023;46:845–53.
D’Angelo MW. Transcatheter alcohol embolization of an aldosteronoma. Semin Interv Radio. 2007;24:96–9.
Salsamendi JT, Gortes FJ, Ayala AR, Palacios JD, Tewari S, Narayanan G. Transarterial embolization of a hyperfunctioning aldosteronoma in a patient with bilateral adrenal nodules. Radio Case Rep. 2017;12:87–91.
Van der Walt IS, Brown M, Lodh S. Adrenal gland-sparing transcatheter embolisation of an aldosteronoma for the treatment of refractory hypertension. Radio Case Rep. 2022;17:1088–94.
Zhou Y, Wang D, Liu Q, Hou J, Wang P. Case report: percutaneous adrenal arterial embolization cures resistant hypertension. Front Cardiovasc Med. 2022;9:1013426.
Kometani M, Yoneda T, Demura M, Karashima S, Mori S, Oe M, et al. The long-term effect of adrenal arterial embolization for unilateral primary aldosteronism on cardiorenovascular protection, blood pressure, and the endocrinological profile. Intern Med. 2016;55:769–73.
Inoue H, Nakajo M, Miyazono N, Nishida H, Ueno K, Hokotate H. Transcatheter arterial ablation of aldosteronomas with high-concentration ethanol: preliminary and long-term results. AJR Am J Roentgenol. 1997;168:1241–5.
Zhang H, Li Q, Liu X, Zhao Z, He H, Sun F, et al. Adrenal artery ablation for primary aldosteronism without apparent aldosteronoma: an efficacy and safety, proof-of-principle trial. J Clin Hypertens. 2020;22:1618–26.
Zhou Y, Liu Q, Wang X, Wan J, Liu S, Luo T, et al. Adrenal ablation versus mineralocorticoid receptor antagonism for the treatment of primary aldosteronism: a single-center prospective cohort study. Am J Hypertens. 2022;35:1014–23.
Sun F, Liu X, Zhang H, Zhou X, Zhao Z, He H, et al. Catheter-based adrenal ablation: an alternative therapy for patients with aldosterone-producing adenoma. Hypertens Res. 2023;46:91–99.
Zhao Z, Liu X, Zhang H, Li Q, He H, Yan Z, et al. Catheter-based adrenal ablation remits primary aldosteronism: a randomized medication-controlled trial. Circulation. 2021;144:580–82.
Huang KH, Yu CC, Hu YH, Chang CC, Chan CK, Liao SC, et al. Targeted treatment of primary aldosteronism - The consensus of Taiwan Society of Aldosteronism. J Formos Med Assoc. 2019;118:72–82.
Kimura G, Saito F, Kojima S, Yoshimi H, Abe H, Kawano Y, et al. Renal function curve in patients with secondary forms of hypertension. Hypertension. 1987;10:11–5.
Adolf C, Asbach E, Dietz AS, Lang K, Hahner S, Quinkler M, et al. Worsening of lipid metabolism after successful treatment of primary aldosteronism. Endocrine. 2016;54:198–205.
Kramers BJ, Kramers C, Lenders JW, Deinum J. Effects of treating primary aldosteronism on renal function. J Clin Hypertens. 2017;19:290–95.
Utsumi T, Kamiya N, Kaga M, Endo T, Yano M, Kamijima S, et al. Development of novel nomograms to predict renal functional outcomes after laparoscopic adrenalectomy in patients with primary aldosteronism. World J Urol. 2017;35:1577–83.
Kobayashi H, Abe M, Nakamura Y, Takahashi K, Fujita M, Takeda Y, et al. Association between acute fall in estimated glomerular filtration rate after treatment for primary aldosteronism and long-term decline in renal function. Hypertension. 2019;74:630–38.
Onohara T, Takagi T, Yoshida K, Iizuka J, Okumi M, Kondo T, et al. Assessment of postoperative renal function after adrenalectomy in patients with primary aldosteronism. Int J Urol. 2019;26:229–33.
Lu YC, Liu KL, Wu VC, Wang SM, Lin YH, Chueh SJ, et al. Factors associated with renal function change after unilateral adrenalectomy in patients with primary aldosteronism. Int J Urol. 2022;29:831–37.
Kotchen TA, Piering AW, Cowley AW, Grim CE, Gaudet D, Hamet P, et al. Glomerular hyperfiltration in hypertensive African Americans. Hypertension. 2000;35:822–26.
Funding
The present study was funded by the National Natural Science Foundation of China (81960088).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Lai, ZQ., Fu, Y., Liu, JW. et al. The impact of superselective adrenal artery embolization on renal function in patients with primary aldosteronism: a prospective cohort study. Hypertens Res 47, 944–958 (2024). https://doi.org/10.1038/s41440-023-01503-8
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41440-023-01503-8
Keywords
This article is cited by
-
Re: The impact of superselective adrenal artery embolization on renal function in patients with primary aldosteronism: a prospective cohort study
Hypertension Research (2024)
-
The application of superselective adrenal artery embolization in primary aldosteronism: evaluation, challenges, and response to Mr. Cabrelle and his team
Hypertension Research (2024)
-
Salt and seasonal variation research in Asia
Hypertension Research (2024)
-
Accumulating evidence suggests the potential of selective adrenal artery embolization as a standard treatment for primary aldosteronism
Hypertension Research (2024)
