
Abstract
Study design
Retrospective epidemiological study.
Objectives
Since the causes and incidences of traumatic spinal cord injury (TSCI) in each country change over time, up-to-date epidemiological studies are required for countermeasures against TSCI. However, no nationwide survey in Japan has been conducted for about 30 years. The purpose of this study was therefore to investigate the recent incidence and characteristics of TSCI in Japan.
Setting
Japan
Methods
Survey sheets were sent to all hospitals (emergency and acute care hospitals) that treated TSCI persons in Japan in 2018 and case notes were retrospectively reviewed. Frankel grade E cases were excluded from analysis.
Results
The response rate was 74.4% (2804 of 3771 hospitals). The estimated annual incidence of TSCI excluding Frankel E was 49 per million, with a median age of 70.0 years and individuals in their 70s as the largest age group. Male-to-female ratio was 3:1. Cervical cord injuries occurred in 88.1%. Frankel D was the most frequent grade (46.3%), followed by Frankel C (33.0%). The most frequent cause was fall on level surface (38.6%), followed by traffic accident (20.1%). The proportion of fall on level surface increased with age. TSCI due to sports was the most frequent cause in teenagers (43.2%).
Conclusions
This nationwide survey in Japan showed that estimated incidence of TSCI, rate of cervical cord injury, and incomplete injury by falls appear to be increasing with the aging of the population.
Similar content being viewed by others

Introduction
Traumatic spinal cord injury (TSCI) can lead to life-long severe dysfunction as complete or incomplete paraplegia/tetraplegia and is sometimes life-threatening due to recurrent complications including pneumonia, severe decubitus, and urinary tract infection. This results in huge medical expenses for continued management of cases, and prevention of TSCI is therefore a very important socio-economic issue. Due to advances in medical technology, cutting-edge medical treatments such as spinal cord regeneration and robotic rehabilitation for TSCI have just begun to be introduced to overcome this pathological condition [1,2,3]. However, a long time will be required to establish these treatment strategies for all individuals with TSCI. Prevention of TSCI based on epidemiological studies is therefore an urgent issue as a realistic countermeasure.
According to a 2014 literature review initiated by the International Spinal Cord Society Prevention Committee, the global-incident rate of TSCI in 2007 was estimated as 23 cases per million (179,312 cases per annum) [4]. The incidence varies according by country and region, due to differences such as social background. A systematic review on the worldwide incidence of TSCI published in 2015 [5], consisting of data from 41 individual countries, showed that the incidence of TSCI ranged from 3.6 per million in a subnational study in Canada [6] to 195.4 per million in a subnational study in Ireland [7]. If data available for review [5] are limited to nationwide surveys or national registries, the incidence of TSCI ranges from 5.1 per million in Pakistan [8] to 71 per million in Brazil [9]. However, just as the causes and incidence of TSCI vary from region to region or country to country, the cause and incidence change over time due to changes in population and socio-economic development, requiring up-to-date and detailed epidemiological studies in each country and region.
Japan is aging rapidly and is now the most aging country in the world, with the highest rate of individuals ≥65 years old, at 28.1% in 2018 [10]. However, in Japan, no nationwide epidemiological survey on TSCI has been reported since the 1990–1992 survey [11], when the elderly population ≥65 years old comprised 12.1–13.1% (http://www.stat.go.jp/english/data/jinsui/2.html). The purpose of this nationwide study in Japan was therefore to investigate the current demographic and epidemiologic characteristics of persons with TSCI in Japan, with reference to age distribution, sex, cause of injury, neurological level of injury, and injury severity. This nationwide survey was an initiative of the Japan Medical Society of Spinal Cord Lesion.
Methods
We hypothesized that the causes, incidence, and characteristics of TSCI in Japan have changed with the continued aging of society, compared to the data surveyed about 30 years ago [11]. The present study was a nationwide multicenter retrospective study. Acutely hospitalized or emergency-treated TSCI persons dated from January 1 to December 31 in 2018 were retrospectively investigated from all over Japan. Survey sheets were sent to a total of all 3771 secondary or tertiary medical facilities registered in the country as a hospital treating emergency patients or providing acute care.
Age, sex, date of injury, level of injury (cervical or thoracic/lumbar), presence of skeletal injury, cause of injury, neurological status, and primary treatment were investigated. Causes of TSCI were categorized as follows: traffic accident (four-wheeled vehicle, two-wheeled vehicle, bicycle, pedestrian); fall from ≥3 m (high fall); fall from <3 m (low fall); struck by object; sports; fall on level surface; fall downstairs or other [12]. Neurological severity at the time of injury was graded according to Frankel classification [13] for comparison with previous studies in Japan [11]. Individuals with non-TSCI such as delayed-onset paralysis following osteoporotic vertebral fractures, paralysis due to spinal or spinal cord tumor, infarction, infection, spontaneous epidural hematoma, or myelitis were excluded. Persons with Frankel E at the time of injury were also excluded from analysis.
Statistical analyses
According to the previous nationwide epidemiological study in Japan, the number of TSCI persons was estimated by dividing the number of registered TSCI persons by the response rate [11, 14]. The Mann–Whitney U test for continuous variables or Fisher’s exact test for categorical variables were used to compare cervical injuries with thoracic/lumbar injuries. Persons with both cervical and thoracic/lumbar injuries were excluded from comparative analyses. Statistical analyses were performed using IBM® computer software and SPSS® Statistics version 25.0 for Mac. Values of p < 0.05 were considered significant.
Results
Characteristics of the study group
Valid response rate was 74.4% (2804 of 3771 hospitals). The registered number of TSCI persons in 2018 was 4603. The total population of Japan in 2018 was 126.44 million. The estimated incidence of TSCI excluding Frankel E in 2018 for Japan was 49 per million, with a median age of 70.0 years and individuals in their 70s as the largest age group (Table 1). In this study, 74.4% of TSCI persons were male (male-to-female ratio, 3:1). In this population, the most frequent Frankel grade was D, seen in nearly half of persons (46.3%), followed by grades C, A, and B, in that order.
Overall rate of cervical cord injuries was 88.1% among study subjects (62.3% cervical TSCI without skeletal injury, 25.8% with skeletal injury). Among cervical TSCI, cervical cord injuries without skeletal injuries occurred in 70.7% of persons (Table 1).
Causes of TSCI
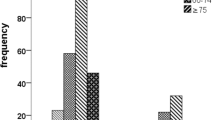
The most frequent cause of overall TSCI was fall on level surface (38.6%), followed by traffic accident (20.1%) (Table 1). Causes of TSCI by age group are shown in Fig. 1. Sports-related injuries were the most frequent in teenagers (43.2%). The proportion of fall on level surface markedly increased with age. Among the five major causes of TSCI, traffic accident, low fall, fall on level surface, and fall downstairs showed a peak in the 70–79-year-old age group, and high fall showed a peak at 60–69 years (Table 2).

Sports-related injuries were the most frequent in teenagers (43.2%). The proportion of fall on level surface increased with age.
The most frequent cause of traffic accidents was four-wheeled vehicles (46.3%), followed by two-wheeled vehicles (26.6%) (Fig. 2). The most frequent cause of TSCI due to sports was skiing (11.9%), followed by cycle sports (10.4%), snowboarding (8.9%), rugby (8.9%), and surfing (8.9%) (Fig. 3). TSCI due to swimming (diving) only comprised 4.4% of sports-related injuries.

The most frequent cause of traffic accidents was four-wheeled vehicles (46.3%), followed by two-wheeled vehicles (26.6%).

The most frequent cause of TSCI due to sports was skiing (11.9%), followed by cycle sports (10.4%), snowboarding (8.9%), rugby (8.9%), and surfing (8.9%).
Comparison between cervical injuries and thoracic/lumbar injuries
Median age was significantly higher for cervical injuries than for thoracic/lumbar injuries (p < 0.001) (Table 3). The most frequent cause of cervical injury was fall on level surface, and the most frequent cause of thoracic/lumbar injury was high fall. Proportions of traffic accident, high fall, struck by object, fall on level surface, and fall downstairs differed significantly between groups (p < 0.05). The proportion of Frankel A was significantly higher for thoracic/lumbar injuries than for cervical injuries (p < 0.001), while the proportion of Frankel D was significantly higher for cervical injuries than for thoracic/lumbar injuries (p < 0.001). The proportion of conservative treatment as primary care was significantly higher for cervical injuries than for thoracic/lumbar injuries (p < 0.001).
Discussion
Global trends of TSCI
TSCI is almost always a catastrophic event that changes the quality of life of the individual from the moment of injury. In particular, if TSCI victims are of working age, TSCI exerts not only a negative impact on quality of life, but also significant socio-economic consequences. A review article published in 2014 on the global incidence rate of TSCI estimated that TSCI in developed (high-income) and developing countries primarily affects males at 18–32 years old, and in developed countries, due to the aging population, affects males and females ≥65 years old [4]. That review article also reported that global changes in the proportion of TSCI from land transport are decreasing/stable in developed countries, but increasing in developing countries due to trends in transition to motorized transport, poor infrastructure, and regulatory challenges. Conversely, TSCIs from low falls in the elderly are increasing in developed countries with aging populations [4]. In fact, according to an analysis of survey data from the United States Nationwide Inpatient Sample databases for 1993–2012, including a total of 63,109 persons with TSCI, the percentage of spinal cord injury associated with falls increased significantly from 28% [95% confidence interval (CI), 26–30%] in 1997–2000 to 66% (95% CI, 64–68%) in 2010–2012 in those ≥65 years old (p < 0.001) [15].
According to a recent systematic review of time-related changes in total TSCI incidence in countries around the world, a decreasing/stable incidence of TSCI is seen in Australia, Austria, Canada, France, Iceland, New Zealand, Turkey, and the United States, whereas TSCI is increasing in Ireland, Italy, Norway, Russia, Saudi Arabia, Spain, and Taiwan [5]. Decreasing/stable TSCI in the first group of countries might be a consequence of preventive strategies. That systematic review speculated that the increase in incidence of TSCI in the latter countries may be due to improved recognition, registration, and health care systems [5]. However, epidemiological data on TSCI have not been studied in many countries worldwide [4, 5]. The United States, Australia, Canada, and high-income European countries have been noted to provide various valuable reports of TSCI based on spinal registry data, while African and Asian countries still lack appropriate epidemiologic data on TSCI [5]. A review study comparing TSCIs around the world have shown that Japan (assigned as a high-income region) has the highest proportion of tetraplegia in the world [4]. However, the Japanese data used in this review were over 20 years old [11], since Japan has no recent nationwide epidemiological data on TSCI.
Changes to TSCI in Japan
The first nationwide epidemiological survey for TSCI in Japan reported by Shingu et al. was conducted by the Japan Medical Society of Paraplegia as a compilation data of 1990–1992 data [11]. Following this initial nationwide survey, several studies of TSCI incidence in specific areas of Japan have been conducted [12, 16]. However, no nationwide survey of TSCI in Japan has been conducted since the 1990–1992 survey, and the present study offers an updated nationwide survey after an interval of about 30 years. The present study set survey items in common with the first nationwide survey to facilitate direct comparison. Therefore, for the assessment of severity, we adopted the Frankel grade [13] as used in the first survey.
Table 4 summarizes the key variables from other initial nationwide surveys [11] and the present study. In both surveys, the neurological level of TSCI was most often located in the cervical segments (75.0% and 88.1%, respectively). Severity in accordance with Frankel grade A was most common in 1990–1992 [11], while Frankel grade D was the most common in the current survey. In addition, proportions of leading cause differ between surveys. In the initial nationwide survey, the leading cause of TSCI was traffic accidents (43.7%), followed by falls from heights (28.9%) and fall on level surface (12.9%) [11], while in the present study, the leading cause of TSCI was fall on level surface (38.6%), followed by traffic accidents (20.1%) and a fall from height (13.7% low fall, 10.2% high fall, respectively). In the present study, falls on level surfaces increased gradually with age. These differences seemed to be caused by the rapidly progressing aging of society in Japan.
In Japan, the elderly population is still increasing rapidly and the proportion of the elderly ≥65 years in Japan is now the highest in the world [16]. The percentage of the elderly population in Japan, defined as individuals ≥65 years old, was 12.1–13.1% in 1990–1992 (http://www.stat.go.jp/english/data/jinsui/2.html), and the estimated incidence of TSCI in those years was 39–41 per million, with a main peak at 59 years old, and an additional smaller peak at 20 years old according to the first nationwide survey [11]. In the present study, the estimated incidence of TSCI was 49 per million, with one peak in the eighth decade, when the percentage of the Japanese elderly population ≥65 years old was 28.1% in 2018. These results suggest that in current Japan, the most advanced aging country in the world, the incidence of total TSCI, and the rate of cervical TSCI have increased, with falls as the most common cause of TSCI.
We recently investigated the incidence and characteristics of TSCI persons with injuries dating from 2012 to 2016 in Akita prefecture of Japan, which has a population of 1.06 million (2012) to 1.01 million (2016) (~0.8% of the Japanese population) [16]. Akita is the fastest aging society in Japan. The proportion of elderly individuals ≥65 years old in Akita has been increasing more rapidly (from 30.4% in 2012 to 34.6% in 2016) than the mean in Japan. The percentage of the population of Akita ≥65 years old is estimated to be the same as that of the average in Japan 20 years from now. In our previous study, the leading cause of TSCI was falls on level surface (32.1%) and the rate is comparable with the current nationwide survey, but the incidence of TSCI was 86 per million in Akita, higher than in the current survey (49 per million). These data suggest the possibility that TSCI will increase as society ages.
The current survey also found that some preventive measures identified in previous epidemiological survey were useful. TSCI due to diving during swimming was conspicuously high (21.6% of sports injuries) in the past [11, 17], but had been markedly reduced in the current survey (4.4%). This preventive effect of swimming-related TSCI was considered as a result of notifying the public of the risk of diving by the Japan Medical Society of Paraplegia after the previous survey.
Preventive measures for TSCI in aged society
Preventing TSCI requires various technological advances to prevent traffic accidents and occupational accidents, improvement of work and social environments, and sports safety measures. However, in Japan with its rapidly advancing aged society, the present study confirmed that there is an urgent need to take measures to prevent TSCI caused by falls in the elderly.
Japan is a racially homogeneous nation of people with a relatively narrow spinal canal [18]. Japanese are thus considered to have a high risk of cervical TSCI caused by minor trauma of the cervical spine due to falls [16]. In fact, a retrospective investigation of 122 consecutive Japanese persons with cervical TSCI without bone injury showed that pre-existing severe cervical spinal cord compression due to spinal canal stenosis was significantly associated with more severe paralysis on multivariate analysis (odds ratio 5.3, 95% CI 1.5–24.1, p = 0.01) [19]. Therefore, it had been hypothesized that the risk of cervical TSCI due to falls increases with aging in Japan. The present study provides strong evidence supporting this hypothesis. Indeed, the present study showed that 88.1% of TSCIs affect the cervical segments.
To prevent the fall-related cervical TSCIs that often occur in the elderly, several measures such as preventive decompression surgery and fall-prevention measures including exercise therapy can be considered. However, to date, little evidence exists for prophylactic decompression surgery for cervical TSCI [20, 21]. Studies have suggested that the utility of prophylactic decompression surgery for persons with asymptomatic or mildly symptomatic cervical stenosis to prevent TSCI is still inadequate [20, 21].
On the other hand, evidence strongly suggests that therapeutic exercise programs reduce the rate of falls and the number of people experiencing falls in older people living in the community [22]. A recent systematic review and meta-analysis of the elderly has shown that exercise reduces the rate of falls by 23% (rate ratio, 0.77; 95% CI, 0.71–0.83), and reduces the number of people experiencing one or more falls by 15% (risk ratio 0.85, 95% CI 0.81–0.89) [22].
However, limits exist to fall prevention by exercise therapy. In particular, in the case of elderly individuals for whom physical function has deteriorated significantly, exercise therapy alone cannot prevent falls. A recent meta-analysis examined the effects of various fall prevention measures on elderly people in care facilities and hospitals, and did not show any significant fall prevention effect from exercise [23]. To prevent falls in these elderly people, not only exercise therapy, but also multifactorial interventions including improvement of living environment and enhancement of assistance are also necessary.
Strengths and limitations of this study
The strengths of this study were the nationwide study design, the satisfactory response rate, and the very low level of missing data, suggesting the reliability of our findings. However, several limitations need to be mentioned. First, because this study was retrospective in design, 100% of the data had not been collected. The hospitals that responded to the questionnaire and those others that did not answer might thus have differed in terms of the scale and number of TSCI patients treated. In the present study, the estimated number of TSCIs was calculated using the simple method adopted in the previous nationwide study in Japan, since we needed to compare numbers between surveys. However, in future surveys, more detailed estimation regarding this concern should be addressed. Second, since this was the first nationwide survey in about 30 years, regular time point changes since 30 years ago could not be investigated. Establishment of a prospective registry system for TSCI in Japan is anticipated.
Conclusions
In conclusion, a comprehensive nationwide survey of TSCI in 2018 was conducted in Japan for the first time in about 30 years and the recent incidence and characteristics of TSCI are presented. The estimated incidence of TSCI, rate of cervical cord injuries, and incomplete injuries by falls appear to be increasing because of the aging of the population.
Data availability
The datasets used in this study are publicly available.
Change history
02 September 2020
This article has had values in Table 1 and Table 4 updated. These updates do not affect the integrity of the data, but improve the clarity of the tables.
References
Assinck P, Duncan GJ, Hilton BJ, Plemel JR, Tetzlaff W. Cell transplantation therapy for spinal cord injury. Nat Neurosci. 2017;20:637–47.
Tsuji O, Sugai K, Yamaguchi R, Tashiro S, Nagoshi N, Kohyama J, et al. Concise review: laying the groundwork for a first-in-human study of an induced pluripotent stem cell-based intervention for spinal cord injury. Stem Cells. 2019;37:6–13.
Cheung EYY, Ng TKW, Yu KKK, Kwan RLC, Cheing GLY. Robot-assisted training for people with spinal cord injury: a meta-analysis. Arch Phys Med Rehabil. 2017;98:2320–31.
Lee BB, Cripps RA, Fitzharris M, Wing PC. The global map for traumatic spinal cord injury epidemiology: update 2011, global incidence rate. Spinal Cord. 2014;52:110–6.
Jazayeri SB, Beygi S, Shokraneh F, Hagen EM, Rahimi-Movaghar V. Incidence of traumatic spinal cord injury worldwide: a systematic review. Eur Spine J. 2015;24:905–18.
Tator CH, Duncan EG, Edmonds VE, Lapczak LI, Andrews DF. Changes in epidemiology of acute spinal cord injury from 1947 to 1981. Surg Neurol. 1993;40:207–15.
Roche SJ, Sloane PA, McCabe JP. Epidemiology of spine trauma in an Irish regional trauma unit: a 4-year study. Injury. 2008;39:436–42.
Raja IA, Vohra AH, Ahmed M. Neurotrauma in Pakistan. World J Surg. 2001;25:1230–7.
Masini M. An estimation of incidence and prevalence of spinal cord injury in Brazil. J Bras Neurocir. 2001;12:97–100.
Saiki S. Population. In: Statistics Bureau Ministry of Internal Affairs and Communications Japan, editor. Statistical handbook of japan 2019. Tokyo: Statistics Bureau; 2019. pp. 10.
Shingu H, Ohama M, Ikata T, Katoh S, Akatsu T. A nationwide epidemiological survey of spinal cord injuries in Japan from January 1990 to December 1992. Paraplegia. 1995;33:183–8.
Katoh S, Enishi T, Sato N, Sairyo K. High incidence of acute traumatic spinal cord injury in a rural population in Japan in 2011 and 2012: an epidemiological study. Spinal Cord 2014;52:264–7.
Frankel HL, Hancock DO, Hyslop G, Melzak J, Michaelis LS, Ungar GH, et al. The value of postural reduction in the initial management of closed injuries of the spine with paraplegia and tetraplegia. I. Paraplegia. 1969;7:179–92.
Hashimoto S, Fukutomi K, Nagai M, Nakamura Y, Yanagawa H, Sasaki R, et al. Response bias in the nationwide epidemiological survey of an intractable disease in Japan. J Epidemiol. 1991;1:27–30.
Jain NB, Ayers GD, Peterson EN, Harris MB, Morse L, O’Connor KC, et al. Traumatic spinal cord injury in the United States, 1993-2012. JAMA. 2015;313:2236–43.
Kudo D, Miyakoshi N, Hongo M, Kasukawa Y, Ishikawa Y, Ishikawa N, et al. An epidemiological study of traumatic spinal cord injuries in the fastest aging area in Japan. Spinal Cord. 2019;57:509–15.
Katoh S, Shingu H, Ikata T, Iwatsubo E. Sports-related spinal cord injury in Japan (From the nationwide spinal cord injury registry between 1990 and 1992). Spinal Cord. 1996;34:416–21.
Yukawa Y, Kato F, Suda K, Yamagata M, Ueta T. Age-related changes in osseous anatomy, alignment, and range of motion of the cervical spine. Part I: radiographic data from over 1,200 asymptomatic subjects. Eur Spine J. 2012;21:1492–8.
Oichi T, Oshima Y, Okazaki R, Azuma S. Preexisting severe cervical spinal cord compression is a significant risk factor for severe paralysis development in patients with traumatic cervical spinal cord injury without bone injury: a retrospective cohort study. Eur Spine J. 2016;25:96–102.
Takao T, Morishita Y, Okada S, Maeda T, Katoh F, Ueta T, et al. Clinical relationship between cervical spinal canal stenosis and traumatic cervical spinal cord injury without major fracture or dislocation. Eur Spine J. 2013;22:2228–31.
Wu JC, Ko CC, Yen YS, Huang WC, Chen YC, Liu L, et al. Epidemiology of cervical spondylotic myelopathy and its risk of causing spinal cord injury: a national cohort study. Neurosurg Focus. 2013;35:E10.
Sherrington C, Fairhall NJ, Wallbank GK, Tiedemann A, Michaleff ZA, Howard K, et al. Exercise for preventing falls in older people living in the community. Cochrane Database Syst Rev. 2019;1:CD012424.
Cameron ID, Dyer SM, Panagoda CE, Murray GR, Hill KD, Cumming RG, et al. Interventions for preventing falls in older people in care facilities and hospitals. Cochrane Database Syst Rev. 2018;9:CD005465.
Acknowledgements
The authors wish to thank all doctors (Drs Satoko Matsumoto, Hiroshi Taneichi, Satoshi Inami, Hirotaka Chikuda, Masao Koda, Katsunori Yoshinaga, Masaya Nakamura, Osahiko Tsuji, Takashi Asazuma, Yoshiyuki Yato, Tsunehiko Konomi, Masahiko Watanabe, Shinji Kimura, Hideaki Nakajima, Toshiyuki Takahashi, Jun Takahashi, Hiroki Oba, Masakazu Takayasu, Eiichi Saitoh, Hideki Nagashima, Tadao Morino, Tadanori Ogata, Takeshi Maeda and Takayoshi Ueta) for their help in data collection.
Funding
This study was supported by Japan Medical Society of Spinal Cord Lesion.
Author information
Authors and Affiliations
Contributions
NM and DK analyzed the data, prepared, and revised paper content. KS, HS, YN, YM, SS, TT, AT, and HT designed this study and collected the data. SK and YS designed and oversaw the study and were responsible for conclusions.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
This study was performed in accordance with the Declaration of Helsinki. However, this study did not require ethics committee approval because information in this study was anonymized in an unlinkable manner before analysis. These methods conform to the Ethical Guidelines for Medical and Health Research Involving Human Subjects in Japan.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
About this article

Cite this article
Miyakoshi, N., Suda, K., Kudo, D. et al. A nationwide survey on the incidence and characteristics of traumatic spinal cord injury in Japan in 2018. Spinal Cord 59, 626–634 (2021). https://doi.org/10.1038/s41393-020-00533-0
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41393-020-00533-0
This article is cited by
-
Epidemiology features of traumatic and non-traumatic spinal cord injury in China, Wuhan
Scientific Reports (2024)
-
Trend differences in cervical spinal cord injuries before and after the coronavirus disease 2019 pandemic
Spinal Cord Series and Cases (2024)
-
Traumatic spinal cord injury in South Korea for 13 years (2008–2020)
Scientific Reports (2024)
-
Effects of the walking independence on lower extremity and trunk muscle activity during straight-leg raising following incomplete cervical cord injury
Scientific Reports (2024)
-
Impact of malnutrition on mortality and neurological recovery of older patients with spinal cord injury
Scientific Reports (2024)
