
Abstract
Gefitinib has been available in the market for 20 years, but its pharmacokinetic mechanism of response is little known. In this study, we examined the pharmacokinetic and metabolomic profiles in non-small cell lung cancer (NSCLC) patients with sensitive EGFR mutations. A total of 216 advanced NSCLC patients were enrolled, and administered gefitinib at the standard dosage of 250 mg/day, which was established in heterogeneous subjects with non-sensitive mutations. We identified and quantified three main metabolites (named as M1, M2 and M3) in the plasma of patients, the correlations between the concentration of gefitinib/metabolites and efficacy were analyzed. In exploratory and validation set, gefitinib concentration was not correlated with clinical effects. Considering the result that the therapeutic effects of 250 mg/2-day was better than that of 250 mg/day in a multiple center clinical trial, the standard dose might be higher than that for maximal efficacy according to the hypothetical dose-response curve. Among the three metabolites, the IC50 of M2 in HCC827 and PC9 cell lines was significantly lower, and Conc.brain/Conc.plasma of M2 in mice was significantly higher than those of gefitinib, suggesting its higher potential to penetrate blood–brain barrier and might be more effective in the treatment of brain metastatic tumor than gefitinib. Consistently and attractively, higher M2 plasma concentration was found to be correlated with better clinical outcome in patients with brain metastases (the median PFS of CM2 < 12 ng/mL and CM2 ≥ 12 ng/mL were 17.0 and 27.1 months, respectively, P = 0.038). The plasma concentration of M2 ≥ 12 ng/mL was a strong predictor of the PFS of NSCLC patients. In conclusion, for NSCLC patients with EGFR sensitive mutations, the standard dose is suspectable and could be decreased reasonably. M2 plays an important role in efficacy and may be more effective in the treatment of metastatic tumor than gefitinib.
Similar content being viewed by others


Introduction
Gefitinib, the first marketed inhibitor of the epidermal growth factor receptor-tyrosine kinase (EGFR-TKI), is administered at the standard dosage of 250 mg/day to patients with advanced non-small cell lung cancer (NSCLC) [1]. The standard dosage of 250 mg/day was recommended by a randomized, double-blind, parallel group, phase II multicenter trial where the subjects were heterogeneous and most of whom were lack of the sensitive mutation of EGFR [2]. However, at present, the targeted patients of gefitinib are those with sensitive mutation of EGFR. Therefore, it is possible that the standard dosage of 250 mg/day is not suitable for the real patients.
In fact, almost all the TKIs were marketed by accelerated approval or fast-track without systemic clinical research at all [3, 4]. Moreover, even post-market, no extensive clinical trials are conducted to investigate the pharmacokinetic (PK) and pharmacodynamic (PD) characteristics of TKIs, including gefitinib [3]. This was caused by two aspects: one is high frequency of resistance, for example, more than 80% patients treated with gefitinib suffered resistance after two-years’ administration [5]. The other is the rapid development of the second- and third-generation TKIs [6]. The patients who experienced the resistance of gefitinib are often alternatively treated with the second and third generation TKIs [7]. Time and costs are reduced on the systemic investigation to resolve the problems faced in the clinical application of the marketed TKIs, including gefitinib, due to rapid marketing approval process and rapid replacement.
Without PK study, it is not known what happened for the TKIs in vivo. For example, significant inter-individual variability was observed in the therapeutic responses (progression free survival ranging from 1 to 20 months) and the incidence of adverse effects was high, but the underlying mechanism remains unclear [1, 8]. A clinical trial found that low-dose gefitinib (250 mg/2-day) showed clinically equivalent efficacy to standard-dose gefitinib (250 mg/day) for NSCLC with sensitive EGFR mutations, but the dosing regimen has not yet been translated into clinical application due to lack of further support from PK/PD data [9]. Even more, in many countries, patients treated with gefitinib are covered by Medicare system, suggesting that gefitinib is widely prescribed. Therefore, it’s worth of thorough investigation consequently providing solid evidence for its rational use in clinic.
In this study, pharmacokinetic and metabolomic investigations were conducted in NSCLC patients with sensitive EGFR mutations (i.e., EGFR 19 exon del, 20 exon L858R) and the influence of gefitinib and its main metabolites on therapeutic effects were analyzed both in vivo and in vitro.
Materials and methods
Patients and study design
From November 2011 to September 2019, a total of 216 NSCLC patients in Sun Yat-Sen University cancer center (Guangzhou, China), were enrolled in this study. All enrolled patients were ≥18-year-old with adequate hematological, renal and hepatic functions, histologically or molecular-diagnosis confirmed NSCLC. All cases were pathologically confirmed stage IIIB/IV adenocarcinoma with Eastern Cooperative oncology group performance status of 0 or 1, which were carrying EGFR activating mutation and treated with 250 mg gefitinib daily. Patients with uncontrolled systemic disease, other tumors, poor compliance, interstitial lung disease, and receiving CYP3A4 or CYP3A5 inhibitors such as St John’s Wort, cimetidine were excluded from this study. The study was approved by the Ethical Committee of Sun Yat-Sen university cancer center. Written informed consent was obtained from all participating subjects.
Patients were treated with 250 mg gefitinib daily monotherapy until progression, intolerable adverse events or other reasons for withdrawal. A total of 3 mL peripheral blood with EDTA anticoagulation was collected before each subsequent treatment cycle. Upon completion of routine laboratory tests (hematology and biochemistry assessments), the samples were kept in −80 °C refrigerator until analysis.
Assessment
Response evaluation was performed by Computed Tomography or Magnetic Resonance Imaging scans according to the response evaluation criteria in solid tumors [RECIST1.1]. Objective responses (complete response or partial response) were confirmed 4 or more weeks after responses were first observed, stable disease [SD] was confirmed 4 weeks after responses were first observed. Central nervous system metastasis was recorded as progression disease (PD). The duration of progression free survival (PFS) is defined as the time from enrollment to objective disease progression, regardless of whether a patient was withdrawn from another cancer treatment prior to progression.
Chemicals and reagents
Gefitinib and M1 (O-Desmethyl Gefitinib, M537194) were purchased from Toronto Research Chemicals (Toronto, ON, Canada). M2 (M605211) was purchased from Nayuansu Biological Technology Co., Ltd (Shanghai, China). Vatalanib was provided by Selleck Chemicals (Pittsburgh, PA, USA). Acetonitrile, methanol, formic acid, ethyl acetate, tert-butyl methyl ether, and dichloromethane of high-performance liquid chromatography (HPLC) grade were produced by Tedia Company Inc (Fairfield, OH, USA). Other reagents were of HPLC grade or analytical purity grade meeting the experimental requirements. All the solvents for liquid chromatography and mass spectrometry were of the highest grade commercially available.
Targeted metabolomics of gefitinib and its metabolites in NSCLC patients
Three metabolites of gefitinib were identified by Targeted metabolomics. The identification and relative quantification of metabolites were completed by Thermo Scientific Q ExactiveTM benchtop Orbitrap high-resolution mass spectrometer (Thermo Scientific, San Jose, CA, USA) coupled with Thermo Scientific Dionex Ultimate 3000 UHPLC system. In brief, an aliquot (5 µL) was injected into a Thermo Scientific Q ExactiveTM benchtop Orbitrap high-resolution mass spectrometer (Thermo Scientific, San Jose, CA, USA) coupled with Thermo Scientific Dionex Ultimate 3000 UHPLC system after removing proteins and particulates. The metabolites were separated on a reverse-phase 100 × 2.1 mm Xterra MS 5 µm C18 column (Waters, Milford, MA, USA). MS data were acquired in the scan range of m/z 100–1500 and were processed using software version 2.2 (Thermo Scientific, San Jose, CA, USA).
Determination of gefitinib and its metabolites in NSCLC patients
Gefitinib and its metabolites were determined sensitively by using method with a TSQ Ultra triple-quadrupole mass spectrometer (Thermo Scientific, San Jose, CA, USA) [10]. Briefly, gefitinib and its metabolites were separated on a X-Terra RP18 column (50 mm × 2.1 mm, 3.5 μm) at 40 °C. An aliquot of 100 μL plasma was extracted with Tert butyl methyl ether and dried in a vacuum concentrator at room temperature. The resultant residues were dissolved with mobile phase and 10 μL was injected into the HPLC–MS/MS system for analysis.
Studies in cell lines
HCC827 cell line and PC9 cell line were used to assess the anti-tumor effect of M2 and gefitinib in vitro. The cancer cells were maintained with an RPMI-1640 medium containing 10% fetal bovine serum and 100 ng/mL penicillin and streptomycin at 37 °C in a humidified atmosphere with 5% CO2. Viable cells treated with different concentrations of M2 and gefitinib after 72 h were evaluated by using CCK8 Cell Kit.
Studies in mice
Four- to six-week-old KM male/female mice with an average body weight of 20 g were obtained from Laboratory Animal Center of Southern Medical University. Before experiment, all mice were subjected to 12-h light/dark cycle with normal diet and water in a week. All animal experiments were approved by the Animal Ethics Committee of Sun Yat‐Sen University (Guangzhou, China). The animal study was compliant with Laboratory animal–Guideline for ethical review of animal welfare (GBT 2035892-2018).
In this study, 90 mice were separated into 18 groups randomly with 5 mice in each time point. Gefitinib was dissolved on the experiment day by DMSO at concentration of 50 mg/mL, and resuspended in 1% polysorbate 80 solution in saline at final concentration of 5 mg/mL. In this study, 50 mg/kg of gefitinib and M2 were administered to each mouse, after which blood and brain were sampled at 0 min, 0.5 h, 1 h, 2 h, 4 h, 6 h, 8 h, 12 h, 24 h (n = 5 for each group). Animals were euthanized at the desired time point using a CO2 chamber. Blood was collected by extracting the eyeball, and the blood was transferred to heparinized tubes. Plasma was separated from whole blood by centrifugation at 3000 r/min for 10 min at 4 °C. All tissues were sampled immediately and stored at −80 °C until analysis by HPLC-MS/MS after flash-frozen in liquid nitrogen.
Statistical analysis
Centroid and integrated mass chromatographic data were processed by SIEVE 2.2 (Thermo Scientific, San Jose, CA, USA) software to generate a multivariate data matrix. The corresponding data matrices were then exported into SIMCA 13.0 software (Umetrics, Kinnelon, NJ, USA) for multivariate data analysis.
A log-rank test, stratified by concentrations of gefitinib, M1, and M2, was used to assess progression-free survival. The cutoff value was carried out by X-Tile [11]. We compared the differences in objective responses and these compounds concentrations with One Way ANOVA test. A Cox proportional hazards model, clarified compound concentrations, EGFR mutation status (19 exon del vs 21 exon L858R vs other mutant status), age (≥60 vs <60 years), sex (female vs male), and smoking history, was used to calculate hazard ratio (HR) and 95% confidence interval (CI). All statistical tests were carried out at two-sided a nominal 5% significance level, without adjustment for multiplicity.
All statistical analyses of the results were performed using R 3.6.0 and GraphPad 7.0 (San Diego, CA, USA). This study is ongoing and is registered with ClinicalTrials.gov, number NCT01994057.
Results
Clinical and pathologic features of NSCLC patients
In total, 216 patients were included in the final analysis. Seventy-six subjects belonged to the metabolomics/exploratory data set and 140 subjects belonged to the confirmatory data set. Patient characteristics were summarized in Table 1 and the comparison was made in two data sets by t test or Chi-test. There was no significant difference in patient baseline characteristics between the two analysis sets, which provided a reliable basis for subsequent analysis.
Gefitinib concentration was not correlated with clinical effects
As shown in Supplementary Fig. S1a and b, no statistical significance in PFS was found between patients with high gefitinib concentration and low gefitinib concentration in the exploratory data set (Cgefitinib range: 30.100–709.992 ng/mL) and confirmatory data set (Cgefitinib range: 32.178–816.453 ng/mL). Meanwhile, gefitinib exposure was unassociated with gefitinib-induced toxicities (data not shown).
The detection of metabolites (M1-M3) of gefitinib by targeted metabolomic and HPLC–MS/MS
According to known metabolites combined with Fisher function of software Mass Forinter, 3 metabolites (M1, M2, M3) of gefitinib were defined in 5 patients with NSCLC and metabolomic analysis revealed two clusters corresponding to the control and gefitinib group by the PCA and OPLS-DA (Fig. 1a and b), which indicated the chemical components were different between control and gefitinib groups and the patients’ metabolism in vivo was significantly changed by gefitinib. Major fragment ions (Fig. 1c) of gefitinib were identified by the standard solution (100 ng/mL). The potential structures of metabolites were shown in Fig. 1d. After the three metabolites were defined, the absolute quantification was also completed by HPLC–MS/MS. The distributions of gefitinib and M2 in plasma were shown in Supplementary Fig. S1c.

Metabolomic analysis revealed two clusters corresponding to the control and gefitinib groups by the PCA (a) and OPLS-DA (b); c The fragmentation of characteristic fragment ions of gefitinib; d The structures of gefitinib and its metabolites.
M2 has a potential antitumor effect
The IC50 of M2 was lower than that of the gefitinib in HCC827 and PC9 cell lines. The IC50 of M2 was 0.0046 μM and 0.030 μM in HCC827 and PC9 cell lines, respectively, and the value of gefitinib was 0.019 μM and 0.093 μM in the two cell lines, respectively (Fig. 2a and b). Remarkably, M2 showed a 4.0-fold greater inhibition of tumor activity than gefitinib in HCC827 cell line.

a PC9HCC827 cell line; b PC9 cell line; c the ratios of brain and plasma concentration of BBB permeability of gefitinib and M2; d AUC of BBB permeability of gefitinib and M2. BBB, brain blood barrier; *P < 0.05, **P<0.01, ***P < 0.0001.
M2 is more apt to cross the blood–brain barrier (BBB) than gefitinib
The mice treated with gefitinib or M2, we found that the ratio of Cbrain/Cplasma of each compound was statistically different (Fig. 2c and d), suggesting that M2 might be more apt to cross the BBB than gefitinib.
Relationship between concentrations of M1–M3 and PFS of NSCLC patients
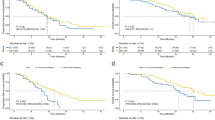
The Kaplan-Meier test was used to analyze the relationship between the concentration of three metabolites and the PFS in NSCLC patients. No significant difference was found between two groups with high and low plasma concentrations of gefitinib, M1, or M3 in median PFS (Supplementary Fig. S2a, b, d, Fig. 3a and c). The median PFS between CM2 < 12 ng/mL and CM2 ≥ 12 ng/mL (Supplementary Fig. S3a and b) were significantly different (16.2 vs. 26.8 months; P = 0.038) in exploratory data set (Fig. 3b and Supplementary Fig. S2c). Consistent conclusions were obtained in the validation set. The median PFS between CM2 < 12 ng/mL and CM2 ≥ 12 ng/mL (Fig. 3d) were 12.4 months and 19.8 months (P = 0.038), respectively. No significant difference was found in NSCLC patients between response rate (PR/SD/PD) with different plasma concentrations of gefitinib, M1, or M2 (Supplementary Fig. S4).

M1 was disassociated with PFS in exploratory data set (a) and validation set (c); M2 was correlated with PFS in exploratory data set (b) and validation set (d).
The relationship between M2 and efficacy was more obvious in NSCLC patients with brain metastases regarding to the results of Kaplan-Meier test. The median PFS between CM2 < 12 ng/mL and CM2 ≥ 12 ng/mL were 17.0 months (95% CI: 13.357–20.643) and 27.1 months (95% CI: 16.345–37.655) (P = 0.0092), respectively (Fig. 4c). No significant difference was found in NSCLC patients with brain metastases between two groups with different plasma concentrations of gefitinib or M1 in median PFS (Fig. 4a and b).

a gefitinib; b M1; c M2.
Cox regression analysis was applied to evaluate the impact of M2 concentration on therapeutic effects in NSCLC patients under the adjustment of cofactors including smoke status, EGFR mutation, gender, and age. The plasma concentration of M2 ≥ 12 ng/mL (P = 0.035, HR = 1.831, 95% CI: 1.027–3.263) was a strong predictor of the PFS of NSCLC patients. In confirmatory data set, the HR between CM2 < 12 ng/mL and CM2 ≥ 12 ng/mL was 1.643 (95% CI: 1.100–2.455) (Table 2). The same analysis was applied to NSCLC patients with brain metastases and the HR between CM2 < 12 ng/mL and CM2 ≥ 12 ng/mL was 2.762 (95% CI: 1.122–6.800) (Table 3).
Discussion
The present study showed that: first, the standard dosage (250 mg/day) is overdose for the patients with EGFR sensitive mutation, and should be decreased reasonably; second, M2, the mophiline metabolite of gefitinib, plays an important role in efficacy, which was verified in the validation set. Furthermore, M2 has more potential to penetrate BBB and may play a more important role in the treatment of brain metastases tumor than gefitinib.
As mentioned previously, the standard dosage (250 mg/day) was determined by IDEAL1 and IDEAL2 where most of the studied subjects do not carry the sensitive mutation of EGFR, and the results showed that patients on 250 mg/day did not have inferior therapeutic outcome and had less adverse effects than 500 mg/day [2, 12]. The present pharmacokinetic study showed that gefitinib plasma concentration is not correlated with efficacy, with the PFS of 19.4 vs 18.4 months between patients with high and low concentrations of gefitinib (P = 0.32). However, the concentration of M2, the main metabolite of gefitinib, is significantly correlated with efficacy, with the PFS of 16.2 months vs. 26.8 months between patients with high and low concentrations of M2 (P = 0.038). Consistent conclusions were obtained in the confirmative set. The median PFS between CM2 < 12 ng/mL and CM2 ≥ 12 ng/mL were 12.4 months and 19.8 months (P = 0.038), respectively. According to the concentration-effect curve, we proposed that the dosage of gefitinib is overdose for the greatest efficacy [13]. Even more, a clinical trial found that low-dose gefitinib (250 mg/2-day) showed clinically equivalent efficacy to standard-dose gefitinib (250 mg/day) for NSCLC with sensitive EGFR mutations [9]. Taken together, it is reasonable and feasible to decrease the standard dosage of gefitinib (250 mg/day) for patients with EGFR sensitive mutation.
Some investigations about the metabolism of gefitinib were conducted and some metabolites of gefitinib were identified, but most of those investigations were performed in vitro such as in microsomes of human, dog, and rat [14]. The present study is the first research on the metabolism of gefitinib in human plasma in NSCLC patients with EGFR sensitive mutations. In the present study, we employed a UHPLC-ESI-HRMS-based metabolomic approach to explore gefitinib metabolism and three metabolites (M1, M2, M3) were identified in the plasma of NSCLC patients. Our data showed that higher concentration of M2 lead to better response regarding to PFS, indicating that M2 plays an important role in efficacy. These metabolomic and pharmacokinetic studies found M2, the morpholine metabolite, plays an important role in the therapeutic effect of gefitinib, which was verified in a validation cohort. This result suggests that it be urgent and necessary to disclose the pharmacokinetic process of TKIs in the target patients.
Some studies showed that morpholine derivatives have strong antiproliferative activity and significantly inhibit the growth of lung cancer cells in a dose-dependent manner [15, 16]. In the present study, the IC50 of M2 in HCC827 and PC9 cell lines are 0.0046 and 0.030 μM, respectively, which are significantly lower than that of gefitinib (P < 0.0001 and P = 0.032, respectively). All these results indicated the further investigation about M2 is warranted.
Meanwhile, we found that M2 was significantly associated with gefitinib efficacy in patients with brain metastases. The brain metastases patients with higher concentrations of M2 showed better PFS, which suggested that M2 might be able to penetrate the BBB. We verified the hypothesis in an animal model study where the mice were administered M2 or gefitinib, the results suggested that M2 might be more apt to cross the BBB than gefitinib.
Brain metastases are the most common and severe complication of NSCLC due to lack of effective treatment. Patients with brain metastases usually have a low quality of life and poor prognosis [17, 18]. Commonly used therapies for brain metastases such as surgery or radiotherapy are associated with only modest benefits [19,20,21]. Historically, the treatment of brain metastases has been limited by concerns regarding limited penetration across the BBB [22, 23]. The data in our study showed that M2 has higher penetration across the BBB than gefitinib, indicating M2 be a promising candidate for developing anti-cancer drugs for patients with brain metastases.
This study has several limitations. First, it was a retrospective analysis, and the results could not be regarded as completely definitive, although the patients’ original charts were thoroughly reviewed and the correlation between this morpholine metabolite (M2) and PFS was verified in an independent patient group. Second, the study sample size was not large enough, although we believe that the results of the present study are useful because according to the prediction of G*power version 3.1.9.2 (Heinrich-Heine-Universität Düsseldorf), the sample numbers are sufficient to elucidate the question in our study. In addition, we have demonstrated that M2 has a greater ability to cross the BBB than gefitinib in animal studies, but the mechanisms have not been well explored. Because of these limitations, the data should be interpreted with caution and more validation of the results is needed.
In conclusion, for the patients with EGFR sensitive mutation, the standard dosage (250 mg/day) is in noticeable suspense and could be decreased reasonably. The present metabolomic and pharmacokinetic study found that M2, the morpholine metabolite of gefitinib, plays an important role in efficacy and has more potential to penetrate BBB and may be more effective in the treatment of metastatic tumor than gefitinib. More valuable research is warranted to investigate gefitinib and its morpholine metabolite.
References
Maemondo M, Inoue A, Kobayashi K, Sugawara S, Oizumi S, Isobe H, et al. Gefitinib or chemotherapy for non-small-cell lung cancer with mutated EGFR. N Engl J Med. 2010;362:2380–8.
Fukuoka M, Yano S, Giaccone G, Tamura T, Nakagawa K, Douillard JY, et al. Multi-institutional randomized phase II trial of gefitinib for previously treated patients with advanced non-small-cell lung cancer (The IDEAL 1 Trial). J Clin Oncol. 2003;21:2237–46.
Frantz S. Iressa failure raises fears about accelerated approvals. Nat Rev Drug Discov. 2005;4:94–95.
Cohen MH, Williams GA, Sridhara R, Chen G, Pazdur R. FDA drug approval summary: gefitinib (ZD1839) (Iressa) tablets. Oncologist. 2003;8:303–6.
Cortot AB, Jänne PA. Molecular mechanisms of resistance in epidermal growth factor receptor-mutant lung adenocarcinomas. Eur Respir Rev. 2014;23:356–66.
Yang Z, Hackshaw A, Feng Q, Fu X, Zhang Y, Mao C, et al. Comparison of gefitinib, erlotinib and afatinib in non-small cell lung cancer: a meta-analysis. Int J Cancer. 2017;140:2805–19.
Oxnard GR, Hu Y, Mileham KF, Husain H, Costa DB, Tracy P, et al. Assessment of resistance mechanisms and clinical implications in patients with EGFR T790M-positive lung cancer and acquired resistance to osimertinib. JAMA Oncol. 2018;4:1527–34.
Sharma J, Lv H, Gallo JM. Intratumoral modeling of gefitinib pharmacokinetics and pharmacodynamics in an orthotopic mouse model of glioblastoma. Cancer Res. 2013;73:5242–52.
Satoh H, Inoue A, Kobayashi K, Maemondo M, Oizumi S, Isobe H, et al. Low-dose gefitinib treatment for patients with advanced non-small cell lung cancer harboring sensitive epidermal growth factor receptor mutations. J Thorac Oncol. 2011;6:1413–7.
Guan S, Chen X, Wang F, Xin S, Feng W, Zhu X, et al. Development and validation of a sensitive LC-MS/MS method for determination of gefitinib and its major metabolites in human plasma and its application in non-small cell lung cancer patients. J Pharm Biomed Anal. 2019;172:364–71.
Camp RL, Dolled-Filhart M, Rimm DL. X-tile: a new bio-informatics tool for biomarker assessment and outcome-based cut-point optimization. Clin Cancer Res. 2004;10:7252–9.
Kris MG, Natale RB, Herbst RS, Lynch TJ, Prager D, Belani CP, et al. Efficacy of gefitinib, an inhibitor of the epidermal growth factor receptor tyrosine kinase, in symptomatic patients with non-small cell lung cancer—a randomized trial. J Am Med Assoc. 2003;290:2149–58.
Xin S, Zhao Y, Wang X, Huang Y, Zhang J, Guo Y, et al. The dissociation of gefitinib trough concentration and clinical outcome in NSCLC patients with EGFR sensitive mutations. Sci Rep. 2015;5:12675.
McKillop D, Hutchison M, Partridge EA, Bushby N, Cooper CM, Clarkson-Jones JA, et al. Metabolic disposition of gefitinib, an epidermal growth factor receptor tyrosine kinase inhibitor, in rat, dog and man. Xenobiotica. 2004;34:917–34.
Helwa AA, Gedawy EM, Taher AT, Ed El-Ansary AK, Abou-Seri SM. Synthesis and biological evaluation of novel pyrimidine-5-carbonitriles featuring morpholine moiety as antitumor agents. Future Med Chem. 2020;12:403–21.
Yan XQ, Wang ZC, Qi PF, Li G, Zhu HL. Design, synthesis and biological evaluation of 2-H pyrazole derivatives containing morpholine moieties as highly potent small molecule inhibitors of APC-Asef interaction. Eur J Med Chem. 2019;177:425–47.
Bui N, Woodward B, Johnson A, Husain H. Novel treatment strategies for brain metastases in non-small-cell lung cancer. Curr Treat Options Oncol. 2016;17:25.
Frega S, Bonanno L, Guarneri V, Conte P, Pasello G. Therapeutic perspectives for brain metastases in non-oncogene addicted non-small cell lung cancer (NSCLC): towards a less dismal future? Crit Rev Oncol Hematol. 2018;128:19–29.
Goldberg SB, Gettinger SN, Mahajan A, Chiang AC, Herbst RS, Sznol M, et al. Pembrolizumab for patients with melanoma or non-small-cell lung cancer and untreated brain metastases: early analysis of a non-randomised, open-label, phase 2 trial. Lancet Oncol. 2016;17:976–83.
Goldberg SB, Schalper KA, Gettinger SN, Mahajan A, Herbst RS, Chiang AC, et al. Pembrolizumab for management of patients with NSCLC and brain metastases: long-term results and biomarker analysis from a non-randomised, open-label, phase 2 trial. Lancet Oncol. 2020;21:655–63.
Khalifa J, Amini A, Popat S, Gaspar LE, Faivre-Finn C. Brain metastases from NSCLC: radiation therapy in the era of targeted therapies. J Thorac Oncol. 2016;11:1627–43.
Kim M, Laramy JK, Mohammad AS, Talele S, Fisher J, Sarkaria JN, et al. Brain distribution of a panel of epidermal growth factor receptor inhibitors using cassette dosing in wild-type and Abcb1/Abcg2-deficient mice. Drug Metab Dispos. 2019;47:393–404.
Zeng YD, Liao H, Qin T, Zhang L, Wei WD, Liang JZ, et al. Blood-brain barrier permeability of gefitinib in patients with brain metastases from non-small-cell lung cancer before and during whole-brain radiation therapy. Oncotarget 2015;6:8366–76.
Acknowledgements
This study was funded by the National Natural Science Foundation of China (Grant Nos. 81973398, 81473283, 81730103, 81573507, and 82020108031), The National Key Research and Development Program (Grant Nos. 2017YFC0909300 and 2016YFC0905000), Guangdong Provincial Key Laboratory of Construction Foundation (Grant No. 2017B030314030), Science and Technology Program of Guangzhou (201607020031), National Engineering and Technology Research Center for New Drug Druggability Evaluation (Seed Program of Guangdong Province, No. 2017B090903004), the 111 project (Grant: B16047), China Postdoctoral Science Foundation (Grant no. 2019M66324, 2020M683140, and 2020M683139). We thank the patients and their families. We thank the staff of Sun Yat-sen University Cancer Center.
Author information
Authors and Affiliations
Contributions
WF, XC, SXG, MH, XDW, LZ designed the study. SXG, HLR, YH and XDW performed the study and wrote the manuscript. HZZ, WFF, WZ, SX, YG, YHC, YPY, HYZ and FW participated in data analysis. All authors contributed to the article and approved the submitted version.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Supplementary information
Rights and permissions
About this article

Cite this article
Feng, W., Chen, X., Guan, Sx. et al. Rational application of gefitinib in NSCLC patients with sensitive EGFR mutations based on pharmacokinetics and metabolomics. Acta Pharmacol Sin 43, 1857–1864 (2022). https://doi.org/10.1038/s41401-021-00791-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41401-021-00791-5
