
Abstract
Study design
Cross-sectional.
Objectives
To evaluate current practice of Latin American spine surgeons regarding surgical timing in patients with traumatic spinal cord injury (tSCI) and to identify potential barriers for early surgery.
Setting
Web-based.
Methods
A web-based questionnaire was sent to members of AOSpine Latin America. Questions involved demographic features, familiarity with management of tSCI, and timing of surgery in various tSCI scenarios. The participants were also asked if they would like to operate earlier on patients with tSCI, indicating potential obstacles to early surgery.
Results
A total of 307 surgeons answered the questionnaire. Early surgery (<24 h) is performed by 66.8% for ASIA A, 76.9% for ASIA B, and 76.9% for ASIA C/D injuries. For traumatic cauda equina syndrome (tCES), 85.2% performed surgery within 24 h. For traumatic central cord syndrome (tCCS) without osteoligamentous instability, only 31.5% performed surgery within 24 h and 41.2% follow-up on these patients, indicating surgery if no symptom improvement. Early surgery was performed always or in most cases by 50.4% and 41.8% of surgeons for incomplete and complete tSCI, respectively. The majority (85.4%) would like to operate earlier on patients with tSCI than they actually do. The most frequently perceived barriers to early surgery were difficulty of access to surgical implants (70.9%) and delay in patient transport to reference hospital for surgery (57.8%).
Conclusion
Latin American spine surgeons tend to operate earlier on patients with tCES and incomplete tSCI, then on those with complete tSCI and tCCS. The most reported obstacles for early surgery involved healthcare resources.
Similar content being viewed by others

Introduction
Traumatic spinal cord injury (tSCI) is a catastrophic event that affects patients’ lives. Despite the recent advances in neuroprotective and neurodegenerative strategies, no pharmacological therapy has proved clinical efficacy to be implemented in routine clinical practice [1]. On the other hand, there is growing evidence demonstrating that timely surgical decompression and stabilization may improve neurological recovery by reducing secondary damage to the spinal cord [2,3,4,5,6,7,8,9,10,11,12,13,14]. In addition, potential benefits of early surgery include less complications, reduced length of hospital stay, and reduced costs [15, 16]. The concept of “time is spine” highlights this critical time window after the primary injury to the spinal cord during which secondary injury mechanisms may be minimized by therapies [17]. In fact, recent guidelines recommend surgical decompression and stabilization within 24 h of tSCI [18, 19].
Although early surgery is currently the only intervention that may improve neurological outcomes, it is estimated that only 39% of cervical and 45% of thoracic tSCI are operated within 24 h of injury in Canada [20]. Obstacles for early surgical intervention may be related to local healthcare resources or to patient variables, and they may vary in different healthcare systems and societies. International clinical practice variation and disagreement surrounding best practices in SCI have been previously investigated [21]. To date, there are no data regarding current practices in tSCI in Latin America. Identification of guideline adherence and obstacles for early surgery in tSCI may provide insights for education and address the needs for healthcare interventions in this continent.
Our goal was to evaluate current practice regarding surgical timing in patients with spine trauma with neurological involvement in Latin America. We also assessed potential barriers to early surgical intervention in this region.
Methods
Portuguese and Spanish modified versions of a questionnaire published by Ter Wengel et al. [22] were used to evaluate surgical timing practices in patients with tSCI in Latin America. An e-mail request to participate in the survey was sent to members of AOSpine Latin America (AOSLA) with a cover letter explaining the objective of this study and an attached link to Survey Monkey. The Portuguese-language version was applied to Brazilian members. The link was available for 15 days, and reminders were sent three times in March 2019. Time to complete the questionnaire ranged from 5 to 10 min.
The electronic questionnaire contained topics regarding demographic features of participants (orthopedist versus neurosurgeon; spine fellowship; time of clinical practice; type of clinical practice), familiarity with management of tSCI, and preferred timing of surgical decompression in patients with complete tSCI, incomplete tSCI, traumatic cauda equina syndrome (tCES), and traumatic central cord syndrome (tCCS). In addition, the participants were asked if they would like to operate earlier on patients with tSCI, and to indicate potential barriers to early surgery in these patients.
Statistical analyses were conducted with SPSS. Data were presented as number and percentage. Group comparisons were conducted with a chi-square test.
Results
A total of 307 AOSLA members answered the electronic questionnaire, with a response rate of 24.3% (n = 307/1261). Table 1 presents the general characteristics of the respondents. Most participants were orthopedic surgeons (56.7%), spine fellowship-trained (74.9%), 49.5% had more than 10 years of clinical practice in spine surgery, and most had a mixed practice including public and private (64.5%). Regarding experience with tSCI, only 5 (1.6%) answered that they do not treat spine trauma, and most of the participants treat up to 10 cases per year (53.4%).
Current practice on surgical timing in traumatic spinal lesions with neurological involvement
Figure 1 shows the current practice regarding surgical timing for unstable tSCI, spine fractures presenting with tCES, and tCCS. Regarding unstable tSCI, Latin American spine surgeons report having operated on patients with incomplete SCI earlier than on those with complete injuries. Indeed, 66.8% reported performing early surgery (<24 h) for ASIA A, 76.9% for ASIA B, and 76.9% for ASIA C/D injuries. For tCES, 85.2% reported a surgical timing of less than 24 h. For tCCS without osteoligamentous instability, in turn, only 31.5% operate these patients within 24 h. Conversely, 41.2% reported following up on these patients and indicate surgery if there is no improvement in symptoms.

ASIA American Spinal Injury Association, tCES traumatic cauda equina syndrome, tCCI traumatic central cord injury, ER emergency room.
For incomplete and complete tSCI, 29.3% and 38.3% of respondents never or rarely perform surgery in less than 24 h of trauma, respectively. Early surgery, in turn, was performed always or in most of the cases by 50.4% and 41.8% of surgeons for incomplete and complete tSCI, respectively (Fig. 2).

Frequency of early surgery (<24 h) for traumatic spinal cord injuries in Latin America (N = 307).
Factors associated with early surgery in traumatic spinal lesions with neurological compromise
Table 2 presents factors associated with early surgery (<24 h) in patients with traumatic spine injuries presenting with neurological involvement. It is observed that fellowship-trained spine surgeons are more likely to operate within 24 h in patients with incomplete tSCI ASIA C/D and tCES patients (p < 0.001). Surgeons practicing in public hospitals are less likely to operate within 24 h in all clinical scenarios (p < 0.01). No effect on surgical timing was observed in any of the clinical scenarios according to specialty (neurosurgery versus orthopedics), duration of practice, and volume of SCI per year.
Barriers to early surgery in traumatic spinal cord injury in Latin America
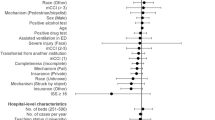
A total of 85.4% of the respondents stated that they would like to operate earlier on patients with traumatic tSCI than they actually do (Fig. 3). The most frequently perceived obstacles that delay the timing of the surgery were difficult access to surgical implants (70.9%) and delay in patient transport to a reference hospital to have surgery (57.8%). Only 11.6% of the participants believe there is not enough scientific evidence to support benefits of early surgery (<24 h) in tSCI.

A Proportion of Latin American spine surgeons that would like to operate earlier on patients with traumatic spinal cord injury than they actually do and B perceived barriers to early surgery (N = 307).
Table 3 demonstrates the perceived barriers for early surgery in tSCI in Latin America stratified by surgical specialty, fellowship training, type of practice, duration of practice and number of tSCI treated per year. It is observed that neurosurgeons are more likely to report problems with spine implants compared to orthopedic surgeons (79.8% versus 64.3%, p = 0.006). On the other hand, orthopedic surgeons were more likely to report difficulty in accessing the OR, anesthesia or ICU than neurosurgeons (44.2% versus 28.1%, p = 0.007). Hospital facilities were also pointed out as an obstacle to perform early surgery more frequently by surgeons who did not undergo fellowship training in spine surgery (49.1% versus 34.1%, p = 0.038).
Discussion
In this survey, we identified current surgical practices for spine trauma in patients presenting with neurological impairment to the emergency department in Latin America. Overall, a clear distinction of surgical timing was observed according to the severity (i.e. ASIA score) of neurological impairment among Latin American spine surgeons. There is a tendency to operate earlier on patients with incomplete tSCI or tCES than on those with complete tSCI (Figs. 1 and 2). Indeed, surgery within 24 h was performed in 67% for ASIA A, 77% for ASIA B, 77% for ASIA C/D, and 85% for tCES. Similarly, prior surveys regarding surgical timing for tSCI also showed that early surgery is more often preferred and performed for incomplete rather than for complete lesions – when these were analyzed separately [20, 22,23,24]. Table 4 details the ideal and actual reported surgical timing for tSCI in other surveys. Although different practices are reported regarding neurological impairment, current clinical practice guidelines (2017) do not make a distinction on surgical timing recommendations in regards to neurological level (i.e. cervical, thoracic or lumbar) and injury severity (i.e. ASIA score) in tSCI [19]. Although it is still controversial, recent studies have suggested that functional and neurological outcomes may be even better with ultra-early decompression (<12 h or less) [10, 25, 26]. Interestingly, a high proportion of Latin American spine surgeons (45%) reported that they operate within 12 h of injury on patients with incomplete tSCI.
We also evaluated the surgical timing of Latin American spine surgeons for two specific entities: tCES and tCCS. The frequency of early surgery within 12 h and 24 h was even higher for tCES compared to tSCI. (Fig. 1). Similarly, Fehlings et al. [23] showed that 69.4% and 89.6% of surgeons prefer to operate on patients with traumatic conus medullaris syndrome (tCMS) with sphicnteric dysfuntion within 12 and 24 h, respectively (Table 4). CES is usually recognized as a surgical urgency. However, while the current evidence supports improved functional outcomes of surgery within 48 h for patients with CES, the benefits of earlier surgery (<24 h) are more controversial [27,28,29,30,31,32]. Of note, the traumatic etiology is usually not addressed separately in these studies. For tCCS without osteoligamentous instability, in turn, we observed a heterogeneous practice among Latin American spine surgeons, with only 31.5% of surgeons performing surgery within 24 h, 41.2% reporting that they do not operate during the same hospital stay, following-up these patients and performing surgery if there is no improvement in symptoms or deterioration. Ter Wengel et al. [22] as well as Fehlings et al. [23] also showed a heterogeneous and less urgent approach for these patients (Table 4). Not only the timing of surgery, but also the surgical management itself are controversial for tCCS without osteoligamentous instability, since patients can improve from baseline status during follow-up. In fact, a recent meta-analysis did not show superiority of the surgery versus conservative management as well as superiority of early over late surgery when this modality of treatment is chosen [33]. A clinical trial (NCT01485458 in ClinicalTrials.gov) evaluating early (<24 h) versus delayed surgery for cervical tSCI grade ASIA C without bone injury in patients with cervical canal stenosis is underway, which may help to guide future management. Despite the controversy and low quality of evidence, early surgery (<24 h) may be offered as an option for patients with acute tCCS according to recent AOSpine clinical practice guidelines [19].
According to the World Bank list of economies of June 2019, the majority of Latin American countries is considered middle-income, including the most populous ones. A very representative fraction of the countries’ populations is covered by public healthcare, being generally complemented by private healthcare [34, 35]. By covering a large portion of the population, public health services may be more subject to lack of advanced resources in the setting of tSCI (e.g. transport, ICU, dedicated spine surgeon, OR), potentially delaying the management. This can obviously vary among countries and even among regions of each country [36, 37]. Disparity among public and private health practices among patients with tSCI was observed in Latin America: surgeons practicing in public hospitals were less likely to operate on spine trauma with neurological involvement within 24 h (Table 2). Surprisingly, we did not identify any association between practice (public versus private) and self-reported obstacles to early surgery. Possibly our study lacks power to detect statistically significant differences in this issue. Of note, the majority of surgeons reported a mixed practice including the public and private sector, and only 12.7% working only in the public healthcare system. We believe that this issue has to be better evaluated taking into consideration the differences of healthcare systems among Latin American countries.
Awareness and education are important in clinician’s adherence to healthcare guidelines [38]. However, we acknowledge that specific clinical practice guidelines should be implemented in Latin America in order to improve tSCI care, and these guidelines have to take into consideration the barriers for early surgery presented in each region. As the evidence for early surgery continues to improve [14], it is important to better educate health professionals that manage SCI. In our study, fellowship-trained spine surgeons were more likely to operate patients with incomplete tSCI ASIA C/D and tCES within 24 h, compared to surgeons who did not have a spine fellowship. Similar findings were identified among Dutch surgeons with spine specialization who more often preferred to operate tSCI patients within 24 h, regardless of injury severity (i.e. ASIA score), when compared to their non-specialized colleagues [22].
A mismatch of ideal versus actual timing of performing surgery for this population was observed in other international surveys (Table 4) [20, 22,23,24]. In Latin America, the majority of spine surgeons (85.4%) reported that they would like to operate earlier on their patients with tSCI (Fig. 2). On the other hand, a similar survey with 88 Dutch neurosurgeons showed that 62.5% (55/88) would not perform surgery for any type of tSCI in a more urgently than they actually do [22]. This discrepancy may be explained by the differences in healthcare systems and society.
Several studies have investigated reasons for surgical delay in tSCI in developed countries. Thompson et al. [39] observed that surgical delay in tSCI (>24 h after injury) was mainly healthcare-related such as delay in transfer to the SCI center, delay before surgical plan completion (i.e. image exams), and waiting time for the operating room in the province of Quebec, Canada. In their analysis of 93 tSCI cases, no patient-related factors such as severity of trauma (i.e. Injury Severity Score), severity of injury (i.e. ASIA score) or age were related to surgical delay. Similar findings were reported by other authors [40, 41]. Glennie et al. [20] evaluated reasons for surgical delay in Canada. They identified the following reasons: lack of operating room availability (52%), delayed transport of patients from place of injury or other centers to the SCI center (28%), medical condition of patient (7%), lack of specialized operating room nursing teams (3%), and lack of surgeon availability on call (3%). Surprisingly, the most commonly reported obstacle for early surgical intervention among Latin American spine surgeons was access to spine implants, being pointed by more than 2/3 of them. Also, 37.3% reported having issues with OR availability, anesthesiology or ICU (Fig. 3). Interestingly, there were different complains according to surgical specially; in general neurosurgeons were more likely to report difficulty with spine implants than orthopedists, and orthopedists were more likely to report lack of OR availability (Table 3). It is possible that the historical differences in spine practice between these specialties still have an impact on current implant availability for neurosurgery programs.
We acknowledge that this survey presents limitations. First, despite the relatively large sample size, the participants may not represent the entire contingent of orthopedic surgeons and neurosurgeons that deal with acute SCI in the continent. However, our results certainly provide a baseline assessment and will be important for future comparisons. Second, the reported surgical timing might not always correspond to the actual timing in daily practice [20]. However, the present survey reflects the opinion of Latin American spine surgeons on current practice. In fact, there is a need to establish clinical registries in Latin America in order to gather better information on current practices for spine injuries [42].
Conclusions
This survey identified current practice regarding surgical timing in patients with spine trauma presenting with SCI, CES, and CCS. Latin American spine surgeons clearly have different approaches according to severity of injury (i.e. ASIA score). They tend to operate earlier on patients with CES and incompete tSCI, compared to patients with complete tSCI and tCCS. Spine fellowship-training was associated with a higher likelihood of indicating early surgery for incomplete tSCI and tCES. Besides education, professionals working in public health systems were less likely to operate within 24 h. We identified healthcare resources obstacles for early surgery for SCI in Latin America such as access to spine implants, OR, anesthesia team and ICU.
Data archiving
The data and analyses performed in this study are available from the corresponding author on request.
References
Shah M, Peterson C, Yilmaz E, Halalmeh DR, Moisi M. Current advancements in the management of spinal cord injury: a comprehensive review of literature. Surg Neurol Int. 2020;11:2.
Facchinello Y, Richard-Denis A, Beausejour M, Thompson C, Mac-Thiong JM. The use of classification tree analysis to assess the influence of surgical timing on neurological recovery following severe cervical traumatic spinal cord injury. Spinal Cord. 2018;56:687–94.
Fehlings MG, Vaccaro A, Wilson JR, Singh A, D WC, Harrop JS, et al. Early versus delayed decompression for traumatic cervical spinal cord injury: results of the Surgical Timing in Acute Spinal Cord Injury Study (STASCIS). PLoS One. 2012;7:e32037.
Wilson JR, Singh A, Craven C, Verrier MC, Drew B, Ahn H, et al. Early versus late surgery for traumatic spinal cord injury: the results of a prospective Canadian cohort study. Spinal Cord. 2012;50:840–3.
Dvorak MF, Noonan VK, Fallah N, Fisher CG, Finkelstein J, Kwon BK, et al. The influence of time from injury to surgery on motor recovery and length of hospital stay in acute traumatic spinal cord injury: an observational Canadian cohort study. J Neurotrauma. 2015;32:645–54.
Wilson JR, Jaja BNR, Kwon BK, Guest JD, Harrop JS, Aarabi B, et al. Natural history, predictors of outcome, and effects of treatment in thoracic spinal cord injury: a multi-center cohort study from the North American Clinical Trials Network. J Neurotrauma. 2018;35:2554–60.
Bourassa-Moreau E, Mac-Thiong JM, Li A, Ehrmann Feldman D, Gagnon DH, Thompson C, et al. Do patients with complete spinal cord injury benefit from early surgical decompression? Analysis of neurological improvement in a prospective cohort study. J Neurotrauma. 2016;33:301–6.
Ter Wengel PV, De Witt Hamer PC, Pauptit JC, van der Gaag NA, Oner FC, Vandertop WP, et al. Early surgical decompression improves neurological outcome after complete traumatic cervical spinal cord injury: a meta-analysis. J Neurotrauma. 2019;36:835–44.
Grassner L, Wutte C, Klein B, Mach O, Riesner S, Panzer S, et al. Early decompression (<8 h) after traumatic cervical spinal cord injury improves functional outcome as assessed by spinal cord independence measure after one year. J Neurotrauma. 2016;33:1658–66.
Wutte C, Klein B, Becker J, Mach O, Panzer S, Strowitzki M, et al. Earlier decompression (<8 h) results in better neurological and functional outcome after traumatic thoracolumbar spinal cord injury. J Neurotrauma. 2019;36:2020–7.
Kim M, Hong SK, Jeon SR, Roh SW, Lee S. Early (</=48 h) versus Late (>48 h) surgery in spinal cord injury: treatment outcomes and risk factors for spinal cord injury. World Neurosurg. 2018;118:e513–e25.
Lee DY, Park YJ, Song SY, Hwang SC, Kim KT, Kim DH, et al. The importance of early surgical decompression for acute traumatic spinal cord injury. Clin Orthop Surg. 2018;10:448–54.
O’Boynick CP, Kurd MF, Darden BV 2nd, Vaccaro AR, Fehlings MG. Timing of surgery in thoracolumbar trauma: is early intervention safe? Neurosurg Focus. 2014;37:E7.
Badhiwala JH, Wilson JR, Witiw CD, Harrop JS, Vaccaro AR, Aarabi B, et al. The influence of timing of surgical decompression for acute spinal cord injury: a pooled analysis of individual patient data. Lancet Neurol. 2021;20:117–26.
Mac-Thiong JM, Feldman DE, Thompson C, Bourassa-Moreau E, Parent S. Does timing of surgery affect hospitalization costs and length of stay for acute care following a traumatic spinal cord injury? J Neurotrauma. 2012;29:2816–22.
Furlan JC, Craven BC, Massicotte EM, Fehlings MG. Early versus delayed surgical decompression of spinal cord after traumatic cervical spinal cord injury: a cost-utility analysis. World Neurosurg. 2016;88:166–74.
Badhiwala JH, Ahuja CS, Fehlings MG. Time is spine: a review of translational advances in spinal cord injury. J Neurosurg Spine. 2018;30:1–18.
Roquilly A, Vigue B, Boutonnet M, Bouzat P, Buffenoir K, Cesareo E, et al. French recommendations for the management of patients with spinal cord injury or at risk of spinal cord injury. Anaesth Crit Care Pain Med. 2020;39:279–89.
Fehlings MG, Tetreault LA, Wilson JR, Aarabi B, Anderson P, Arnold PM, et al. A clinical practice guideline for the management of patients with acute spinal cord injury and central cord syndrome: recommendations on the timing (</=24 h Versus >24 h) of decompressive surgery. Glob Spine J 2017;7:195S–202S. 3 Suppl
Glennie RA, Bailey CS, Tsai EC, Noonan VK, Rivers CS, Fourney DR, et al. An analysis of ideal and actual time to surgery after traumatic spinal cord injury in Canada. Spinal Cord. 2017;55:618–23.
Ahn H, Singh J, Nathens A, MacDonald RD, Travers A, Tallon J, et al. Pre-hospital care management of a potential spinal cord injured patient: a systematic review of the literature and evidence-based guidelines. J Neurotrauma. 2011;28:1341–61.
Ter Wengel PV, Feller RE, Stadhouder A, Verbaan D, Oner FC, Goslings JC, et al. Timing of surgery in traumatic spinal cord injury: a national, multidisciplinary survey. Eur Spine J. 2018;27:1831–8.
Fehlings MG, Rabin D, Sears W, Cadotte DW, Aarabi B. Current practice in the timing of surgical intervention in spinal cord injury. Spine. 2010;35:S166–73. 21 Suppl
Werndle MC, Zoumprouli A, Sedgwick P, Papadopoulos MC. Variability in the treatment of acute spinal cord injury in the United Kingdom: results of a national survey. J Neurotrauma. 2012;29:880–8.
Grassner L, Wutte C, Klein B, Mach O, Riesner S, Panzer S, et al. Early Decompression (<8 h) after traumatic cervical spinal cord injury improves functional outcome as assessed by spinal cord independence measure after one year. J Neurotrauma. 2016;33:1658–66.
Burke JF, Yue JK, Ngwenya LB, Winkler EA, Talbott JF, Pan JZ, et al. Ultra-Early (<12 h) surgery correlates with higher rate of American Spinal Injury Association impairment scale conversion after cervical spinal cord injury. Neurosurgery. 2019;85:199–203.
Hogan WB, Kuris EO, Durand WM, Eltorai AEM, Daniels AH. Timing of surgical decompression for Cauda Equina Syndrome. World Neurosurg. 2019;132:e732–e8.
Busse JW, Bhandari M, Schnittker JB, Reddy K, Dunlop RB. Delayed presentation of cauda equina syndrome secondary to lumbar disc herniation: functional outcomes and health-related quality of life. Can J Emerg Med. 2015;3:285–91.
Ahn UM, Ahn NU, Buchowski JM, Garrett ES, Sieber AN, Kostuik JP. Cauda Equina Syndrome secondary to lumbar disc herniation: a meta-analysis of surgical outcomes. Spine 2000;25:1515–22.
Qureshi A, Sell P. Cauda equina syndrome treated by surgical decompression: the influence of timing on surgical outcome. Eur Spine J. 2007;16:2143–51.
Heyes G, Jones M, Verzin E, McLorinan G, Darwish N, Eames N. Influence of timing of surgery on Cauda equina syndrome: outcomes at a national spinal centre. J Orthop. 2018;15:210–5.
DeLong WB, Polissar N, Neradilek B. Timing of surgery in cauda equina syndrome with urinary retention: meta-analysis of observational studies. J Neurosurg Spine. 2008;8:305–20.
Yelamarthy PKK, Chhabra HS, Vaccaro A, Vishwakarma G, Kluger P, Nanda A, et al. Management and prognosis of acute traumatic cervical central cord syndrome: systematic review and Spinal Cord Society-Spine Trauma Study Group position statement. Eur Spine J. 2019;28:2390–407.
Atun R, de Andrade LOM, Almeida G, Cotlear D, Dmytraczenko T, Frenz P, et al. Health-system reform and universal health coverage in Latin America. Lancet. 2015;385:1230–47.
Machado CV. Políticas de Saúde na Argentina, Brasil e México: diferentes caminhos, muitos desafios. Ciência Saúde Coletiva. 2018;23:2197–212.
Basu S, Andrews J, Kishore S, Panjabi R, Stuckler D. Comparative performance of private and public healthcare systems in low- and middle-income countries: a systematic review. PLoS Med. 2012;9:e1001244–e.
Jin K, Zhang H, Seery S, Fu Y, Yu S, Zhang L, et al. Comparing public and private emergency departments in China: Early evidence from a national healthcare quality survey. Int J Health Plann Manag. 2020;35:581–91.
Cabana MD, Rand CS, Powe NR, Wu AW, Wilson MH, Abboud PA, et al. Why don’t physicians follow clinical practice guidelines? A framework for improvement. JAMA 1999;282:1458–65.
Thompson C, Feldman DE, Mac-Thiong JM. Surgical management of patients following traumatic spinal cord injury: Identifying barriers to early surgery in a specialized spinal cord injury center. J Spinal Cord Med. 2018;41:142–8.
Furlan JC, Tung K, Fehlings MG. Process benchmarking appraisal of surgical decompression of spinal cord following traumatic cervical spinal cord injury: opportunities to reduce delays in surgical management. J Neurotrauma. 2013;30:487–91.
Samuel AM, Bohl DD, Basques BA, Diaz-Collado PJ, Lukasiewicz AM, Webb ML, et al. Analysis of delays to surgery for cervical spinal cord injuries. Spine. 2015;40:992–1000.
Falavigna A, Dozza DC, Teles AR, Wong CC, Barbagallo G, Brodke D, et al. Current status of worldwide use of patient-reported outcome measures (PROMs) in spine care. World Neurosurg. 2017;108:328–35.
Acknowledgements
AO Spine Latin America.
Author information
Authors and Affiliations
Contributions
ART contributed to designing the study, elaboration of questions, statistical analysis, data extraction and interpretation and writing of the report. MBR contributed to data interpretation, confection of tables and figures, and writing of the report. OR contributed to designing the study, elaboration of questions, data interpretation, and provided feedback on the report. AF: contributed to designing the study, elaboration of questions, data interpretation, and provided feedback on the report.
Corresponding author
Ethics declarations
Competing interests
Alisson R. Teles received consulting fees from Medtronic, outside the submitted work.
Statement of ethics
We certify that all applicable institutional and governmental regulations concerning the ethical use of human volunteers were followed during the course of this research.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Teles, A.R., Ramos, M.B., Righesso, O. et al. Surgical timing in traumatic spinal cord injury: current practice and obstacles to early surgery in Latin America. Spinal Cord 60, 368–374 (2022). https://doi.org/10.1038/s41393-022-00789-8
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41393-022-00789-8
This article is cited by
-
Spinal cord injury: molecular mechanisms and therapeutic interventions
Signal Transduction and Targeted Therapy (2023)
-
Early surgical intervention for acute spinal cord injury: time is spine
Acta Neurochirurgica (2023)
