
Abstract
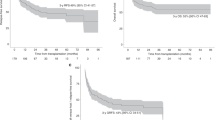
The optimal CD34 + cell dose in the setting of RIC allo-HCT for myelofibrosis (MF) remains unknown. We retrospectively analyzed 657 patients with primary or secondary MF transplanted with use of peripheral blood (PB) stem cells after fludarabine/melphalan or fludarabine/busulfan RIC regimen. Median patient age was 58 (range, 22–76) years. Donors were HLA-identical sibling (MSD) or unrelated (UD). Median follow-up was 46 (2–194) months. Patients transplanted with higher doses of CD34 + cells (>7.0 × 106/kg), had an increased chance of achievement of both neutrophil (hazard ratio (HR), 1.46; P < 0.001) and platelet engraftment (HR, 1.43; P < 0.001). In a model with interaction, for patients transplanted from a MSD, higher CD34 + dose was associated with improved overall survival (HR, 0.63; P = 0.04) and relapse-free survival (HR, 0.61; P = 0.02), lower risk of non-relapse mortality (HR, 0.57; P = 0.04) and higher rate of platelet engraftment. The combined effect of higher cell dose and UD was apparent only for higher neutrophil and platelet recovery rate. We did not document any detrimental effect of high CD34 + dose on transplant outcomes. More bulky splenomegaly was an adverse factor for survival, engraftment and NRM. Our analysis suggests a potential benefit for MF patients undergoing RIC PB-allo-HCT receiving more than 7.0 × 106/kg CD34 + cells.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout


Similar content being viewed by others


References
Moulard O, Mehta J, Fryzek J, Olivares R, Iqbal U, Mesa RA. Epidemiology of myelofibrosis, essential thrombocythemia, and polycythemia vera in the European Union. Eur J Haematol. 2014;92:289–97.
Schieber M, Crispino JD, Stein B. Myelofibrosis in 2019: moving beyond JAK2 inhibition. Blood Cancer J. 2019;9:74.
Harrison CN, Vannucchi AM, Kiladjian JJ, Al-Ali HK, Gisslinger H, Knoops L, et al. Long-term findings from COMFORT-II, a phase 3 study of ruxolitinib vs best available therapy for myelofibrosis. Leukemia. 2016;30:1701–7.
Verstovsek S, Mesa RA, Gotlib J, Gupta V, DiPersio JF, Catalano JV, et al. Long-term treatment with ruxolitinib for patients with myelofibrosis: 5-year update from the randomized, double-blind, placebo controlled, phase 3 COMFORT-I trial. J Hematol Oncol. 2017;10:55.
Barbui T, Tefferi A, Vannucchi AM, Passamonti F, Silver RT, Hoffman R, et al. Philadelphia chromosome-negative classical myeloproliferative neoplasms: revised management recommendations from European LeukemiaNet. Leukemia 2018;32:1057–69.
McLornan DP, Yakoub-Agha I, Robin M, Chalandon Y, Harrison CN, Kroger N. State-of-the-art review: allogeneic stem cell transplantation for myelofibrosis in 2019. Haematologica. 2019;104:659–68.
McLornan DP, Sirait T, Hernández-Boluda JC, Czerw T, Hayden P, Yakoub-Agha I. European wide survey on allogeneic haematopoietic cell transplantation practice for myelofibrosis on behalf of the EBMT chronic malignancies working party. Curr Res Transl Med. 2021;69:103267.
Zaucha JM, Gooley T, Bensinger WI, Heimfeld S, Chauncey TR, Zaucha R, et al. CD34 cell dose in granulocyte colony-stimulating factor-mobilized peripheral blood mononuclear cell grafts affects engraftment kinetics and development of extensive chronic graft-versus-host disease after human leukocyte antigen-identical sibling transplantation. Blood. 2001;98:3221–7.
Perez-Simon JA, Diez-Campelo M, Martino R, Sureda A, Caballero D, Canizo C, et al. Impact of CD34+ cell dose on the outcome of patients undergoing reduced-intensity-conditioning allogeneic peripheral blood stem cell transplantation. Blood 2003;102:1108–13.
Törlén J, Ringdén O, Le Rademacher J, Batiwalla M, Chen J, Erkers T, et al. Low CD34 dose is associated with poor survival after reduced-intensity conditioning allogeneic transplantation for acute myeloid leukemia and myelodysplastic syndrome. Biol Blood Marrow Transpl. 2014;20:1418–25.
Remberger M, Törlén J, Ringdén O, Engström M, Watz E, Uhlin M, et al. Effect of Total Nucleated and CD34(+) Cell Dose on Outcome after Allogeneic Hematopoietic Stem Cell Transplantation. Biol Blood Marrow Transpl. 2015;21:889–93.
McLornan D, Szydlo R, Koster L, Chalandon Y, Robin M, Wolschke C, et al. Myeloablative and Reduced-Intensity Conditioned Allogeneic Hematopoietic Stem Cell Transplantation in Myelofibrosis: a Retrospective Study by the Chronic Malignancies Working Party of the European Society for Blood and Marrow Transplantation. Biol Blood Marrow Transpl. 2019;25:2167–71.
Robin M, Porcher R, Wolschke C, Sicre de Fontbrune F, Alchalby H, Christopeit M, et al. Outcome after Transplantation According to Reduced-Intensity Conditioning Regimen in Patients Undergoing Transplantation for Myelofibrosis. Biol Blood Marrow Transpl. 2016;22:1206–11.
Giralt S, Ballen K, Rizzo D, Bacigalupo A, Horowitz M, Pasquini M, et al. Reduced-intensity conditioning regimen workshop: defining the dose spectrum. Report of a workshop convened by the center for international blood and marrow transplant research. Biol Blood Marrow Transpl. 2009;15:367–9.
Bacigalupo A, Ballen K, Rizzo D, Giralt S, Lazarus H, Ho V, et al. Defining the intensity of conditioning regimens: working definitions. Biol Blood Marrow Transpl. 2009;15:1628–33.
Przepiorka D, Weisdorf D, Martin P, Klingemann HG, Beatty P, Hows J, et al. 1994 Consensus Conference on Acute GVHD Grading. Bone Marrow Transpl. 1995;15:825–8.
Shulman HM, Sullivan KM, Weiden PL, McDonald GB, Striker GE, Sale GE, et al. Chronic graft-versus-host syndrome in man. A long-term clinicopathologic study of 20 Seattle patients. Am J Med. 1980;69:204–17.
Kaplan EL, Meier P. Non parametric estimation from incomplete observations. J Am Stat Assoc. 1958;53:457–81.
Gooley TA, Leisenring W, Crowley J, Storer BE. Estimation of failure probabilities in the presence of competing risks: new representations of old estimators. Stat Med. 1999;18:665–706.
Cox DR. Regression models and life tables. J R Stat Soc. 1972;34:187–202.
Therneau TM, Grambsch PM. Modeling survival data: extending the cox model. Berlin:Springer;2000.
Pulsipher MA, Chitphakdithai P, Logan BR, Leitman SF, Anderlini P, Klein JP, et al. Donor, recipient, and transplant characteristics as risk factors after unrelated donor PBSC transplantation: beneficial effects of higher CD34+ cell dose. Blood 2009;114:2606–16.
Remberger M, Mattsson J, Hassan Z, Karlsson N, LeBlanc K, Omazic B, et al. Risk factors for acute graft-versus-host disease grades II-IV after reduced intensity conditioning allogeneic stem cell transplantation with unrelated donors: a single centre study. Bone Marrow Transpl. 2008;41:399–405.
Nakamura R, Auayporn N, Smith DD, Palmer J, Sun JY, Schriber J, et al. Impact of graft cell dose on transplant outcomes following unrelated donor allogeneic peripheral blood stem cell transplantation: higher CD34+ cell doses are associated with decreased relapse rates. Biol Blood Marrow Transpl. 2008;14:449–57.
Czerw T, Labopin M, Schmid C, Cornelissen JJ, Chevallier P, Blaise D et al. High CD3+ and CD34+ peripheral blood stem cell grafts content is associated with increased risk of graft-versus-host disease without beneficial effect on disease control after reduced-intensity conditioning allogeneic transplantation from matched unrelated donors for acute myeloid leukemia - an analysis from the Acute Leukemia Working Party of the European Society for Blood and Marrow Transplantation. Oncotarget. 2016;7:27255–66.
Tsirigotis P, Shapira MY, Or R, Bitan M, Samuel S, Gesundheit B, et al. The number of infused CD34+ cells does not influence the incidence of GVHD or the outcome of allogeneic PBSC transplantation, using reduced-intensity conditioning and antithymocyte globulin. Bone Marrow Transpl. 2010;45:1189–96.
Collignon A, Calmels B, Harbi S, Fürst S, Granata A, Faucher C, et al. Impact of CD34-positive cell dose on outcome after peripheral blood stem cell allogeneic transplantation prepared with ATG-based reduced intensity conditioning regimen. Am J Hematol. 2017;92:E57–E59.
Gómez-Almaguer D, Gómez-Peña Á, Jaime-Pérez JC, Gómez-Guijosa MÁ, Cantú-Rodríguez O, Gutiérrez-Aguirre H, et al. Higher doses of CD34+ progenitors are associated with improved overall survival without increasing GVHD in reduced intensity conditioning allogeneic transplant recipients with clinically advanced disease. J Clin Apher. 2013;28:349–55.
Alchalby H, Yunus DR, Zabelina T, Ayuk F, Kröger N. Incidence and risk factors of poor graft function after allogeneic stem cell transplantation for myelofibrosis. Bone Marrow Transpl. 2016;51:1223–7.
Hernández-Boluda JC, Pereira A, Kröger N, Beelen D, Robin M, Bornhäuser M, et al. Determinants of survival in myelofibrosis patients undergoing allogeneic hematopoietic cell transplantation. Leukemia 2021;35:215–24.
Slot S, Smits K, van de Donk NW, Witte BI, Raymakers R, Janssen JJ, et al. Effect of conditioning regimens on graft failure in myelofibrosis: a retrospective analysis. Bone Marrow Transpl. 2015;50:1424–31.
Hart C, Klatt S, Barop J, Müller G, Schelker R, Holler E, et al. Splenic pooling and loss of VCAM-1 causes an engraftment defect in patients with myelofibrosis after allogeneic hematopoietic stem cell transplantation. Haematologica 2016;101:1407–16.
Lickliter JD, McGlave PB, DeFor TE, Miller JS, Ramsay NK, Verfaillie CM, et al. Matched-pair analysis of peripheral blood stem cells compared to marrow for allogeneic transplantation. Bone Marrow Transpl. 2000;26:723–8.
Anasetti C, Logan BR, Lee SJ, Waller EK, Weisdorf DJ, Wingard JR, et al. Blood and Marrow Transplant Clinical Trials Network. Peripheral-blood stem cells versus bone marrow from unrelated donors. N Engl J Med. 2012;367:1487–96.
Polverelli N, Mauff K, Kröger N, Robin M, Beelen D, Beauvais D, et al. Impact of spleen size and splenectomy on outcomes of allogeneic hematopoietic cell transplantation for myelofibrosis: a retrospective analysis by the chronic malignancies working party on behalf of European society for blood and marrow transplantation (EBMT). Am J Hematol. 2021;96:69–79.
Bacigalupo A, Soraru M, Dominietto A, Pozzi S, Geroldi S, Van Lint MT, et al. Allogeneic hemopoietic SCT for patients with primary myelofibrosis: a predictive transplant score based on transfusion requirement, spleen size and donor type. Bone Marrow Transpl. 2010;45:458–63.
Acknowledgements
The authors would like to thank all investigators and data managers in the EBMT participating centers for their contribution to this analysis. Detailed list is presented in Supplementary Appendix.
Author information
Authors and Affiliations
Contributions
TC was the primary investigator for this study. TC, SI, VM, LC, PH, JCH-B, DM, and IY-A designed the study, the synopsis of which was approved by the Chronic Malignancies Working Party of the EBMT. SI, VM, and LC did the statistical analysis. TC wrote the first draft of the paper. All other co-authors contributed data to the EBMT registry, read the paper and approved the final version.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
About this article

Cite this article
Czerw, T., Iacobelli, S., Malpassuti, V. et al. Impact of donor-derived CD34 + infused cell dose on outcomes of patients undergoing allo-HCT following reduced intensity regimen for myelofibrosis: a study from the Chronic Malignancies Working Party of the EBMT. Bone Marrow Transplant 57, 261–270 (2022). https://doi.org/10.1038/s41409-021-01540-2
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41409-021-01540-2
This article is cited by
-
Fresh or frozen grafts for allogeneic stem cell transplantation: conceptual considerations and a survey on the practice during the COVID-19 pandemic from the EBMT Infectious Diseases Working Party (IDWP) and Cellular Therapy & Immunobiology Working Party (CTIWP)
Bone Marrow Transplantation (2023)
-
Myelofibrosis: let’s go high!
Bone Marrow Transplantation (2021)
