
Abstract
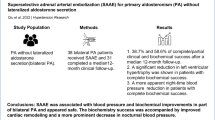
The importance of cosyntropin stimulation during adrenal vein sampling (AVS) is not fully established, partly due to insufficient AVS data relating the presence and absence of cosyntropin stimulation with postoperative outcome. Therefore, we investigated differences in AVS indices before and after cosyntropin stimulation, and determined whether unstimulated or stimulated AVS indices better correlated with treatment outcome. A retrospective study was conducted in two parts: one with 185 patients who underwent AVS and the other with 81 patients who underwent unilateral adrenalectomy for unilateral aldosterone oversecretion. The selectivity index (SI), lateralized ratio (LR), and contralateral ratio (CR) before and after cosyntropin stimulations were determined, along with blood pressure outcome 1 year after surgery. Primary aldosteronism was diagnosed according to the Japanese Endocrine Society 2009 guidelines. The percentage of AVS patients with successful catheterization, defined as unstimulated SI > 2 before and stimulated SI > 5, increased after cosyntropin stimulation from 52% to 93% and from 74% to 98% for the right and left adrenal veins, respectively. LR decreased after cosyntropin stimulation (P < 0.001). In the postoperative patients, complete and partial clinical success was achieved in 49 and 27%, respectively. Low CR (<1) and high LR (≥2.6) after cosyntropin stimulation better correlated with postoperative blood pressure outcome than those before stimulation (CR < 1 and LR ≥ 2). These data suggest that cosyntropin stimulation facilitated the judgment of catheter insertion and postcosyntropin AVS indices may be more useful for predicting treatment outcome after unilateral adrenalectomy. Further study should examine the usefulness of cosyntropin stimulation in AVS performed in other settings.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout




Similar content being viewed by others


References
Rossi GP, Auchus RJ, Brown M, Lenders JW, Naruse M, Plouin PF, et al. An expert consensus statement on use of adrenal vein sampling for the subtyping of primary aldosteronism. Hypertension 2014;63:151–60.
Rossi GP, Barisa M, Allolio B, Auchus RJ, Amar L, Cohen D, et al. The Adrenal Vein Sampling International Study (AVIS) for identifying the major subtypes of primary aldosteronism. J Clin Endocrinol Metab. 2012;97:1606–14.
Bardet S, Chamontin B, Douillard C, Pagny JY, Hernigou A, Joffre F, et al. SFE/SFHTA/AFCE consensus on primary aldosteronism, part 4: Subtype diagnosis. Ann Endocrinol (Paris). 2016;77:208–13.
Nishikawa T, Omura M, Satoh F, Shibata H, Takahashi K, Tamura N, et al. Guidelines for the diagnosis and treatment of primary aldosteronism-the Japan Endocrine Society 2009. Endocr J. 2011;58:711–21.
The Japan Society of Endocrinology. Consensus statement on the clinical practice of primary aldosteronism in Japan. Folia Endocrinol Jpn. 2016;92.
Amar L, Baguet JP, Bardet S, Chaffanjon P, Chamontin B, Douillard C, et al. SFE/SFHTA/AFCE primary aldosteronism consensus: introduction and handbook. Ann Endocrinol (Paris). 2016;77:179–86.
Tanemoto M, Suzuki T, Abe M, Abe T, Ito S. Physiologic variance of corticotropin affects diagnosis in adrenal vein sampling. Eur J Endocrinol. 2009;160:459–63.
Nakamura Y, Satoh F, Morimoto R, Kudo M, Takase K, Gomez-Sanchez CE, et al. 18-oxocortisol measurement in adrenal vein sampling as a biomarker for subclassifying primary aldosteronism. J Clin Endocrinol Metab. 2011;96:E1272–8.
Laurent I, Astère M, Zheng F, Chen X, Yang J, Cheng Q, et al. Adrenal venous sampling with or without adrenocorticotropic hormone stimulation: a meta-analysis. J Clin Endocrinol Metab. 2018;104:1060–8.
Seccia TM, Miotto D, De Toni R, Pitter G, Mantero F, Pessina AC, et al. Adrenocorticotropic hormone stimulation during adrenal vein sampling for identifying surgically curable subtypes of primary aldosteronism: comparison of 3 different protocols. Hypertension 2009;53:761–6.
Funder JW, Carey RM, Mantero F, Murad MH, Reincke M, Shibata H, et al. The management of primary aldosteronism: case detection, diagnosis, and treatment: an Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab. 2016;101:1889–916.
Carr CE, Cope C, Cohen DL, Fraker DL, Trerotola SO. Comparison of sequential versus simultaneous methods of adrenal venous sampling. J Vasc Inter Radiol. 2004;15:1245–50.
Rossi GP, Pitter G, Bernante P, Motta R, Feltrin G, Miotto D. Adrenal vein sampling for primary aldosteronism: the assessment of selectivity and lateralization of aldosterone excess baseline and after adrenocorticotropic hormone (ACTH) stimulation. J Hypertens. 2008;26:989–97.
Monticone S, Satoh F, Giacchetti G, Viola A, Morimoto R, Kudo M, et al. Effect of adrenocorticotropic hormone stimulation during adrenal vein sampling in primary aldosteronism. Hypertension 2012;59:840–6.
Satoh F, Abe T, Tanemoto M, Nakamura M, Abe M, Uruno A, et al. Localization of aldosterone-producing adrenocortical adenomas: significance of adrenal venous sampling. Hypertens Res. 2007;30:1083–95.
Morita S, Yamazaki H, Sonoyama Y, Nishina Y, Ichihara A, Sakai S. Successful adrenal venous sampling by non-experts with reference to CT images. Cardiovasc Interv Radiol. 2016;39:1001–6.
Morita S, Nishina Y, Yamazaki H, Sonoyama Y, Ichihara A, Sakai S. Dual adrenal venous phase contrast-enhanced MDCT for visualization of right adrenal veins in patients with primary aldosteronism. Eur Radiol. 2016;26:2073–7.
Omura M, Sasano H, Saito J, Yamaguchi K, Kakuta Y, Nishikawa T. Clinical characteristics of aldosterone-producing microadenoma, macroadenoma, and idiopathic hyperaldosteronism in 93 patients with primary aldosteronism. Hypertens Res. 2006;29:883–9.
Umakoshi H, Tanase-Nakao K, Wada N, Ichijo T, Sone M, Inagaki N, et al. Importance of contralateral aldosterone suppression during adrenal vein sampling in the subtype evaluation of primary aldosteronism. Clin Endocrinol (Oxf). 2015;83:462–7.
Wolley MJ, Gordon RD, Ahmed AH, Stowasser M. Does contralateral suppression at adrenal venous sampling predict outcome following unilateral adrenalectomy for primary aldosteronism? A retrospective study. J Clin Endocrinol Metab. 2015;100:1477–84.
Ogihara T, Kikuchi K, Matsuoka H, Fujita T, Higaki J, Horiuchi M, et al. The Japanese Society of Hypertension Guidelines for the Management of Hypertension (JSH 2009). Hypertens Res. 2009;32:3–107.
Shimamoto K, Ando K, Fujita T, Hasebe N, Higaki J, Horiuchi M, et al. The Japanese Society of Hypertension Guidelines for the Management of Hypertension (JSH 2014). Hypertens Res 2014;37:253–390.
Williams TA, Lenders JWM, Mulatero P, Burrello J, Rottenkolber M, Adolf C, et al. Outcomes after adrenalectomy for unilateral primary aldosteronism: an international consensus on outcome measures and analysis of remission rates in an international cohort. Lancet Diabetes Endocrinol. 2017;5:689–99.
Lefebvre H, Thomas M, Duparc C, Bertherat J, Louiset E. Role of ACTH in the interactive/paracrine regulation of adrenal steroid secretion in physiological and pathophysiological conditions. Front Endocrinol (Lausanne). 2016;7:98.
Steichen O, Amar L. Diagnostic criteria for adrenal venous sampling. Curr Opin Endocrinol Diabetes Obes. 2016;23:218–24.
Kita T, Furukoji E, Sakae T, Kitamura K. Efficient screening of patients with aldosterone-producing adenoma using the ACTH stimulation test. Hypertens Res. 2019;42:801–6.
Steichen O, Zinzindohoué F, Plouin PF, Amar L. Outcomes of adrenalectomy in patients with unilateral primary aldosteronism: a review. Horm Metab Res. 2012;44:221–7.
Bokuda K, Yatabe M, Mizuguchi Y, Niiyama M, Seki Y, Watanabe D, et al. Body mass index and contralateral ratio predict outcome following unilateral adrenalectomy in primary aldosteronism. Hypertens Res. 2017;40:988–93.
Umakoshi H, Tsuiki M, Yokomoto-Umakoshi M, Takeda Y, Takashi Y, Kurihara I, et al. Correlation between lateralization index of adrenal venous sampling and standardized outcome in primary aldosteronism. J Endocr Soc. 2018;2:893–902.
Shibayama Y, Wada N, Naruse M, Kurihara I, Ito H, Yoneda T, et al. The occurrence of apparent bilateral aldosterone suppression in adrenal vein sampling for primary aldosteronism. J Endocr Soc. 2018;2:398–407.
Funding
The study was funded in part by Novartis Research Grant and Tanabe Mitsubishi Research Grant to MY and supported in part by a JSPS KAKENHI Grant Number 16H05316 to AI.
Author information
Authors and Affiliations
Contributions
The research was designed by MY, KB, and AI, and was conducted by MY, KB, SM, JY, YS, DW, TA, SM, SS, and AI. MY and KY analyzed the data and performed the statistical analysis. MY drafted the article. Critical revision of the article was performed by SM, JY, SM, and AI. MY was granted the JSH Women Investigator’s Award by the Japanese Society of Hypertension for this work.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
About this article

Cite this article
Yatabe, M., Bokuda, K., Yamashita, K. et al. Cosyntropin stimulation in adrenal vein sampling improves the judgment of successful adrenal vein catheterization and outcome prediction for primary aldosteronism. Hypertens Res 43, 1105–1112 (2020). https://doi.org/10.1038/s41440-020-0445-x
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41440-020-0445-x
