
Abstract
Hypertension is a global health issue, and a reduced exercise capacity is unavoidable for older people. According to recent clinical studies, the intestinal microbiota play a crucial role in the pathogenesis of many human diseases. We investigated whether specific alterations in the gut microbiota contribute to the reduced exercise capacity of elderly patients with hypertension. This study enrolled 56 subjects, and all patients performed a cardiopulmonary exercise test and underwent fecal bacteria sequencing (16 s ribosomal RNA V4 region). According to peak oxygen uptake values, patients were divided into three groups (Weber A = 19, Weber B = 20, and Weber C = 17). The alpha diversity was not significantly different among the three groups. Regarding the beta diversity, Weber A samples were separate from the other two groups in the nonmetric multidimensional scaling ordination plot (ANOSIM pairwise comparisons generated an R > 0.5; p < 0.05). The abundance of Betaproteobacteria, Burkholderiales, Alcaligenaceae, Faecalibacterium and Ruminococcaceae was diminished in subjects with a reduced exercise capacity (LDA score > 4.0). Escherichia coli are a primary producer of trimethylamine and inflammation in the human gut, and the abundance of this bacteria was increased in patients with a reduced exercise capacity (LDA score > 4.0). On the other hand, Lachnospiraceae-Eubacterium_hallii_group, Lachnospiraceae-Lachnoclostridium, Lachnospiraceae-Blautia-Ruminococcus_sp__5_1_39BFAA, and Ruminococcaceae-Faecalibacterium belong to the order Clostridiales that are likely to produce short-chain fatty acids (LDA score > 4.0), and some of these species were enriched in the Weber B or Weber C group in multiple comparisons. Our data pointed to an altered gut microbiota as a potential contributor to the pathogenesis and progression of the reduced exercise capacity of elderly patients with hypertension.
Similar content being viewed by others


Introduction
In recent decades, hypertension has become a major global health burden and one of the most common chronic diseases in the elderly. [1] For elderly people, a reduced exercise capacity is an unavoidable condition. Minimal stressors cause functional impairments in individuals suffering from physical frailty, which is a geriatric syndrome that enhances an individual’s vulnerability. [2] To date, evidence on the validity of interventions to prevent frailty in older people is scarce. [3] Therefore, studies aiming to obtain deeper insights into the pathogenic factors contributing to this condition are urgently needed.
The human gastrointestinal tract is inhabited by a large microbiota, which plays important roles in human health and disease. [4] Recently, accumulating evidence has suggested a link between gut dysbiosis and various disorders, such as hypertension, cardiovascular diseases (CVDs), atherosclerosis, type 2 diabetes and obesity. [5, 6] Many potential mechanisms by which the gut microbiota contributes to diseases have been revealed. For example, metabolic diseases correlate with a chronic state of systemic low-grade inflammation that is related to the clinical disease severity, and the intestinal microbiota is a major source of this pathomechanism. [7, 8] In patients with chronic heart failure characterized by a reduced exercise capacity, the gut overgrowth of pathogenic bacteria such as Shigella, Yersinia, Salmonella, and Candida species has been observed. [9] Moreover, trimethylamine (TMA), a microbial metabolite of dietary choline and L-carnitine, is absorbed via the intestinal epithelium and further oxidized to trimethylamine N-oxide (TMAO), which promoted atherosclerosis and aggravate cardiovascular disease in several studies. [10, 11] In contrast, short-chain fatty acids (SCFAs) produced by a number of gut microbiota play a protective role in many chronic diseases. [12, 13] Therefore, changes in the composition and structure of the gut microbiome are pathogenic factors for many diseases. The present study was conducted in elderly patients with hypertension to determine whether changes in the intestinal microbiota are associated with a reduced exercise capacity.
Methods
Study population
This study enrolled 56 patients with hypertension from Hangzhou, a large modern city in southern China, who volunteered to participate. Subjects who met the following criteria were included: patients diagnosed with primary hypertension; aged from 65 to 80 years; and lived independently. Exclusion criteria were: any contradictions for cardiopulmonary exercise testing (CPET), uncontrolled hypertension despite the administration of medical therapy, smoking, infection, cancer, stroke, peripheral artery disease, renal failure, water retention, endocrine disorders (e.g., thyroid disease), and inflammatory or malabsorptive intestinal diseases. In addition, the patients had not undergone any laxative, antidiarrheal, steroid, probiotic, and antibiotic treatments within the past 3 months. The participants’ demographic, clinical, and functional characteristics are shown in Table 1. In addition, no statistically significant differences in medication use were observed among groups (Supplementary Table 1).
This study was approved by the Medical Ethics Committee of Zhejiang Hospital, and the procedures were performed in accordance with the Declaration of Helsinki. All subjects provided written informed consent. The trial was registered in the Chinese Clinical Trial Registry (ChiCTR-IOR-17011799).
Assessment of clinical parameters
The anthropometric variables were measured, and body mass index (BMI) was calculated according to the following formula: weight/height². Blood variables were determined in fasting venous blood samples. CPET (Cosmed, Rome) was performed according to the standard Bruce protocol to evaluate peak oxygen uptake (peak VO2), a measure of exercise capacity.
Sampling and DNA extraction
Fresh stool samples were collected in standard stool collection tubes one day after enrollment and stored at −80 °C. DNA was extracted from the fecal samples according to the QIAamp Fast DNA Stool Mini Kit (Qiagen, Hilden) operation manual. All DNA samples were frozen at −80 °C until further processing.
16 s rRNA PCR and sequencing
Extracted DNA samples were used as template for amplification the bacterial 16 s rRNA gene V4 region using specific primers (515 F 5′-GTGCCAGCMGCCGCGGTAA-3′ and 806 R 5′-GGACTACHVGGGTWTCTAAT-3′) with the barcode. [14] PCR was performed in 30 µl reactions with 15 µl of Phusion® High-Fidelity PCR Master Mix; 10 ng of template DNA, 3 µl (6 µM) of forward and reverse primers, and 2 µl of double-distilled H2O. Thermal cycling consisted of initial denaturation at 98 °C for 1 min, followed by 30 cycles of 98 °C for 10 s, 50 °C for 30 s, 72 °C for 30 s and a final extension at 72 °C for 5 min. After quantification and qualification, amplicons were mixed in equidensity ratios. Then, the samples were purified using the Qiagen Gel Extraction Kit (Qiagen, Hilden). Sequencing libraries were produced using a TruSeq® DNA PCR-Free Sample Preparation Kit (Illumina, San Diego) according to the manufacturer’s instructions. Then, the library quality was assessed on the Qubit@ 2.0 Fluorometer (Thermo Scientific) and Agilent Bioanalyzer 2100. Finally, the library was sequenced on the IlluminaHiSeq2500 platform and 250 bp paired-end reads were generated.
Sequencing analysis
Paired-end reads from the original DNA fragments were merged using FLASH software. Sequences were analyzed using the QIIME software package (Quantitative Insights Into Microbial Ecology), and in-house Perl scripts were used to analyze alpha (within samples) and beta (among samples) diversity. Sequences with ≥97% similarity were assigned to the same operational taxonomic units (OTUs). We chose representative sequences for each OTU and used the RDP classifier to annotate taxonomic information for each representative sequence. Relative abundance was calculated at the phylum and genus levels. We rarified the OTU table and computed three metrics to calculate the alpha diversity: Observed Species, Chao1, and Shannon index. QIIME calculates both weighted and unweighted unifrac values, which are phylogenetic measures of beta diversity. Distance ordination was plotted using the nonmetric multidimensional scaling (NMDS) method. Tests were conducted with linear discriminate analysis (LDA) effect size (LefSe) and ANOSIM.
Statistics
The Chi-square test was used to analyze enumeration data. Continuous data were compared using ANOVAs, and the LSD-t test was used for multiple comparisons. If numerical data violated the normal distribution and homogeneity of variance, the nonparametric Kruskal-Wallis H test was used to compare data among groups and a Dunn-Bonferroni test was used for post hoc comparisons. Spearman’s rank correlation coefficient was calculated to estimate the linear correlations between variables. All statistical analyses were completed using the SPSS 19.0 software. Statistical analyses of sequencing data were performed using the R package (version 2.15.3) and tools such as Chao 1, Simpson, Shannon, non-metric multidimensional scaling (NMDS), ANOSIM, and LefSe. P < 0.05 was considered statistically significant.
Results
Demographic, clinical, and functional profiles of study participants
Based on the peak VO2 values obtained during CPET, patients were divided into three functional classes according to Weber’s classification system: 19 patients were in class A (normal exercise capacity), 20 in class B and 17 in class C (reduced exercise capacity). Significantly higher levels of the plasma inflammatory biomarker CRP were observed in the Weber A group compared to the Weber C group (p = 0.004). Although the increase in CRP levels in Weber B and Weber C groups was not clinically significant, we detected a trend towards systemic low-grade inflammation in the patients with hypertension who presented a reduced exercise capacity. Peak VO2/kg and VO2/kg at the anaerobic threshold (AT) were both significantly different between groups according to the multiple comparisons test (p < 0.01). The VTmax in the Weber C group was significantly lower than the Weber A (p < 0.001) and Weber B groups (p = 0.001), respectively. Notably, the ratio of DM type II was statistically significantly different in the global comparison, but no difference was observed in the multiple comparisons test (Table 1).
Intestinal microbiome
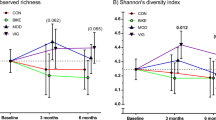
The composition of the gut microbiota of all patients was mainly dominated by the 4 phyla: Firmicutes, Bacteroidetes, Proteobacteria, and Actinobacteria (Fig. 1a, b). The ratio of members of the phylum Firmicutes to Bacteroidetes (F/B ratio) is considered a potential biomarker of pathological conditions. [15] Although patients in the Weber A group had a lower F/B ratio than the other two groups, the difference was not statistically significant (Supplementary Table 2). Next, an overview of the abundances of the top 35 genera in the three groups is presented (Fig. 1c). However, we did not detect significant differences among three groups in the relative abundances of the major phyla or in alpha diversity measures (Chao 1, Simpson, Shannon; Kruskal–Wallis H test, p > 0.05). Regarding beta diversity, which represents interindividual variances, the NMDS plots based on OTU distribution showed partial overlapping distributions among each group (Fig. 2), and Weber A samples were still separate from the other groups (ANOSIM pairwise comparisons generated an R > 0.5, p < 0.05).

a Relative abundances of the top 10 phyla by composition in individual samples. b Relative abundances of the top 10 phyla by composition in the three groups. c The abundances of the top 35 bacteria at the genus level in each group are shown. The heat map is color-coded based on row Z-scores. The groups with the highest and lowest bacterial abundances are shown in red and blue, respectively

Nonmetric multidimensional scaling (NMDS) ordination plot of the Weber A, Weber B, and Weber C samples. Ordination was based on Bray-Curtis dissimilarity calculated with OTU-level data. Each point represents one sample; the closer the points are located to one another, the more similar the microbiome compositions of the samples
The results of the LefSe analysis (LDA score > 4.0, p < 0.05) performed on the relative abundance data for the microbiota are presented in Fig. 3. In terms of the overall situation (Fig. 3A), the abundance of the class Betaproteobacteria was prominently increased in the Weber A group, including the order Burkholderiales and the family Alcaligenaceae; the family Ruminococcaceae and the genus Faecalibacterium were also enriched in the Weber A group compared to the other two groups. The genus Escherichia_Shigella and the species Escherichia coli were significantly increased in the Weber C group, and the genus Blautia and Eubacterium hallii were enriched in the Weber B group. In pairwise comparisons, the gut microbes mentioned above that were enriched in Weber A were decreased in the Weber B, Weber C and Weber B + C (Weber B. C) groups (Fig. 3b–d). The abundances of the genera Blautia, Ruminococcus_2, Escherichia_Shigella and the species Escherichia coli (E. coli) were significantly increased in the Weber B group compared to the Weber A group (Fig. 3b). The relative abundances of the class Bacilli, the order Lactobacillales, the family Lachnospiraceae, the genera Blautia and Escherichia_Shigella, the species E. coli and Ruminococcus_sp__5_1_39BFAA were enriched in the Weber C group compared to the Weber A group (Fig. 3c), The abundances of the genera Blautia, Escherichia_Shigella, Ruminococcus_2, the species E. coli and Ruminococcus_sp__5_1_39BFAA were significantly increased in the Weber B. C group (Fig. 3d). Consistent with the alpha and beta diversity values, little difference was observed between the Weber B and Weber C groups (Fig. 3e).

A LefSe analysis along with linear discriminate analysis (LDA) was applied to identify indicator bacterial in the groups. a Weber A vs. Weber B vs. Weber C, (b) Weber A vs. Weber B, (c) Weber A vs. Weber C, (d) Weber A vs. Weber B + C and (e) Weber B vs. Weber C
A reduced exercise capacity negatively associates with the core gut microbiota
We next determined the correlations between the core gut microbiota and clinical parameters of patients (Table 2). The bacterial counts of Lactobacillales, Eubacterium_hallii_group and Blautia were positively correlated with CRP levels (r = 0.385, p = 0.003; r = 0.296, p = 0.027 and r = 0.268, p = 0.046; respectively), while Alcaligenaceae was negatively correlated with CRP levels (r = −0.294, p = 0.028). Bacterial counts of the Lactobacillales, Blautia, Ruminococcus_sp._5_1_39BFAA and E. coli were negatively correlated with the peak VO2/kg (r = −0.284, p = 0.034; r = −0.290, p = 0.030; r = −0.273, p = 0.042 and r = −0.355, p = 0.007; respectively), while Alcaligenaceae was positively correlated with peak VO2/kg levels (r = 0.318, p = 0.017). Meanwhile, the E. coli count negatively correlated with VO2/kg at AT (r = −0.364, p = 0.006).
Discussion
Based on accumulating evidence obtained from recent studies, gut dysbiosis and induces a chronic state of systemic low-grade inflammation that plays a crucial role in the pathophysiology of CVDs, including hypertension. [7, 16] Hypertension is a chronic disease that is considered a main risk factor for the development and progression of CVDs and displays a low control rate and high prevalence in several populations, particularly elderly people in developing countries. [17] On the other hand, physical exercise is possibly the most promising nonpharmacological approach to prevent and treat hypertension, and the optimal levels of exercise capacity are associated with lower all-cause and cardiovascular mortality and morbidity. [18, 19] Interestingly, robust associations between the effects of age and frailty on both the composition and function of the gut microbiome were identified. [20] Therefore, we investigated the relationship between the gut microbiota and exercise capacity in the elderly patients with hypertension.
To our knowledge, this study is the first systematic analysis of the correlation between the intestinal microbiota and reduced exercise capacity in elderly patients with hypertension using high-throughput sequencing of bacterial 16 s rRNA gene sequences. Because all samples were obtained from elderly patients with hypertension, a difference in the alpha diversity was not identified in this analysis. A reduced exercise capacity is one of the most common clinical symptoms of stable heart failure and many other chronic diseases. Recently, alterations in the composition and metabolism of the intestinal microbiota have been identified as pathogenic factors contributing to the development of atherosclerosis and CVD. [16, 21] Notably, TMAO, the hepatic oxidation product of the gut microbial metabolite TMA, has attracted increasing attention as a potential promoter of atherosclerosis. [22] Two independent cohort studies suggested that plasma concentrations of TMAO predict an enhanced risk of major adverse cardiac incidents. [23] Moreover, E. coli is a primary producer of TMA and inflammation in humans. [22] Interestingly, the abundances of Escherichia_Shigella and E. coli were higher in patients with a reduced exercise capacity than in patients with a normal exercise capacity and were negatively correlated with exercise capacity. Additionally, CRP levels were increased in the Weber C group compared to the Weber A group, although a clinical implication was not determined. This finding is consistent with a previous report showing a correlation between increased CRP levels and the intestinal abundance of pathological Shigella species in patients with moderate-to-severe heart failure. [9] Therefore, we concluded that E. coli may play an important role in decreasing the exercise capacity of elderly patients with hypertension.
SCFAs are produced by specific gut microbes through the fermentation of soluble fiber and are predicted to have anti-inflammatory properties. [24, 25] The predominant intestinal bacteria that produce SCFAs are classified as Eubacterium (cluster XIVa) and Ruminococcaceae (cluster IV) in the order Clostridiales, and class Clostridia. [25] Additionally, Lachnospiraceae possess rich carbohydrate-active enzyme (CAZyme) repertoires that utilize complex polysaccharides to form the major energy source for several Clostridium XIVa strains and colon-resident bacteria. [22, 26] In our study, Lachnospiraceae-Eubacterium_hallii_group, Lachnospiraceae-Lachnoclostridium, Lachnospiraceae-Blautia-Ruminococcus_sp__5_1_39BFAA, and Ruminococcaceae-Faecalibacterium belong to the order Clostridiales; some of these species were enriched in the Weber B or Weber C group in multiple comparisons tests. However, the bacterial counts of Lactobacillales and Blautia were positively correlated with CRP levels and were negatively associated with peak VO2/kg. Hence, we deduced that the gut may employ a compensatory mechanism to alleviate the actions of pathogenic bacteria. Moreover, the abundances of Betaproteobacteria, Burkholderiales, and Alcaligenaceae were diminished in subjects with a reduced exercise capacity and were positively correlated with peak VO2/kg and were negatively correlated with CRP levels. This study is the first to focus on correlations between the alterations in the gut microbiota with reduced exercise capacity in elderly individuals with hypertension, and it provided a new concept of this condition for further exploration. However, the present study has several limitations. First, we did not examine the serum concentrations of TMAO and SCFAs; therefore, we were unable to directly determine the relationship between the intestinal microbiota and TMAO or SCFAs. Second, our results were based on relatively small sample sizes, and further large-scale studies are needed to prove our findings. Finally, comprehensive metagenomic and metabolomic analyses are needed in the future to perform a more in-depth assessment of the gut microbiota composition and metabolism in elderly subjects.
In conclusion, a striking negative correlation between a reduced exercise capacity and specific taxonomic abundances. Intestinal dysbiosis plays a potential pathogenic role in reducing the exercise capacity of elderly patients with hypertension. Further research is needed in this area to provide additional supporting evidence for the development of a novel specific therapy or strategy to alleviate this condition.
References
Su P, Ding H, Zhang W, Duan G, Yang Y, Long J, et al. Joint association of obesity and hypertension with disability in the elderly—A community-based study of residents in Shanghai, China. J Nutr. 2017;21:362–9.
Morley JE, Vellas B, Abellan van Kan G, Anker SD, Bauer JM, Bernabei R, et al. Frailty consensus: a call to action. J Am Med Dir Assoc. 2013;14:392–7.
Serra-Prat M, Sist X, Domenich R, Jurado L, Saiz A, Roces A, et al. Effectiveness of an intervention to prevent frailty in pre-frail community-dwelling older people consulting in primary care: a randomised controlled trial. Age Ageing. 2017;46:401–7.
Lynch SV, Pedersen O. The human intestinal microbiome in health and disease. N Engl J Med. 2016;375:2369–79.
Li J, Zhao F, Wang Y, Chen J, Tao J, Tian G, et al. Gut microbiota dysbiosis contributes to the development of hypertension. Microbiome. 2017;5:14.
Liu R, Hong J, Xu X, Feng Q, Zhang D, Gu Y, et al. Gut microbiome and serum metabolome alterations in obesity and after weight-loss intervention. Nat Med. 2017;23:859–68.
Wen L, Duffy A. Factors influencing the gut microbiota, inflammation, and type 2 diabetes. J Nutr. 2017;147:1468S–1475S.
Sandek A, Anker SD, von Haehling S. The gut and intestinal bacteria in chronic heart failure. Curr Drug Metab. 2009;10:22–28.
Pasini E, Aquilani R, Testa C, Baiardi P, Angioletti S, Boschi F, et al. Pathogenic gut flora in patients with chronic heart failure. JACC Hear Fail. 2016;4:220–7.
Koeth RA, Wang Z, Levison BS, Buffa JA, Org E, Sheehy BT, et al. Intestinal microbiota metabolism of l-carnitine, a nutrient in red meat, promotes atherosclerosis. Nat Med. 2013;19:576–85.
Trøseid M, Ueland T, Hov JR, Svardal A, Gregersen I, Dahl CP, et al. Microbiota-dependent metabolite trimethylamine-N-oxide is associated with disease severity and survival of patients with chronic heart failure. J Intern Med. 2015;277:717–26.
Wang L, Zhu Q, Lu A, Liu X, Zhang L, Xu C, et al. Sodium butyrate suppresses angiotensin II-induced hypertension by inhibition of renal (pro)renin receptor and intrarenal renin-angiotensin system. J Hypertens. 2017;35:1899–908.
Wong JM, de Souza R, Kendall CW, Emam A, Jenkins DJ. Colonic health: fermentation and short chain fatty acids. J Clin Gastroenterol. 2006;40:235–43.
Evans CC, LePard KJ, Kwak JW, Stancukas MC, Laskowski S, Dougherty J, et al. Exercise prevents weight gain and alters the gut microbiota in a mouse model of high fat diet-induced obesity. PLoS One. 2014;9:e92193.
Yang T, Santisteban MM, Rodriguez V, Li E, Ahmari N, Carvajal JM, et al. Gut dysbiosis is linked to hypertension. Hypertension. 2015;65:1331–40.
Vinjé S, Stroes E, Nieuwdorp M, Hazen SL. The gut microbiome as novel cardio-metabolic target: the time has come! Eur Heart J. 2014;35:883–7.
De Sousa EC, Abrahin O, Ferreira ALL, Rodrigues RP, Alves EAC, Vieira RP. Resistance training alone reduces systolic and diastolic blood pressure in prehypertensive and hypertensive individuals: meta-analysis. Hypertens Res. 2017;40:927–31.
Cornelissen VA, Smart NA. Exercise training for blood pressure: a systematic review and meta−analysis. J Am Heart Assoc. 2013;2:e004473
Dekleva M, Lazic JS, Arandjelovic A, Mazic S. Beneficial and harmful effects of exercise in hypertensive patients: the role of oxidative stress. Hypertens Res. 2017;40:15–20.
Jackson M, Jeffery IB, Beaumont M, Bell JT, Clark AG, Ley RE, et al. Signatures of early frailty in the gut microbiota. Genome Med. 2016;8:1–11.
Serino M, Blasco-Baque V, Nicolas S, Burcelin R. Far from the eyes, close to the heart: dysbiosis of gut microbiota and cardiovascular consequences. Curr Cardiol Rep. 2014;16:1–7.
Rath S, Heidrich B, Pieper DH, Vital M. Uncovering the trimethylamine-producing bacteria of the human gut microbiota. Microbiome. 2017;5:54.
Li XS, Obeid S, Klingenberg R, Gencer B, Mach F, Räber L, et al. Gut microbiota-dependent trimethylamine N-oxide in acute coronary syndromes: a prognostic marker for incident cardiovascular events beyond traditional risk factors. Eur Heart J. 2017;38:814–24.
Mizuno M, Noto D, Kaga N, Chiba A, Miyake S. The dual role of short fatty acid chains in the pathogenesis of autoimmune disease models. PLoS One. 2017;12:1–15.
Ohira H, Tsutsui W, Fujioka Y. Are short chain fatty acids in gut microbiota defensive players for inflammation and atherosclerosis? J Atheroscler Thromb. 2017;24:660–72.
Cantarel BL, Lombard V, Henrissat B. Complex carbohydrate utilization by the healthy human microbiome. PLoS One. 2012;7:1–10.
Acknowledgements
This work was supported by grants from the National Natural Science Foundation of China (31670701), the Health Bureau of Zhejiang Province (2018KY852 and 2018KY194), and the Chinese Traditional Medicine Science and Technology Projects of Zhejiang Province (2018ZB004).
Author information
Authors and Affiliations
Corresponding authors
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Electronic supplementary material
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Yu, Y., Mao, G., Wang, J. et al. Gut dysbiosis is associated with the reduced exercise capacity of elderly patients with hypertension. Hypertens Res 41, 1036–1044 (2018). https://doi.org/10.1038/s41440-018-0110-9
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41440-018-0110-9
Keywords:
This article is cited by
-
Alterations of gut microbiota are associated with blood pressure: a cross-sectional clinical trial in Northwestern China
Journal of Translational Medicine (2023)
-
Effects of exercise and physical activity on gut microbiota composition and function in older adults: a systematic review
BMC Geriatrics (2023)
-
The role of the gut microbiota in health and cardiovascular diseases
Molecular Biomedicine (2022)
-
Nine weeks of high-intensity indoor cycling training induced changes in the microbiota composition in non-athlete healthy male college students
Journal of the International Society of Sports Nutrition (2021)
-
Blood pressure management in an ecosystem context
Hypertension Research (2020)
