
Abstract
Study design
Triangulated mixed-methods validation study.
Objectives
To validate the Danish version of the Spinal Cord Lesion-related Coping Strategies Questionnaire (SCL-CSQ).
Setting
Community in Denmark.
Methods
Participants were invited via a patient organization and its specialized hospital. Eligibility criteria were having a spinal cord injury (SCI), being 18 years or older, and able to understand and respond in Danish. Quantitative data were collected to determine internal consistency and criterion validity of the three subscales of SCL-CSQ, i.e., acceptance, fighting spirit, and social reliance. The Three-Step Test-Interview approach was employed to determine whether items measured what they were intended to measure (i.e., construct validity based on response processes).
Results
The quantitative sample consisted of 107 participants, and the interview sample comprised 11 participants. The acceptance and fighting spirit subscales showed adequate internal consistency (Cronbach’s alpha of 0.72 and 0.76 respectively) and satisfactory criterion validity (expected correlations with quality of life and depression). The social reliance subscale showed inadequate internal consistency (Cronbach’s alpha of 0.58) and criterion validity. All fighting spirit items and all but one acceptance items were interpreted congruently by most participants. Conversely, two social reliance items were only interpreted congruently by 9 and 27%.
Conclusion
The acceptance and fighting spirit subscales of the Danish version of the SCL-CSQ showed good psychometric properties, while the social reliance subscale showed serious issues and should be revised. Researchers and clinicians are urged to reflect on these findings when revising the SCL-CSQ or adapting it to other languages, cultural contexts, and rehabilitation settings.
Similar content being viewed by others


Introduction
Spinal cord injury (SCI) is an overwhelming condition often accompanied by paralysis, chronic pain, bowel and bladder issues, and psychological morbidities [1, 2]. Despite the myriad of physical implications, injury characteristics are generally poor predictors of psychological adjustment [3]. Instead, research has focused on how coping strategies affect adjustment outcomes like quality of life (QoL), mental health, and social participation [1, 4, 5]. This research is mostly based on self-reported questionnaire data, and one of the widely used scales is the Spinal Cord Lesion-related Coping Strategies Questionnaire (SCL-CSQ). The SCL-CSQ was developed based on content analysis of interviews with individuals with disabilities, including three with SCI [6]. An initial pool of 42 statements reflecting different coping strategies was reduced to 12 items using factor analysis. These were divided into three subscales based on multi-trait analysis: Acceptance, fighting spirit, and social reliance [6]. Individuals who use acceptance try to cope with the SCI by accepting the new circumstances as a part of life and revising their values and interests accordingly [7]. In essence, they are making changes within themselves to create a better fit with their life circumstances. Conversely, individuals who use fighting spirit try to take control over their life circumstances by fighting to achieve their goals, acting independently in life, and finding ways to make life easier and getting the most out of it [7]. Individuals who use social reliance have become passive in engaging with the stressors of life and feel psychologically and socially dependent on others for help and support [7]. Generally, greater acceptance and fighting spirit are related with favorable adjustment outcomes, while social reliance is negatively related with adjustment outcomes [7,8,9]. The initial validation of the SCL-CSQ showed adequate internal consistency within all subscales (i.e., Cronbach’s alpha for acceptance = 0.79, fighting spirit = 0.72, and social reliance = 0.73), item-internal validity (i.e., correlations between items and hypothesized scale were all above 0.4), and item-discriminant validity (all items correlated higher with its own scale than with competing scales) [6]. The SCL-CSQ has been adapted to and validated in a range of cultural settings including Sweden [9], United Kingdom, Germany, Austria and Switzerland [7], Turkey [10], Spain [11], and Iran [12]. However, a Danish version has not yet been developed and validated. Furthermore, to the best of our knowledge, no studies have investigated whether respondents understand and interpret the items correctly. Indeed, some translated items of the first English and German fighting spirit and social reliance subscales have been revised [7], and it has also been difficult to reproduce the social reliance subscale in the Turkish translation [10]. Investigating whether items are interpreted correctly is thus an important part of determining construct validity [13]. According to the Standards for Educational and Psychological Testing, this is categorized as validity evidence based on the response processes [14]. This source of evidence is concerned with the fit between the construct and how the items are actually understood and interpreted by respondents [14].
The aim of this study was thus to translate and validate a Danish version of the SCL-CSQ in a triangulated mixed-methods design using survey data to determine internal consistency and criterion validity, and interview data to determine construct validity based on response processes. Based on prior validation of the SCL-CSQ [6, 11], all subscales were hypothesized to show acceptable internal consistency (Cronbach’s alpha ≥ 0.70). Further, weak to moderate positive correlations were hypothesized between acceptance and QoL; fighting spirit and QoL; and social reliance and depression. Weak to moderate negative correlations were hypothesized between acceptance and depression; fighting spirit and depression; and social reliance and QoL.
Methods
Participants and procedure
Participants were recruited through the patient organization Accident Victims Denmark and its Specialized Hospital for Polio and Accident Victims. These two organizations include individuals with SCI, but also many members and patients who were not our target population (e.g., relatives, other patient groups). Information about the study, including a link to the questionnaires and an email address for one of the authors (AA), was distributed via flyers at the hospital and in the newsletter and social media pages of Accident Victims Denmark. To participate in the survey, individuals simply had to copy the link into their browser, while people interested in the interview had to contact AA via the listed email. Following completion of the survey, participants could also give their permission to be contacted if they were interested in participating in the interviews. AA contacted people on this list to provide more information about the study and, if still interested, arranged a date for the interview.
In both the survey and the interviews, eligibility criteria were having an SCI, being 18 years of age or older, and being able to understand and respond to questions in Danish. This was clearly described in the study information prior to filling out the questionnaires, and participants were also required to confirm that they had an SCI before responding.
Quantitative data were collected via an online survey to determine internal consistency and criterion validity of the SCL-CSQ. The online survey consisted of the SCL-CSQ [7], the Patient Health Questionnaire (PHQ-9) [15], and the International Spinal Cord Injury Quality of Life Basic Data Set (SCI-QOL) [16]. Data were collected from November 2019 to August 2020.
To determine the construct validity based on response processes, the Three-Step Test Interview (TSTI) approach was used [17]. TSTI is a systematic approach to explore whether questionnaire items measure what they are intended to measure [17]. According to protocol, the interviews consisted of three phases [17]. In the first phase, respondents were asked to respond to the items while thinking aloud. The aim was to collect primary data about how the items are responded to (e.g., introspective reasoning, skipping questions, hesitation). Observations of for example hesitancy was based on clinical impressions of utterances, tone of voice, body language, and facial expressions. In the second phase, the interviewer asked probing questions to fill in potential gaps in the primary data (e.g., “I noticed that you seemed to hesitate with this question. Is that correct, and can you tell me what you were thinking?”). The last phase was debriefing. Here, respondents were asked to explain the reasoning behind their responses, what they understood by specific words or phrases, give examples from their own life, and elaborate on their experiences and opinions of each item. All interviews were conducted by author AA and were audio recorded and transcribed verbatim. Data were collected from August 2019 to October 2020.
Measurement scales
Spinal Cord Lesion-related Coping Strategies Questionnaire
The SCL-CSQ is a self-reported scale with 12 items in total measuring three coping strategies: Acceptance (four items), fighting spirit (five items), and social reliance (three items) [7]. Acceptance is defined as perceiving the injury and its consequences as an integrated part of life and finding new values and interests to replace those that are no longer attainable. Fighting spirit is defined as trying to make the most out of life by acting independently, setting goals to achieve, and finding ways to make life easier. Lastly, social reliance is defined as psychologically dependent behavior where an individual feels helpless without help and support from others. Please see Supplementary Information Appendix 1 for an overview of all 12 items in both English and Danish. It is scored on a four-point Likert-scale ranging from “completely disagree” to “completely agree”.
Patient Health Questionnaire
The PHQ-9 is a self-reported measure of depression severity with nine items corresponding to the DSM-IV criteria for depression [15]. Respondents are asked to consider symptoms within the previous 2 weeks and score each item on a four-point scale ranging from 0 (“not at all”) to 3 (“nearly every day”). The PHQ-9 has been shown to be a valid tool for measuring depression severity in both medical settings [15] and the general population [18]. It has also shown good psychometric properties, including internal consistency (Cronbach’s alphas between 0.86 and 0.89) and test-retest reliability [15]. The PHQ-9 was originally developed and validated in the United States [15], but has since been adapted to and validated in a range of cultural settings [18,19,20,21]. It has also been translated into Danish and validated using Item Response Theory, which showed unidimensionality and good reliability [22].
International Spinal Cord Injury Quality of Life Basic Data Set
The SCI-QOL is a self-reported questionnaire that consists of three items measuring satisfaction with physical health, psychological health, and life as a whole within the past 4 weeks [23]. Each item of the SCI-QOL is scored on an 11-point numeric rating scale ranging from 0 (“completely dissatisfied”) to 10 (“completely satisfied”). Initial validation procedures showed moderate to strong inter-correlations and good convergent validity between each item and their respective reference measure (i.e., selected items from the abbreviated World Health Organization Quality of Life measure and from the Mental Health Inventory-5) [23].
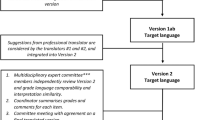
Translation procedure
The SCL-CSQ and SCI-QOL were translated from English to Danish using a back-translation procedure. First, two authors (AA and TEA) translated each item from English to Danish. Next, discrepancies were discussed, and a third author (SLR) was consulted when necessary. After consensus was reached, a native English-speaking person translated back to English. Three authors (AA, TEA, and SLR) discussed any discrepancies between the back-translated English version and the original English version, and minor adjustments were made when necessary. Finally, the translated version was reviewed and approved by author MLE, one of the developers of the SCL-CSQ.
Data analysis
Quantitative data
SPSS 28.0 software [24] was used in all descriptive and statistical analyses, and statistical significance was set at p < 0.05. Internal consistency of each subscale was estimated using Cronbach’s alpha coefficient. Values ≥0.70 were considered acceptable [25]. Pearson’s Product-Moment Correlation was used to determine criterion validity of each subscale.
Qualitative data
Qualitative data from the three interview phases were pooled and analyzed collectively. The analysis consisted of several steps. The first step was to explore the responses of each item across all three phases of the interview to investigate whether the participants understood the items as intended and replied accordingly. For this, a coding framework was developed with five codes: Congruent, incongruent, ambiguous, confusion with content, and confusion with response categories (for details, please see Table 1). This was based on previous research [26] but with confusion split into two separate codes, namely confusion with content and confusion with response categories to illustrate the fact that some were confused by the item itself, while others were confused with how to translate their response to the available response options.
The two authors conducting the analysis (AA and SLR) familiarized themselves with the data and coding framework. All responses were analyzed and compared against the theoretical conceptualization of each subscale (for details, please see the introduction of this paper) and coded in accordance with the coding framework. Key points and illustrative passages were identified and indexed in a data extraction matrix to enable further analysis and quotations. Coding was carried out by AA and SLR independently. Then, disagreements were discussed, and two other authors (TEA and MLE) were consulted when necessary. The second analytical step was to sum the number of different responses for each item. Items with less than 50% congruent responses were characterized as problematic and in need of further analysis. This cutoff was chosen prior to data analysis and was based on previous research using this method [27]. For these problematic items, a third analytical step was initiated, in which relevant themes among noncongruent responses were identified. This was carried out to explore common issues and reasons for non-congruency for each item. This was carried out by author AA and was inspired by Braun and Clarke’s thematic analysis [28]. To illustrate these themes, some quotes were identified. These were translated into English by author AA and paraphrased to help comprehension.
Results
Sample characteristics
Of the 117 individuals with SCI who participated in the survey, 10 did not provide complete data on all three scales (SCL-CSQ, PHQ-9, and SCI-QOL) and were thus excluded. Hence, the final sample consisted of 107 participants. Sample characteristics are presented in Table 2.
Interviews were conducted with 12 individuals with SCI. The final sample consisted of 11 individuals, as one interview could not be transcribed due to poor audio quality. The sample included 5 women and 6 men with a mean age of 58 years. Most had incomplete tetraplegia (n = 5) and had lived with their injury 5 to 10 years (n = 5). Further sample characteristics are presented in Table 3.
Internal consistency and criterion validity
Internal consistency was acceptable for both the acceptance subscale (Cronbach’s alpha = 0.72) and the fighting spirit subscale (Cronbach’s alpha = 0.76), while the social reliance subscale had inadequate internal consistency (Cronbach’s alpha = 0.58).
In terms of criterion validity, acceptance showed a strong negative correlation with depression (r = −0.64, p < 0.001) and a moderate positive correlation with QoL (r = 0.49, p < 0.001) as expected. Fighting spirit likewise showed expected moderate negative correlation with depression (r = −0.36, p < 0.001) and a weak positive correlation with QoL (r = 0.26, p = 0.007). Social reliance showed a weak, but non-significant, positive correlation with depression (r = 0.10, p = 0.31) and a weak, but also non-significant, negative correlation with QoL (r = −0.18, p = 0.07).
Construct validity based on response processes
Overall, the acceptance and fighting spirit subscales showed mostly congruent responses, as only item 6 was problematic with only 45% congruent responses. Conversely, item 4 and item 9 from the social reliance subscale showed issues with only 9% and 27% congruent responses, respectively. The distribution of responses across the items are represented in Fig. 1.

Within each subscale (i.e., acceptance, fighting spirit, and social reliance) the number of responses coded as congruent (green), incongruent (red), ambiguous (yellow), confusion with content (blue), and confusion with response categories (purple) are counted.
Analysis of noncongruent responses to problematic items
As described above, a total of three items had under 50% of congruent responses and were therefore deemed problematic and in need of further analysis. These were item 6 (acceptance subscale) and item 4 and 9 (social reliance subscale).
Item 6 (i.e., “What I have lost physically I have regained in so many other ways”) was the only acceptance item with less than 50% congruent responses. The congruent responses centered on an interpretation of losing something physical but gaining something in other aspects of life such as new interests and meaning in life:
“I agree that I am missing out on some things, and then I have offset these with other things that have become an interest” (P6).
“Well, I have lost the ability to get up and go for a walk and stuff like that […], but it is about organizing your life in other ways to make it meaningful” (P1).
Conversely, a common theme among all four incongruent responses centered on an interpretation that linked the physical loss to a physical gain. In this interpretation, losing something physical could never be regained by something non-physical:
“I think that would mean that I was back to the [physical] level I was before, and that is not the case at all” (P2).
Two responses were coded as ambiguous reflecting both a congruent and incongruent interpretation. For instance, one participant (P8) described that what he understood by the item was similar to the saying: “What you lose on the swings, you gain on the roundabouts”, which was deemed congruent, but elaborates further that he can never win back physically what he has lost physically, which was deemed incongruent.
Item 4 (i.e., You have to believe that other people are able to help you) was interpreted incongruently by a large majority; in fact, only one participant interpreted the item congruently. This person’s interpretation reflected the distinction between believing others can help and having to believe that others can help:
“I disagree that I have to believe that others can help me. If I am being asked whether I believe that others can help me, I would definitely say agree, but here I have to believe they can help” (P4).
On the other hand, there were several incongruent interpretations, including an entitlement to receive help and a willingness to ask for help. However, the dominating theme reflected an interpretation focusing on whether other people have been able to help:
“If I was in need of help, there is not a doubt in my mind that someone would be there and would be ready to do it” (P1).
Lastly, item 9 (i.e., “My lesion has taught me that we are all dependent upon others”) was interpreted congruently by only three, while five interpreted it incongruently and another three ambiguously. The congruent responses focused on their feelings of dependency because of their injury:
“When you have an injury like I have, you are dependent on others. You absolutely must be” (P7).
In all five incongruent responses, the participants did not interpret the item as a psychological or social dependency due to their injury. Rather, it was interpreted in a societal perspective in the sense that we all have things we cannot do ourselves, so we are all dependent on each other:
“Well, my friend has always fixed my car, and he still does that, so I think that whether you are injured or not, you are still dependent on others” (P5).
The three ambiguous responses reflected both congruent and incongruent interpretations. For instance, one participant (P6) focused on feelings of being dependent on others but elaborated that it was not the injury per se but life in general that had taught her that.
Discussion
Summary of findings
This study aimed to translate and validate a Danish version of the SCL-CSQ in a triangulated mixed-methods design to determine internal consistency, criterion validity, and construct validity based on response processes. Internal consistency was adequate for both the acceptance and fighting spirit subscales, and both correlated, as hypothesized, positively with QoL and negatively with depression underlining satisfactory criterion validity. Moreover, in the TSTI, the acceptance and fighting spirit subscales mostly showed congruent responses. Only item 6 of the acceptance subscale was denoted problematic with 45% congruent responses. Conversely, the social reliance subscale showed inadequate internal consistency and did not significantly correlate with either QoL or depression as was hypothesized. In the TSTI, the social reliance subscale showed serious issues with two items having only 9% and 27% congruent responses. In sum, the acceptance and fighting spirit subscales of the Danish version of the SCL-CSQ showed good psychometric properties, while the social reliance subscale showed serious issues and should only be used with considerable caution and preferably revised prior to use.
Previous research
Previous research has found similar issues with the social reliance subscale including inadequate internal consistency [7, 10] and criterion validity [7, 29]. Some authors have even speculated that items 4 and 9 might have been interpreted opposite than what was intended and thus reflected social support [7]. The TSTI findings help explain why these issues emerge within the social reliance subscale. First, item 4 was interpreted incongruently in various ways, but the most common theme was an interpretation reflecting availability of social support rather than psychological or social dependency on others. Furthermore, the interpretation of item 9 often reflected a sense of interconnectedness with others on a societal scale. As item 8 was mostly interpreted congruently, these three items seem to measure different constructs with opposite valence, which manifests itself in both inadequate internal consistency and a lack of significant correlations with depression and QoL. Items 4 and 9 should be revised to better reflect the intended meaning of being psychologically or socially dependent on others in a negative way.
While the acceptance subscale showed good psychometric properties, the TSTI findings showed potential interpretation issues with item 6. Previous research has not found this item to be an issue [6, 7, 10,11,12]. There are several potential explanations for this discrepancy. First, the quantitative data did not show any issues with item 6, and all the previous studies have only used quantitative data. Hence, it might be an issue that mostly emerges within the TSTI methodology. Second, it could be due to translation issues. While the items were translated as directly as possible, the word “regained” might carry somewhat different connotations in English than Danish. In fact, the authors of the Iranian version of the SCL-CSQ considered this issue and chose to use a Persian word meaning “to compensate” instead of a direct translation [12]. This carries a somewhat different connotation while still conveying the intended meaning.
Strengths and limitations
The use of both quantitative and qualitative methods was an important strength of the present study. For instance, the social reliance subscale showed issues in terms of internal consistency and criterion validity, which has also been found in previous research, and the TSTI findings helped explain why these issues arose. Further, the TSTI data also highlighted how item 6 could be misinterpreted even though the acceptance subscale functioned adequately overall. These findings can be used as a foundation in future studies that aim to revise the original English version of the SCL-CSQ or in the adaptation of the SCL-CSQ into new languages and cultural settings.
There are also several limitations that should be considered when interpreting the findings of the present study. One of the major limitations concerns the potential unique characteristics of the Danish language or Danish context. There is often an assumption of exact translation in validation studies that ignores unique language variations and context [30]. For instance, the Danish word for “regained” in item 6 caused some issues in the present study, but the same word might not cause issues in the original English version or other languages.
Furthermore, the 50% cutoff to denote problematic items was chosen to focus the data analysis on the items with most frequent issues, but this is fundamentally an arbitrary cutoff, so the remaining items did also show some, albeit fewer, issues. The noncongruent responses to the other items were mostly idiosyncratic but might still be relevant to reflect on in future studies that aim to revise or adapt the SCL-CSQ to other languages, cultural contexts, and rehabilitation settings. An overview of these noncongruent interpretations is therefore provided in Supplementary Information Appendix 2.
Another limitation of the present study concerns the rather long time most participants had lived with their SCI. This meant that they had likely been in contact with several rehabilitation services and had thus been well versed in the rehabilitation language and shaped by the specific context that characterizes the Danish health care system. For instance, rehabilitation in Denmark generally focuses more on solving specific issues related to the SCI such as pain, physical limitations, secondary health conditions etc. This individualized approach to solving problems aligns well with the fighting spirit subscale and may help explain why these items were mostly understood congruently as opposed to acceptance and especially social reliance. How the items are understood by individuals who are either newly injured or have been in rehabilitation that focuses on other ways of coping (e.g., acceptance of the current situation) should therefore be explored in future studies.
Another limitation of the TSTI methodology is that thinking aloud in front of a researcher is an unusual way to respond to a questionnaire. It is possible that some participants read the questions more carefully than they would have if responding to the questionnaire by themselves. This could both have given participants a better understanding of the items but reading every word very carefully could also have caused confusion or ambiguities. The unusual setting was in fact mentioned by some of the participants following the interviews.
Lastly, as we were not able to send out invitations directly to people in the target population, we instead distributed study information, a link to the survey, and contact information via flyers, newsletter, and social media pages. While this was the best approach at hand, we do not have a reliable estimate of how many eligible individuals were reached, and a response rate could therefore not be calculated. As such, we do not have a reliable assessment of the representativeness of the study sample. However, comparing the study sample with recent Danish large-scale studies indicated a higher proportion of women (~50% compared to 33–37%), but similar sample demographics in terms of age, type of injury, injury completeness, and time since injury [31, 32].
Conclusion
The present study aimed at validating the Danish version of the SCL-CSQ using a mixed-methods approach. The acceptance and fighting spirit subscales showed adequate internal consistency and criterion validity, and all items except one was understood congruently by most participants. Conversely, the social reliance subscale showed issued both in terms of internal consistency and criterion validity, and the two out of three items were only understood congruently by a small minority.
Data availability
The quantitative dataset generated during the current study is available in deidentified form from the corresponding author upon reasonable request and following approval from the Danish Data Protection Agency.
References
Chevalier Z, Kennedy P, Sherlock O. Spinal cord injury, coping and psychological adjustment: a literature review. Spinal Cord. 2009;47:778–82.
Crewe NM, Krause JS. Spinal cord injury. In: Brodwin MG, Siu FW, Howard J, Bronwin ER, editors. Medical, psychosocial and vocational aspects of disability. Athens, GA: Elliott & Fitzpatrick, Inc.; 2009. pp. 289–305.
North N. The psychological effects of spinal cord injury: a review. Spinal Cord. 1999;37:671–9.
Post MWM, van Leeuwen C. Psychosocial issues in spinal cord injury: a review. Spinal Cord. 2012;50:382–9.
van Leeuwen C, Kraaijeveld S, Lindeman E, Post MWM. Associations between psychological factors and quality of life ratings in persons with spinal cord injury: a systematic review. Spinal Cord. 2012;50:174–87.
Elfström ML, Rydén A, Kreuter M, Persson L-O, Sullivan M. Linkages between coping and psychological outcome in the spinal cord lesioned: Development of SCL-related measures. Spinal Cord. 2002;40:23–9.
Elfström ML, Kennedy P, Lude P, Taylor N. Condition-related coping strategies in persons with spinal cord lesion: a cross-national validation of the Spinal Cord Lesion-related Coping Strategies Questionnaire in four community samples. Spinal Cord. 2007;45:420–8.
Bonanno GA, Kennedy P, Galatzer-Levy IR, Lude P, Elfström ML. Trajectories of resilience, depression, and anxiety following spinal cord injury. Rehabil Psychol. 2012;57:236–47.
Elfström ML, Kreuter M, Persson L-O, Sullivan M. General and condition-specific measures of coping strategies in persons with spinal cord lesion. Psychol Health Med. 2005;10:231–42.
Paker N, Bugdayci D, Kesiktas N, Sahin M, Elfström ML. Reliability and validity of the Turkish version of spinal cord lesion-related coping strategies. Spinal Cord. 2014;52:383–7.
Saurí J, Umaña MC, Chamarro A, Soler MD, Gilabert A, Elfström ML, et al. Adaptation and validation of the Spanish version of the Spinal Cord Lesion-related Coping Strategies Questionnaire (SCL CSQ-S). Spinal Cord. 2014;52:842–9.
Saffari M, Pakpour AH, Yaghobidoot M, Al Zaben F, Koenige HG. Cross-cultural adaptation of the spinal cord lesion-related coping strategies questionnaire for use in Iran. Injury. 2015;46:1539–44.
Markus KA, Borsboom D. Open questions about test score meaning. In: Frontiers of test validity theory. New York: Routledge; 2013. pp. 247–272.
American Educational Research Association, American Psychological Association, National Council on Measurement in Education. Standards for educational and psychological testing. Washinton, DC: American Educational Research Association; 2014.
Kroenke K, Spitzer RL, Williams JBW. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16:606–13.
Charlifue S, Post MW, Biering-Sørensen F, Catz A, Dijkers M, Geyh S, et al. International spinal cord injury quality of life basic data set. Spinal Cord. 2012;50:672–5.
Hak T, van der Veer K, Jansen H. The three-step test-interview (TSTI): an observation-based method for pretesting self-completion questionnaires. Surv Res Methods. 2008;2:143–50.
Martin A, Rief W, Klaiberg A, Braehler E. Validity of the Brief Patient Health Questionnaire Mood Scale (PHQ-9) in the general population. Gen Hosp Psychiatry. 2006;28:71–7.
Zhang Y-L, Liang W, Chen Z-M, Zhang H-M, Zhang J-H, Weng X-Q, et al. Validity and reliability of Patient Health Questionnaire-9 and Patient Health Questionnaire-2 to screen for depression among college students in China. Asia Pac Psychiatry. 2013;5:268–75.
Maroufizadeh S, Omani-Samani R, Almasi-Hashiani A, Amini P, Sepidarkish M. The reliability and validity of the Patient Health Questionnaire-9 (PHQ-9) and PHQ-2 in patients with infertility. Reprod Health. 2019;16:137.
Adewuya AO, Ola BA, Afolabi OO. Validity of the patient health questionnaire (PHQ-9) as a screening tool for depression amongst Nigerian university students. J Affect Disord. 2006;96:89–93.
Pedersen SS, Mathiasen K, Christensen KB, Makransky G. Psychometric analysis of the Patient Health Questionnaire in Danish patients with an implantable cardioverter defibrillator (The DEFIB-WOMEN study). J Psychosom Res. 2016;90:105–12.
Post MWM, Adriaansen JJE, Charlifue S, Biering-Sørensen F, van Asbeck FWA. Good validity of the international spinal cord injury quality of life basic data set. Spinal Cord. 2016;54:314–8.
IBM Corp. IBM SPSS Statistics for Macintosh, Version 28.0. Armonk, NY: IBM Corp; 2021.
Cortina JM. What is coefficient alpha? An examination of theory and applications. J Appl Psychol. 1993;78:98–104.
Bunzli S, Maujean A, Andersen TE, Sterling M. Whiplash patients’ responses on the impact of events scale-R. Clin J Pain. 2019;35:229–37.
Dornonville de la Cour FL, Norup A, Schow T, Andersen TE. Evaluation of response processes to the Danish Version of the Dutch Multifactor Fatigue Scale in stroke using the three-step test-interview. Front Hum Neurosci. 2021;15.
Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3:77–101.
Kennedy P, Evans M, Sandhu N. Psychological adjustment to spinal cord injury: the contribution of coping, hope and cognitive appraisals. Psychol Health Med. 2009;14:17–33.
Evans C, Paz C, Mascialino G. “Infeliz” or “Triste”: a paradigm for mixed methods exploration of outcome measures adaptation across language variants. Front Psychol. 2021;12.
Aaby A, Ravn SL, Kasch H, Andersen TE. Structure and conceptualization of acceptance: a split-sample exploratory and confirmatory factor analysis approach to investigate the multidimensionality of acceptance of spinal cord injury. J Rehabil Med. 2021;53.
Larsen CM, Juul-Kristensen B, Kasch H, Hartvigsen J, Frich LH, Boyle E, et al. The Danish Spinal Cord Injury Shoulder (DanSCIS) cohort: methodology and primary results. Spinal Cord. 2021;59:821–31.
Acknowledgements
We would like to thank all the participants for completing the survey and participating in the interviews.
Funding
The study was carried out as part of a Ph.D. project with internal funding from The Specialized Hospital for Polio and Accident Victims in Roedovre, Denmark. No additional funding was required.
Author information
Authors and Affiliations
Contributions
AA contributed to the conception and design of the study, and was responsible for data collection, quantitative and qualitative data analysis, creating figures and tables, and writing the paper. SLR contributed to the conception and design of the study, and was responsible for qualitative data analysis, provided continuous guidance and feedback on the manuscript, tables, and figures, and approved the final version of the paper. MLE contributed to the conception and design of the study, provided continuous guidance and feedback on the manuscript, tables, and figures, and approved the final version of the paper. HK contributed to the conception and design of the study, provided continuous guidance and feedback on the paper, tables, and figures, and approved the final version of the paper. TEA contributed to the conception and design of the study, provided continuous guidance and feedback on the paper, tables, and figures, and approved the final version of the paper.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval
The study was registered with University of Southern Denmark’s internal records of scientific projects (case no. 10.672), and ethics approval was not necessary according to Danish law (case no. 20192000-107).
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
About this article

Cite this article
Aaby, A., Ravn, S.L., Elfström, M.L. et al. Does the Danish version of the Spinal Cord Lesion-related Coping Strategies Questionnaire measure what we think it measures? A triangulated mixed-methods validation approach. Spinal Cord 60, 1080–1086 (2022). https://doi.org/10.1038/s41393-022-00825-7
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41393-022-00825-7
