
Abstract
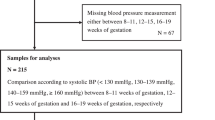
To analyze the relationship between the level of BP achieved with treatment and the risk for development of preeclampsia/eclampsia (PE), we conducted a historical cohort study on 149 consecutive pregnant women with treated chronic hypertension, evaluated between January 1, 2016, and November 31, 2022. According to office BP readings and ambulatory blood pressure monitoring (ABPM) performed after 20 weeks of gestation, the cohort was classified in controlled hypertension, white-coat uncontrolled hypertension, masked uncontrolled hypertension and sustained hypertension. Risks for the development of PE were estimated using logistic regression. One hundred and twenty-four pregnant women with a control BP evaluation were included in this analysis. The rates of PE were 19.4%, 27.3%, 44.8% and 47.1% for controlled, white-coat uncontrolled, masked uncontrolled and sustained uncontrolled hypertension, respectively. Compared with women with controlled hypertension, the relative risk for PE increased markedly in women with sustained uncontrolled (OR 3.69, 95% CI, 1.19–11.45) and masked uncontrolled (OR 3.38, 95% CI, 1.30–11.45) hypertension, but not in those with white-coat uncontrolled (OR 1.56 95% CI, 0.36–6.70); adjustment for covariates did not modify the results. Each mmHg higher of systolic and diastolic daytime ABPM increased the relative risk for PE ~4% and ~5%, respectively. Each mmHg higher of systolic and diastolic nocturnal BP increased the risk ~5% and ~6%, respectively. When these risks were adjusted for ABPM values in opposite periods of the day, only nocturnal ABPM remained as a significant predictor. In conclusion, masked uncontrolled hypertension implies a substantial risk for the development of PE, comparable to those of sustained uncontrolled. The presence of nocturnal hypertension seems important.

This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout


Similar content being viewed by others


References
Ananth CV, Duzyj CM, Yadava S, Schwebel M, Tita ATN, Joseph KS. Changes in the prevalence of chronic hypertension in pregnancy, United States, 1970 to 2010. Hypertension. 2019;74:1089–95.
Greene MF, Williams WW. Treating hypertension in pregnancy. N Engl J Med. 2022;386:1846–7. https://doi.org/10.1056/NEJMe2203388.
Sinkey RG, Battarbee AN, Bello NA, Ives CW, Oparil S, Tita ATN. Prevention, diagnosis, and management of hypertensive disorders of pregnancy: a comparison of international guidelines. Curr Hypertens Rep. 2020;22:66.
Garovic VD, Dechend R, Easterling T, Karumanchi SA, McMurtry Baird S, Magee LA, et al. Hypertension in pregnancy: diagnosis, blood-pressure goals, and pharmacotherapy: a scientific statement from the American Heart Association. Hypertension. 2022;79:e21–41.
Tita AT, Szychowski JM, Boggess K, Dugoff L, Sibai B, Lawrence K, et al. Treatment for mild chronic hypertension during pregnancy. N Engl J Med. 2022;386:1781–92.
Abalos E, Duley L, Steyn DW, Gialdini C. Antihypertensive drug therapy for mild to moderate hypertension during pregnancy. Cochrane Database Syst Rev. 2018;10:CD002252.
Webster LM, Conti-Ramsden F, Seed PT, Webb AJ, Nelson-Piercy C, Chappell LC. Impact of antihypertensive treatment on maternal and perinatal outcomes in pregnancy complicated by chronic hypertension: a systematic review and meta-analysis. J Am Heart Assoc. 2017;6:e005526.
Magee LA, von Dadelszen P, Rey E, Ross S, Asztalos E, Murphy KE, et al. Less-tight versus tight control of hypertension in pregnancy. N Engl J Med. 2015;372:407–17.
Magee LA, von Dadelszen P. Treatment for mild chronic hypertension during pregnancy. N Engl J Med. 2022;387:664 https://doi.org/10.1056/NEJMc2207889.
Gleeson PJ, O’Seaghdha CM. Treatment for mild chronic hypertension during pregnancy. N Engl J Med. 2022;387:663–4. https://doi.org/10.1056/NEJMc2207889.
Salazar MR, Espeche WG, Leiva Sisnieguez BC, Balbín E, Leiva Sisnieguez CE, Stavile RN, et al. Significance of masked and nocturnal hypertension in normotensive women coursing a high-risk pregnancy. J Hypertens. 2016;34:2248–52. https://doi.org/10.1097/HJH.0000000000001067.
Salazar MR, Espeche WG, Leiva Sisnieguez CE, Juliano PL, Vulcano MV, Sanchez Caro L, et al. Masked hypertension and neonatal outcome in high-risk pregnancies. J Hum Hypertens. 2023;37:36–41. https://doi.org/10.1038/s41371-021-00649-7.
Salazar MR, Espeche WG, Leiva Sisnieguez CE, Minetto J, Balbín E, Soria A, et al. Nocturnal hypertension and risk of developing early-onset preeclampsia in high-risk pregnancies. Hypertens Res. 2021;44:1633–40. https://doi.org/10.1038/s41440-021-00740-z.
Espeche WG, Salazar MR, Minetto J, Leiva Sisnieguez CE, Cerri G, Balbín E, et al. Hypertension arising after 20 weeks of gestation: gestational hypertension or masked chronic hypertension? J Hum Hypertens. 2023;37:813–7. https://doi.org/10.1038/s41371-022-00767-w.
The jamovi project. jamovi (Version 2.3) [Computer Software]. 2022. https://www.jamovi.org.
R Core Team. R: a language and environment for statistical computing (Version 4.1) [Computer software]. 2021. https://cran.r-project.org (R packages retrieved from MRAN snapshot January 1, 2022).
Abe M, Arima H, Yoshida Y, Fukami A, Sakima A, Metoki H, et al. Optimal blood pressure target to prevent severe hypertension in pregnancy: a systematic review and meta-analysis. Hypertens Res. 2022;45:887–99. https://doi.org/10.1038/s41440-022-00853-z.
Ueda A, Hasegawa M, Matsumura N, Sato H, Kosaka K, Abiko K, et al. KAMOGAWA study group. Lower systolic blood pressure levels in early pregnancy are associated with a decreased risk of early-onset superimposed preeclampsia in women with chronic hypertension: a multicenter retrospective study. Hypertens Res. 2022;45:135–45. https://doi.org/10.1038/s41440-021-00763-6.
Ohkuchi A, Ichihara A. Tight control of blood pressure in pregnant women with nonsevere hypertension: expectations for decreasing adverse maternal and fetal pregnancy outcomes. Hypertens Res. 2022;45:926–8. https://doi.org/10.1038/s41440-022-00881-9.
Sánchez RA, Boggia J, Peñaherrera E, Barroso WS, Barbosa E, Villar R, et al. Ambulatory blood pressure monitoring over 24 h: a Latin American Society of Hypertension position paper-accessibility, clinical use and cost effectiveness of ABPM in Latin America in year 2020. J Clin Hypertens (Greenwich). 2020;22:527–43. https://doi.org/10.1111/jch.13816.
Villar R, Sánchez RA, Boggia J, Peñaherrera E, Lopez J, Barroso WS, et al. Recommendations for home blood pressure monitoring in Latin American countries: a Latin American Society of Hypertension position paper. J Clin Hypertens (Greenwich). 2020;22:544–54. https://doi.org/10.1111/jch.13815.
Bilo G, Parati G. Ambulatory blood pressure monitoring: a mandatory approach in high-risk pregnancy? J Hypertens. 2016;34:2140–2. https://doi.org/10.1097/HJH.0000000000001113.
Yang WY, Melgarejo JD, Thijs L, Zhang ZY, Boggia J, Wei FF, et al. Association of office and ambulatory blood pressure with mortality and cardiovascular outcomes. JAMA. 2019;322:409–20. https://doi.org/10.1001/jama.2019.9811.
Hoshide S. Nocturnal hypertension-solving the puzzle of preeclampsia risk. Hypertens Res. 2021;44:1681–2. https://doi.org/10.1038/s41440-021-00770-7.
Lv LJ, Ji WJ, Wu LL, Miao J, Wen JY, Lei Q, et al. Thresholds for ambulatory blood pressure monitoring based on maternal and neonatal outcomes in late pregnancy in a southern Chinese population. J Am Heart Assoc. 2019;8:e012027. https://doi.org/10.1161/JAHA.119.012027.
Acknowledgements
We acknowledge Luz Salazar Landea for the final English corrections.
Author information
Authors and Affiliations
Contributions
All the authors have seen and approved the final version.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Salazar, M.R., Espeche, W.G., Minetto, J. et al. Uncontrolled and masked uncontrolled blood pressure in treated pregnant women with chronic hypertension and risk for preeclampsia/eclampsia. Hypertens Res 46, 2729–2737 (2023). https://doi.org/10.1038/s41440-023-01443-3
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41440-023-01443-3
Keywords
This article is cited by
-
More need to optimize the prediction model of sFlt- 1/PIGF ratio and ambulatory blood pressure monitoring in preeclampsia
Hypertension Research (2024)
-
Mitigating preeclampsia risk through effective uncontrolled blood pressure management
Hypertension Research (2024)
