
Abstract
Growing epidemiological evidence has shown an association of the urinary sodium (Na) to potassium (K) ratio (Na/K ratio) with blood pressure and cardiovascular diseases. However, no clear cutoff level has been defined. We investigated the cutoff level of the urinary Na/K ratio under different dietary guidelines for Japanese individuals, especially that endorsed by the 2020 revised Japanese Dietary Reference Intakes (DRIs). A population of 1145 Japanese men and women aged 40 to 59 years from the INTERMAP study was examined. Using high-quality standardized data, the averages of two 24 h urinary collections and four 24 h dietary recalls were used to calculate the 24 h urinary and dietary Na/K ratios, respectively. Associations between the urinary and dietary Na/K ratios were tested by sex- and age-adjusted partial correlation. The optimal urinary Na/K ratio cutoff level was determined by receiver operating characteristic (ROC) curves and sex-specific cross tables for recommended dietary K and salt. Overall, the average molar ratio of 24 h urinary Na/K was 4.3. We found moderate correlations (P < 0.001) of the 24 h urinary Na/K ratio with 24 h urinary Na and K excretion (r = 0.52, r = −0.49, respectively) and the dietary Na/K ratio (r = 0.53). ROC curves showed that a 24 h urinary Na/K ratio of approximately 2 predicted Na and K intake that meets the dietary goals of the Japanese DRIs. The range of urinary Na/K ratios meeting the dietary goals of the Japanese DRIs for both Na and K was 1.6‒2.2 for men and 1.7‒1.9 for women. Accomplishing a urinary Na/K ratio of 2 would be desirable to achieve the DRIs dietary goals for both Na and K simultaneously in middle-aged Japanese men and women accustomed to Japanese dietary habits. This observational study is registered at www.clinicaltrials.gov as NCT00005271.
Similar content being viewed by others

Introduction
Regardless of whether 24 h measurement or casual spot urine is used, repeated urinary collection is considered an objectively reliable measure to estimate an individual’s habitual consumption level of sodium (Na) and potassium (K) from the excreted Na and K in the urine, respectively [1,2,3,4,5]. Cumulative evidence has shown that the sodium-to-potassium (Na/K) ratio is a more important measure in relation to blood pressure (BP) and cardiovascular diseases (CVDs) than Na and K alone [2, 6,7,8,9]. Several studies have shown a linear positive relationship between the urinary Na/K ratio and hypertension and CVDs [6, 8,9,10,11,12,13,14]. Therefore, monitoring the urinary Na/K ratio is a useful and valid estimate of the dietary intake of Na and K as a method for disease prevention.
Thus far, established dietary guidelines have identified intake goals for Na and K among different populations. In April 2020, the Japanese Ministry of Health, Labor and Welfare revised the Dietary Reference Intakes (DRIs) for Japanese individuals and set the dietary goal for salt intake to be less than 7.5 g/day for men (Na < 2.95 g/day [128.3 mmol/day]) and less than 6.5 g/day for women (Na < 2.56 g/day [111.3 mmol/day]) [15]. The daily K intake goal according to the DRIs did not change from the previous guideline, which was set to at least 3 g/day for men (77 mmol/day) and at least 2.6 g/day for women (67 mmol/day) [15]. Other dietary guidelines differ regarding the dietary intake goal of Na and K. The 2012 World Health Organization (WHO) guidelines recommend a Na intake of less than 2 g/day (equivalent to <85 mmol/day), a salt equivalent intake of 5.1 g/day, and a K intake of at least 3.51 g/day (equivalent to ≥90 mmol/day) [16, 17], whereas the 2019 dietary guidelines of the Japanese Society of Hypertension (JSH) recommended a salt intake of less than 6 g/day (equivalent to Na < 2.36 g/day [102.6 mmol/day]) [18].
Although a few multiethnic studies suggested a preferable urinary Na/K ratio cutoff range between 1‒2 molar ratios using standard dietary guidelines [8, 19, 20], a cutoff value exclusive to the Japanese population following the recently revised DRIs guidelines has not yet been investigated. Additionally, to estimate if the dietary intakes of salt (Na equivalent) and K matches the recommendations proposed by the DRIs guidelines, the excretion of these elements in urine could help in dietary goal assessment and adjusting dietary habits using the urinary Na/K ratio. The relevance of this knowledge will serve to update the guidelines for the optimal urinary Na/K ratio cutoff level and promote individualized dietary plans and the careful monitoring of urinary excretion. Therefore, we investigated the cutoff level of the urinary Na/K ratio in a middle-aged Japanese population from an international cooperative epidemiological study using high-quality data from two 24 h urine collections and four 24 h dietary recalls.
Methods
Study population
The participants were from the INTERnational study of MAcro- and micronutrients and blood Pressure (INTERMAP), an epidemiological investigation conducted between 1997 and 1999 aiming to clarify the role of macro- and micronutrient intakes on BP using high quality standardized data collection. This study surveyed 4680 randomly selected men and women aged 40‒59 years from four countries (China, Japan, the UK, and the US). Detailed methods are described elsewhere [21, 22]. Here, we analyzed the INTERMAP data of 1145 Japanese participants from four study centers: Sapporo, Toyama, Aito Town, and Wakayama. Each participant had four 24 h dietary recalls, two complete timed 24 h urine collections, and eight BP measurements from four visits to their local research center. Each of the local research centers provided institutional ethics committee approval, and all participants provided written informed consent. This observational study is registered as NCT00005271.
Demographic characteristics, lifestyle data collection, and measurements
The demographic characteristics, lifestyle data and medical data were obtained using interviewer-assisted questionnaires, including height, weight (both measured at the first and third visits), alcohol intake, smoking status, sociodemographic characteristics, physical activity level, vitamin/mineral supplement use, medical history and medication use. Body mass index (BMI) was calculated as weight (kg) divided by height squared (m2). At each of the four visits, two systolic blood pressures (SBPs) and diastolic blood pressures (DBPs) were measured by trained staff using a random-zero sphygmomanometer with an adjustable cuff size on the right arm after the participant was seated for at least 5 min in a quiet room [21]. We used the average of the eight total BP measurements. Alcohol intake was recorded at the 1st and 3rd visits for the preceding 7 days, and a total of 14 days of alcohol consumption recall was obtained. The weekly average alcohol consumption in mL was calculated, and participants were grouped into 0 mL/week, 1‒299 mL/week, and ≥300 mL/week.
Dietary recall data collection
The four 24 h dietary recalls were divided into two pairs of successive days, and the pairs had intervals of 3‒6 weeks. One of the days selected for dietary recall was on a day following a weekend. Dietary data were collected and tape-recorded by trained certified interviewers using the in-depth multipass 24 h recall method, recording all food, drinks and supplements consumed in the previous 24 h [22]. The study center’s nutritionist listened to and checked all the dietary recall tapes. Participants were excluded from the study if (1) they did not attend any of the four visits to their local research center, (2) the dietary data collected were considered unreliable, or (3) any of the 24 h dietary recall energy intakes were <500 kcal/day or >5000 kcal/day. Data collected from the 24 h dietary recall were used to calculate nutrient intake using the Japanese INTERMAP food table compiled by a Japanese nutritionist based on the Japanese Standard Food Tables 4th edition in cooperation with the Nutrition Coordination Center [23, 24]. The average of the four 24 h dietary recalls was used, the dietary Na and K intakes were calculated as mmol/day, and the dietary Na/K ratio was calculated as mmol/mmol.
Urine collection
At the 1st and 3rd visits, after participants emptied their bladder at the study center and received 2 of the standard 1 L plastic jars with boric acid for preservation, an observer timed the start of 24 h urinary collection for participation, and participants returned the following day (visits 2 and 4) to complete the 24 h urinary collection. Participants were asked to repeat their urine collection when (1) they reported “more than few drops” of missing urine, (2) the collection time fell outside the range of 22‒26 h, or (3) the total volume of urine was <250 mL. Participants were excluded from the study if they did not submit two complete urine collections. Urine aliquots were frozen and air-freighted to the Central Laboratory (Leuven, Belgium) [21]. To ensure quality control, 10% of the urine samples were randomly split at the study centers and forwarded to the laboratory under a different ID number. Emission flame photometry was used to measure the concentrations of urinary Na and K, which were reported as mmol/day. The average of the two 24 h urinary collections was used, and the 24 h Na/K ratio was calculated from the 24 h Na and K urinary excretion values obtained.
Statistical analysis
Continuous and categorical variables are presented as the mean ± standard deviation (SD) and numbers (%), respectively. Na and K concentrations were converted from mmol/day to g/day, calculated as g/day = [mmol/day x atomic weight (Na = 23.0, K = 39.1)]÷1000. The 24 h estimated dietary salt (NaCl) intake was calculated as g/day, enumerated as NaCl (g/day) = dietary Na intakex2.54. Pearson’s partial correlation coefficient, adjusted for sex and age, and Pearson’s correlation coefficient were used to examine the correlation between the 24 h dietary Na/K ratio and 24 h urinary Na/K ratio, the 24 h dietary Na/K ratio and dietary Na and K intake, and the 24 h urinary Na/K ratio and urinary Na and K excretion. The partial correlation coefficient was reported for the overall population, and Pearson’s correlation coefficient was reported and stratified by sex. The Bland‒Altman method was used to examine the bias of agreement between the 24 h urinary and dietary Na/K ratios.
The 24 h urinary K excretion is a good estimate of the dietary K intake; however, an average of 63‒77% of the dietary K intake is reflected in the urinary K excretion [24,25,26,27,28]. To approximate the urinary K excretion to dietary K intake, we calculated a population-specific correction coefficient derived from the INTERMAP Japanese population by dividing the population’s average of two 24 h urinary K excretions by the population’s average of four 24 h dietary K intakes: correction coefficient = 48.9÷71.5 = 0.684. We then divided the 24 h urinary K excretion by the correction coefficient to calculate the corrected urinary K excretion equivalent to the dietary K intake. The corrected urinary K excretion was used in all the following analyses. Based on the dietary intake standards recommended by the 2020 Japanese DRIs for each sex and the overall population (men: Na intake < 2.95 g/day [NaCl < 7.5 g/day] and K intake ≥ 3 g/day; women: Na intake < 2.56 g/day [NaCl < 6.5 g/day], and K intake ≥ 2.6 g/day), receiver operating characteristic (ROC) curves were used to explore the relationships between (1) the 24 h urinary excretion of Na and K and 24 h urinary Na/K ratio, (2) the 24 h dietary intake of Na and K and 24 h dietary Na/K ratio, and (3) the 24 h dietary intake of Na and K and 24 h urinary Na/K ratio. The area under the receiver operating characteristic curve (AUC) was examined for the explored relationships and cutoff level satisfying the Japanese DRIs guidelines by sex. The Na/K ratio cutoff level was reported as follows: (1) the distance to 0,1: closest cutoff to (0,1) perfect prediction [minimum distance to X = 0, Y = 1], \({{{{{{{\mathrm{d}}}}}}}} = \sqrt {\left( {1 - {{{{{{{\mathrm{sensitivity}}}}}}}}} \right)^2 + \left( {1 - {{{{{{{\mathrm{specificity}}}}}}}}} \right)^2}\); (2) sensitivity = specificity: cutoff point equates to near equal sensitivity and specificity; and (3) the Youden index: the maximum vertical line from the uninformative line, Youden index = sensitivity+specificity −1 [29, 30]. ROC curves and cutoff values were also examined following the dietary intake guidelines of the WHO and JSH [16,17,18]. To test the accuracy of predicting urinary and dietary Na and K by the Na/K ratio under the range of cutoff values of less than 2.0, 3.0 and 4.0 by the DRIs guidelines, sensitivity and specificity tests were performed.
For clinical implementation purposes, Japanese-specific guidance tables were created to visualize the estimated urinary Na/K ratio by the dietary K intake estimated from the corrected urinary K excretion and the dietary salt intake estimated from the 24 h urinary Na excretion based on the Japanese DRIs dietary goals. Both dietary K intake and salt intake are presented in g/day. The molar urinary Na/K ratio was presented as the range of the mean ± SD by subtracting the SD value from the mean to calculate the lower limit and adding the SD to the mean value to calculate the upper limit. Following the Japanese DRIs guidelines, dietary salt intake (g/day) was divided into four groups: < 5, 5‒7.5, 7.5‒12, and ≥12 for men, and < 5, 5–6.5, 6.5–10, and ≥10 for women. Dietary K intake from the corrected urinary K excretion (g/day) was divided into three groups: < 2, 2‒3, and ≥3 for men, and <1.8, 1.8‒2.6, and ≥2.6 for women. The cross-classified tables are presented as a heatmap by sex with dietary salt intake in rows and dietary K intake in columns, displayed in a color-shaded matrix with the color expressing the severity of the range of the mean urinary Na/K ratio as follows: ≥6 (red), 3‒6 (yellow), 2–3 (green), and <2 (blue). All analyses were performed using SAS software, version 9.4 (SAS Institute, Cary, NC).
Results
A total of 1145 Japanese participants from the INTERMAP study were analyzed in this study. Table 1 shows the characteristics of the overall participants by sex (574 men and 571 women). Among the overall participants, the average age was 49.4 ± 5.3 years, and 6.4% were taking hypertension medications. The average 24 h estimated dietary salt intake was 11.8 ± 3.2 g/day, and the average 24 h dietary K intake was 71.5 ± 18.0 mmol/day. The average estimated 24 h urinary salt excretion was 11.6 ± 3.3 g/day, and the corrected 24 h urinary K excretion was 71.4 ± 19.8 mmol/day. The average molar ratios of 24 h dietary and urinary Na/K were 3.0 ± 0.7 and 4.3 ± 1.3, respectively. The mentioned characteristics were observed to be higher in men.
Sex- and age-adjusted Pearson’s partial correlation coefficients for the 24 h urinary Na/K ratio with Na and K excretion were 0.52 and −0.49, respectively, while those with Na and K intake were 0.20 and −0.27, respectively (P < 0.001) (Supplementary Tables 1, 2, 3). Pearson’s correlation coefficients were examined by sex (Supplementary Tables 2 and 3), and the correlation coefficients for the 24 h urinary Na/K ratio with Na and K excretion were slightly higher for women. The bias between the 24 h dietary and urinary Na/K ratios using the Bland‒Altman method showed good agreement (bias 1.31) (Supplementary Fig. 1).
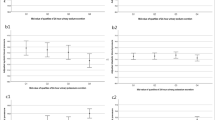
Figures 1 and 2 show the ROC curves of the 24 h urinary and dietary Na/K ratios based on the DRIs-recommended dietary Na and K intake for men (Na < 2.95 g/day [128.3 mmol/day], K ≥ 3 g/day [77 mmol/day]) and women (Na < 2.56 g/day [111.3 mmol/day], K ≥ 2.6 g/day [67 mmol/day]), respectively. Table 2 shows the cutoff level for predicting urinary and dietary Na and K by 24 h urinary and dietary Na/K ratios following the DRIs dietary goals by sex. Using the three determining methods of the optimal cutoff level, most of the 24 h urinary Na/K ratio values predicting Na and K excretion separately following the DRIs dietary goals by sex fell between 3 and 4. The AUC for the relationship between the 24 h urinary Na/K ratio and dietary Na and K intakes was the lowest compared with those for the 24 h urinary Na/K ratio and urinary Na and K excretion and the 24 h dietary Na/K ratio and dietary Na and K intakes. The ROC curves and AUCs of the 24 h urinary and dietary Na/K ratios based on the DRIs recommendations for both dietary Na and K intakes together in the overall INTERMAP population showed higher predictivity than each element alone (Fig. 3). The cutoff of approximately 2 for the urinary Na/K ratio showed better predictions of estimated Na and K intakes by the guidelines’ recommended levels.

The area under the receiver operating characteristic curve (AUC) of the 24 h urinary and dietary Na/K ratio based on the DRIs recommendations for Na and K dietary intake for men (N = 574). A Predicting Na excretion and dietary intake by the 24 h urinary Na/K ratio and dietary Na/K ratio (DRI for men: Na < 2.95 g/day [128.3 mmol/day] or salt < 7.5 g/day) B Predicting K excretion and dietary intake by the 24 h urinary Na/K ratio and dietary Na/K ratio (DRI for men: K ≥ 3 g/day [77 mmol/day]). U-Na urinary sodium, D-Na dietary sodium, U-K urinary potassium, D-K dietary potassium, U-Na/K urinary Na/K, D-Na/K dietary Na/K

The area under the receiver operating characteristic curve (AUC) of the 24 h urinary and dietary Na/K ratio based on the DRIs recommendations for Na and K dietary intake for women (N = 571). A Predicting Na excretion and dietary intake by the 24 h urinary Na/K ratio and dietary Na/K ratio (DRI for women: Na <2.56 g/day [111.3 mmol/day] or salt <6.5 g/day). B Predicting K excretion and dietary intake by the 24 h urinary Na/K ratio and dietary Na/K ratio (DRI for women: K ≥ 2.6 g/day [67 mmol/day]). U-Na urinary sodium, D-Na dietary sodium, U-K urinary potassium, D-K dietary potassium, U-Na/K urinary Na/K, D-Na/K dietary Na/K

The area under the receiver operating characteristic curve (AUC) of the 24 h urinary and dietary Na/K ratio based on the DRIs recommendations for Na and K dietary intake by sex in the overall INTERMAP population (N = 1145). Predicting Na and K excretion and dietary intake by the 24 h urinary Na/K ratio and dietary Na/K ratio (Na for men: <7.5 g/day (Na < 2.95 g/day [128.3 mmol/day]) and for women: <6.5 g/day (Na < 2.56 g/day [111.3 mmol/day]) and (K for men: K ≥ 3 g/day [77 mmol/day] and for women: K ≥ 2.6 g/day [67 mmol/day]). U-Na urinary sodium, D-Na dietary sodium, U-K urinary potassium, D-K dietary potassium, U-Na/K urinary Na/K, D-Na/K dietary Na/K
The AUCs and cutoff levels were also examined for the 24 h urinary Na/K ratio based on the recommended guidelines of the WHO dietary goals for Na and K and the JSH dietary goal for Na (Supplementary Tables 4 and 5 and Supplementary Figs 2 and 3). The cutoff threshold for the 24 h urinary Na/K ratio predicting Na and K separately under these two guidelines was similar to the DRIs threshold ranging between 3 and 4.
Additionally, in the sensitivity and specificity analysis of the 24 h urinary and dietary Na and K predicted by the Na/K ratio, the cutoff value between 3 and 4 seemed to show better predictions for each element separately (Supplementary Tables 6, 7).
The Japanese sex-specific guidance tables for the 24 h urinary Na/K ratio under the DRIs dietary goals for Na intake (presented as salt intake estimated from urinary Na excretion) and K intake (presented as dietary K intake in g/day estimated from the corrected urinary K excretion) showed the optimal 24 h urinary Na/K ratio range between 1.6 and 2.2 for men when the dietary K intake was greater than or equal to 3 g/day and the dietary salt intake was less than 7.5 g/day (the number of men meeting both dietary intake recommendations was 4). For women, the optimal 24 h urinary Na/K ratio range was between 1.7 and 1.9 when the dietary K intake was greater than or equal to 2.6 g/day and the dietary salt intake was less than 6.5 g/day (the number of women meeting both dietary intake recommendations was 5) (Fig. 4).

Range (means ± standard deviations) and number of participants in each category of the 24 h urinary Na/K ratio, cross classified by estimated salt and K intake by sex. A In men (N = 574), and B in women (N = 571). Color-shaded matrix guide of the range of the mean urinary Na/K ratio: red, urinary Na/K ratio ≥6, yellow, urinary Na/K ratio of 3–6, green, urinary Na/K ratio of 2-3, blue, urinary Na/K ratio <2. The DRIs dietary goal of salt intake of <7.5 g/day (Na < 2.95 g/day [128.3 mmol/day]) for men and <6.5 g/day (Na < 2.56 g/day [111.3 mmol/day]) for women. The daily K intake goal is ≥3 g/day for men (77 mmol/day) and ≥2.6 g/day for women (67 mmol/day). N.A. not applicable, SD standard deviation, K potassium
Discussion
In this study, we investigated the cutoff level of the 24 h urinary Na/K ratio in middle-aged Japanese men and women based on three dietary guidelines, mainly the Japanese DRIs. Overall, the 24 h urinary Na/K ratio showed better predictions of Na and K than the 24 h dietary Na/K ratio. The ROC curve of the 24 h urinary Na/K ratio at a cutoff of approximately 2 predicted combined Na and K dietary intake based on the recommended DRIs guidelines by sex. Furthermore, the range of urinary Na/K ratios to meeting both Na and K dietary goals simultaneously shown in the cross-classified tables was 1.6‒2.2 for men and 1.7‒1.9 for women. Advocating for a urinary Na/K ratio of approximately 2 would be desirable to achieve the goals for both Na and K intake recommended by the Japanese DRIs, which takes into account the habitual diet of the Japanese population.
It is widely accepted that 24 h urine collection is the most reliable measure for assessing the dietary intake of Na and K in clinical and epidemiological studies. Previous reports have shown an association between the urinary 24 h Na/K ratio and BP [7, 8, 13, 19]. Although the estimation of the dietary intake of these nutrients from 24 h urine collection is valid, it is inconvenient and involves considerable burden for participants in epidemiological studies and patients in clinical settings. Existing evidence shows, with appropriate bias correction, that the mean of 6 random daytime spot urine samples is a suitable estimate of an individual’s Na/K ratio, substituting for 2-day 24 h urine collection. The Pearson correlation coefficient of the means of the 24 h urine and spot urine Na/K ratio was r = 0.96 across different INTERSALT populations [3, 4]. In this study, we used the average of 2 repeated 24 h urine collections to estimate the Na/K ratio, which is the first study in the Japanese population using high standard repeated measurements of 24 h urine collection. Even though comparable high-quality studies are limited due to its high burden and low feasibility and more population-based evidence is needed to solidify the findings in this paper, the use of spot urine to estimate the Na/K ratio is an affordable, practical substitute and is comparable to the 24 h urinary Na/K ratio.
Both the 24 h urinary and dietary Na/K ratios predicted urinary and dietary Na and K under the sex-specific DRIs dietary goals, and overall, the urinary Na/K ratio showed slightly better predictions than the dietary Na/K ratio. A paper from the INTERSALT study used casual and 24 h urinary Na/K ratios to predict Na intake following the WHO dietary goal of Na < 85 mmol/day (Na < 2 g/day [salt intake < 5 g/day] [20]. They showed that the 24 h urinary Na/K ratio was a better predictor than casual urine samples, with an AUC similar to our findings (24 h urine Na/K ratio AUC=0.84). In addition, they found that the 24 h urinary Na/K ratio could predict Na intake under the WHO dietary goal with a sensitivity over 90% when the Na/K ratio was less than 1. In the current study, the cutoff level of urinary 24 h Na/K predicting Na intake following the sex-specific DRIs dietary goal was between 3 and 4 for Na and K separately; however, the cutoff level of approximately 2 for both elements simultaneously was deemed to be appropriate. Nevertheless, the gap between the two studies could be due to the lower dietary goal of the WHO and the relatively lower K intake in Japanese individuals.
An additional note seen from the sensitivity and specificity results of the current paper reveals that participants with lower Na dietary intake also show a tendency to have lower K intake. In the dietary recommendations, it is important to emphasize decreasing Na intake and increasing K intake to balance out the estimated Na/K ratio and reach the proposed threshold in this paper.
The sex-specific cross-classified tables of salt and K intakes showed a desirable range of the mean 24 h urinary Na/K ratio to meet the DRIs dietary goals for both Na and K with a range of 1.6‒2.2 for men and 1.7‒1.9 for women. It is important to mention that the total number of participants meeting both dietary goals recommended by the DRIs was only 9, which was <1% of the 1145 participants. Nevertheless, this is the first study to try and establish sex-specific dietary goals for salt and K intakes evaluated by the urinary Na/K ratio. The suggested optimal range of the urinary Na/K ratio is relevant to the proposed level of urinary Na/K cutoff value of approximately 2 [8, 19, 20]. Compared to international dietary guidelines for the two elements, the Japanese dietary guideline recommendations are considerably high for Na (salt equivalent) and low for K. One of the reasons is to accommodate the special dietary habits and sources of intake for Na and K in the Japanese diet. Additionally, although the international guidelines of strict dietary intake to reach a Na/K ratio of 1 could be difficult to achieve in some populations and would require drastic changes in dietary habits nationwide, it is important to advocate for the proper threshold considering the applicability of the proposed level per population; we conclude that a cutoff level of approximately 2 used for our Japanese participants may help them achieve the recommended dietary goal for both Na and K simultaneously and it is not far from the internally proposed threshold and guidelines. Several papers emphasized the importance of setting a practical cutoff level of the Na/K ratio, which is appropriate for the population’s dietary habits and is applicable for implementation in medical practice to follow the diet and health of the population [20, 31, 32]. The implications of this study’s findings of the cutoff value for the urinary Na/K ratio might instigate further population-based studies to help establish an acceptable and practical guidelines for estimating dietary salt and K intake using the urinary Na/K ratio in a middle-aged Japanese population.
This study has some limitations. First, the study participants were from the Japanese population of middle-aged individuals aged 40 to 59 years. It is difficult to apply the findings to other countries and younger or older age groups. Second, in the sex-specific cross-classified table, the number of participants meeting the goals for both salt and K intake following the Japanese DRIs guidelines was low (4 men and 5 women), which might be due to the low amount of raw and leafy vegetables as a source of K in the Japanese diet. Third, 24 h urine collection is the gold standard for measuring Na and K excretion; nonetheless, it is an impractical measure for monitoring population intake of these elements. A more feasible measure, such as repeated spot urine samples, might be a future approach to confirm the cutoff level of the urinary Na/K ratio. Finally, the data were collected more than 20 years ago, which may affect the relationship of dietary and urinary Na and K values considering the changes in health habits, medications, and dietary intake sources of these elements, among other factors. However, we believe the application of our findings from the matrix tables of the urinary Na/K ratio by salt and K intake are important, and further studies are needed to investigate similar concepts with recent data. There are noteworthy strengths to this study. We used high-quality standardized data in a general population from two 24 h urine collections, which is the gold standard for assessing salt intake. Finally, the average of two urinary collections and four dietary recalls were used, which would be a representative measure of the actual habitual intake compared to a single measure.
Perspective of Asia
The WHO recommends strict daily intake goals for Na (<2 g/day) and K ( > 3.51 g/day), which yields Na/K ratio of ≤1.0 measured by urinary excretion [16, 17]. However, this study concluded that a urinary Na/K ratio cutoff level of approximately 2 was feasible for simultaneously meeting the daily goals for both Na and K in the Japanese DRIs guidelines. Following the local recommendations was deemed appropriate to accommodate the dietary supply and habitual consumption of food by the Japanese population.
In Japan and other Asian countries, it is important to use the proposed Na/K ratio as an index to monitor the dietary intake of these essential health elements, especially in Asia, where the diet is composed of high salt and low potassium intake, leading to an imbalance of these elements by daily recommendations.
In conclusion, in the general middle-aged Japanese population, a 24 h urinary Na/K ratio cutoff level of approximately 2 would be desirable to simultaneously achieve dietary goal recommendations for both Na and K and may help the population meet the recommended dietary goals for Na and K intake by the Japanese DRIs. An achievable level of the 24 h urinary Na/K ratio could serve as a better approach to help advocate for lowering Na intake and increasing K intake in the Japanese population.
References
Pietinen PI, Findley TW, Clausen JD, Finnerty FA Jr, Altschul AM. Studies in community nutrition: estimation of sodium output. Prev Med. 1976;5:400–7.
Kogure M, Hirata T, Nakaya N, Tsuchiya N, Nakamura T, Narita A, et al. Multiple measurements of the urinary sodium-to-potassium ratio strongly related home hypertension: TMM Cohort Study. Hypertens Res. 2020;43:62–71.
Iwahori T, Ueshima H, Miyagawa N, Ohgami N, Yamashita H, Ohkubo T, et al. Six random specimens of daytime casual urine on different days are sufficient to estimate daily sodium/potassium ratio in comparison to 7-day 24-h urine collections. Hypertens Res. 2014;37:765–71.
Iwahori T, Miura K, Ueshima H, Chan Q, Dyer AR, Elliott P, Stamler J, et al. Estimating 24-h urinary sodium/potassium ratio from casual (‘spot’) urinary sodium/potassium ratio: the INTERSALT Study. Int J Epidemiol. 2017;46:1564–72.
Meyer HE, Johansson L, Eggen AE, Johansen H, Holvik K. Sodium and Potassium Intake Assessed by Spot and 24-h Urine in the Population-Based Tromsø Study 2015-6. Nutrients 2019;11(7):1619.
INTERSALT Co-operative Research Group. INTERSALT: an international study of electrolyte excretion and blood pressure: results for 24-hr urinary sodium and potassium excretion. BMJ 1988;297:319–28.
Tzoulaki I, Patel CJ, Okamura T, Chan Q, Brown IJ, Miura K, et al. A nutrient-wide association study on blood pressure. Circulation 2012;126:2456–64.
Cook NR, Obarzanek E, Cutler JA, Buring JE, Rexrode KM, Kumanyika SK, et al. Joint effects of sodium and potassium intake on subsequent cardiovascular disease: the Trials of Hypertension Prevention follow-up study. Arch Intern Med. 2009;169:32–40.
Kogure M, Nakaya N, Hirata T, Tsuchiya N, Nakamura T, Narita A, et al. A. Correction: Sodium/potassium ratio change was associated with blood pressure change: possibility of population approach for sodium/potassium ratio reduction in health checkup. Hypertens Res 2021;44:262 https://doi.org/10.1038/s41440-020-00547-4. Erratum for: Hypertens Res. 2021; 44(2):225-31
Tabara Y, Takahashi Y, Kumagai K, Setoh K, Kawaguchi T, Takahashi M, et al. Descriptive epidemiology of spot urine sodium-to-potassium ratio clarified close relationship with blood pressure level: the Nagahama study. J Hypertens. 2015;33:2407–13.
Higo Y, Nagashima S, Tabara Y, Setoh K, Kawaguchi T, Takahashi Y, et al. Association of the spot urine sodium-to-potassium ratio with blood pressure is independent of urinary Na and K levels: The Nagahama study. Hypertens Res. 2019;42:1624–30.
Hedayati SS, Minhajuddin AT, Ijaz A, Moe OW, Elsayed EF, Reilly RF, et al. Association of urinary sodium/potassium ratio with blood pressure: sex and racial differences. Clin J Am Soc Nephrol. 2012;7:315–22.
Binia A, Jaeger J, Hu Y, Singh A, Zimmermann D. Daily potassium intake and sodium-to-potassium ratio in the reduction of blood pressure: a meta-analysis of randomized controlled trials. J Hypertens. 2015;33:1509–20.
Hisamatsu T, Lloyd-Jones DM, Colangelo LA, Liu K. Urinary sodium and potassium excretions in young adulthood and blood pressure by middle age: the Coronary Artery Risk Development in Young Adults (CARDIA) Study. J Hypertens. 2021;39:1586–93.
Ministry of Health, Labour and Welfare of Japan. Dietary Reference intakes for Japanese (2020) (Japanese version).
World Health Organization (WHO). WHO Guideline: Sodium intake for adults and children. Geneva, 2012.
World Health Organization (WHO). WHO Guideline: Potassium intake for adults and children. Geneva, 2012.
Umemura S, Arima H, Arima S, Asayama K, Dohi Y, Hirooka Y, et al. The Japanese Society of Hypertension Guidelines for the Management of Hypertension (JSH 2019). Hypertens Res. 2019;42:1235–481.
Stamler J, Rose G, Stamler R, Elliott P, Dyer A, Marmot M. INTERSALT study findings. Public health and medical care implications. Hypertension. 1989;14:570–7.
Iwahori T, Miura K, Ueshima H, Tanaka-Mizuno S, Chan Q, Arima H, et al. Urinary sodium-to-potassium ratio and intake of sodium and potassium among men and women from multiethnic general populations: the INTERSALT Study. Hypertens Res. 2019;42:1590–8.
Stamler J, Elliott P, Dennis B, Dyer AR, Kesteloot H, Liu K, et al. INTERMAP: background, aims, design, methods, and descriptive statistics (nondietary). J Hum Hypertens. 2003;17:591–608.
Dennis B, Stamler J, Buzzard M, Conway R, Elliott P, Moag-Stahlberg A, et al. INTERMAP: the dietary data–process and quality control. J Hum Hypertens. 2003;17:609–22.
Okuda N, Okayama A, Choudhry SR, Ueshima H. Development of an integrated food database as Japanese standard food table for International Cooperative Study on the Relation of Diet to Blood Pressure (INTEMRAP) (in Japanese). Jpn J Cardiovascular Dis Prev 1997;32:124–9.
Schakel SF, Dennis BH, Wold AC, Conway R, Zhao L, Okuda N, et al. Enhancing data on nutrient composition of foods eaten by participants in the INTERMAP Study in China, Japan, the United Kingdom and the United States. J Food Compos Anal. 2003;16:395–408.
Voors AW, Dalferes ER Jr, Frank GC, Aristimuno GG, Berenson GS. Relation between ingested potassium and sodium balance in young Blacks and whites. Am J Clin Nutr. 1983;37:583–94.
Clark AJ, Mossholder S. Sodium and potassium intake measurements: dietary methodology problems. Am J Clin Nutr. 1986;43:470–6.
Holbrook JT, Patterson KY, Bodner JE, Douglas LW, Veillon C, Kelsay JL, et al. Sodium and potassium intake and balance in adults consuming self-selected diets. Am J Clin Nutr. 1984;40:786–93.
Tasevska N, Runswick SA, Bingham SA. Urinary potassium is as reliable as urinary nitrogen for use as a recovery biomarker in dietary studies of free living individuals. J Nutr. 2006;136:1334–40.
Habibzadeh F, Habibzadeh P, Yadollahie M. On determining the most appropriate test cut-off value: the case of tests with continuous results. Biochem Med (Zagreb). 2016;26:297–307.
One ROC curve and cutoff analysis, Chapter 546, NCSS Statistical Software, 546-6 – 546-7.
Iwahori T, Ueshima H, Torii S, Saito Y, Fujiyoshi A, Ohkubo T, et al. Four to seven random casual urine specimens are sufficient to estimate 24-h urinary sodium/potassium ratio in individuals with high blood pressure. J Hum Hypertens. 2016;30:328–34.
Iwahori T, Miura K, Ueshima H. Time to Consider Use of the Sodium-to-Potassium Ratio for Practical Sodium Reduction and Potassium Increase. Nutrients 2017;9:700.
Acknowledgements
We thank all INTERMAP staff at the local, national, and international centers for their invaluable efforts. A partial list of these colleagues is given in Ref. [21] of this paper. We thank every participant in the study for their invaluable contributions. This study was planned and analyzed by the authors. The funders had no role in the study design, data collection and analysis, interpretation of results, decision to publish, or preparation of the manuscript. All authors participated in the critical revision of the manuscript. All authors approved the final version of the manuscript for submission.
Funding
INTERMAP was supported by grants R01-HL50490, R01-HL65461, R01-HL84228, and R01-HL135486 from the National Heart, Lung, and Blood Institute, NIH (Bethesda, MD, USA) and Ministry of Education, Culture, Sports, Science, and Technology of Japan (Grant-in-Aid for Scientific Research [A], No. 090357003 and No. 17H01553), the United Kingdom (a project grant from the West Midlands National Health Service Research and Development, and grant R2019EPH from the Chest, Heart and Stroke Association), and a grant from OMRON Healthcare Co. Ltd.
Author information
Authors and Affiliations
Consortia
Corresponding author
Ethics declarations
Conflict of interest
ES is an employee of OMRON Healthcare Co., Ltd., which manufactures a device for monitoring the Na/K ratio in urine samples. KM received a grant from OMRON Healthcare Co. Ltd. The other authors declare that they have no conflicts of interest. Supplementary information is available at Hypertension Research’s website.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Salman, E., Kadota, A., Okami, Y. et al. Investigation of the urinary sodium-to-potassium ratio target level based on the recommended dietary intake goals for the Japanese population: The INTERMAP Japan. Hypertens Res 45, 1850–1860 (2022). https://doi.org/10.1038/s41440-022-01007-x
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41440-022-01007-x
Keywords
This article is cited by
-
Regional variation in pre-dialysis blood pressure and its association with cardiovascular mortality rates in Japanese patients undergoing dialysis
Hypertension Research (2024)
-
Low urinary sodium-to-potassium ratio in the early phase following single-unit cord blood transplantation is a predictive factor for poor non-relapse mortality in adults
Scientific Reports (2024)
-
Winners for the 14th Hypertension Research Awards and outstanding papers in Hypertension Research
Hypertension Research (2024)
-
2023 update and perspectives
Hypertension Research (2024)
-
Lifetime home BP-centered approach is the core from onset to aggravation of hypertension
Hypertension Research (2023)
