
Abstract
Background
Obesity is an important and growing health problem whose treatment involves dietary changes. In this context, studying the role of macronutrients in weight loss is required in order to understand which strategies may be applied for weight loss. We aimed to evaluate the effects of diets rich in polyunsaturated (PUFAs) and monounsaturated fatty acids (MUFAs) on resting energy expenditure (REE), substrate oxidation, and weight loss in women with obesity.
Methods
Randomized, controlled, single blind, parallel-group clinical trial was conducted for 60 days. Participants (n = 32) were divided into three groups: G1= normocaloric PUFAs-rich diet (12% of total energy expenditure (TEE), 10% of n-6 and up to 2% of n-3); G2= normocaloric MUFAs-rich diet (15–20% TEE); and G3= maintenance of the usual diet. Anthropometric and metabolic variables (REE and substrate oxidation by indirect calorimetry) were evaluated.
Results
G2 decreased body weight (−1.92 ± 1.99 kg, P = 0.02), body mass index (BMI) (−0.69 ± 0.70 kg/m2; P = 0.02), waist circumference (WC) (−1.91 ± 1.82 cm; P = 0.02), and body fat (−1.14 ± 1.53 kg; P = 0.04).
Conclusion
MUFAs-rich diet reduces body weight, BMI, body fat, and WC. Clinical Trials: NCT02656940.
Clinical trial registration
Clinical Trials: NCT02656940.
Similar content being viewed by others
Introduction
In the last decades, studies have searched for nutritional strategies to optimize body weight loss [1]. Some authors believe that decreasing energy is more relevant than managing the distribution of macronutrients [2, 3]. However, studies have emphasized the impact of changing the amount of protein, carbohydrate or fat in the treatment of obesity [4, 5].
Manipulation of dietary fats has been suggested as an option to control the obesity epidemic. Studies showed fatty acids may affect the balance between intake and energy expenditure (EE) through different factors related to adipogenesis, such as resting energy expenditure (REE), substrate oxidation [6], diet-induced thermogenesis (DIT) [7], and satiety [8], reducing body mass and/or fat storage in adipose tissue [6]. However, these effects have not been fully elucidated in humans and the results are still controversial.
The benefits of high-unsaturated fats diets, such as Mediterranean diet, have been explored in the last years. However, there are few studies evaluating the isolated effect of high-monounsaturated fatty acids (MUFAs) or high-polyunsaturated fatty acids (PUFAs) diets on health and weight loss [9, 10].
A systematic review showed weight loss after high-MUFAs diet, in which some studies evaluated the acute effects of high-MUFAs meals and others studies verified the effects of high-MUFAs diets in varying intervention periods [11]. On the other hand, some studies investigated the effects of PUFAs, especially n-3 PUFAs, in the treatment of obesity [12, 13]. However, most studies used n-3 PUFAs supplementation, and few studies had control diet for n-3 and n-6 PUFAs. In this context, our study aimed to evaluate the effects of high n-3 and n-6 PUFAs or high-MUFAs diets on REE, substrate oxidation, and body weight loss in obese women without comorbidities.
Subjects and methods
Study subjects
The study was performed at the Laboratory of Nutritional Assessment (LANUTRI) of the Institute of Nutrition Josué de Castro of the Federal University of Rio de Janeiro. Volunteers were recruited from March 2013 to June 2014. Inclusion criteria were as follows: (1) adult women (aged between 20–40 years); (2) any ethnic; (3) obesity classes I and II (body mass index (BMI) between 30 and 39.9 kg/m2); (4) pre-menopause; (5) without weight loss greater than 3 kg in 3 months; (6) and elementary school complete.
The exclusion criteria were: (1) women previously diagnosed with diabetes mellitus, cardiovascular, kidney, liver or autoimmune diseases, thyroid disorder, inflammatory bowel diseases, acquired immunodeficiency syndrome, or cancer; cholecystectomy and other surgeries (last 12 months); (2) pregnant or breastfeeding; (3) smoking; (4) using lipid-lowering, hypoglycemic, diuretics, antidepressants, or antihypertensive drugs, supplements, herbal products, and/or diets for weight loss in the last 4 weeks; (5) and those with food allergy or intolerance to vegetable oils (olive, soy, or canola oil), fish oil, fish, and/or seafood.
The research was approved by the Research Ethics Committee of the University Hospital Clementino Fraga Filho (Rio de Janeiro, RJ, Brazil) (protocol n.072/10) according to the declaration of Helsinki. All participants provided written informed consent. In addition, the present study was registered at ClinicalTrial.gov (NCT02656940).
Experimental design and characteristics of dietary intervention
A parallel, single blind, randomized, controlled clinical trial was conducted for 60 days with a convenience sample. Randomization was determined in advance, through a list of allocation groups, before the volunteer recruitment steep. Based on the previously established list, the women were continuously assigned to one of three groups: G1 (N = 10) - normocaloric n-3 and n-6 PUFAs-rich diet; G2 (N = 11) - normocaloric MUFAs-rich diet; or G3 (N = 11) - placebo and their usual diet.
The energy value of prescribed diets (G1 and G2) was calculated based on the REE obtained by indirect calorimetry (Vmax 29®, Viasys Healthcare, USA), using Weir equation [14] and corresponding physical activity factor [15]. The diets were previously calculated using the diet analysis program Diet Pro®5i (Federal University of Viçosa) based to the Brazilian Table of Food Composition [16].
The G1 and G2 diets were adequate in carbohydrates (50–55% of total energy expenditure (TEE)), proteins (15–20% of TEE), and fats (30–35% of TEE) [17]. The G1 diet contained 12% of TEE of PUFAs (10% of n-6 PUFAs and up to 2% of n-3 PUFAs), and G2 17% of TEE of MUFAs [18]. Both groups were oriented to consume up to 10% saturated fatty acids (SFA) [18]. The average chemical composition of the prescribed diets is described in Table 1.
Sachets containing soy oil and extra virgin olive for G1, sachet with extra virgin olive oil for G2 (amounts according to the prescribed diet) and soy oil (2 g/day) as a placebo for G3 were offered to achieve the desired amounts of dietary lipids. The volunteers were instructed to add the individualized portions of oils directly to the dish (lunch and dinner), no cooking the oil. Regarding the type of oil used to prepare food, G1 and G2 were oriented to use soybean oil and canola oil to cook, respectively, while G3 was instructed to maintain usual oil.
G1 received fish oil capsules (Vital Fish®, Vital Âtman Ltda, SP, Brazil - 2 capsules/ day containing 420 mg of eicosapentaenoic acid [EPA], 220 mg of docosahexaenoic acid [DHA] and 5 mg of vitamin E each) to achieve n-3 PUFAs intake. G2 and G3 received capsule containing 1 g of soybean oil per day (Officilab®, RJ, Brazil). The volunteers were instructed to maintain their usual physical activities during the study, and the level of physical activity was classified as sedentary or light [17].
Adherence to the dietary intervention was assessed by 3-day food record and conference of leftover sachets and capsules, and plasma fatty acids composition analysis was evaluated by gas chromatography (Agilent Technologies, model 7890 A CG System) [19]. Fatty acid composition analysis of the oils was conducted by gas chromatography [20]. For both chromatographic analyses, the internal standard C13:0 (Sigma Aldrich) at 5 mg/mL was used.
For quality control of the oils used during the dietary intervention, the physical-chemical parameters (acidity and peroxide indexes) were monitored per lot (oils and capsules). The extra virgin olive oil was controlled monthly, and the open packages of soybean oil and olive oil were monitored each 15 days for 45 days. The analysis was performed according to the methods proposed by the Institute Adolfo Lutz [21] and the results were evaluated according to the current legislation [22].
Dietary intake assessment
Dietary intake was assessed by 3-day food record (2 typical days and 1 atypical) before and during the intervention period.
The records were analyzed using the Diet Pro®5.5i software (Federal University of Viçosa) and Brazilian Table of Food Composition [16]. Tables of United States Department of Agriculture [23], University of São Paulo [24] and Philippi [25] were used in order of priority when food were not included in Brazilian Table of Food Composition.
The oil supplements (sachets and capsules) were considered in the prescribed diet calculation and in the dietary intake assessment. The chemical composition of the oil supplements was recorded in the diet analysis program based on the results obtained via gas chromatography, and oils used in the preparation of meals were considered in the analysis, as reported in the diet records.
Assessment of energy expenditure and substrate oxidation
The preparation for the EE assessment started 3 days previously. During this period, volunteers were instructed to maintain only their daily activities, avoiding any physical exercises. In addition, the volunteers were instructed not to drink alcoholic beverages, and to avoid excessive intake of foods high in fats, proteins and caffeine.
The evaluation was performed at LANUTRI, using an indirect calorimetry system with a respiratory chamber (Vmax Encore 29 Systems®, Viasys Healthcare, USA). The measurements were performed after a 12-h overnight fast. The volumes of oxygen consumption (VO2) and carbon dioxide produced (VCO2) were measured for 30 min, with the initial 5 min being disregarded. The appropriated equilibrium state was considered when the coefficient of variation for VO2 and VCO2 measurements was up to 10% in five consecutive minutes [26].
The ratio between VCO2 and VO2 (L/min) was used to calculate the respiratory quotient (RQ). The values used for interpreting the RQ were as follows: 0.72 for lipids, 0.80 for proteins, and 1.0 for carbohydrates [14]. The equation described by Weir [14] was used to determine REE: ([3.9 × VO2 L/min] + [1.1 × VCO2 L/min]) × 1440. To determine the TEE, the REE value was multiplied by the corresponding physical activity factor [15].
The equations described by Jéquier, Acheson, and Schutz [27] were used to calculate the substrate oxidation: lipids = (0.75 × NPVO2)/2.019 (g/min); carbohydrate = (0.25 × NPVO2)/0.829 (g/min); and proteins = PVO2/0.966 (g/min). Since NPVO2 = non-protein oxygen volume in L/min; PVO2 = protein oxygen volume in L/min; in which PVO2 (L/min) = nitrogen × 6.25 × 0.966. The NPVO2 value (L/min) was obtained by the difference between VO2 (L/min) and PVO2 (L/min). For the calculation of PVO2, the nitrogen excretion constant of 0.14 g/kg/day was used instead of the urinary nitrogen [28].
Anthropometric and body composition assessments
Anthropometric and body composition assessments were performed in fasting. Total body mass and height were measured using the Filizola® electronic platform scale Personal Line (0.1 kg accuracy and 150 kg maximum capacity) and Alturexata® portable vertical stadiometer (1 mm accuracy and 213 cm maximum capacity), respectively. Measures were performed with light clothing and no footwear. BMI was calculated [29]. The waist circumference (WC) was measured at the midpoint between the last rib and the iliac crest [29], using an inelastic anthropometric tape 2.0 meters long, Sanny® brand with a scale in cm.
Body composition was evaluated by single-frequency electric bioimpedance analysis (Biodynamics® model 450), the fat free mass (FFM) was calculated by the equations of Segal et al. [30], following protocol.
Statistical analysis
Results were expressed as mean and standard deviation (SD). The Kolmogorov–Smirnov test was performed, and the data had a non-normal distribution. Non-parametric tests were used to analyze the data [31]. Statistical analyzes were conducted in SPSS 20.0 program (SPSS, IBM Corporation, NY).
Comparisons between three groups were evaluated by Kruskal-Wallis test. For the variable that presented P < 0.05 post hoc Mann–Whitney U was conducted for comparisons between groups (G1 × G2, G1 × G3, and G2 × G3), followed by adjustment for type I error [32]. Variations between groups were similar. Differences between times in group (from baseline to final value) were evaluated using the Wilcoxon signed-rank test, with a 5% probability.
Results
Quality of the oils
Acidity and peroxide index analysis of the oils used during the dietary intervention showed satisfactory results in all oils lots used (Table 2). The monthly control of extra-virgin olive oil supplied in gallons of 5 liters (Fig. 1) and biweekly monitoring of open packages of soybean oil and olive oil for a period of up to 45 days (Fig. 2) showed suitable values of acidity and peroxide index.

Recommended values: acidity—up to 0.8 g/100 g in oleic acid; peroxide index—up to 20 meq/kg [22]. a Acidity of extra-virgin olive oil; b peroxide index of extra-virgin olive oil.

a Acidity of extra-virgin olive oil; b acidity of soybean oil; c peroxide index of extra-virgin olive oil; d peroxide index soybean oil. Recommended values: olive oil acidity, up to 0.8 g/100 g in oleic acid; soybean oil acidity, up to 0.6 mg KOH/g; olive oil peroxide index, up to 20 meq/kg; soybean oil peroxide index, up to 10 meq/kg [22].
Volunteers and adherence to proposed dietary intervention
Of the 252 volunteers who showed interest in participating of the study, 34 were included and 32 had their data analyzed. The exclusion reasons were no adherence ( < 70%) to the dietary guidelines and insufficient intake of oil supplements (sachets) (Fig. 3).

G1 n-6/n-3 PUFAs-rich diet, G2 MUFAs-rich diet, G3 control group.
Dietary records confirmed differences in SFAs, MUFAs and PUFAs intake between groups. G1 ingested higher total PUFAs, and n-6 and n-3 PUFAs than G2. While G2 had higher MUFAs and higher n-6/n-3 ratio intake than G1. In addition, no differences were found between groups for calories, carbohydrates (g and %), proteins (g and %), total lipids (g and %), and SFAs (g and %) (Table 3).
The intervention groups (G1 and G2) showed lower carbohydrates intake (percentage of TEE) compared to baseline (G1: 50.27% + 5.36 to 43.73% + 4.34, p = 0.02; G2: 52.55% + 5.63 to 44.36% + 4.74, p < 0.01) [data not shown].
Capsules and sachets intake were equivalent in three groups (93.92 ± 5.01%; 97.45 ± 4.00%, and 95.32 ± 5.07%; P = 0.13; 91.26 ± 6.47%; 93.97 ± 6.17 and 91.70 ± 7.99%; P = 0.53, for capsules and sachets in G1, G2 and G3, respectively).
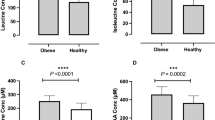
The changes observed in the plasma fatty acids profile at the end of the study confirmed the adherence of the dietary intervention. G1 presented an increase in n-3, EPA and DHA PUFAs, while G2 showed an increase in oleic acid (Fig. 4).

Values are represented as mean ± standard error (for all values). aDifferences between groups analyzed using the Kruskal- Wallis test (for all values). For the variables that presented P < 0.05, the Mann–Whitney U test was used for comparisons between groups (G1 × G2, G1 × G3 and G2 × G3), followed by adjustment for type I error. bG1 differed from G2. cG1 differed from G3. C18:1 n-9, oleic; C18:3 n-3, linolenic; C20:5 n-3, EPA; C22:6 n-3, DHA; C18:2 n-6, linoleic; C20:4 n-6, arachidonic; G1, n-3 and n-6 PUFAs-rich diet (n = 9); G2, MUFAs-rich diet (n = 11); G3, control group (n = 10).
Effect of intervention on anthropometric variables
In the baseline, age, BMI, WC and body fat mass (BFM) were similar between groups. All volunteers presented class I obesity, accumulation of visceral fat and high body adiposity [29]. After intervention, anthropometric and body composition variables did not differ between groups (Table 4).
Comparing anthropometric and body composition data at baseline and after intervention, only G2 showed a decrease in body weight, BMI, WC, and BFM (kg). On the other hand, G3 showed increased BMI and tendency to increase in body weight and WC (Table 4).
Effect of intervention on energy expenditure and substrate oxidation
In the baseline, there was no difference between groups for the EE-related variables. The diets did not change EE and the substrates oxidation. No differences between times and groups was observed, except for protein oxidation. G2 showed a slight increase in protein oxidation after the intervention, however, the variation was very small without clinical relevance and may be due to the small variability of the data (Table 5).
Discussion
Dietary intervention and fats manipulation studies in humans are scarce, especially with individualized dietary prescription and dietary intake control. The present study showed no effect of high-PUFAs diet on anthropometric and body composition parameters. However, high-MUFAs diet caused weight loss and improvement in body composition, with a decrease in abdominal fat accumulation. These results suggest a strategy that may improve management the body weight of women with obesity.
Piers et al. [33] found that the high-MUFAs diet decreases body weight and fat when compared to low-MUFAs diet. Weech et al. [34] observed a reduction in WC after high-MUFAs intervention, but no difference between results provided by high-SFAs or high-n-6 PUFAs diets. According Tutinchi et al. [11], diets enriched in oleic acid can influence fat balance, body weight, central obesity, and possibly energy expenditure. The potential mechanisms involved are regulation of food intake, stimulation lipid oxidation, decreased adipose tissue inflammation and adipogenesis.
Long-term dietary intervention has shown UFAs induce greater EE, DIT, and fat oxidation compared to SFAs [10]. Chain size and saturation degree of fatty acids have been pointed as mechanisms responsible for these effects. DeLany et al. [35] observed that PUFAs and MUFAs are higher oxidized, and SFAs oxidation decreases based on the increase of carbon numbers. However, these effects did not occur in the present study. G2 decreased body weight and fat mass without EE and lipid oxidation alteration.
Studies are inconsistent about the effects of UFAs on weight loss and body fat [36, 37]. Nevertheless, MUFAs resulted in weight loss, and a decrease in WC, BMI, and body fat. These effects may be correlated with the greater satiety promoted by MUFAs [38]. G2 showed lower caloric intake than other groups, but no significant difference between groups.
In addition, G2 and G1 reduced carbohydrates intake (% of TEE) during the intervention when compared to usual intake (P < 0.05) (data not shown), which did not occur in control group (G3), although carbohydrates intake during the intervention was similar in all groups. According to Paniagua et al. [39], increased carbohydrates intake may increase abdominal fat accumulation, and the opposite could be observed with MUFA-rich diet.
Some evidence suggests that n-3 PUFAs provides an additional effect to caloric restriction on weight loss, WC, and body fat decrease [12, 40]. Nevertheless, other study did not verify these effects [41], confirming our results. These divergences may be related to the offered amounts of PUFAs and gender-related differences [40,42]. Crochemore et al. [42] found higher weight loss and decrease in WC with low dose of n-3 PUFAs (540 mg EPA and DHA/day vs 900 mg EPA and DHA/day). Thorsdottir et al. [40] observed additional benefits in fish intake or n-3 PUFAs oil supplementation in men, but not in women. We emphasize that the dose offered in the present study (1.28 g per day of EPA and DHA) was higher than doses used by Crochemore et al. [42].
The limitations of study include the small sample size and short intervention period. Considering these limitations, the controversial results, and the scarcity of long-term investigations, we emphasize the need to conduct new researches with standardized protocols and long-term intervention to evaluate the influence of UFAs in weight loss, body composition and energy metabolism.
High-MUFAs diet for 60 days contributed to weight loss, especially body and abdominal fat, but did not influence EE and substrate oxidation. However, high-n-3 and n-6 PUFAs diet did not change the variables studied. This result suggests a possible benefit of a high-MUFAs diet for the treatment of obesity, however further studies are needed to clarify the effects of different lipids on individuals with obesity.
Data availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Matarese LE, Pories WJ. Adult weight loss diets: metabolic effects and outcomes. Nutr Clin Pract. 2014;29:759–67.
Tay J, Brinkworth GD, Noakes M, Keogh J, Clifton PM. Metabolic effects of weight loss on a very-low-carbohydrate diet compared with an isocaloric high-carbohydrate diet in abdominally obese subjects. J Am Coll Cardiol. 2008;51:59–67.
Kerksick CM, Wismann-Bunn J, Fogt D, Thomas AR, Taylor L, Campbell BI, et al. Changes in weight loss, body composition and cardiovascular disease risk after altering macronutrient distributions during a regular exercise program in obese women. Nutr J. 2010;9:59–78.
de Luis D, Izaola O, Primo D, Aller R. A randomized trial with two hypocaloric diets with different lipid profiles and effects on serum omentin-1 levels in obese subjects. Dis Markers. 2022;2022:6777283.
Yang Q, Lang X, Li W, Liang Y. The effects of low-fat, high-carbohydrate diets vs. low-carbohydrate, high-fat diets on weight, blood pressure, serum liquids and blood glucose: a systematic review and meta-analysis. Eur J Clin Nutr. 2021;76:16–27.
Logan SL, Spriet LL. Omega-3 fatty acid supplementation for 12 weeks increases resting and exercise metabolic rate in healthy community-dwelling older females. PLoS One. 2015;10:e0144828.
Rust BM, Raatz SK, Casperson SL, Duke SE, Picklo MJ. Dietary fat chain length, saturation, and PUFA source acutely diet-induced thermogenesis but not satiety in adults in a randomized, crossover trial. Nutrients. 2021;13:2615.
Smith-Ryan AE, Hirsh KR, Blue MNM, Mock MG, Trexler ET. High-fat breakfast meal replacement in overweight and obesity: implications on body composition, metabolic markers, and satiety. Nutrients. 2019;11:865.
Austel A, Ranke C, Wagner N, Görge J, Ellrott T. Weight loss with a modified Mediterranean-type diet using fat modification: a randomized controlled trial. Eur J Clin Nutr. 2015;69:878–84.
Krishnan S, Cooper JA. Effect of dietary fatty acid composition on susbtrate utilization and body weight maintenance in humans. Eur J Nutr. 2014;53:691–710.
Tutunchi H, Ostadrahimi A, Saghafi-Asl M. The effect of diets enriched in monounsaturated oleicacid on the management and prevention of obesity: a systematic review of human intervention studies. Adv Nutr. 2020;11:864–77.
Salman HB, Salman MA, Akal EY. The effect of omega-3 fatty acid supplementation on weight loss and cognitive function in overweight or obese individuals on weight-loss diet. Nutr Hosp. 2022;39:803–13.
Bellenger J, Bellenger S, Escoula Q, Bidu C, Narce M. N-3 polyunsaturated fatty acids: An innovative strategy against obesity and related metabolic disorders, intestinal alteration and gut microbiota dysbiosis. Biochimie. 2019;159:66–71.
Weir JB. New methods for calculating metabolic rate with special reference to protein metabolism. J Physiol. 1949;109:1–9.
Food and Agriculture Organization of the United Nations (FAO). World Health Organization (WHO). United Nations University (UNU). Human energy requirements. Report of a joint FAO/WHO/UNU expert consultation. Rome: FAO; 2001. [Food and Nutrition Technical Report Series 1.].
Núcleo de Estudos e Pesquisa em Alimentação (NEPA). Universidade Estadual de Campinas (UNICAMP). Tabela brasileira de composição de alimentos (Brazilian table of food composition - Portuguese). versão II. 2th ed. NEPA-UNICAMP, Campinas, SP.
Associação Brasileira para o Estudo da Obesidade e da Síndrome Metabólica (ABESO) (2016) Diretrizes brasileiras de obesidade 2016 (Brazilian obesity guidelines 2016-Portuguese). 4th ed. São Paulo, SP. 2006.
Food and Agriculture Organization of the United Nations (FAO). Fats and fatty acids in human nutrition, Report of an expert consultation. Rome: FAO; 2010.
Xu Z, Harvey K, Pavlina T, Dutot G, Zaloga G, Siddiqui R. An improved method for determining medium- and long-chain FAMEs using gas chromatography. Lipids. 2010;45:199–208.
American Oil Chemists Society (AOCS). AOCS Official Method Ce 2b-11. Sampling and analysis of commercial fats and oils. Direct methylation of lipids in foods by alkali hydrolysis. Champaign, USA: American Oil Chemists Society; 2011.
Instituto Adolfo Lutz. Métodos físico-químicos para análise de alimentos (Physical and chemical methods for food analysis - Portuguese). 4th ed. Instituto Adolfo Lutz: São Paulo; 2008.
Brasil. Agência Nacional de Vigilância Sanitária (ANVISA). Resolução RDC no 270 de 22 de setembro de 2005 (Resolution RDC no 270 of September 22, 2005 - Portuguese). Brasília, DF: Diário Oficial da União, Poder Executivo; 2005.
United States Department of Agriculture (USDA). Agricultural Research Service. National nutrient database for standard reference, release 20. 2007. Nutrient Data Laboratory Home Page. http://www.ars.usda.gov/ba/bhnrc/ndl. Accessed November 2014.
Universidade de São Paulo (USP). Faculdade de Ciências Farmacêuticas. Departamento de Alimentos e Nutrição Experimental/BRASILFOODS. Tabela brasileira de composição de alimentos versão 5.0 (Brazilian food composition table version 5.0- Portuguese). USP, São Paulo. 2008. Internet: http://www.fcf.usp.br/tabela/. Accessed November 2014.
Philippi ST. Tabela de composição de alimentos: suporte para decisão nutricional (Foodcompositiontable: support for nutritional decision - Portuguese). 2th ed. São Paulo: Coronário; 2002.
Compher C, Frankenfield D, Keim N, Roth-Yousey L. Evidence Analysis Working Group. Best practice methods to apply to measurement of resting metabolic rate in adults: a systematic review. J Am Diet Assoc. 2006;106:881–903.
Jéquier E, Acheson K, Schutz Y. Assessment of energy expenditure and fuel utilization in man. Ann Rev Nutr. 1987;7:187–208.
Jones PJ, Schoeller DA. Polyunsaturated: saturated ratio of diet fat influences energy substrate utilization in the human. Metabolism. 1988;37:145–51.
World Health Organization (WHO). Obesity: preventing and managing the global epidemic. Report of a WHO Consultation on Obesity. WHO Technical Report Series, no 894. Geneva: WHO; 2000.
Segal KR, Van Loan M, Fitzgerald PI, Hodgdon JA, Van Itallie TB. Lean body mass estimation by bioelectrical impedance analysis: a four-site cross-validation study. Am J Clin Nutr. 1988;47:7–14.
Chan YH. Biostatistics 101: data presentation. Singapore Med J. 2003;44:280–285.
Chan YH. Biostatistics 102: quantitative data – parametric & non-parametric tests. Singapore Med J. 2003;44:391–96.
Piers LS, Walker KZ, Stoney RM, Soares MJ, O’Dea K. Substitution of saturated with monounsaturated fat in a 4-week diet affects body weight and composition of overweight and obese men. Br J Nutr. 2033;90:717–27.
Weech M, Vafeiadou K, Hasaj M, Todd S, Yaqoob P, Jackson KG, et al. Development of a food-exchange model to replace saturated fat with MUFAs and n-6 PUFAs in adults at moderate cardiovascular risk. J Nutr. 2014;144:846–55.
DeLany JP, Windhauser MM, Champagne CM, Bray GA. Differential oxidation of individual dietary fatty acids in humans. Am J Clin Nutr. 2000;72:905–11.
Tapsell L, Batterham M, Huang XF, Tan SY, Teuss G, Charlton K, et al. Short term effects of energy restriction and dietary fat sub-type on weight loss and disease risk factors. Nutr Metab Cardiovasc Dis. 2010;20:317–25.
Tan SY, Batterham M, Tapsell L. Increased intake of dietary polyunsaturated fat does not promote whole body or preferential abdominal fat mass loss in overweight adults. Obes Facts. 2011;4:352–57.
Maljaars J, Romeyn EA, Haddeman E, Peters HP, Masclee AA. Effect of fat saturation on satiety, hormone release, and food intake. Am J Clin Nutr. 2009;89:1019–24.
Paniagua JA, De La Sacristana AG, Romero I, Vidal-Puig A, Latre JM, Sánchez E, et al. Monounsaturated fat-rich diet prevents central body fat distribution and decreases postprandial adiponectin expression induced by a carbohydrate-rich diet in insulin-resistant subjects. Diabetes Care. 2007;30:1717–23.
Thorsdottir I, Tomasson H, Gunnarsdottir I, Gisladottir E, Kiely M, Parra MD, et al. Randomized trial of weight-loss-diets for young adults varying in fish and fish oil content. Int J Obes. 2007;31:1560–66.
Tapsell LC, Batterham MJ, Charlton KE, Neale EP, Probst YC, O’Shea JE, et al. Foods, nutrients or whole diets: effects of targeting fish and LCn3PUFA consumption in a 12mo weight loss trial. BMC Public Health. 2013;13:1231.
Crochemore IC, Souza AF, de Souza AC, Rosado EL. Omega-3 polyunsaturated fatty acid supplementation does not influence body composition, insulin resistance, and lipemia in women with type 2 diabetes and obesity. Nutr Clin. 2012;27:553–60.
Acknowledgements
We thank for Officilab® (RJ, Brazil) and Vital Âtman® (SP, Brazil) for provide the supplements used by volunteers in this research.
Funding
This work was supported by the Carlos Chagas Filho Foundation for Research Support of the State of Rio de Janeiro (FAPERJ / RJ, Brazil); National Council for Scientific and Technological Development (CNPq / Brasília, DF, Brazil).
Author information
Authors and Affiliations
Contributions
MCOSL concived and designed the experiments, contributed to data extraction, data analysis, and helped write the manuscript, VCK concived and designed the experiments, contributed to data extraction, data analysis, and helped write the manuscript, LC contributed to data extraction and helped write the manuscript, DPC contributed reagentes and materials, provided feedback on the report, ELR concived and designed the experiments, data analysis and provided feedback on the report designed experiments and helped write the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Lopes, M.C.O.d.S., Kaippert, V.C., Crovesy, L. et al. Monounsaturated fat-rich diet reduces body adiposity in women with obesity, but does not influence energy expenditure and substrate oxidation: a parallel randomized controlled clinical trial. Eur J Clin Nutr 78, 335–343 (2024). https://doi.org/10.1038/s41430-024-01401-3
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41430-024-01401-3
