
Abstract
Study design
Retrospective cohort study.
Objectives
To study the incidence of concomitant calcaneum fractures in participants with traumatic spine fractures and to study the association of calcaneum injury with the mode of trauma, morphology and level of vertebral fracture and neurological status in participants with concomitant spine and calcaneum fracture.
Setting
Central Institute of Orthopaedics, Safdarjung Hospital, New Delhi, India.
Methods
Records of participants with traumatic spine fractures were analyzed. Participants who had calcaneum fracture confirmed on radiographs were considered to have concomitant spine and calcaneum fracture. In these participants, variables noted were age, gender, mode of trauma, level and morphology of vertebral fracture and neurological status.
Results
Concomitant calcaneum fracture was present in 43 participants out of a total of 358. The lumbar spine was involved in 72.09% of participants. 46.51% of participants had complete burst type of vertebral fractures. Neurology was found to be intact in 58.13% of participants. The association of concomitant calcaneum injury with the level of spine fracture and type of fracture were found to be statistically significant (p < 0.05). In particular, the association of concomitant calcaneal fracture with intact neurology and incomplete paraplegia (ASIA B, C or D) as compared to spinal injury cases without calcaneal fractures was statistically significant (p < 0.001).
Conclusion
Calcaneum fractures co-exist with spine fractures in 12.01% participants. Concomitant calcaneal fracture(s) with spine trauma indicate a greater chance of incomplete injury or intact neurology possibly due to dispersion of force vectors.
Similar content being viewed by others

Introduction
Traumatic spinal fractures are common injuries that can result in significant disability, deformity and neurological deficit [1]. Major causes of these injuries include motor vehicle accidents, fall from height and direct violence. Since these injuries are high velocity in nature, association with life-threatening injuries like head injury, thoracoabdominal injuries, pelvic injuries and long bone fractures is common. Spine fractures are found to have an association with calcaneum fractures.
Various studies have cited that spine fractures and calcaneum fractures co-exist in ~10 percent of participants [2, 3]. Walters JL et al. [4] undertook a retrospective cohort study that included 208 consecutive participants with data recorded in a radiographic database to determine the incidence of concomitant vertebral fracture in association with fracture of the calcaneus. A total of 15 calcaneal fractures (7.21%) were associated with concomitant vertebral fracture, and the lumbar spine was involved in 12 (80%) of these cases. Bohl et al. [5] in one of the largest series studied the association of calcaneum fractures with other injuries in 14,516 participants. They observed that concurrent spine fractures occurred in 23% of participants, of which the most common were lumbar spine fractures. In 1962, Lance et al. [6] described 205 fractures of the calcaneum in which they observed that 21 participants had concomitant spinal fractures (10.24%) and 19 of these cases had an injury in the lumbar spine. Erturar E et al. [7] evaluated vertebral fractures and associated injuries in adults, in the year 2005. They found associated injuries in 29.6% of participants, the most common being calcaneum fractures in 9.4% of participants.
In our study, we aimed to determine the incidence of calcaneum injury in participants with spine fractures, to study the association of calcaneum injury with the mode of trauma, the morphology of vertebral fracture, level of vertebra involvement and neurological status in participants with concomitant spine and calcaneum fractures.
Methods
This retrospective cohort study was conducted at our hospital from June 2018 to June 2020. Participants’ medical records were obtained from the hospital database. All participants with traumatic spine fracture, including sacral fracture, who were admitted to the central institute of orthopaedics were included in this study. Participants with osteoporotic and pathological fractures were excluded from the study. Participants’ clinical records, plain radiographs, CT scans and MRI scans were analyzed. The participants who had calcaneum fracture confirmed on radiographs were considered to have concomitant fractures of the spine and calcaneum. In these participants, the variables noted were age, gender, mode of trauma, level of vertebral fracture, the morphology of vertebral fracture and neurological status. Spinal fracture classification was done according to AO-Classification of spinal fractures and thoracolumbar injury classification system (TLICS) [8,9,10]. The neurology of the participants was recorded as per American Spinal Injury Association (ASIA) score [11]. Denis classification was used for sacral fractures. Participants were managed operatively or nonoperatively as per AO guidelines. All participants were referred to the physical medicine and rehabilitation department at the time of discharge from the orthopaedic-spine unit.
The data entry was done in the Microsoft EXCEL spreadsheet and the final analysis was done with the use of Statistical Package for Social Sciences (SPSS) software version 21.0. For statistical significance, a p < 0.05 was considered significant. The presentation of the Categorical variables was done in the form of numbers and percentages (%). The continuous data were checked for normality by using the Kolmogorov–Smirnov test. The presentation of the continuous variables was done as median (interquartile range). The Chi-square test was used for group comparisons of categorical data. In cases where the expected frequency in the contingency table was less than 5 for more than 20% cells, Fisher’s exact test was used instead. The association of the age was analyzed using Mann–Whitney Test. Accordingly, the association of neurology was analyzed using the Chi-Square test and the mode of trauma, the morphology of vertebral fracture, level of vertebral fracture was analyzed using Fisher’s Exact test.
Results
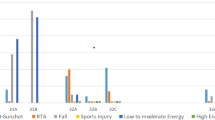
Total records of 358 participants with traumatic spine fractures were retrieved. There were 43 participants who had concomitant calcaneum fracture. The median age of presentation in participants with concomitant spinal and calcaneal fractures was 26 years (range 21.5–33 years) and in participants without calcaneum fracture was 33 years (range 28–45 years). Twenty-two (51.16%) of the participants with calcaneum injury were male participants. The gender distribution was non-significant when compared with participants without concomitant calcaneum fracture (p = 0.2949). In participants where there was no concomitant calcaneum fracture, road traffic accidents were the most common mode of trauma (55.24%) whereas fall from height was the mode of trauma in 86.04% of participants with concomitant calcaneal injury (p < 0.001). In participants with concomitant fractures, the lumbar spine was seen to be involved in the largest proportion of participants, that is in 72.09 % cases, whereas in others, the most common level of vertebral involvement was thoracic (42.85%). The most common level of lumbar spine involvement was L1 in 15 participants. Isolated fracture of L2, L3 and L5 was present in 6, 5 and 2 participants, respectively. One participant had combined L3 and L5 fracture and 2 participants had both L1 and L4 involvement. Neurology was intact in 58.13% of participants with concomitant spine and calcaneum fractures, 30.23% of participants had incomplete paraplegia (ASIA B, C or D) and 11.63% had complete paraplegia (ASIA A). On the other hand, in participants who did not have associated calcaneum injury, only 27.62% had intact neurology. The association of concomitant calcaneal fracture with intact neurology or incomplete paraplegia (ASIA B, C or D) as compared to spinal injury cases without calcaneal fractures was statistically significant (p < 0.001).
The most common morphology of spine fracture in cases of concomitant injury was burst fracture. 46.51% of participants with calcaneal fractures participants had complete burst fracture (AO A4) in comparison to 35% in other participants without concomitant calcaneal fractures and the association was found to be statistically significant (p < 0.05). In our study, a statistically significant association was found between sacral and calcaneum fractures. Out of total 18 cases of sacrum fractures, 10 had concomitant calcaneum fracture sacrum was seen to be the second most prevalent level of spinal involvement (20.93%) in such participants.
Table 1 summarizes the prevalence of variables in spine injury cases with concomitant calcaneum fractures (n = 43) and those without calcaneal fractures (n = 315).
Discussion
Spinal fractures are known to co-exist with calcaneum fractures. Most studies that have reported concomitance of spinal and calcaneum fractures have studied the incidence of spine injuries in participants of calcaneum injuries and not vice versa. Our study of concomitant spinal and calcaneum fractures has one of the largest datasets evaluated to date. Our research not only studies the incidence and association of spinal fractures with calcaneum fractures but also other parameters that may possibly have an association such as mode of trauma, neurology of the participant, level of the vertebra involved and morphology of the fractured vertebra.
The incidence of concomitant spinal and calcaneum fracture in our study was found to be 12.01% which correlates well with the incidence figures that have been traditionally reported [2, 3]. In cases of concomitant calcaneal and vertebral fractures, the most prevalent level of spinal involvement was the lumbar spine (72.09% of cases).
The majority of records indicate that spine injury cases with concomitant calcaneal fractures had burst type of vertebral fractures. This may be due to the fact that the most common mode of trauma in participants with concomitant calcaneum injury was fall from height thus causing burst fractures. Neurology was intact in 58.13% of participants with concomitant fractures in comparison to participants without concomitant injuries in which neurology was found to be intact in 27.62% of participants. This difference was statistically significant (p < 0.001). Saboe LA et al. [12] conducted a study on 508 spine trauma participants and concluded that the participants of spine injuries who have other associated injuries were less likely to have a neural deficit. This may be due to possible landing of the person on foot during fall and dissipation of energy at the calcaneus, and hence lesser impact and retropulsion at vertebral level.
Our study presents one of the largest dataset evaluated to date on concomitant calcaneum and spinal fractures. The main limitation of this retrospective study is the non-uniformity of data recording. Also, there are chances that calcaneum fracture may have been missed in a few cases.
We conclude that calcaneum fractures co-exist with spine fractures in around 12% of participants of spinal trauma. The lumbar spine is the most commonly involved in cases of concomitant injuries and most of these participants have no neural deficit. A strong suspicion of calcaneum injury is warranted in cases of spinal fractures, especially if the mode of trauma is fall from height. Knowledge about such association is even more important in cases with spinal injury and neurological deficit as they may lack the ability to complain of pain in the foot and ankle region. The presence of concomitant calcaneal fracture(s) is an indication of a greater chance of incomplete injury or intact neurology and this could indicate that the dynamics of the fall are such that the fracture may lead to a dispersion of force vectors at the calcaneus and that may lead to a less extensive spinal injury. In patients with concomitant spine and calcaneum injury due to fall, sacrum fracture should be looked for with a high degree of suspicion as sometimes these fractures can be missed on plain radiograph. A well-planned prospective study can help in better understanding of this association as that can ensure better evaluation of participants at the time of presentation.
Data archiving
All data generated or analysed during this study are included in this published article [and its Supplementary Information files].
References
Rajasekaran S, Kanna RM, Shetty AP. Management of thoracolumbar spine trauma: an overview. Indian J Orthop. 2015;49:72–82.
Rowe CR, Sakellarides H, Freeman P. Fractures of os calcis: a long-term follow-up study of one hundred forty-six participants. JAMA. 1963;184:920–3.
Mitchel MJ, McKinely JC, Robinson CM. The epidemiology of calcaneal fractures. Foot. 1994;19:197–200.
Walters JL, Gangopadhyay P, Malay DS. Association of calcaneal and spinal fractures. J Foot Ankle Surg. 2014;53:279–81.
Bohl DD, Ondeck NT, Samuel AM, Diaz-Collado PJ, Nelson SJ, Basques BA, et al. Demographics, mechanisms of injury, and concurrent injuries associated with calcaneus fractures: a study of 14,516 participants in the American College of Surgeons National Trauma Data Bank. Foot Ankle Spec. 2017;10:402–10.
Lance E, Wade EC. Factures of the os calcis: a follow-up study. Proceedings of the 22nd Annual Session of the American Association for the Surgery of Trauma, Hot Springs, VA, October 29–31, 1962.
Ertürer E, Tezer M, Oztürk I, Kuzgun U. Evaluation of vertebral fractures and associated injuries in adults. Acta Orthop Traumatol Turc. 2005;39:387–90.
Vaccaro AR, Oner C, Kepler CK, Dvorak M, Schnake K, Bellabarba C, et al. AO Spine thoracolumbar spine injury classification system: fracture description, neurological status, and key modifiers. Spine (Philos Pa 1976). 2013;38:2028–37.
Vaccaro AR, Koerner JD, Radcliff KE, Oner FC, Reinhold M, Schnake KJ, et al. AOSpine subaxial cervical spine injury classification system. Eur Spine J. 2016;25:2173–84.
Vaccaro AR, Lehman RA Jr, Hurlbert RJ, Anderson PA, Harris M, Hedlund R, et al. A new classification of thoracolumbar injuries: the importance of injury morphology, the integrity of the posterior ligamentous complex, and neurologic status. Spine (Philos Pa 1976). 2005;30:2325–33.
Maynard FM Jr, Bracken MB, Creasey G, Ditunno JF Jr, Donovan WH, Ducker TB, et al. International standards for neurological and functional classification of spinal cord injury. American Spinal Injury Association. Spinal Cord. 1997;35:266–74.
Saboe LA, Reid DC, Davis LA, Warren SA, Grace MG. Spine trauma and associated injuries. J Trauma. 1991;31:43–8.
Author information
Authors and Affiliations
Contributions
TB conceptualized the study and was involved in the overall manuscript planning and supervision. AS and RS gave valuable insights. SK was mainly involved in data collection, manuscript writing, submission, and revision as the corresponding author. VC was involved in data collection and manuscript writing. MKP provided valuable interpretations regarding the data analysis and meaning of the results, and participated in responding to reviewers and revising the manuscript. RK was involved in overall supervision of the study, manuscript writing, and provided valuable critical insights. All authors had approved the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Boruah, T., Sareen, A., Sreenivasan, R. et al. Concomitant spine and calcaneum fractures: a possible indication of less extensive injury. Spinal Cord Ser Cases 8, 1 (2022). https://doi.org/10.1038/s41394-021-00473-8
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41394-021-00473-8
