
Abstract
Study design
Cross-sectional study.
Objective
To elucidate the association between age and incidence of deep vein thrombosis (DVT) in patients with spinal cord injury (SCI).
Setting
Rehabilitation Medicine Department of the First Affiliated Hospital of China University of Science and Technology.
Methods
Patients from August 2018 to December 2020 with SCI (N = 260) were tertiles divided the age into three groups to analyze the association between age and incidence of DVT.
Results
American Spinal Cord Injury Association impairment scale (AIS), urinary tract infection (UTI), pulmonary infection (PI), and anticoagulation therapy (AT) were confounders for the association between age and incidence of DVT. The incidence of DVT increased by 1.07-fold (Non-adjusted model, OR = 1.07, P < 0.001), 1.05-fold (Minimally-adjusted model: adjusted for confounders, OR = 1.05, P = 0.010) and 1.06-fold [Fully-adjusted model: adjusted for confounders and unbalanced probable variables: AIS, UTI, PI, AT, Sex, D-dimer(new), Fibrinogen (new), Modes of injury and Level of injury, OR = 1.06, P = 0.012] when age increased by 1 year. The incidence of DVT had an increasing trend with age in different age tertile in the three models (P for trend <0.05). Age had a linearly association with incidence of DVT (OR = 1.07, P = 0.065) and stable in different subgroups, for lower age, the association was also linearly (OR = 4.40, P = 1.000), for middle (fold point = 46.46, P < 0.001) and higher age (fold point = 66, P = 0.017), the association was curvilinear.
Conclusion
Age had a linearly association with incidence of DVT. Quitting smoking, preventing/treating UTI and AT should be adopted in advance for patients with SCI for all age, especially for older.
Similar content being viewed by others
Introduction
In a clinical setting, many patients with spinal cord injury (SCI) are generally screened for deep vein thrombosis (DVT) during rehabilitation, especially the older population. The incidence of DVT in the lower extremities ranges from 88 to 112 per 100,000 person-years and increases with age [1]. Older patients with SCI had higher complication and mortality rates than younger patients [2]. In acute traumatic SCI, older age was one of the independent risk factors for positive duplex screening for any (proximal and/or distal) DVT detected on rehabilitation admission [3]. Age and presence of other injured sites along with SCI were independent risk factors for symptomatic venous thromboembolism (VTE) [4]. Another study showed that advanced age was one of the statistically significant risk factors for perioperative DVT for degenerative cervical spine disease [5].
As mentioned above, age is an independent risk factor for DVT in patients with SCI. However, an analysis of 36,335 patients with idiopathic scoliosis who had undergone spinal fusion surgery revealed that younger patients may have higher rates of postoperative complications (including DVT) than older age [6]. To the best of our knowledge, no study has reported the relationship between age and DVT in patients with SCI hospitalized in the Department of Rehabilitation Medicine. This study aimed to investigate the effect of age on incidence of DVT for patients with SCI. Our findings may be useful for developing personalized DVT prevention strategies for patients with SCI of different ages.
Methods
Data collection and flowchart of the study
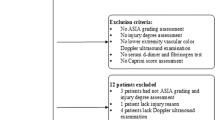
We collected the data of 262 patients with SCI who were hospitalized in the Rehabilitation Medicine Department of First Affiliated Hospital of China University of Science and Technology from August 1, 2018 to December 31, 2020. Finally, 260 (99.24%) patients with SCI were included; out of all the patients who were screened using Doppler ultrasonography, 87 (34.46%) had lower-extremity DVT. On admission, the following were collected: sex, age, mode of injury, American Spinal Cord Injury Association impairment scale (AIS), smoking history, D-dimer, fibrinogen, incidence of DVT and complications (urinary tract infection [UTI] and pulmonary infection [PI]).The patients were divided into three groups according to the age tertile (divided into three equal groups according to 33.3 and 66.6% cutoff points),The lower age group included 83 cases, the middle age group included 89 cases, and the higher age group included 88 cases (Fig. 1).

Inclusion and exclusion criteria are as follows. AIS: American Spinal Cord Injury Association impairment scale; DVT: deep vein thromobosis.
Study design
This was an observational cross-sectional study.
Statistical methods
Continuous variables were expressed as mean ± standard deviation (SD) (Gaussian distribution) or median (minimum, maximum) (skewed distribution), and categorical variables were expressed as frequencies and percentages (N%). χ2 (categorical variable), one-way analysis of variance test (normal distribution), or the Kruskal–Wallis H test (skewed distribution) was used to analyze differences between ages (third quartiles). Multivariate binary logistic regression models were used to analyze the association between age and incidence of DVT with three distinct models. Multivariate logistic regression was used to screen out the covariates of age and incidence of DVT, the variables were excluded if the variance inflation factor (VIF) was greater than ten [7], then the potential confounders were selected if they changed the estimates of incidence of DVT by at least 10% in the final models [8, 9]. Model 1 was the non-adjusted model with no covariates adjusted. Model 2 was the minimally-adjusted model with only confounders adjusted. Model 3 was the fully-adjusted model with the confounders and unbalanced probable variables (presented in Table 1) adjusted. Since binary logistic regression model-based methods were often suspected to be unable to handle nonlinear models, we used the generalized additive model (GAM) and smooth curve fitting (penalized spline method) to address the nonlinearity between age and incidence of DVT. When nonlinearities were detected, the fold point was first computed using a recursive algorithm, and then a two-piece binary logistic regression model was constructed on either side of the fold point. A subgroup analysis was performed using a layered (stratified) binary logistic regression model. For continuous variables (D-dimer and fibrinogen), we first converted them into categorical variables according to third quartile (tertile), and then an interaction analysis was performed. A test for modifying the effect on the subgroup indicator was followed by a likelihood ratio test. Additionally, a sensitivity analysis was performed to analyze the robustness of the results. To validate the results of age group as a continuous variable and investigate the likelihood of nonlinearity, age group was transformed into a continuous variable, and the P for trend was calculated. Dummy variables were used to indicate missing covariate values; [10] for continuous variable, if covariate values missed, we assignment it zero and the new transformed continuous variable was named “variable (new)”, and then transformed to a categorical variable named “variable (indicator)” based on whether the data missed; for categorical variables, if covariate values missed, we named it as “not recorded”. A two-sided P < 0.05 was indicated as statistically significant. All analyses were performed using EmpowerStats (www.empowerstats.com; X&Y Solutions Inc.) and R statistical package (R Foundation; http://www.r-project.org; version 3.6.1).
Results
Characteristics of the study population
In the higher age group, the age (P < 0.001), D-dimer (new) level (P = 0.016), sex of male (P = 0.037), injury of cervical (P = 0.009), AT (P < 0.001) and incidence of DVT (P < 0.001) were all higher than in the middle and lower age groups. The middle age group had the highest fibrinogen (new) level, followed by the higher age group and the lower age group (P = 0.015). For variable of D-dimer (indicator) (P = 0.244) and fibrinogen (indicator) (P = 0.352), the ratio of data missing was stable in three age groups. SCI caused by trauma was the highest in the middle age group, followed by the higher and lower age groups (82.02% vs. 78.41% vs. 77.11%, respectively) (P = 0.029). For AIS-A, the lower age group had the highest grades, followed by the middle and higher age groups (AIS-A: 30.12% vs. 23.60% vs. 18.18%, respectively); for AIS-B, the middle age group had the highest grades, followed by the lower and higher age groups (AIS-B: 23.60% vs. 19.28% vs. 9.09% respectively); for AIS-C, the higher age group had the highest grades, followed by the lower and middle age groups (AIS-C: 31.82% vs. 16.87% vs. 16.85%, respectively); for AIS-D, the higher age group had the highest grades, followed by the middle and lower age groups (AIS-D: 39.77% vs. 34.83% vs. 32.53%, respectively) (P = 0.063). For smoking history, the higher age group had the highest number, followed by the lower and middle age groups (23.86% vs. 21.69% vs. 15.73%, respectively) (P = 0.381). The middle age group had UTI the most, followed by the lower and higher age groups (58.43% vs. 54.22% vs. 48.86%, respectively) (P = 0.393). The higher age group had PI the most, followed by the middle and lower age groups (27.27% vs. 21.35% vs. 10.84%, respectively) (P = 0.053). The duration of anticoagulation was stable in three age groups (P = 0.315) (Table 1).
Multivariate analysis of age and incidence of DVT
We added all variables to the logistic regression model and in the covariate screening analysis, D-dimer (indicator) and fibrinogen (indicator) were excluded because multicollinearity (VIF ≥ 10), then we found that AIS, UTI, PI and AT were confounders for the association between age and incidence of DVT. As seen in Supplementary Table 1, we selected these covariates on the basis of their associations with a change in effect estimate of over 10% [8, 9]. Based on the dummy strategies, the D-dimer (new), fibrinogen (new), modes of injury, sex level of injury and AT were selected for adjusting as these variables were not stable in different age group in Table 1. For the non-adjusted model, minimally-adjusted model (adjusted for: AIS, UTI, PI, and AT) and fully-adjusted model [adjusted for: AIS, UTI, PI, AT, Sex, D-dimer(new), Fibrinogen (new), Modes of injury and Level of injury], the incidence of DVT increased by 1.07, 1.05, and 1.06-fold when age increased by 1 year (P < 0.001, P = 0.010 and 0.012, respectively), which means the association of age and incidence of DVT was very close and stable in three models. Meanwhile, the incidence of DVT had an increasing trend with age in the three models (P for trend < 0.001, P for trend = 0.021 and 0.026, respectively) (Table 2).
Curvilinear fitting analysis of age and incidence of DVT
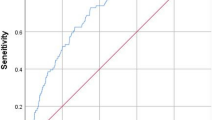
After adjusting for the confounders and unbalanced probable variables [AIS, UTI, PI, AT, Sex, D-dimer(new), Fibrinogen (new), Modes of injury and Level of injury], a linear association was observed between age and incidence of DVT for patients with SCI. The estimated change was −2.81 (95% CI: 0.00–1.03, Fig. 2).

General additive models demonstrate the relationship between age and the incidence of DVT. The resulting figures showed the predicted incidence of DVT in the y-axis and the age in the x-axis. The black line was the fitting curve and the interval between the dot lines was 95% CI.
Threshold saturation effect analysis of age and incidence of DVT
After adjusting for the confounders and unbalanced probable variables [AIS, UTI, PI, AT, Sex, D-dimer(new), Fibrinogen (new), Modes of injury and Level of injury] using the threshold saturation analysis conducted using the GAM, the logarithmic likelihood ratio test showed that age had a linear association with incidence of DVT (P = 0.065), the incidence of DVT increased by 1.07-fold when age increased by 1 year (OR = 1.07, P = 0.140). For the lower age group, the logarithmic likelihood ratio test showed that age also had a linear association with incidence of DVT (P = 1.000), the incidence of DVT increased by 4.40-fold when age increased by 1 year (OR = 4.40, P = 1.000). However, age had a curvilinear association with incidence of DVT in the middle and higher age groups, and the fold point was 46.46 (P < 0.001) and 66 (P = 0.017) years, respectively. For the middle age, the incidence of DVT did not been computed when age increased by 1 year for segmental analysis at the fold point of 46.46 years, the reason may be was the small sample size of this subgroup. For the higher age group, the incidence of DVT increased by 0.77-fold when age increased by 1 year if age was <66 years (OR = 0.77, P = 0.118), and increased by 1.69-fold if age was >66 years (OR = 1.69, P = 0.087) (Table 3). After adjusting for the confounders and unbalanced probable variables, segmental curvilinear fitting analysis also showed lower age had a linear association with incidence of DVT, middle, and higher age had a curvilinear association with incidence of DVT (Supplementary Fig. 1).
Sensitivity analysis of age and incidence of DVT
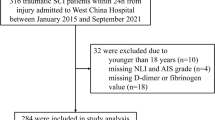
For different sexes (male: OR = 1.06, P < 0.01; female: OR = 1.08, P < 0.01), AIS (AIS-A:OR = 1.07, P = 0.003; AIS-B:OR = 1.08, P = 0.035; AIS-C:OR = 1.06, P = 0.005; AIS-D:OR = 1.08, P < 0.001), UTI (No: OR = 1.14, P < 0.001; Yes: OR = 1.03, P = 0.010), PI (No: OR = 1.06, P < 0.001; Yes: OR = 1.11, P = 0.003) and fibrinogen (tertile) (Lower: OR = 1.12, P < 0.001; Middle: OR = 1.03, P = 0.049; Higher: OR = 1.08, P < 0.001), the subgroup analysis showed that the plots were all at the right of the reference line (OR > 1, P < 0.05). For mode of injury (Trauma: OR = 1.06, P < 0.001; Cervical spondylotic myelopathy: OR = 1.22, P = 0.068), smoking history (No: OR = 1.08, P < 0.001; Yes: OR = 1.02, P = 0.385), D-dimer (tertile)(Lower: OR = 1.04, P = 0.144; Middle: OR = 1.07, P = 0.001; Higher: OR = 1.07, P = 0.002), D-dimer and Fibrinogen (Recorded: OR = 1.07, P < 0.001), level of injury (Cervical: OR = 1.09, P < 0.001; Thoracic: OR = 1.06, P = 0.004; Lumbar: OR = 1.04, P = 0.104), AT (No: OR = 1.04, P = 0.232; Yes: OR = 1.05, P = 0.005), the plots were also all at the right of the reference line(OR > 1). Which indicated that the estimated changes (OR > 1) were stable in this subgroups (Fig. 3).

The dot plots are OR value, the perpendicular line is the reference line and the horizontal lines are 95% CIs.
Missing data can’t been tested in interaction screening analysis, two hundred forty-six cases were included in the final logistic regression model (Supplementary Tables 2, 3), multi-categorical variables with small sample size (modes of injury and level of injury) also cannot been tested in interaction screening analysis, so these two variables were transformed to binary variables, and the results showed smoking history (P interaction value = 0.011) and UTI (P interaction value <0.001) were effect modifiers for the association between age and incidence of DVT (Supplementary Table 4). After adjusted the confounders (minimally-adjusted model: AIS, UTI, PI and AT) and all the unbalanced variables presented in Table 1 [fully-adjusted model: AIS, UTI, PI, AT, Sex, D-dimer(new), Fibrinogen (new), Modes of injury, and Level of injury], smoking history was not an effect modifier (P interaction value = 0.065 and 0.062, respectively) (Supplementary Table 5). After adjusted the confounders (minimally-adjusted model: AIS, PI and AT) and all the unbalanced variables presented in Table 1 [fully-adjusted model: AIS, PI, AT, Sex, D-dimer (new), Fibrinogen (new), Modes of injury and Level of injury], UTI was also not an effect modifier (P interaction value = 0.070 and 0.076, respectively) (Supplementary Table 6). Further, we performed a curvilinear fitting analysis of age and incidence of DVT between the subgroups of smoking history and UTI. For subgroups of smoking history, after adjusting the confounder and unbalanced probable variables [AIS, UTI, PI, AT, Sex, D-dimer (new), Fibrinogen (new), Modes of injury, and Level of injury], the incidence of DVT of patients with SCI who had smoking history had a U-shaped curvilinear association with aging, and the association between age and incidence of DVT was linear for patients without smoking history (Supplementary Fig. 2). For subgroups of UTI, after adjusting the confounder and unbalanced probable variables [AIS, PI, AT, Sex, D-dimer (new), Fibrinogen (new), Modes of injury, and Level of injury]), the incidence of DVT of patients with UTI had a linearly increasing association with aging, and the incidence of DVT of patients with SCI who had UTI was greater than those without UTI before the age of 54 years than after the age of 54 years (Supplementary Fig. 3).
Discussion
AIS, UTI, PI, and AT were covariates of the association between age and incidence of DVT. After adjusting for the confounders and unbalanced probable variables [AIS, UTI, PI, AT, Sex, D-dimer(new), Fibrinogen (new), Modes of injury and Level of injury], The incidence of DVT increased by 1.07-fold (Non-adjusted mode), 1.05-fold (Minimally-adjusted model: adjusted for confounders) and 1.06-fold [Fully-adjusted model: adjusted for confounders and unbalanced probable variables: AIS, UTI, PI, AT, Sex, D-dimer(new), Fibrinogen (new), Modes of injury and Level of injury] when age increased by 1 year. Lower age also had a linearly association with incidence of DVT, middle and higher age had a curvilinear association with incidence of DVT (fold point = 46.46 and 66 years, respectively).
Serum fibrinogen levels in patients with SCI were significantly increased after injury and were associated with the severity of neurologic deficits [11]. Fibrinogen was a risk factor for DVT [12], and fibrinogen level on day 10 was a predictor of postoperative incidence of DVT for patients undergoing hip replacement [13]. However, another study has shown that the fibrinogen test underestimated the degree of femoral vein thrombosis in a significant proportion of cases [14]. D-dimer level was also associated with incidence of DVT, compared to traditional D-dimer, age-adjusted D-dimer performed better in DVT screening, this was clinically useful [15]. Measurements of D-dimer levels should be complemented by routine compressive Doppler ultrasonography to detect DVT within 6 months after SCI; for 6 months or more, the usefulness of D-dimer screening alone was superior to DVT detection [16]. According to a report on the epidemiological characteristics of SCI in northwestern China, the incidence of SCI in northwestern China was increasing and the proportion of male was high, the occupations most threatened by SCI were farmers and workers [17]. AIS grade (A/B) and D-dimer > 1.08 µg/ml were risk factors independently correlated to DVT for patients with spinal fracture [18]. Age and severe neurological impairment (AIS-A/B/C) were independent risk factors for DVT in patients with SCI [3]. A study reported that when age was >45 years and smoking history and AIS-A of SCI were present, preventive measures should be taken in advance to prevent DVT formation [19]. Here, we found that AIS grades were covariates for the association between age and incidence of DVT. The baseline of sex, career, D-dimer and fibrinogen level was not stable in different age group. Age had a linearly association with incidence of DVT in patients with SCI; lower age also had a linearly association with incidence of DVT, middle and higher age had a curvilinear association with incidence of DVT.
Tobacco use was a risk factor for VTE [20], and smoking and older age were consistently associated with a higher VTE risk [21]. Smoking significantly increased the incidence of DVT for patients following elective arthroscopic knee surgery [22]. Moreover, a mendelian randomization study supports a causal association between smoking and a broad range of cardiovascular diseases, in particular peripheral arterial disease and arterial hypertension [23]. Another study concluded that the management of tobacco use during the preoperative period for a short-term suspension (at least 4–8 weeks before intervention), or long-term suspension could reduce the occurrence of VTE events [24]. However, there have been no reports on the association between smoking and DVT in patients with SCI. Here, we found that smoking was an effect modifier for the association between age and incidence of DVT in crude model; however, after adjusting for the confounders and unbalanced probable variables, smoking was not an effect modifier.
Neuromuscular patients (including patients with SCI) had an increased risk for the occurrence of UTI and DVT [25]. Most UTIs are uncomplicated UTIs, defined as cystitis in non-pregnant women, without immunodeficiency, without anatomical and functional abnormalities of the genitourinary system, and without signs of tissue infiltration and systemic infection, all UTIs that are not uncomplicated are considered to be complicated UTIs [26]. Complicated UTI carries an increased risk of developing complications for those who have a functional abnormality of the urogenital tract (e.g., patients with SCI) [26]. For patients with SCI, treating and preventing UTI could prevent systemic complications [27]. Hospitalization with infection was a strong VTE-trigger in immobilized and non-immobilized patients, so the researchers concluded that infection and immobilization had a synergistic effect on the VTE risk [28]. Our study found that UTI had an interaction with age and incidence of DVT for patients with SCI in crude model; however, after adjusting for the confounders and unbalanced probable variables, UTI was not an effect modifier.
Our study has some limitations. First, due to the lack of follow up, we were unable to confirm the long-term effect of the change in age on incidence of DVT. Second, as this was a single-center, cross-sectional study, and the results may be biased in other centers. Third, due to the actual clinical situation, the time of immobilization was hard to collect, so we cannot conclude the interactive associations of this variable on age and incidence of DVT; in the future, further animal experiments or high-quality random control clinical trials are needed to determine the association between the time of immobilization and incidence of DVT. Fourth, the rank of evidence is not sufficiently high for the cross-sectional design; nevertheless, our study may be useful as a reference for further clinical studies of advanced rank, such as cohort and random control clinical trials.
Conclusion
In patients with SCI, AIS, UTI, PI, and AT were covariates of the association between age and incidence of DVT. Age had a linearly association with incidence of DVT for patients with SCI, and the incidence of DVT increased by 1.07-fold when age increased by 1 year. Lower age also had a linearly association with incidence of DVT, middle and higher age had a curvilinear association with incidence of DVT (fold point = 46.46 and 66 years, respectively). Although smoking history and UTI were not effect modifiers for the association between age and incidence of DVT in minimally and fully-adjusted model, which still had an interaction with the association between age and incidence of DVT in crude model. Thus, it is necessary to adopt active DVT prevention strategies in advance, such as quitting smoking, preventing or treating UTI, and providing AT, especially for older patients with SCI.
Data availability
The datasets analyzed during the current study are available from the corresponding author on reasonable request.
References
Chopard R, Albertsen IE, Piazza G. Diagnosis and treatment of lower extremity venous thromboembolism: a review. JAMA. 2020;324:1765–76.
Lau D, Dalle Ore CL, Tarapore PE, Huang M, Manley G, Singh V, et al. Value of aggressive surgical and intensive care unit in elderly patients with traumatic spinal cord injury. Neurosurg Focus. 2019;46:E3.
Hon B, Botticello A, Kirshblum S. Duplex ultrasound surveillance for deep vein thrombosis after acute traumatic spinal cord injury at rehabilitation admission. J Spinal Cord Med. 2020;43:298–305.
Piran S, Schulman S. Incidence and risk factors for venous thromboembolism in patients with acute spinal cord injury: a retrospective study. Thromb Res. 2016;147:97–101.
Yamada K, Suda K, Matsumoto Harmon S, Komatsu M, Ushiku C, Takahata M, et al. Rapidly progressive cervical myelopathy had a high risk of developing deep venous thrombosis: a prospective observational study in 289 cases with degenerative cervical spine disease. Spinal Cord. 2019;57:58–64.
De la Garza Ramos R, Goodwin CR, Abu-Bonsrah N, Jain A, Miller EK, Huang N, et al. Patient and operative factors associated with complications following adolescent idiopathic scoliosis surgery: an analysis of 36,335 patients from the Nationwide Inpatient Sample. J Neurosurg Pediatr. 2016;25:730–6.
Kim JH. Multicollinearity and misleading statistical results. Korean J Anesthesiol. 2019;72:558–69.
Ernst M, Hartz A. Phenylpropanolamine and hemorrhagic stroke. N Engl J Med. 2001;344:1094.
Jaddoe V, de Jonge L, Hofman A, Franco O, Steegers E, Gaillard R. First trimester fetal growth restriction and cardiovascular risk factors in school age children: population based cohort study. BMJ. 2014;348:1–11.
Vetter C, Devore E, Wegrzyn L, Massa J, Speizer F, Kawachi I, et al. Association Between Rotating Night Shift Work and Risk of Coronary Heart Disease Among Women. JAMA. 2016;315:1726–34.
Liu JM, Lan M, Zhou Y, Chen XY, Huang SH, Liu ZL. Serum concentrations of fibrinogen in patients with spinal cord injury and its relationship with neurologic function. World Neurosurg. 2017;106:219–23.
Bozic M, Teran N, Peterlin B, Stegnar M. Fibrinogen polymorphisms TaqI, HaeIII and BclI are not associated with a higher risk of deep vein thrombosis. Pathophysiol Haemost Thromb. 2003;33:164–9.
Crippa L, Ravasi F, D’Angelo SV, Varagona R, Milani E, Safa O, et al. Diagnostic value of compression ultrasonography and fibrinogen-related parameters for the detection of postoperative deep vein thrombosis following elective hip replacement: a pilot study. Thromb Haemost. 1995;74:1235–9.
McLvor J, Anderson DR, Britt RP, Dovey P. Comparison of 125I-labelled fibrinogen uptake and venography in the detection of recent deep-vein thrombosis in the legs. Br J Radiol. 1975;48:1013–8.
Wu J, Qing J, Yao Y, Chen D, Jiang Q. Performance of age-adjusted D-dimer values for predicting DVT before the knee and hip arthroplasty. J Orthop Surg Res. 2021;16:82.
Mackiewicz-Milewska M, Cisowska-Adamiak M, Pyskir J, Świątkiewicz I. Usefulness of D-dimer and ultrasonography screening for detecting deep vein thrombosis in patients with spinal cord injury undergoing rehabilitation. J Clin Med. 2021;10:689.
Wang ZM, Zou P, Yang JS, Liu TT, Song LL, Lu Y, et al. Epidemiological characteristics of spinal cord injury in Northwest China: a single hospital-based study. J Orthop Surg Res. 2020;15:214.
Ma J, Du P, Qin J, Zhou Y, Liang N, Hu J, et al. Incidence and risk factors predicting deep venous thrombosis of lower extremity following spinal fractures. Sci Rep. 2021;11:2441.
Yu X, Liu W, Zhang HW. [Analysis of related factors of deep venous thrombosis after spinal cord injury]. Zhongguo Gu Shang. 2020;33:140–3.
Teter K, Schrem E, Ranganath N, Adelman M, Berger J, Sussman R, et al. Presentation and management of inferior vena cava thrombosis. Ann Vasc Surg. 2019;56:17–23.
Gregson J, Kaptoge S, Bolton T, Pennells L, Willeit P, Burgess S, et al. Cardiovascular risk factors associated with venous thromboembolism. JAMA Cardiol. 2019;4:163–73.
Özcan M, Erem M, Turan FN. Symptomatic deep vein thrombosis following elective knee arthroscopy over the age of 40. Clin Appl Thromb Hemost. 2019;25:1–6.
Larsson SC, Mason AM, Bäck M, Klarin D, Damrauer SM, Michaëlsson K, et al. Genetic predisposition to smoking in relation to 14 cardiovascular diseases. Eur Heart J. 2020;41:3304–10.
Al-Nasser B. Influence of tobacco smoking on perioperative risk of venous thromboembolism. Turkish J Anaesthesiol Reanim. 2020;48:11–6.
Cichos KH, Lehtonen EJ, McGwin G Jr., Ponce BA, Ghanem ES. Inhospital complications of patients with neuromuscular disorders undergoing total joint arthroplasty. J Am Acad Orthop Surg. 2019;27:e535–43.
Geerlings SE. Clinical presentations and epidemiology of urinary tract infections. Microbiol Spectr. 2016;4:1–11.
Hu HZ, Granger N, Jeffery ND. Pathophysiology, clinical importance, and management of neurogenic lower urinary tract dysfunction caused by suprasacral spinal cord injury. J Vet Intern Med. 2016;30:1575–88.
Grimnes G, Isaksen T, Tichelaar Y, Brækkan SK, Hansen JB. Acute infection as a trigger for incident venous thromboembolism: Results from a population-based case-crossover study. Res Pract Thromb Haemost. 2018;2:85–92.
Acknowledgements
We would like to thank Tingting Zhang, CuicuiChang, Tingting Bao, Nanzu Chengjiang, Liai Sun, and Lina Ma for collecting the data. We would also like to thank Xinglin Chen for helping us analyze the data and thanks to Editage (www.editage.com) for editing the English.
Author information
Authors and Affiliations
Contributions
JLZ: Conducted the study and wrote the draft. YYF: Designed the study, interpreted the data, and edited the manuscript. HYP, YT, JZ, and SSZ: Collected the data. CW: Planned the project, created, and statistical analyzed the data. The authors all read and approved the final paper.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
Informed consent was waived due to the nature of the retrospective study, which consistent with ethical requirements and waiver from the Ethics Committee of First Affiliated Hospital of the University of Science and Technology of China (Anhui Provincial Hospital), this study also approved by the committee, the approved number was 2020-RE-008.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
About this article

Cite this article
Zhang, J., Fang, Y., Pang, H. et al. Association between age and incidence of deep vein thrombosis in patients with spinal cord injury: an observational cross-sectional study. Spinal Cord 60, 1006–1013 (2022). https://doi.org/10.1038/s41393-022-00814-w
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41393-022-00814-w
This article is cited by
-
Distribution characteristics of perioperative deep vein thrombosis (DVT) and risk factors of postoperative DVT exacerbation in patients with thoracolumbar fractures caused by high-energy injuries
European Journal of Trauma and Emergency Surgery (2024)
