
Abstract
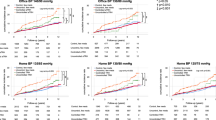
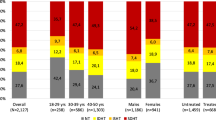
Patients with coronary heart disease (CHD) can be particularly susceptible to the adverse effects of excessive blood pressure (BP) lowering by antihypertensive treatment. The identification of hypotension is thus especially important. This study estimated the prevalence of hypotension among CHD-treated hypertensive patients undergoing ambulatory blood pressure monitoring (ABPM) in routine clinical practice. We performed a cross-sectional study with 2892 CHD-treated hypertensive patients from the Spanish ABPM Registry. Based on previous studies, hypotension was defined as systolic/diastolic BP < 120 and/or 70 mmHg according to office measurements, <115 and/or 65 mmHg according to daytime ABPM, <100 and/or 50 mmHg according to nighttime ABPM, and <110 and/or 60 mmHg according to 24 h ABPM. The participants’ mean age was 67.1 years (69.8% men). A total of 19.6% of the patients had office hypotension, 26.5% had daytime hypotension, 9.0% had nighttime hypotension, and 16.1% had 24-hr ABPM hypotension. Low diastolic BP values were responsible for most cases of hypotension. Fifty-eight percent of the cases of hypotension detected by daytime ABPM did not correspond to hypotension according to office BP. The variables independently associated with daytime ambulatory systolic/diastolic hypotension and diastolic hypotension (the latter being the most frequent type of ambulatory hypotension) were age, female sex, and the number of antihypertensive medications. In conclusion, in a large ABPM registry, one out of every four CHD-treated hypertensive patients was potentially at risk because of hypotension according to daytime ABPM, and more than half of them were not identified if office BP was relied on alone. We suggest that ABPM should be performed in these patients.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout
Similar content being viewed by others
References
Lim SS, Vos T, Flaxman AD, Danaei G, Shibuya K, Adair-Rohani H, et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor cluster in 21 regions 1990–2010: a systematic analysis for the global burden of disease study 2010. Lancet. 2012;380:2224–60.
Rapsomaniki E, Timmis A, George J, Pujades-Rodriguez M, Shah AD, Denaxas S, et al. Blood pressure and incidence of twelve cardiovascular diseases: lifetime risk, healthy life-years lost and age specific associations in 1.25 million people. Lancet. 2014;383:1899–911.
Thomopoulos C, Parati G, Zanchetti A. Effects of blood pressure lowering on outcome incidence in hypertension: 3. Effects in patients at different levels of cardiovascular risk-overview and meta-analyses of randomized trials. J Hypertens. 2014;32:2305–14.
Mancia G, Fagard R, Narkiewicz K, Redon J, Zanchetti A, Böhm M, et al. 2013 ESH/ESC guidelines for the management of arterial hypertension: the Task Force for the Management of Arterial Hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). Eur Heart J. 2013;34:2159–219.
James PA, Oparil S, Carter BL, Cushman WC, Dennison-Himmelfarb C, Handler J, et al. 2014 evidence-based guideline for the management of high blood pressure in adults: report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA. 2014;311:507–20.
Thomopoulos C, Parati G, Zanchetti A. Effects of blood pressure lowering on outcome incidence in hypertension: 7. Effects of more vs less intensive blood pressure lowering and different achieved blood pressure levels-update overview and meta-analyses of randomized trials. J Hypertens. 2016;34:613–22.
Ettehad D, Emdin CA, Kiran A, Anderson SG, Callender T, Emberson J, et al. Blood pressure lowering for prevention of cardiovascular disease and death: a systematic review and meta-analysis. Lancet. 2016;387:957–67.
Rosendorff C, Lackland DT, Allison M, Aronow WS, Black HR, Blumenthal RS, et al. Treatment of hypertension in patients with coronary artery disease. A scientific statement from the American Heart Association, American College of Cardiology and American Society of Hypertension. Hypertension. 2015;65:1372–407.
Whelton PK, Carey RM, Aronow WS, Casey DE Jr, Collins KJ, Dennison Himmelfarb C, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol. 2018;71:2199–269.
Pepine CJ, Handberg EM, Cooper-DeHoff RM, Marks RG, Kowey P, Messerli FH, et al. A calcium antagonist vs a non-calcium antagonist hypertension treatment strategy for patients with coronary artery disease. The International Verapamil-Trandolapril Study (INVEST): a randomized controlled trial. JAMA. 2003;290:2805–16.
Bangalore S, Qin J, Sloan S, Murphy SA, Cannon CP, PROVE IT-TIMI 22 trial investigators. What is the optimal blood pressure in patients after acute coronary syndromes? Relationship of blood pressure and cardiovascular events in the PRavastatin OR atorVastatin Evaluation and Infection Therapy. Thrombolysis In Miocardial Infarction (PROVE IT-TIMI) 22 trial. Circulation. 2010;122:2142–51.
Owens P, O´Brien E. Hypotension in patients with coronary disease: can profound hypotensive events cause myocardial ischaemic events? Heart. 1999;82:477–81.
Vidal-Petiot E, Ford I, Greenlaw N, Ferrari R, Fox KM, Tardif JC, et al. Cardiovascular event rates and mortality according to achieved systolic and diastolic blood pressure in patients with stable coronary artery disease: an international cohort study. Lancet. 2016;388:2142–52.
Ruilope LM, Segura J, Zamorano JL. New clinical concepts after the ONTARGET trial. Expert Rev Cardiovasc Ther. 2011;9:685–9.
Divisón-Garrote JA, Banegas JR, De la Cruz JJ, Escobar-Cervantes C, De la Sierra A, Gorostidi M, et al. Hypotension based on office and ambulatory monitoring blood pressure. Prevalence and clinical profile among a cohort of 70.997 treated hypertensives. J Am Soc Hypertens. 2016;10:714–23.
Wright JT,Jr, Williamson JD, Whelton PK, Snyder JK, Sink KM, SPRINT Research Group, et al. A randomized trial of intensive versus standard blood pressure control. N Engl J Med. 2015;373:2103–16.
Banegas JR, Segura J, Sobrino J, Rodríguez-Artalejo F, de la Sierra A, de la Cruz JJ, et al. Effectiveness of blood pressure control outside the medical setting. Hypertension. 2007;49:62–68.
De la Sierra A, Banegas JR, Segura J, Gorostidi M, Ruilope LM, CARDIORISC Event Investigators. Ambulatory blood pressure monitoring and development of cardiovascular events in high-risk patients included in the Spanish ABPM registry: the CARDIORISC Event study. J Hypertens. 2012;30:713–9.
Banegas JR, Ruilope LM, de la Sierra A, Vinyoles E, Gorostidi M, de la Cruz JJ, et al. Clinic versus daytime ambulatory blood pressure differences among hypertensive patients. The impact of age on clinic blood pressure. Hypertension. 2017;69:211–9.
Banegas JR, de la Sierra A, Segura J, Gorostidi M, de la Cruz J, Rodríguez-Artalejo F, et al. Control of hypertension in coronary heart disease. Int J Cardiol. 2009;134:245–7.
Mak G, Murphy NF, Ali A, Walsh A, O’Loughlin C, Conlon C, et al. Multiple neurohumoral modulating agents in systolic dysfunction heart failure: are we lowering blood pressure too much? J Card Fail. 2008;14:555–60.
Yusuf S, Teo KK, Pogue J, Dyal L, Copland I, ONTARGET Investigators, et al. Telmisartan, ramipril or both in patients at high risk for vascular events. N Engl J Med. 2008;358:1547–59.
Patel A, MacMahon S, Chalmers J, Neal B, Woodward M, ADVANCE Collaborative Group, et al. Effects of a fixed combination of perindopril and indapamide on macrovascular and microvascular outcomes in patients with type 2 diabetes mellitus (the ADVANCE trial): a randomised controlled trial. Lancet. 2007;370:829–40.
Jamerson K, Weber MA, Bakris GL, Dahlöf B, Pitt B, Shi V, et al. Benazepril plus amlodipine or hydrochlorothiazide for hypertension in high-risk patients. N Engl J Med. 2008;359:2417–28.
Messerli FH, Panjrath GS. The J-curve between blood pressure and coronary artery disease or essential hypertension exactly how essential? J Am Coll Cardiol. 2009;54:1827–34.
Rabkin SW, Waheed A, Poulter RS, Wood D. Myocardial perfusion pressure in patients with hypertension and coronary disease: implications for DBP targets in hypertension management. J Hypertens. 2013;31:975–82.
Owens PE, Lyons SP, O´Brien ET. Arterial hypotension: prevalence of low blood pressure in the general population using ambulatory blood pressure monitoring. J Hum Hypertens. 2000;14:243–7.
Scuteri A, Modestino A, Frattari A, Di Daniele N, Tesauro M. Occurrence of hypotension in older participants. Which 24-hour ABPM parameter better correlate with? J Gerontol. 2012;67:867–74.
Matsushita K, Harada K, Miyazaki T, Miyamoto T, Kohsaka S, Iida K, et al. Effect of heart failure secondary to ischemic cardiomyopathy on body weight and blood pressure. Am J Cardiol. 2017;120:1589–94.
Lee SE, Lee HY, Cho HJ, Choe WS, Kim H, Choi JO, et al. Reverse J-curve relationship between on-treatment blood pressure and mortality in patients with heart failure. J Am Coll Cardiol Heart Fail. 2017;5:810–9.
Yannoutsos A, Ahouah M, Dreyfuss Tubiana C, Topouchian J, Safar ME, Blacher J. Aortic stiffness improves the prediction of both diagnosis and severity of coronary artery disease. Hypertens Res. 2018;41:118–25.
Hashimoto J, Ito S. Central diastolic pressure decay mediates the relationship between aortic stiffness and myocardial viability: potential implications for aortosclerosis-induced myocardial ischemia. J Hypertens. 2017;35:2034–343.
Franklin SS, Gokhale SS, Chow VH, Larson MG, Levy D, Vasan RS, et al. Does low diastolic blood pressure contribute to the risk of recurrent hypertensive cardiovascular disease events? The Framingham heart study. Hypertension. 2015;65:299–305.
Ungar A, Pepe G, Lambertucci L, Fedeli A, Monami M, Mannucci E, et al. Low diastolic ambulatory blood pressure is associated with greater all-cause mortality in older patients with hypertension. J Am Geriatr Soc. 2009;57:291–6.
Vidal-Petiot E, Greenlaw N, Ford I, Ferrari R, Fox KM, Tardif JC, et al. Relationships between components of blood pressure and cardiovascular events in patients with stable coronary artery disease and hypertension. Hypertension. 2018;71:168–76.
Benetos A, Labat C, Rossignol P, Fay R, Rolland Y, Valbusa F, et al. Treatment with multiple blood pressure medications, achieved blood pressure, and mortality in older nursing home residents. The PARTAGE study. JAMA Intern Med. 2015;175:989–95.
Gomadam P, Shah A, Qureshi W, Yeboah PN, Freedman BI, Bowden D, et al. Blood pressure indices and cardiovascular disease mortality in persons with or without diabetes mellitus. J Hypertens. 2018;36:85–92.
Shiue I. Increased health service use for hypotension in the very old: Northumbriam hospital episode statistics, 2013–2014. Int J Cardiol. 2015;201:185–7.
Ricci F, Manzoli L, Sutton R, Melander O, Flacco ME, Gallina S, et al. Hospital admissions for orthostatic hypotension and syncope in later life: insights from the Malmo Preventive Project. J Hypertens. 2017;35:776–83.
Bress AP, Kramer H, Khatib R, Beddhu S, Cheung AK, Hess R, et al. Potential deaths averted and serious adverse events incurred from adoption of the SPRINT (Systolic Blood Pressure Intervention Trial) intensive blood pressure regimen in the United States. Circulation. 2017;135:1617–28.
Banegas JR, Ruilope LM, Sierra A, Vinyoles E, Gorostidi M, Cruz JJ, et al. Relationship between clinic and ambulatory blood-pressure measurements and mortality. N Engl J Med. 2018;378:1509–20.
Verdecchia P, Reboldi G, Angeli F, Trimarco B, Mancia G, Pogue J, et al. Systolic and diastolic blood pressure changes in relation with myocardial infarction and stroke in patients with coronary artery disease. Hypertension. 2015;65:108–14.
Williams B, Mancia G, Spiering W, Agabiti Rosei E, Azizi M, Burnier M, et al. ESC Scientific Document Group; 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur Heart J. 2018;39:3021–104.
Montalescot G, Sechtem U, Achenbach S, Andreotti F, Arden C, Task Force Members, et al. 2013 ESC guidelines on the management of stable coronary artery disease: the Task Force on the management of stable coronary artery disease of the European Society of Cardiology. Eur Heart J. 2013;34:2949–3003.
Funding
The Spanish ABPM Registry was initiated and is maintained by an unrestricted grant from Lacer Laboratories, Spain, and the Spanish Society of Hypertension. Specific funding for this analysis was obtained from Fondo de Investigación Sanitaria (FIS) (Instituto de Salud Carlos III and FEDER/FSE) grants PI16/01460, and Catedra de epidemiologia y control del riesgo cardiovascular (#820024). The funding agencies had no role in the study design; data collection, analysis, and interpretation; writing of the report; or the decision to submit it for publication.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Divisón-Garrote, J.A., de la Cruz, J.J., de la Sierra, A. et al. Prevalence of office and ambulatory hypotension in treated hypertensive patients with coronary disease. Hypertens Res 43, 696–704 (2020). https://doi.org/10.1038/s41440-020-0462-9
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41440-020-0462-9
