
Abstract
There is currently no consensus on the guidelines for vitamin D prophylaxis in healthy children. The purpose of this study was to investigate the prescribing behaviour of vitamin D prophylaxis among Belgian paediatricians. Between June and September 2022, a questionnaire was distributed by email to all Belgian paediatricians who are a member of at least one of three scientific or professional organisations, as well as to the heads of every Belgian paediatric or neonatal hospital ward. We analysed 426 completed questionnaires. All regions, age categories and subspecialties were represented. Vitamin D prophylaxis is always or frequently recommended by 98% of paediatricians. Fifty-eight per cent of paediatricians advise vitamin D prophylaxis up to the age of six years and 66% of paediatricians advise a daily dose of 400 IU. In nearly every hospital in Belgium (96%), there is a specific protocol for vitamin D prophylaxis for newborns; but not for the paediatric unit (only 30%). Nearly all Belgian paediatricians prescribe vitamin D prophylaxis to infants. Although not recommended by guidelines, 25(OH)D is frequently measured by paediatricians. Practices regarding duration and dosing of vitamin D prophylaxis show large variability. Most neonatal wards do have a protocol, whereas most paediatric wards do not.
Similar content being viewed by others

Introduction
Vitamin D is a prohormone that is indispensable for calcium and phosphorus homeostasis. In its active form, it plays an important role in skeletal development. Recent studies show growing evidence for beneficial effects of vitamin D in extra-skeletal disease such as infectious, auto-immune, cardiovascular and psychiatric disease [1,2,3,4,5]. Consequently, ensuring an adequate vitamin D status might be of major importance. Despite the long-standing recognition for nearly two decades of these advantageous effects and the widespread recommendation of vitamin D supplementation, a high global prevalence of vitamin D deficiency continues to persist [2, 4, 6,7,8,9,10,11].
The absolute threshold for vitamin D deficiency, measured by 25-hydroxy vitamin D (25(OH)D), is still a subject for debate [4, 12]. The current threshold for vitamin D deficiency in Belgium, and neighbouring countries such as the Netherlands and the United Kingdom, is a 25(OH)D level <12 ng/ml (or <30 nmol/l) [13, 14]. Sioen et al. investigated the 25(OH)D status in 4–11 years old Belgian children (n = 357) in 2011 and reported an insufficiency (25(OH)D between 10 and 20 ng/ml) in 58% and vitamin D deficiency (<10 ng/ml) in 5% of children [15].
Studies investigating the 25(OH)D status in Belgian children in the past decennium are lacking. The Belgian Health Council recommends 10 μg (400 international units (IU)) of vitamin D from birth until adolescent age and 15 μg (600 IU) of vitamin D from adolescent age until 18 years [16]. In contrast, the Flemish Society of Paediatrics recommends a daily dose of 400 IU vitamin D from birth until the age of six years, independent of the type of feeding in the neonate and infant and to continue the supplementation beyond six years of age in high-risk populations [14, 17]. Continuing prophylaxis beyond six years of age in healthy children remains a topic of debate. Worldwide, a wide variation in dosing regimens and prophylaxis duration exists (Table 1) [4, 18].
This study evaluates the actual prescribing behaviour of Belgian paediatricians which could ensure a better understanding of the current vitamin D prophylaxis practices.
Materials and methods
We conducted a questionnaire survey among Belgian paediatricians assessing the prescribing behaviour of vitamin D prophylaxis in healthy children. All data were pseudonymised and collected via REDCap© (version 12.4.17, Ghent University, 2022).
In adherence to the requirements stipulated by the General Data Protection Regulation, paediatricians were sent an email containing a questionnaire link through three prominent Belgian paediatric organisations (Belgian Society of Paediatrics (BVK-SBP),Union of Belgian Professional Associations of Doctors-Specialists (VBS-GBS) and Flemish Society of Paediatrics (VVK)). Additionally, all heads of Belgian paediatric and neonatology wards received the same email and were encouraged to share the email with their colleagues. Questionnaires were completed from June 2022 until September 2022.
The email was sent to a total of 786 (VVK), 357 (VBS-GBS), and 1600 (BVK) paediatricians; hereby addressing an unknown proportion of paediatricians more than once. Out of the received 536 questionnaires, 110 were incomplete, resulting in 426 completed questionnaires. We received 66 questionnaires from heads of department, with 57 of them being fully completed. As of 2021, there were 1631 active Belgian paediatricians. Therefore, an estimated response rate of 26% was achieved.
The questions were mainly close-ended and multiple choice (with multiple answer possibilities), a minority was open-ended. The first part concerned characteristics of paediatricians and obtaining informed consent, the second part consisted of the evaluation of individual prescribing behaviour and the last part only addressed heads of department regarding ward protocols. It was only possible to start the second part of the questionnaire once an informed consent was given. Only fully completed questionnaires were included in the analyses. A manual search was performed and no duplicates were found. The time needed to complete the questionnaire was less than five minutes.
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Ethics Committee of University of Ghent (BC-11765, Belgium, 21 March 2022).
Results
We received 426 fully completed questionnaires. In 2021, there were 1631 active Belgian paediatricians in Belgium [19]. Consequently, an estimated response rate of 26% was achieved.
Characteristics
The percentage of respondents per region, per work setting and per duration of career can be found in Table 2. The duration of career as a licensed paediatrician is <5 years, 5–20 years or more than 20 years in, respectively, 22.5%, 44.6% and 32.9% of all participants. There are 57 heads of department (13.4%) participating. Of the 57 heads of department participating in this study, 89.5% are head of a paediatric ward with maternity ward, 3.5% of a paediatric ward without maternity ward and 7% of a Neonatal intensive care unit (NICU). Most (77.2%) heads of department work in Flanders and 10.5% and 12.2% in Brussels and Wallonia, respectively.
Vitamin D suppletion
Most paediatricians (86.9%) always recommend supplementation of vitamin D in healthy children, in general and irrespective of comorbidity, duration or dosage. However, 1% of paediatricians rarely or never recommend vitamin D suppletion (Fig. 1).

Vitamin D supplementation is always, frequently, sometimes, rarely, and never recommended in healthy children by 86.9%, 11%, 1.2%, 0.2% and 0.7% of paediatricians, respectively.
When vitamin D prophylaxis is indicated, 89.9% of Belgian paediatricians ask routinely whether vitamin D suppletion is already started.
Daily dosage
The most frequent recommended daily dose of vitamin D suppletion is 400 IU (66%). The answers ranged from 200 IU to 2000 IU with a median of 400 IU (Fig. 2), with 800 IU being recommended by 24% and >800 IU by 5%. Recommendation of 400 IU by 295 paediatricians and 800 IU by 102 paediatricians. Three and 23 paediatricians answered to recommend <400 IU and ≥1000 IU, respectively.

X-as: percentage of participants, y-as: the dosage of vitamin D in international units.
When adjusted for region, the dosage of 800 IU is more frequently recommended in Wallonia (54.9%) and Brussels (32.7%) than in Flanders (11,9%). When adjusted for work setting, 11 out of 102 paediatricians that answered 800 IU work at a NICU.
The majority of paediatricians (81.6%) adjust the daily dose of vitamin D depending on skin colour (78.6%), disease (acute or chronic) (30.7%), seasonality (17.7%), age (26.7%) and/or based on other reasons (e.g. low vitamin D status, prematurity, …) (23.5%).
Duration
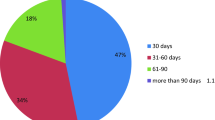
Only 58% recommend vitamin D prophylaxis until 6 years of age, although up to 6 years is the Flemish consensus recommendation. A wide variety in answers is observed (Fig. 3). A duration of <6, 6, 6–18 and \(\ge \)18 years is recommended by 15%, 57.7%, 18.7% and 8.4% paediatricians, respectively. Ten per cent recommend vitamin D suppletion until 18 years of age and another 8% recommend vitamin D prophylaxis into adulthood (i.e. ≥18 years). When adjusted for region, paediatricians working in Flanders more frequently recommend a duration of 6 years. Ninety-six per cent of all paediatricians recommending six years of prophylaxis, work in Flanders; the remaining 3% in Brussels and 2.4% in Wallonia. Six years is the least recommended duration of the four groups (<6, 6, 6–18, >18) in Brussels and Wallonia.

X-as: percentage of participants, y-as: duration of recommended vitamin D prophylaxis in years.
In contrast to the daily dosage, most paediatricians (60.6%) do not adapt the duration of vitamin D prophylaxis based on individual characteristics of the children. The paediatricians that adapt the duration do so based on skin colour (60.7%), seasonality (56.5%), disease (acute or chronic) (50.6%), age (47.9%) or because of another reason that was not otherwise specified (18.5%).
In general
In general, independently of dosage and duration, vitamin D suppletion is adjusted by 71.6% of paediatricians based on skin colour. Moreover, 41.4% take seasonality into account, 38.3% the amount of sun exposure and 6.8% the amount of vitamin D already present in nutrition.
Determination of 25(OH)D levels
The percentage of Belgian paediatricians that measure 25(OH)D and alkaline phosphatase, when a blood draw is required for whatever indication, is represented in Table 3.
Protocols on the wards
Maternity ward
Fifty-five (96.5%) out of 57 heads of department indicate that their maternity ward has a specific vitamin D protocol, recommending vitamin D suppletion in all children. In 43/55 (78%) maternity wards, the recommended daily dose of vitamin D suppletion is 400 IU. There are 10 maternity wards that recommend a daily dose of 800 IU, one ward that recommends 200 IU and one ward that recommends 1000 IU. In 34/55 (61.8%) maternity wards, the dosage is respectively adjusted for skin colour (97.1%), prematurity (38.2%), disease (acute or chronic) (8.8%), seasonality (2.9%) and exclusive breastfeeding (2.9%).
Vitamin D is recommended until the age of six years in 43/55 (78%) maternity wards, in line with the current recommendations. However, in 8/55 (14.5%) departments vitamin D is recommended only until the age of two years and one department recommends supplementation until the age of 18 years.
Paediatric ward
Only 17 (29.8%) of the 57 heads of department confirm the existence of a specific vitamin D protocol on the paediatric ward. Of these 17 heads of department, four work solely in a NICU, one at a paediatric ward without maternity ward and the remaining 12 work at a paediatric ward with a maternity ward. When analysed per region, a lack of protocols of vitamin D on the paediatric wards is most common in Brussels. In Flanders and Wallonia, 14/44 (31.8%) and 3/7 (42.9%) hospitals have a paediatric protocol, in contrast with Brussels; were none of the six hospitals have a specific paediatric protocol for vitamin D suppletion.
The recommended daily dose of vitamin D is 400 IU in 13 (76%) paediatric wards. In the remaining 4 wards, 800 IU is recommended daily. The daily dose of vitamin D is adjusted based on certain characteristics in 14/17 (82.4%) paediatric wards. Skin colour, disease (acute or chronic), age, sun exposure, seasonality and other reasons (exclusive breastfeeding, and pregnancy duration and blood results) are respectively adjusted for in all wards (100%), three (21.4%), two (14.3%), two (14.3%), one (7.1%) and two (14.3%), respectively. Furthermore, vitamin D is recommended until the age of 6 years in 12 wards (70%). Two wards recommend vitamin D until three years, one ward until five years and one ward until 12 years. There is 1 ward that recommends vitamin D prophylaxis beyond the age of 18. When a child is admitted to the hospital, it is standard practice in 31/57 (54,4%) wards to ask if the patient is already taking vitamin D suppletion.
Discussion
The high prevalence of vitamin D deficiency and the worldwide variation in guidelines for vitamin D prophylaxis warrant an evaluation of the prescribing behaviour of vitamin D. In our study, vitamin D suppletion in healthy children is generally recommended in healthy children by over 99% of paediatricians and 98% recommend suppletion until at least 1 year of age, in line with the Flemish consensus statement [14]. Recommendations about dosing (400–1000 IU) and duration (1–18 years) vary substantially. Moreover, paediatricians generally take different factors into account for dose and duration adjustments. Skin colour, seasonality, sun exposure and presence in nutrition is adjusted for by 71.6%, 41.4%, 38.3% and 6.8% of participants. Vitamin D protocols are substantially more present in maternity wards than in paediatric wards (96% vs. 30%).
Approximately 26% of Belgian paediatricians participated in our study. All age categories, regions and working contexts were represented. Most participating paediatricians work at a paediatric ward in Flanders, in line with the current Belgian context. Although the data on characteristics of the paediatricians was limited; a good representation of the current population of Belgian paediatricians can be assumed.
In most Western countries the recommended daily dosage for vitamin D prophylaxis is 400 IU per day [4, 13, 18, 20]. This is also the dosage recommended by the majority of Belgian paediatricians. However, 800 IU or more is recommended by 29% of the participants. European authorities and authors have generally recommended a dose of 800 IU to 1000 IU vitamin D daily in preterm infants, however, only 11 out of 102 paediatricians that answered 800 IU indicated to work at an NICU. Interestingly, 800 IU is more frequently recommended in Wallonia and Brussels. In Brussels, this could be attributed to a more diverse population with a large diversity in pigmented skin and the need for a higher dosage of vitamin D can be more frequently present. In Wallonia, it can be attributed to the close relation with France where 400 to 800 IU is recommended daily (Table 1) [16, 18]. However, the national recommendation of the Belgian Health Council also recommends 400 IU daily [16]. In our study, skin colour, notably the pigmentation of the skin, was the most important characteristic for an adjustment in dosage of vitamin D.
In 2019, Santi et al. investigated the prescribing behaviour of vitamin D in healthy children by Swiss paediatricians. Vitamin D supplementation in Switzerland is recommended in the first three years of life and during winter in older children. Santi et al. found that vitamin D is routinely prescribed in children of \(\le \)1 year but only few paediatricians prescribe a vitamin D supplement in children older than three years of age in winter [21]. The duration of vitamin D prophylaxis in healthy children varies amongst most countries; however, most recommend vitamin D prophylaxis at least until one year of age [4, 14, 18, 21, 22], some until 18 years of age [18].
Six years is the median recommended duration of vitamin D suppletion by our participants, in line with the Flemish consensus statement. However, only 58% recommend vitamin D prophylaxis until six years of age and 18% recommend vitamin D suppletion until 18 years or older. Paediatricians working in Flanders adhere mostly to the Flemish consensus statement. The absence of recommendation until six years of age in Wallonia and Brussels could be attributed to influence of the national guideline of France recommending vitamin D suppletion until 18 years of age [18].
In contrast to the daily dosage of vitamin D prophylaxis, most paediatricians (60.6%) generally do not adapt the duration of vitamin D prophylaxis based on individual characteristics of the children. When prescribing vitamin D prophylaxis in general, 72% of paediatricians take skin colour into account. Additionally, more than 40% take seasonality into account.
Overall, Belgian paediatricians encourage vitamin D prophylaxis. Consequently, in more than half of the hospital wards it is routinely checked whether the admitted child is taking vitamin D prophylaxis. More than half of the Belgian paediatricians frequently measure 25(OH)D whenever a blood draw is required for whatever reason. However, the interpretation of the status of 25(OH)D is a subject of controversy. It is not recommended to routinely measure 25(OH)D levels due to the insufficient evidence supporting the benefits of screening for vitamin D deficiency at a population level [14, 22]. In our study, the frequent measurement of 25(OH)D could be attributed to the unclarity of screening guidelines for 25(OH)D status or to the idea that if a blood draw is required, the clinical image would be sufficiently severe warranting a 25(OH)D status. Almost one-third of paediatricians rarely to never measure alkaline phosphatase although alkaline phosphatase is a good biochemical marker of metabolic disease [23].
Concerning the ward-specific protocols, in most paediatric wards, a vitamin D prophylaxis protocol is lacking. This is in great contrast with the maternity ward, where a vitamin D prophylaxis protocol exists in 96,5% of wards. It could, however, be attributed to the expectation that every paediatrician should be familiar with and implement the current Flemish consensus recommendation and recommendation of the Belgian Health Council.
The recommendations of the vitamin D protocols on the paediatric wards are mostly but not completely in line with the current Flemish consensus statement. The recommendations of the vitamin D protocol in most maternity wards, lay in line with the current Flemish consensus statement. The observed higher dosage of 800 IU can be attributed to the admission of moderate to late preterm infants for whom 800 IU can be indicated following the international guidelines [24, 25]. In addition, given the large gap between the recommended daily dosage and the toxicity limit, it could be that paediatricians tend to dose higher because the risk of vitamin D intoxication is low [10]. The suppletion duration is limited to two years of age in 14% of hospitals, however, recommending the correct duration of vitamin D prophylaxis from the start to avoid confusion and mistrust among parents is important.
Our study should be interpreted within the context of its limitations. Firstly, we potentially did not reach every paediatrician. Moreover, the response rate remains an estimate. Secondly, the study is subject to all types of bias inherent to a survey (a.o. sampling bias, (non-)response bias, acquiescence bias). Finally, this study does not disclose why Belgian paediatricians sometimes do not adhere to the current Flemish consensus recommendation. In depth semi-structured interviews could further investigate this issue.
One national guideline that suits all healthy Belgian children could facilitate uniformity in practice. This article aims to guide future guideline updates at the national level. In addition, research confirming normalising 25(OH)D status in Belgian children when following the current guideline is needed, next to well-defined global definitions of hypovitaminosis D and vitamin D deficiency. Routine 25(OH)D testing should not be performed [14, 18, 22], although about half of the respondents did add 25(OH)D to their requests when a blood draw was indicated for whatever reason. Future information campaigns and/or guidelines should further address this issue. The availability of a standardised vitamin D protocol in both maternity and paediatric wards following the current Flemish consensus statement could help diminish the observed differences.
Conclusions
Overall, Belgian paediatricians are well-informed and adherent to the recommendations regarding vitamin D prophylaxis in healthy children. Different dosing regimens and prophylaxis duration have been observed. Lack of existence of protocols for vitamin D prophylaxis in the paediatric wards may contribute to this variability, but most neonatal wards do have a protocol.
Although routine 25(OH)D testing is not recommended, Belgian paediatricians report regular routine add-on measurements. To our knowledge, this is the first study investigating Belgian paediatricians’ prescribing behaviour of vitamin D prophylaxis in healthy children. This study aims to guide Belgian paediatricians and policy makers in developing future guidelines for vitamin D prophylaxis in healthy children. Future research investigating the 25(OH)D levels in Belgian children receiving vitamin D prophylaxis following the current guideline might direct future recommendations.
Data availability
Our data was collected via REDCap. The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
References
Focker M, Antel J, Ring S, Hahn D, Kanal O, Ozturk D, et al. Vitamin D and mental health in children and adolescents. Eur Child Adolesc Psychiatry. 2017;26:1043–66.
Antonucci R, Locci C, Clemente MG, Chicconi E, Antonucci L. Vitamin D deficiency in childhood: old lessons and current challenges. J Pediatr Endocrinol Metab. 2018;31:247–60.
Holick MF. Vitamin D deficiency. N Engl J Med. 2007;357:266–81.
Saggese G, Vierucci F, Prodam F, Cardinale F, Cetin I, Chiappini E, et al. Vitamin D in pediatric age: consensus of the Italian Pediatric Society and the Italian Society of Preventive and Social Pediatrics, jointly with the Italian Federation of Pediatricians. Italian J Pediatrics. 2018;44. https://doi.org/10.1186/s13052-018-0488-7.
Glabska D, Kolota A, Lachowicz K, Skolmowska D, Stachon M, Guzek D. The influence of vitamin D intake and status on mental health in children: a systematic review. Nutrients. 2021;13. https://doi.org/10.3390/nu13030952.
Kumar J, Muntner P, Kaskel FJ, Hailpern SM, Melamed ML. Prevalence and associations of 25-hydroxyvitamin D deficiency in US children: NHANES 2001-4. Pediatrics. 2009;124:e362–370.
Zhu Z, Zhan J, Shao J, Chen W, Chen L, Li W, et al. High prevalence of vitamin D deficiency among children aged 1 month to 16 years in Hangzhou, China. BMC Public Health. 2012;12:126.
Ganji V, Zhang X, Tangpricha V. Serum 25-hydroxyvitamin D concentrations and prevalence estimates of hypovitaminosis D in the U.S. population based on assay-adjusted data. J Nutr. 2012;142:498–507.
Gonzalez-Gross M, Valtuena J, Breidenassel C, Moreno LA, Ferrari M, Kersting M, et al. Vitamin D status among adolescents in Europe: the Healthy Lifestyle in Europe by Nutrition in Adolescence study. Br J Nutr. 2012;107:755–64.
Holick MF. The vitamin D deficiency pandemic: approaches for diagnosis, treatment and prevention. Rev Endocr Metab Disord. 2017;18:153–65.
Mogire RM, Mutua A, Kimita W, Kamau A, Bejon P, Pettifor JM, et al. Prevalence of vitamin D deficiency in Africa: a systematic review and meta-analysis. Lancet Glob Health. 2020;8:e134–e142.
Cashman KD, Dowling KG, Skrabakova Z, Gonzalez-Gross M, Valtuena J, De Henauw S, et al. Vitamin D deficiency in Europe: pandemic? Am J Clin Nutr. 2016;103:1033–44.
Passeron T, Bouillon R, Callender V, Cestari T, Diepgen TL, Green AC, et al. Sunscreen photoprotection and vitamin D status. Br J Dermatol. 2019;181:916–31.
Raaijmakers A, Van Winckel M, Plaete J, Bovijn L, Van Overmeire B, Vandenplas Y, et al. Vitamine D voor kinderen in Vlaanderen. Tijdschrift voor Geneeskunde. 2023;79. https://doi.org/10.47671/tvg.78.22.064.
Sioen I, Mouratidou T, Kaufman JM, Bammann K, Michels N, Pigeot I, et al. Determinants of vitamin D status in young children: results from the Belgian arm of the IDEFICS (Identification and Prevention of Dietary- and Lifestyle-Induced Health Effects in Children and Infants) Study. Public Health Nutr. 2012;15:1093–9.
Voedingsaanbevelingen voor België - 2016. Brussels: Superior Health Council; 2016. Report No.: 9285.
De Ronne N, De Schepper J, Societe flamande de P [Recommendations for vitamin D supplementation in infants and young children]. J Pharm Belg. 2013:12–21. https://www.ncbi.nlm.nih.gov/pubmed/24804408.
Bacchetta J, Edouard T, Laverny G, Bernardor J, Bertholet-Thomas A, Castanet M, et al. Vitamin D and calcium intakes in general pediatric populations: A French expert consensus paper. Arch Pediatr. 2022;29:312–25.
RIZIV. Beroepsbeoefenaars met recht om prestaties te verrichten (31-12-2021) en actieve beroepsbeoefenaars (jaar 2021) per beroepsgroep 2022 [1.11.2022]. Available from: https://www.riziv.fgov.be/SiteCollectionDocuments/statistiek_2021_gv_proff_tabel1.pdf.
EFSA NDA Panel (EFSA Panel) on Dietetic Products NaA Dietary reference values for vitamin D. EFSA J. 2016;14:4547.
Santi M, Janner M, Simonetti GD, Lava SAG. Prescription of vitamin D among Swiss pediatricians. Eur J Pediatr. 2019;178:1119–23.
Holick MF, Binkley NC, Bischoff-Ferrari HA, Gordon CM, Hanley DA, Heaney RP, et al. Evaluation, treatment, and prevention of vitamin D deficiency: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2011;96:1911–30.
Pereira-da-Silva L, Virella D, Fusch C. Nutritional assessment in preterm infants: a practical approach in the NICU. Nutrients. 2019;11. https://doi.org/10.3390/nu11091999.
Yadav B, Gupta N, Sasidharan R, Thanigainathan S, Purohit P, Singh K, et al. 800 IU versus 400 IU per day of vitamin D(3) in term breastfed infants: a randomized controlled trial from an LMIC. Eur J Pediatr. 2022;181:3473–82.
Natarajan CK, Sankar MJ, Agarwal R, Pratap OT, Jain V, Gupta N, et al. Trial of daily vitamin D supplementation in preterm infants. Pediatrics. 2014;133:e628–634.
Author information
Authors and Affiliations
Contributions
Conceptualisation: CDC, MVW, AR, YV. Methodology: CDC, MVW, AR, YV. Software: CDC. Validation: CDC, MVW, AR, YV. Formal Analysis: CDC. Investigation: CDC, MVW, AR, YV. Resources: does not apply. Data Curation: CDC, MVW, AR, YV. Writing – Original Draft Preparation: CDC. Writing - Review & Editing: CDC, MVW, AR, YV. Visualisation: CDC. Supervision: MVW, AR, YV. Project Administration: CDC, MVW, AR, YV.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Ethics Committee of University of Ghent (BC-11765, Belgium, 21 March 2022).
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
De Crem, C., Van Winckel, M., Vandenplas, Y. et al. Self-reported prescribing behaviour of vitamin D prophylaxis in healthy children by Belgian paediatricians. Eur J Clin Nutr 78, 295–300 (2024). https://doi.org/10.1038/s41430-023-01387-4
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41430-023-01387-4
