
Abstract
Background and importance
Congenital dermal sinus tract (DST) is a rare spinal dysraphism characterized by a persistent tract lined by epithelial cells, beginning at the epidermis and terminating in deeper tissue layers. With 1% of all congenital DST cases found in the cervical region, only 4% of all cases are diagnosed after the age of 20.
Clinical presentation
In this case, a 65-year-old woman with a congenital DST at the cervical level presented with symptoms of neck and some arm pain, suboccipital headaches, and unique external characteristics. Neck Disability Index and visual analog scale were used to assess the patient’s preoperative and postoperative pain, and quality of life. Patient underwent an operative intervention, where the DST was surgically removed followed by interlaminar decompression at C1–C2, excision of the epidural component, and biopsy followed by plastic surgical repair. Pathology analysis indicated a squamous epithelial-lined sinus tract interacting with the dura. Most notably, a meningothelial proliferation with associated psammomatous calcifications was identified, similar to a meningioma.
Conclusion
A review of literature was conducted to further discuss clinical and radiological presentation as well as to document the novel appearance of this congenital DST. As one of the oldest cases of DST, it demonstrated unusual pathological characteristics with a meningothelial proliferation, compatible with meningioma, reported at the epidural level.
Similar content being viewed by others

Background and importance
Congenital dermal sinus tract (DST) is a rare spinal dysraphism characterized by a persistent tract lined by epithelial cells, beginning at the epidermis and terminating in deeper tissue layers [1]. With an incidence rate of 1 case per 2500 live births, congenital DST is found in the cervical region in around 1% of all cases [2, 3]. In 2020, Petrov reported a clinical case of a 58-year-old as one of the oldest patients with congenital DST in the cervical region [2]. Adding to the current literature, we would like to report a 65-year-old woman with congenital DST at the C1–C2 level who presented with symptoms and pathological findings unusual for this entity.
Clinical presentation
A 65-year-old female presented to the clinic with complaints of chronic suboccipital headaches consistent with occipital neuralgia. The patient’s chief complaints were a pain in the neck and head and tingling on the left side of the body, including the scalp, arm, leg, and lip. Patient has a family history of headache disorders, but no history of spinal problems. To alleviate the pain, the patient regularly took tramadol and even steroids. Patient mentioned that she was born with a “hole” in her neck, the persistent DST in the posterior cervical area, which gave her significant personal discomfort in its appearance as shown in Fig. 1.

The DST presented as hypopigmented, no signs of infection, and contracted external sphincter-like outer boundary with hypotrichosis.
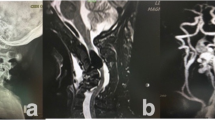
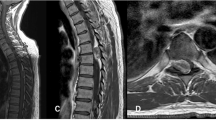
Preoperatively, the patient reported a Neck Disability Index Score (NDI) of 46, and visual analog scale (VAS) neck 9.8. Neurological examination indicated the range of motion as stiff but relatively intact, motorically intact at 5/5, normal sensory, gait, and reflexes. The patient’s congenital DST was unique in its physical appearance as it was a hypopigmented, contracted external sphincter-like outer boundary with hypotrichosis, and no signs of infection. She denied any pain in that area or drainage from the opening. Contrary to a typical case of congenital DST, there was an absence of associated neurological dysfunction, swelling, infection in the area, or associated hemangioma. The cervical MRI shows C1 bifid arch traversed by the congenital DST as shown in Fig. 2. Initial impression indicates that the cervical osteoarthritis O–C1 on the left side is the likely cause of her neck pain and the suboccipital headaches could be associated with the DST, to be explored in the biopsy.

The C1 bifid arch is traversed by the congenital dermal sinus tract.
The surgical intervention was an excision of the posterior cervical pathologic lesion that extends from the skin to the spine along with a plastic surgical repair. A circular posterior cervical incision around the DST was made, and the dissection was taken down along the tract past the cervicodorsal fascia. An excision of the congenital sinus tract and associated fistula tissues along with interlaminar decompression of C1 and top of C2 with epidural micro-dissection and excision was performed. The sinus tract was followed all the way to the C1 arch and the C1–C2 interlaminar space via a minimalistic coned-down dissection under microscopic magnification (Fig. 3). During the operation, the tract ended with a thin layer of dense tissue adherent to the dura mater. Subsequently, thinning of the C1 lamina and the top of C2 with a high-speed drill, revealed the terminal epidural tissue in the interlaminar space extending down from the bifid arch of C1. The specimen was removed off the dura mater after the laminotomy, and sent for pathologic analysis. There was no evidence of intradural extension or tethered cord. The true length of the sinus tract was measured to be 7.5 cm (Fig. 4). With the help of the plastic surgical team, a Z flap was rotated with fascial closure with vicryl in layers and primary closure was obtained with excellent cosmesis (Fig. 5). Pathological examination revealed an epithelial-lined sinus tract that extended into the epidural space with meningothelial proliferation and was interpreted as a classic (typical) meningioma.

Under high microscopic magnification the DST is visualized along its tract all the way to the epidural space and at the very center the C1 lamina is reached and the area of decompression is visualized.

Sinus tract length is measured to be 7.5 cm, including the redundant epidermis: the abnormality was submitted for pathological examination upon excision and this was a result of the gross total resection.

Results demonstrated achieved by z-flap plastic surgical closure attained effective cosmesis.
At 3 months postoperatively, the patient was extremely satisfied and indicated resolution of her arm symptoms, C2 neuralgia, suboccipital headaches, and tingling on the left side of the body. The patient reported an NDI of 14 and VAS score of 0.1 (neck). Neurological exam remained stable. Five-month postoperative MRI indicates minimal dorsal nodularity without enhancement in Fig. 6.

Indicating gross total resection.
Discussion
Congenital DSTs are hypothesized to be the embryological result of an incomplete separation between the neural ectoderm and cutaneous surface ectoderm during the 3rd and 8th week of gestation [2]. Less than 1% of all congenital DST cases are found in the cervical region, where only 4% of the cases are diagnosed after the age of 20 [2]. The major clinical presentations and symptoms of congenital DST are hypertrichosis, abnormal pigmentation, infections, neurological deficits, skin dimples, erythema, hemangiomas, drainage of debris from the pit, tethered cords, inclusion tumors, and subcutaneous lipomas [2, 4,5,6,7]. Neurological deficits include motor weakness, sensory and reflex changes, and gait abnormalities [5, 8].
Our case demonstrates unique appearance, and pathology including squamous epithelial-lined sinus tract that extended from the epidermis, through the dermis, into epidural space. Meningothelial proliferation was found along with psammomatous calcifications (Figs. 7 and 8). The meningothelial proliferation was interpreted as a classic (typical) meningioma, fibroblastic type, WHO grade I. A meningothelial hamartoma was considered, but not favored as that entity is traditionally restricted to the dermis and subcutaneous tissue, often involves the scalp, and is not contiguous with the dura [9]. The area of meningioma was free of the cauterized dural margin, and completely excised. Contrary to the current literature on congenital DST, this patient presented as one of the oldest cases to be reported, uniquely with no previous infections and meningothelial proliferation. There was no intradural component or tethered cord [10].

Demonstrates Meningothelial cell proliferation embedded within a collagenous stroma with single psammomatous calcification in the upper left corner.

High power image of meningothelial cell proliferation in a collagenous stroma, with immunohistochemical stain for SSTR2—a meningothelial marker—depicted in the lower right inset.
Conclusion
Diagnosed typically at birth or in early childhood, congenital DSTs are usually located in the lumbosacral region and rarely in the cervical region. Early diagnosis and treatment of congenital DST are important to prevent neurological deficits, infection and pain. To our knowledge, no previous reports of this type of DST with these unique external characteristics, spinal dysraphism with epidural meningioma, have ever been reported.
Timeline

Data availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
References
Karatas Y, Ustun ME. Congenital cervical dermal sinus tract caused tethered cord syndrome in an adult: a case report. Spinal Cord Ser Cases. 2015;1:15021.
Petrov M, Gerganov V, Gabrovsky N, Kamenova M. Congenital dermal sinus tract localized in the cervical region in an adult patient–clinical case. Review of the literature. Interdiscip Neurosurg. 2020;21:100683.
Manfredi M, Donati E, Magni E, Salih S, Orlandini A, Beltramello A. Spinal dysraphism in an elderly patient. Neurol Sci. 2001;22:405–7. https://doi.org/10.1007/s100720100074.
Ackerman LL, Menezes AH, Follett KA. Cervical and thoracic dermal sinus tracts. A case series and review of the literature. Pediatr Neurosurg. 2002;37:137–47.
Ackerman LL, Menezes AH. Spinal congenital dermal sinuses: a 30-year experience. Pediatrics. 2003;112:641–7.
Nishimura Y, Hara M, Natsume A, Wakabayashi T, Ginsberg HJ. Complete resection and untethering of the cervical and thoracic spinal dermal sinus tracts in adult patients. Nagoya J Med Sci. 2020;82:567.
Mishra SS, Panigrahi S. Thoracic congenital dermal sinus associated with intramedullary spinal dermoid cyst. J Pediatr Neurosci. 2014;9:30–2. https://doi.org/10.4103/1817-1745.131478.
Elton S, Oakes WJ. Dermal sinus tracts of the spine. Neurosurg Focus. 2001;10:1–4.
Mete M, Umur AS, Duransoy YK, Barutçuoğlu M, Umur N, Gurgen SG, et al. Congenital dermal sinus tract of the spine: experience of 16 patients. J Child Neurol. 2014;29:1277–82.
Qasho R, Lunardi P, Lo Bianco FM, di Stefano M. Rare combination of spinal lesions and subcutaneous meningioma in a 44 year old man. J Neurooncol. 1998;38:77–82.
Author information
Authors and Affiliations
Contributions
SH and AV conceived the presentation of the case study for publication. AV performed initial neurosurgical consultation, neurosurgical operation, and postoperative neurosurgical evaluation of the patient. TG performed plastic and reconstructive surgery on the patient. SK performed the pathological examination of body tissue. SH performed the literature review for the paper. SH and AV performed writing the initial draft preparation. JP and AV performed writing revisions and edits for the final submission.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Consent for publication
The patient was consented prior to surgery via a consent to medical or surgical care and treatment form that notes that their records may be used for educational research. The patient was ensured anonymity and is aware that they can withdraw consent at any time before online publication.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Vokshoor, A., Jajj, H., Grunwald, T. et al. Posterior cervical congenital dermal sinus tract: case report and review of literature. Spinal Cord Ser Cases 9, 40 (2023). https://doi.org/10.1038/s41394-023-00575-5
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41394-023-00575-5
