
Abstract
Current international tables published on the glycaemic index (GI) of foods represent valuable resources for researchers and clinicians. However, the vast majority of published GI values are of Western origin, notably European, Australian and North American. Since these tables focus on Western foods with minimal inclusion of other foods from non-Western countries, their application is of limited global use. The objective of this review is to provide the GI values for a variety of foods that are consumed in non-Western countries. Our review extends and expands on the current GI tables in an attempt to widen its application in many other regions of the world.
Similar content being viewed by others

Introduction
In many non-Western countries, cereal-based carbohydrates provide ~60% of total energy intake1 compared with 42% for Caucasians2. The consumption of such high-carbohydrate diets yield high glucose and insulin response, thus contributing to insulin resistance. Nonetheless, the quality of carbohydrate consumed is as important as the quantity. Poor quality carbohydrates are quickly digested and absorbed, thereby giving rise to high blood glucose and insulin ‘spikes’. Observational studies have shown that the consumption of low glycaemic index (GI) foods is associated with a lower risk of type 2 diabetes mellitus (T2DM)3, significantly less insulin resistance and a lower prevalence of the metabolic syndrome4. However, the vast majority of these published GI values are of European, Australian and North America origin.
Glycaemic index
The GI is defined as a numerical figure used to represent the ability of a carbohydrate food to raise blood glucose levels. It is expressed as a percentage of the incremental area under the glycaemic response curve (AUC) elicited by a portion of food containing 50 g available carbohydrate in comparison with the AUC elicited by a standard reference food of 50 g glucose or white bread in the same participant5. The principle is that the slower the rate of carbohydrate absorption into the bloodstream, the lower the rise of blood glucose level and the lower the GI value. A GI value of ≥70 is considered high, a GI value 56–69 inclusive is medium and a GI value ≤55 is low, where glucose = 100.
Following the approach of these authors, we are for the first time providing a compendium of GI values of non-Western foods6. Since many of these GI values were published in uncommon journals or located in various sources, it is not surprising that many previous authors may have found it a challenge to access and retrieve such information.
With a global pandemic of T2DM escalating, especially in emerging countries7, it is now recognised that the GI food-based intervention is an important tool in the management and prevention of T2DM8. Ironically, in regions of the world where there is a pandemic of T2DM, there is a shortage of a taxonomy of GI data of non-Western foods (e.g. Middle East, South Asia, Indian sub-continent) in contrast to the current international GI tables6,9.
In 1997, the FAO/WHO Expert Consultation suggested that the concept of GI might provide a useful means of helping to select the most appropriate carbohydrate-containing foods for the maintenance of health and the treatment of several diseases10. A meta-analysis by Brand-Miller et al11. demonstrated that choosing low GI foods in place of conventional or high GI foods exhibited a small but clinically important effect on medium-term glycaemic control in patients with diabetes. Low GI foods have been shown to reduce insulin demand and lipid concentrations, improve blood glucose control and reduce body weight, thus preventing diabetes-related cardiovascular events12,13,14,15.
A typical non-Western diet, such as in South Asia, is high in carbohydrates with cereals such as polished rice, white flour, finger millet, semolina and wheat providing the bulk of the energy16. Furthermore, it has been shown that a unique metabolic feature of South Asians, for an identical carbohydrate load, elicits postprandial glucose peaks that are 2–3 times larger than Caucasians17,18,19. Hence, a compilation of the GI of non-Western foods is necessary for proper selection and modifications that may be of particular benefit to not only these groups of people but to a wider audience.
The objective of this review is, therefore, to consolidate the GI values for a variety of foods that are consumed in non-Western countries. This is in order to capture and encapsulate all the data available on GI that have not been reported in the general literature. Given that the largest preponderance of type 2 diabetes is in Asia, the Middle East, South America and parts of Africa, it is imperative that the database on GI is expanded in order for it to have global utility. With this in mind, papers were critically evaluated based on a strict criterion. The emphasis of this review has inevitably been to record and document the GI of various foods.
Research design and method
We conducted a comprehensive literature search for relevant, original articles published from January 2000 through May 2020. Since 2000 marked the exponential growth in GI testing in non-Western countries, we have decided to take this as the year of data analysis. Briefly, the following string of search terms was used in PubMed and Google Scholar, with no language or other restrictions: (glycaemic index) AND (foods) AND (‘country’). The electronic search was supplemented by manual searches through the reference sections of selected publications, as well as with linked articles that were found to have cited these particular publications. Non-Western countries included in this search were as follows: Singapore, Malaysia, Indonesia, Brunei, Cambodia, Thailand, Japan, Korea, China, Taiwan, Hong Kong, Nepal, India, Myanmar, Vietnam, Sri Lanka, Philippines, United Arab Emirates, Yemen, Oman, Saudi, Qatar, Kuwait, Lebanon, Egypt, Pakistan and Bangladesh. The compiled GI studies in our article have utilised the recommended GI testing method10,20 and fulfilled the minimum requirements for the following inclusion criteria for GI testing studies: minimum 10 participants (healthy/T2DM), instruments such as Yellow Spring Instruments (YSIs) and the use of handheld glucometers such as HemoCue® and other similar devices widely used in clinical studies for GI testing, amount of available carbohydrate and reference food (glucose/white bread/white rice). In the table, most of the foods are based on 50 g available carbohydrate. However, for foods with low to moderate carbohydrate density, it is justified by Brouns et al.20 to use a lower amount of carbohydrate to prevent consumption of an excessively large amount of food. Finally, the GI of non-Western foods were grouped according to the countries. The food list was arranged according to the country of origin so as to allow individuals who are keener on knowing the GI variability of foods from their own country to retrieve this information conveniently.
Results
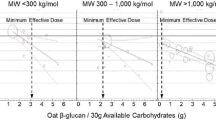
Table 1 lists 940 food items, citing 159 separate studies, representing reliable data derived from healthy subjects or individuals with type 2 diabetes. Figure 1 shows a flow diagram indicating a number of studies screened, excluded and included in this article. Non-Western countries included in this compilation were as follows: Singapore, Malaysia, Thailand, Indonesia, Philippines, Japan, Korea, China, Taiwan, Hong Kong, India, Sri Lanka, Emirates, Oman, Saudi and Lebanon. These countries were chosen based on published studies on GI from these locations, with validated methodologies used and the papers followed the inclusion criteria as described in our paper. The GI of non-Western foods was firstly arranged according to the country it was derived from. This was followed by the food item, the GI, serving size (if any), available carbohydrate portion, subject type and number, and lastly the reference food with time period of GI testing. An important feature of our paper is to encourage readers to interpret the data in a way that will enable them to select healthy foods from the GI range of foods available. Therefore, using the data generated from our GI tables, the illustrative example presented below are simple methods that may be adapted to reduce the GI values of carbohydrate-rich staples (Fig. 2).

N - number of studies, ISO - International Organisation for Standardisation, FAO - Food and Agriculture Organisation.

Figure shows how combination of food ingredients and foods may be used to reduce the glycaemic response of rice-based staples.
Conclusion
We believe that the inclusion of the additional GI values of foods from non-Western countries will enhance the use and application of GI both in research and clinical practice. Many of the staples consumed in these regions are high in GI, notably rice, flatbread, noodles, buns, paus, pastries and so on. The use of these GI tables will also enable consumers to make informed choices on how best to select low GI foods. The GI data compiled in this article consists of both single and mixed meals. This is a major advance to many GI tables that have focused on single foods. Mixed meals in this region are complex in relation to ingredients used and taste. Given its complexity, our table that includes the GI of mixed meals is a major advantage. It is hoped that this compendium will further stimulate additional data collection and enhance the utility of GI tables for a worldwide audience.
References
Cui, Z. & Dibley, M. J. Trends in dietary energy, fat, carbohydrate and protein intake in Chinese children and adolescents from 1991 to 2009. Br. J. Nutr. 108, 1292–1299 (2012).
Mulla, U. Z., Cooper, R., Mishra, G. D., Kuh, D. & Stephen, A. M. Adult macronutrient intake and physical capability in the MRC National Survey of Health and Development. Age Ageing 42, 81–87 (2013).
Schulze, M. B. et al. Glycemic index, glycemic load, and dietary fiber intake and incidence of type 2 diabetes in younger and middle-aged women. Am. J. Clin. Nutr. 80, 348–356 (2004).
McKeown, N. M. et al. Carbohydrate nutrition, insulin resistance, and the prevalence of the metabolic syndrome in the Framingham Offspring Cohort. Diabetes Care 27, 538–546 (2004).
Jenkins, D. et al. Glycemic index of foods: a physiological basis for carbohydrate exchange. Am. J. Clin. Nutr. 34, 362–366 (1981).
Atkinson, F. S., Foster-Powell, K. & Brand-Miller, J. C. International tables of glycemic index and glycemic load values: 2008. Diabetes care 31, 2281–2283 (2008).
IDF. IDF Diabetes Atlas 9th edn (IDF, 2020).
Kelley, D. E. Sugars and starch in the nutritional management of diabetes mellitus. Am. J. Clin. Nutr. 78, 858S–864SS (2003).
Foster-Powell, K., Holt, S. H. & Brand-Miller, J. C. International table of glycemic index and glycemic load values: 2002. Am. J. Clin. Nutr. 76, 5–56 (2002).
FAO/WHO. Carbohydrates in human nutrition: report of a joint FAO/WHO expert consultation. FAO Food Nutr. Pap. 66, 1–140 (1998).
Brand-Miller, J., Hayne, S., Petocz, P. & Colagiuri, S. Low–glycemic index diets in the management of diabetes: a meta-analysis of randomized controlled trials. Diabetes Care 26, 2261–2267 (2003).
Rizkalla, S. W. et al. Improved plasma glucose control, whole-body glucose utilization, and lipid profile on a low-glycemic index diet in type 2 diabetic men: a randomized controlled trial. Diabetes care 27, 1866–1872 (2004).
Salmeron, J. et al. Dietary fiber, glycemic load, and risk of NIDDM in men. Diabetes Care 20, 545–550 (1997).
Salmeron, J. et al. Dietary fiber, glycemic load, and risk of noninsulin-dependent diabetes mellitus in women. JAMA 277, 472–477 (1997a).
Liu, S. et al. A prospective study of dietary glycemic load, carbohydrate intake, and risk of coronary heart disease in US women. Am. J. Clin. Nutr. 71, 1455–1461 (2000).
Holmboe-Ottesen, G. & Wandel, M. Changes in dietary habits after migration and consequences for health: a focus on South Asians in Europe. Food Nutr. Res. 56, 18891 (2012).
Dickinson, S., Colagiuri, S., Faramus, E., Petocz, P. & Brand-Miller, J. Postprandial hyperglycemia and insulin sensitivity differ among lean young adults of different ethnicities. J. Nutr. 132, 2574–2579 (2002).
Venn, B., Williams, S. & Mann, J. Comparison of postprandial glycaemia in Asians and Caucasians. Diabet. Med. 27, 1205–1208 (2010).
Henry, C. et al. Glycaemic index of common foods tested in the UK and India. Br. J. Nutr. 99, 840–845 (2008).
Brouns, F. et al. Glycaemic index methodology. Nutr. Res. Rev. 18, 145–171 (2005).
Chia, M. The glycaemic index and glycaemic load of snack foods consumed by healthy adults. J. Obes. Weight Loss Ther. S2, 2–4 (2012).
Sun, L., Ranawana, D. V., Leow, M. K.-S. & Henry, C. J. Effect of chicken, fat and vegetable on glycaemia and insulinaemia to a white rice-based meal in healthy adults. Eur. J. Nutr. 53, 1719–1726 (2014).
Tan, V., Wu, T., Henry, C. & Lee, Y. S. Glycaemic and insulin responses, glycaemic index and insulinaemic index values of rice between three Asian ethnic groups. Br. J. Nutr. 113, 1228–1236 (2015).
Sun, L. et al. Glycaemic index and glycaemic load of selected popular foods consumed in Southeast Asia. Br. J. Nutr. 113, 843–848 (2015).
Sun, L., Wei Jie Tan, K. & Jeyakumar Henry, C. Co-ingestion of essence of chicken to moderate glycaemic response of bread. Int. J. Food Sci. Nutr. 66, 931–935 (2015).
Soong, Y. Y., Quek, R. Y. C. & Henry, C. J. Glycemic potency of muffins made with wheat, rice, corn, oat and barley flours: a comparative study between in vivo and in vitro. Eur. J. Nutr. 54, 1281–1285 (2015).
Sun, L., Tan, K. W. J., Han, C. M. S., Leow, M. K.-S. & Henry, C. J. Impact of preloading either dairy or soy milk on postprandial glycemia, insulinemia and gastric emptying in healthy adults. Eur. J. Nutr. 56, 77–87 (2017).
Tey, S. L., Lee, D. E. M. & Henry, C. J. Fruit form influences postprandial glycemic response in elderly and young adults. J. Nutr. Health Aging 21, 887–891 (2017).
Tan, W. S. K. et al. The glycaemic index and insulinaemic index of commercially available breakfast and snack foods in an Asian population. Br. J. Nutr. 119, 1151–1156 (2018).
Camps, S. G. et al. Co-ingestion of rice bran soymilk or plain soymilk with white bread: effects on the glycemic and insulinemic response. Nutrients 10, 449 (2018).
Sun, L., Tan, K. W. J., Lim, J. Z., Magkos, F. & Henry, C. J. Dietary fat and carbohydrate quality have independent effects on postprandial glucose and lipid responses. Eur. J. Nutr. 57, 243–250 (2018).
Mohd Yusof, B. N., Abd, Talib, R., Karim, N. A., Kamarudin, N. A. & Arshad, F. Glycaemic index of four commercially available breads in Malaysia. Int. J. Food Sci. Nutr. 60, 487–496 (2009).
Robert, W. et al. Determination of the glycaemic index of selected Malaysian foods. Int. Med. J. 13, 255 (2006).
Robert, S. D., Ismail, A. A., Winn, T. & Wolever, T. M. Glycemic index of common Malaysian fruits. Asia Pac. J. Clin. Nutr. 17, 35–39 (2008).
Karupaiah, T. et al. A transgressive brown rice mediates favourable glycaemic and insulin responses. J. Sci. Food Agric. 91, 1951–1956 (2011).
Robert, S. D. & Ismail, A. A.-S. Glycemic responses of patients with type 2 diabetes to individual carbohydrate-rich foods and mixed meals. Ann. Nutr. Metab. 60, 27–32 (2012).
Ishak, W. R. W., Zin, C. A. J. C. M. & Robert, S. D. Young corn ear addition improves some nutrients and lowering Glycemic Index of chiffon cake. Food Nutr. Sci. 5, 1545–1553 (2014).
Nicholas, D., Hazila, K., Chua, H. & Rosniyana, A. Nutritional value and glycemic index of Bario rice varieties. J. Trop. Agric. Food Sci. 42, 1–8 (2014).
Jeevetha, S., Nisak, M., Ngan, H.-B., Ismail, A. & Azlan, A. Relationship between amylose content and glycemic index of commonly consumed white rice. IOSR J. Agric. Vet. Sci. 7, 12–18 (2014).
CAJCM, Zin, Robert, S. D. & Ishak, W. R. W. Effect of biscuits and muffins added with cornlettes powder on the glycemic responses of healthy individuals. Food Nutr. Sci. 5, 2195 (2014).
Robert, S. D., Ismail, A. A.-S. & Rosli, W. I. W. Reduction of postprandial blood glucose in healthy subjects by buns and flatbreads incorporated with fenugreek seed powder. Eur. J. Nutr. 55, 2275–2280 (2016).
Se, C.-H., Chuah, K.-A., Mishra, A., Wickneswari, R. & Karupaiah, T. Evaluating crossbred red rice variants for postprandial glucometabolic responses: a comparison with commercial varieties. Nutrients 8, 308 (2016).
Ng, S. H., Robert, S. D., WANW, Ahmad & WRW, Ishak Incorporation of dietary fibre-rich oyster mushroom (Pleurotus sajor-caju) powder improves postprandial glycaemic response by interfering with starch granule structure and starch digestibility of biscuit. Food Chem. 227, 358–368 (2017).
Osman, N. M. H., Mohd-Yusof, B.-N. & Ismail, A. Estimating glycemic index of rice-based mixed meals by using predicted and adjusted formulae. Rice Sci. 24, 274–282 (2017).
Sabeetha, S., Nisak, M. & Amin, I. Glycemic index of selected watermelon (Citrullus lanatus). Int. Food Res. J. 25, 2547–2552 (2018).
Abu Bakar, N. A. F., Abd Rashid, A. A., Ishak, M. F. & Jalil, A. M. M. Glycemic index of starch-based foods commonly consumed in Terengganu. Malays. Appl. Biol. 48, 129–138 (2019).
Drewnowski, A. et al. Sugars and sweeteners: science, innovations, and consumer guidance for Asia. Asia Pac. J. Clin. Nutr. 28, 645 (2019).
Supparmaniam, H., Hussin, N. & Jalil, A. M. M. Glycaemic index, palatability, acceptability and perceived satiety of cookies prepared with durian (Durio zibethinus murr.) and β-glucan. Malays. Appl. Biol. 48, 89–99 (2019).
Amiruddin, N., Zahary, M., Bhaskar, R. & Mhd Jalil, A. Glycaemic index, palatability and acceptability of energy drinks prepared with β-glucan and whey protein. Food Res. 4, 421–430 (2020).
Chapagai, M. K. et al. Glycaemic index values and physicochemical properties of five brown rice varieties cooked by different domestic cooking methods. Funct. Foods Health Dis. 6, 506–518 (2016).
Nounmusig, J., Kongkachuichai, R., Sirichakwal, P., Wongwichain, C. & Saengkrajang, W. Glycemic index, glycemic load and serum insulin response of alternative rice noodles from mixed sago palm flour (Metroxylon spp.) and chiang rice flour. Burapha Sci. J. 23, 839–851 (2018).
Chusak, C., Pasukamonset, P., Chantarasinlapin, P. & Adisakwattana, S. Postprandial glycemia, insulinemia, and antioxidant status in healthy subjects after ingestion of bread made from anthocyanin-rich riceberry rice. Nutrients 12, 782 (2020).
Kongkachuichai, R., Charoensiri, R., Meekhruerod, A. & Kettawan, A. Effect of processing conditions on bioactive compounds and glycemic index of the selected landrace rice variety in pre-diabetes. J. Cereal Sci. 102994 (2020).
Marsono, Y. Glycemic index of selected Indonesian starchy foods. Indonesian Food Nutri. Progr. 8, 15–20 (2001).
Marsono, Y. Indeks Glisemik Umbi-Umbian (Gycemic index of tuber foods). Agritech 22, 13–16 (2002).
Marsono, Y., Wiyono, P. & Noor, Z. INDEKS GLISEMIK KACANG-KACANGAN [Glycemic index of selected legumes]. J. Teknol. dan. Ind. Pangan 13, 211 (2002).
Marsono, Y. & PTdS, Kanoni Snap bean (Phaseolus vulgaris) and Yardlong bean (Vigna sesquipedalis): glycemic index and its hypoglycemic effect in Sprague Dawley rats. Biota X, 183–191 (2005).
Hasan, V., Astuti, S. & Susilawati, S. Indeks glikemik oyek dan tiwul dari umbi garut (Marantha arundinaceae L.), suweg (Amorphallus campanullatus BI) dan singkong (Manihot utillisima). J. Teknol. Ind. Has. Pertan. 16, 34–50 (2012).
Astawan, M., Wresdiyati, T., Widowati, S. & Saputra, I. Aplikasi Tepung Bekatul Fungsional Pada Pembuatan Cookies Dan Donat Yang Bernilai Indeks Glikemik Rendah (Application of functional bran in making cookies and donuts with low glycemic index value). J. Pangan 22, 385–394 (2013).
Idril, N. I., Diana, A. & Wargahadibrata, A. F. Preliminary study: glycemic index of brown and white rice variant IR64 in healthy adult men. Int. J. Integr. Health Sci. 1, 37–41 (2013).
Jailani, F., Kusumawardani, S., Puspitasari, C., Maula, A. & Purwandari U. Annealled purple yam (Dioscorea alata var. purpurea) flour improved gelatinisation profile, but increased glycemic index of substituted bread. Int. Food Res. J. 20, 865–871 (2013).
Rimbawan, R. & Nurbayani, R. Nilai indeks glikemik produk olahan gembili (Dioscorea esculenta). J. Gizi dan. Pangan 8, 145–150 (2013).
Avianty. S. & Ayustaningwarno, F. Indeks glikemik snack bar ubi jalar kedelai hitam sebagai alternatif makanan selingan penderita diabetes melitus tipe 2. J. Aplikasi Teknol. Pangan 3, 98–102 (2014).
Pentadini, F., Silvia, A., Sri Hartini, A. T. (eds). Determination of glycemic score on processed food from whole wheat flour (Triticum aestivum L.) Dewata’s variety in terms of amylose content and starch digestibility. In International Conference on Research, Implementation and Education of Mathematics and Sciences. C55–62 (2014).
Haryani, A., Andini, S. & Hartini, S. Kadar gizi, pati resisten, dan indeks glikemik biskuit gandum utuh (Triticum aestivum L) varietas DWR-1621. J. Teknol. Pangan dan. Has. Pertan. 12, 1–12 (2015).
Diniyah, N., Firdaus, L., Windrati, W. S., Prasetyo, A. & Subagio, A. Indeks Glikemik Beras Analog dari Mocaf dengan Substitusi Jagung. Ubi Jalar Ungu dan. Wortel. War. Ind. Has. Pertan. 33, 66–73 (2016).
Indrastati, N. & Anjani, G. Snack Bar Kacang Merah Dan Tepung Umbi Garut Sebagai Alternatif Makanan Selingan Dengan Indeks Glikemik Rendah. J. Nutr. Coll. 5, 546–554 (2016).
Kurniawati, M., Budijanto, S. & Yuliana, N. D. Karakterisasi dan indeks glikemik beras analog berbahan dasar tepung jagung. J. Gizi dan. Pangan 11, 169–174 (2016).
Wijanarka, A., Sudargo, T., Harmayani, E. & Marsono, Y. Changes in resistant starch content and glycemic index of pre-gelatinized gayam (Inocarfus fagifer Forst.) flour. Pakistan J. Nutr. 15, 649–654 (2016).
Hidayat, B., Akmal, S., Muslihudin, M. & Suhada, B. Assessment of corn-based rice analogues made from modified corn flour and cassava starch which processed by granulation method as functional food. Assessment 61, 19–24 (2017).
Lestari, L. A., Huriyati, E. & Marsono, Y. The development of low glycemic index cookie bars from foxtail millet (Setaria italica), arrowroot (Maranta arundinacea) flour, and kidney beans (Phaseolus vulgaris). J. Food Sci. Technol. 54, 1406–1413 (2017).
Nurjanah, N., Julianti, E. D. & Sahara, E. Aplikasi Pati Aren Termodifikasi Ekstrak Daun Jambu Biji Merah Dalam Pengembangan Produk Berindeks Glikemik Rendah (Applications of arenga starch modified with red guava leaf extract in development of a low glycemic index product). Nutr. Food Res. 39, 75–86 (2017).
Putri, S. Kajian Aktivitas Indeks Glikemik Brownies Kukus Substitusi Tepung Ubi Jalar Termodifikasi. J. Kesehat. 8, 18–29 (2017).
Saputrie, A., Murwani, R. & Johan, A. Low glycemic index noodle snack from yellow sweet potato (Ipomoea Batatas) and pumpkin (Cucurbita Moschata) blend. Int. Conference on Translational Medicine and Health Sci. 1, 121–127 (2017).
Trisnawati, W. Analisis Indeks Glikemik dan Komposisi Gizi Keripik Simulasi Substitusi Tepung Bekatul dengan Tepung Labu Kuning. J. Aplikasi Teknol. Pangan 6, 143–147 (2017).
Karimuna, S. R., Paridah, P. & Jufri, N. Penentuan indeks glikemik sikkato (sinonggi, kasuami, kambuse dan kabuto) pada subjek non diabetes mellitus. Preventif J. 3, 1–5 (2018).
Lestari, O. & Purwayantie, S. The glycemic index and organoleptic test of Pekawai (Durio kutejensis) chips. Pro Food 3, 235–239 (2018).
Nugraheni, M., Hamidah, S. & Auliana, R. Glycemic index of Coleus tuberosus crackers rich in resistant starch type III. Int. Food Res. J. 25, 314–320 (2018).
Susanti, A., Wijanarka, A. & Nareswara, A. S. Penentuan indeks glikemiks dan beban glikemik pada cookies tepung beras merah (Oryza nivara) dan biji kecipir (Psophocarpus tetragonolobus L). Ilmu Gizi Indones. 2, 69–78 (2018).
Yulianto, W., Suryani, C., Susiati, A. & Luwihana, S. Evaluation of chromium fortified-parboiled rice coated with herbal extracts: resistant starch and glycemic index. Int. Food Res. J. 25, 2608–2613 (2018).
Arysanti, R. D., Sulistiyani, S. & Rohmawati, N. Indeks Glikemik, Kandungan Gizi, dan Daya Terima Puding Ubi Jalar Putih (Ipomoea batatas) dengan Penambahan Buah Naga Merah (Hylocereus polyrhizus). Amerta Nutr. 3, 107–113 (2019).
Agustia, F. C., Subardjo, Y. P., Ramadhan, G. R. & Betaditya, D. Glycemic index of flakes made from Mocaf-Black rice and bean flour as alternative snacks for people with type 2 diabetes mellitus. Ann. Trop. Public Health 22, S333 (2019).
Lestari, O. A. & Dewi, Y. S. K. (eds). Total consumption of honey which provides low response to glycemic index and glycemic load. Proc. Int. Conf. Food Agric. 1, 349–353 (2019).
Puspita, W., Sulaeman, A. & Damayanthi, E. Snack bar berbahan pati sagu (Metroxylon sp.), tempe, dan beras hitam sebagai pangan fungsional berindeks glikemik rendah. Indonesian J. Nutr. 8, 11–23 (2019).
Manullang, V. A., Rahadiyanti, A., Pratiwi, S. N. & Afifah, D. N. Glycemic index, starch, and protein digestibility in tempeh gembus cookies. J. Food Qual. 2020, 1–6 (2020).
Nurjanah, N., Muchtadi, D., Palupi, N. & Widowati, S. Chemical characteristics and glycemic index of processed products from corn starch modified with green tea polyphenols. EES 443, 012029 (2020).
Surayya, N. A. et al. Sifat organoleptik dan indeks glikemik produk sorgum bar yang diformulasi menggunakan berbagai jenis penyalut nira. J. Pangan dan. Agroindustri 8, 56–67 (2020).
Trinidad, T. P. et al. Glycaemic index of different coconut (Cocos nucifera)-flour products in normal and diabetic subjects. Br. J. Nutr. 90, 551–556 (2003).
Trinidad, T. P. et al. Glycemic index of Sunfibre (Cyamoposis tetragonolobus) products in normal and diabetic subjects. Int. J. Food Sci Technol. 39, 1093–1098 (2004).
Trinidad, T. P., Mallillin, A. C., Sagum, R. S. & Encabo, R. R. Glycemic index of commonly consumed carbohydrate foods in the Philippines. J. Funct. foods 2, 271–274 (2010).
Sugiyama, M., Tang, A., Wakaki, Y. & Koyama, W. Glycemic index of single and mixed meal foods among common Japanese foods with white rice as a reference food. Eur. J. Clin. Nutr. 57, 743–752 (2003).
Ito, Y. et al. Postprandial blood glucose and insulin responses to pre-germinated brown rice in healthy subjects. J. Med. Investig. 52, 159–164 (2005).
Oku, T. et al. Effects of cake made from whole soy powder on postprandial blood glucose and insulin levels in human subjects. Int. J. Food Sci. Nutr. 60, 224–231 (2009).
Oku, T., Nakamura, M. & Nakamura, S. Consideration of the validity of glycemic index using blood glucose and insulin levels and breath hydrogen excretion in healthy subjects. Int. J. Diabetes Mellitus 2, 88–94 (2010).
Sato, S. et al. Glycemic index and glucose utilization of rice vermicelli in healthy subjects. Biol. Pharm. Bull. 33, 1385–1393 (2010).
Taguchi, Y. et al. Evaluation of herbal foods on α-glucosidase activity and glycemic index. Food Sci. Technol. Res. 16, 39–44 (2010).
Nomura, N., Miyoshi, T., Hamada, Y. & Kitazono, E. Glycemic index of boiled BARLEYmax® in healthy Japanese subjects. J. Cereal Sci. 102959 (2020).
Yoshimoto, J. et al. Palatable noodles as a functional staple food made exclusively from yellow peas suppressed rapid postprandial glucose increase. Nutrients 12, 1839 (2020).
Ryu, J.-H. et al. Sugar composition and glycemic indices of frequently consumed fruits in Korea. Korean J. Nutr. 45, 192–200 (2012).
Kim, D.-Y., Kim, Y. & Lim, H. Glycaemic indices and glycaemic loads of common Korean carbohydrate-rich foods. Br. J. Nutr. 121, 416–425 (2019).
Yang, Y.-X. et al. Glycemic index of cereals and tubers produced in China. World J. Gastroenterol. 12, 3430 (2006).
Li, M. et al. Postprandial glycaemic and insulinaemic responses to GM-resistant starch-enriched rice and the production of fermentation-related H 2 in healthy Chinese adults. Br. J. Nutr. 103, 1029–1034 (2010).
Ren, X. et al. In vitro starch digestibility and in vivo glycemic response of foxtail millet and its products. Food Funct. 7, 372–379 (2016).
Shao, S.-y et al. Glycemic index, glycemic load, and glycemic response to pomelo in patients with type 2 diabetes. Curr. Med. Sci. 37, 711–718 (2017).
Zhu, R. et al. Postprandial glycaemic responses of dried fruit-containing meals in healthy adults: results from a randomised trial. Nutrients 10, 694 (2018).
Zhu, R. et al. Acute effects of non-homogenised and homogenised vegetables added to rice-based meals on postprandial glycaemic responses and in vitro carbohydrate digestion. Br. J. Nutr. 120, 1023–1033 (2018).
Zhu, R. et al. Acute effects of three cooked non-cereal starchy foods on postprandial glycemic responses and in vitro carbohydrate digestion in comparison with whole grains: a randomized trial. Nutrients 11, 634 (2019).
Lin, M.-H. A., Wu, M.-C., Lu, S. & Lin, J. Glycemic index, glycemic load and insulinemic index of Chinese starchy foods. World J. Gastroenterol. 16, 4973 (2010).
Lai, M. H. et al. Predicted glycemic index and glycemic index of rice varieties grown in Taiwan. Cereal Chem. 93, 150–155 (2016).
Yang, C.-H., Chang, C.-W. & Lin, J. White rice glycemic index measured in venous and capillary blood samples. Food Sci. Technol. Res. 23, 297–304 (2017).
Yang, C.-H., Lin, M.-H. A. & Lin J. The effect of adding Chinese food supplements to rice on glycemic response. Chiang Mai Univ. J. Nat. Sci. 16, 191–206 (2017).
Chen, Y.-J., Sun, F.-H., Wong, S. H.-s. & Huang, Y.-J. Glycemic index and glycemic load of selected Chinese traditional foods. World J. Gastroenterol. 16, 1512 (2010).
Lok, K. Y. et al. Glycaemic index and glycaemic load values of a selection of popular foods consumed in Hong Kong. The. Br. J. Nutr. 103, 556–560 (2010).
Bahado-Singh, P., Wheatley, A., Ahmad, M., Morrison, E. S. A. & Asemota, H. Food processing methods influence the glycaemic indices of some commonly eaten West Indian carbohydrate-rich foods. Br. J. Nutr. 96, 476–481 (2006).
Anju, T. & Sarita, S. Suitability of foxtail millet (Setaria italica) and barnyard millet (Echinochloa frumentacea) for development of low glycemic index biscuits. Malays. J. Nutr. 16, 361–368 (2010).
Megala, P. & Hymavathi, T. Inulin and fructooligosaccharides incorporated functional fruit bars. World Acad. Sci. Eng. Technol. 59, 600–605 (2011).
Premanath, M., Basavana Gowdappa, H., Mahesh, M., Suresh & Babu, M. A study of glycemic index of ten indian fruits by an alternate approach. E–Int. Sci. Int. Sci. Int. Sci. Res. J. Res. J. 3, 11–18 (2011).
Durgadevi, R. & Nazni, P. Comparative study of processed amaranth grains on glycemic indices in niddm subjects. Int. J. Pharm. Med. Biol. Sci. 1, 194–205 (2012).
Shobana, S. et al. Glycaemic index of three Indian rice varieties. Int. J. Food Sci. Nutr. 63, 178–183 (2012).
Bisht, A. & Srivastava, S. Efficacy of millets in the development of low glycemic index sweets for diabetics. Malays. J. Nutr. 19, 215–222 (2013).
Katare, C. & Sharma, S. Effect of dried bottle gourd pulp supplemented snacks on glycemic status of subjects in normal health. Int. J. Food Nutr. Sci. 2, 104 (2013).
Neelam, Y., Kanchan, C., Alka, S. & Alka, G. Evaluation of hypoglycemic properties of kodo millet based food products in healthy subjects. IOSR J. Pharm. 3, 14–20 (2013).
PriyankaSingh, N. Y., Mishra, P. K. & Sheikh, S. Utilization of rice bran for development of chapatti and its glycemic response in NIDDM patients. Int. Res. J. Pharm. Appl. Sci. 3, 244–248 (2013).
Srinivasa, D. et al. Glycaemic index (GI) of an Indian branded thermally treated Basmati rice variety: a multi centric study. J. Assoc. Phys. India 61, 716–720 (2013).
Bora, P. & Kulshrestha, K. Development of low glycemic index green gram husk incorporated fiber rich food products and their intervention for health benefits. Int. J. Food Nutr. Sci. 3, 196–203 (2014).
Chaturvedi, N., Shukla, K. & Singh, A. Post-prandial glucose response to ficus religiosa based products in normal subjects and their outcome on glycemic index. Int. J. Adv. Res. 2, 219–226 (2014).
Shukla, K. & Srivastava, S. Evaluation of finger millet incorporated noodles for nutritive value and glycemic index. J. Food Sci. Technol. 51, 527–534 (2014).
Beniwal, P. & Jood, S. Development of low glycemic index noodles by legume and cereal by-products incorporation. Int. J. Health Sci. Res. 5, 381–387 (2015).
Bora, P. & Kulshrestha, K. Fiber rich snack food products incorporated with green gram husk and their suitability for diabetics. Asian J. Dairy Food Res. 34, 300–306 (2015).
Eagappan, K., Mathew, M. M. & Sasikumar, S. Assessment of glycaemic index and glycaemic load in selected banana varieties. Int. J. Res. Health Sci. [Online] 3, 89–93 Available from: http://www.ijrhs.com/issues.php?val=Volume3&iss=Issue1.
Patil, K. B., Chimmad, B. V. & Itagi, S. Glycemic index and quality evaluation of little millet (Panicum miliare) flakes with enhanced shelf life. J. Food Sci. Technol. 52, 6078–6082 (2015).
Prasad, M. P. R., Rao, B. D., Kalpana, K., Rao, M. V. & Patil, J. V. Glycaemic index and glycaemic load of sorghum products. J. Sci. Food Agric. 95, 1626–1630 (2015).
Joshi, S. & Srivastava, S. Barnyard millet as a substitute of rice in preparation of khichdi for diabetics. Int. J. Sci. Res. 5, 1798–1802 (2016).
Mohan, V. et al. Glycemic Index of a Novel High-Fiber White Rice Variety Developed in India—A Randomized Control Trial Study. Diabetes Technol. Ther. 18, 164–170 (2016).
Narayanan, J., Sanjeevi, V., Rohini, U., Trueman, P. & Viswanathan, V. Postprandial glycaemic response of foxtail millet dosa in comparison to a rice dosa in patients with type 2 diabetes. Indian J. Med. Res. 144, 712–717 (2016).
Santhi Sirisha, K. & Vijaya Lakshmi, V. Estimation of glycemic index of ragi recipes incorporated with curry leaf powder. Int. J. Recent Adv. Multidiscip. Res. 3, 1936–1939 (2016).
Singh, P., Kulshrestha, K., Kumbhar, B. & Kumar, S. Study on glycemic indices of carrot enriched food products. Progress. Hortic. 48, 110–113 (2016).
Chaturvedi, N., Agarwal, A. & Raj, N. Glycemic indices of Kale leaves based chakli and twisters on normal human subjects. Int. J. Sci. Res. 6, 4 (2017).
Kaur, K., Kaur, H. & Bains, K. Development and nutritional evaluation of cereal and pulse based biscuits for diabetic patients. Br. J. Appl. Sci. Technol. 21, 1–8 (2017).
Kaur, K. Nutritional evaluation and glycemic response of extruded products developed from cereal pulse blends. Chem. Sci. Rev. Lett. 6, 939–946 (2017).
Shanmugam, S. et al. Even minimal polishing of an Indian parboiled brown rice variety leads to increased glycemic responses. Asia Pac. J. Clin. Nutr. 26, 829–836 (2017).
Vijayakumar, G. et al. Glycemic index (GI) and glycemic load (GL) of commonly used breakfast foods in Kerala. Asia Pac. J. Res. 2320, 5504 (2017).
Chaturvedi, N., Raj, N. & Agarwal, A. Value added Indian flat breads with Ashwagandha and its glycemic response among normal healthy subjects. Asian J. Dairy Food Res. 37, 73–76 (2018).
Chauhan, S. & Singh, U. Impact of processing on glycemic index of maize based flour under in vivo condition. J. Pharmacogn. Phytochem. 7, 2021–2023 (2018).
Chockaligam, A., Rao, D., Sarikonda, S., Reddy, K. & Reddy, D. Effect of DiaBliss Herbal Sugar (DHS) in patients with type-II diabetes mellitus. Int. J. Diabetes Res. 7, 31–35 (2018).
Korrapati, D. et al. Development of low glycemic index foods and their glucose response in young healthy non-diabetic subjects. Prev. Nutr. Food Sci. 23, 181 (2018).
Shobana, S. et al. Development and evaluation of nutritional, sensory and glycemic properties of finger millet (Eleusine coracana L.) based food products. Asia Pac. J. Clin. Nutr. 27, 84–91 (2018).
Tomer, V., Kaur, A., Kaur, A. & Kumar, A. Glycaemic index of Indian flatbreads (rotis) prepared using multigrain flour and whole wheat flour. Ann. Biol. 34, 143–147 (2018).
Joseph, J. Nutritional, glycemic and ecological assessment of green jackfruit for diabetes in Kerala. Int. J. Diabetes 1, 14–18 (2019).
RamyaBai, M. et al. Glycemic index and microstructure evaluation of four cereal grain foods. J. Food Sci. 84, 3373–3382 (2019).
Geetha, K., Yankanchi, G. M., Hulamani, S. & Hiremath, N. Glycemic index of millet based food mix and its effect on pre diabetic subjects. J. Food Sci. Technol. 57, 2732–2738 (2020).
Mammen, R. et al. Safety and influence of a novel powder form of coconut inflorescence sap on glycemic index and lipid profile. Bioact. Carbohydr. Diet. Fibre 23, 100217 (2020).
Hettiaratchi, U., Ekanayake, S. & Welihinda, J. Glycaemic indices of three Sri Lankan wheat bread varieties and a bread-lentil meal. Int. J. Food Sci. Nutr. 60, 21–30 (2009).
Widanagamage, R. D., Ekanayake, S. & Welihinda, J. Carbohydrate-rich foods: glycaemic indices and the effect of constituent macronutrients. Int. J. Food Sci. Nutr. 60, 215–223 (2009).
Pirasath, S., Thayaananthan, K., Balakumar, S. & Arasaratnam, V. Effect of dietary curries on the glycaemic index. Ceylon Med. J. 55, 118–122 (2010).
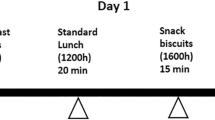
Hettiaratchi, U., Ekanayake, S., Welihinda, J. & Perera, M. Glycemic and insulinemic responses to breakfast and succeeding second meal in type 2 diabetics. Int. J. Diabetes Dev. Ctries 31, 199–206 (2011).
Hettiaratchi, U., Ekanayake, S. & Welihinda, J. Sri Lankan rice mixed meals: effect on glycaemic index and contribution to daily dietary fibre requirement. Malays. J. Nutr. 17, 97–104 (2011).
Hettiaratchi, U., Ekanayake, S. & Welihinda, J. Chemical compositions and glycemic responses to banana varieties. Int. J. Food Sci. Nutr. 62, 307–309 (2011).
Pirasath, S., Thayananthan, K., Balakumar, S. & Arasaratnam V. Effect of soluble fiber on glycaemic index. Galle Med. J. 17, 23–31 (2012).
Pirasath, S., Thayananthan, K., Balakumar, S. & Arasaratnam, V. Glycemic index values of some Jaffna fruits. Funct. Foods Health Dis. 2, 25–34 (2012).
Anuruddhika Subhashinie Senadheera, S. P. & Ekanayake, S. Green leafy porridges: how good are they in controlling glycaemic response? Int. J. Food Sci. Nutr. 64, 169–174 (2013).
Muthalib, A., Naser, K. A., Sivakanesan, R. & Nageeb, M. Effects of consumption of traditional Sri Lankan meals on glycaemic response in healthy individuals. Sri Lanka J. Diabetes Endocrinol. Metab. 4, 12–16 (2014).
Perera, M., Sivakanesan, R., Abeysekara, D. & Sarananda, K. Effect of vegetable mixed curry on glycaemic index and glycaemic load of soy flour incorporated traditional Sri Lankan breakfast foods in healthy adults. Pakistan J. Nutr. 13, 616–621 (2014).
Pirasath, S., Thayananthan, K., Balakumar, S. & Arasaratnam, V. Thosai mixed with side dishes altered the glycaemic index. Batticaloa Med. J. 6, 24–28 (2014).
Gunathilaka, M. & Ekanayake, S. Effect of different cooking methods on glycaemic index of Indian and Pakistani basmati rice varieties. Ceylon Med. J. 60, 57–61 (2015).
Pirasath, S., Balakumar, S. & Arasaratnam, V. Glycemic index of traditional foods in Northern Sri Lanka. Endocrinol. Metab. Synd. 4 (2015).
Senavirathna, R. M. I. S. K., Ekanayake, S. & Jansz, E. R. Traditional and novel foods from indigenous flours: nutritional quality, glycemic response, and potential use in food industry. Starch‐Stärke 68, 999–1007 (2016).
Manokaran, S. et al. Determination of glycaemic responses of low fat milk incorporated with whey proteins and oats powder. J. Clin. Nutr. Diet. 4, 1–4 (2018).
Prasantha, B. D. R. Glycemic index of four traditional red pigmented rice. Integr. Food Nutr. Metab. 5, 1–3 (2018).
Miller, C., Dunn, E. & Hashim, I. The glycaemic index of dates and date/yoghurt mixed meals. Are dates ‘candy that grows trees’?. Eur. J. Clin. Nutr. 57, 427–430 (2003).
Alkaabi, J. M. et al. Glycemic indices of five varieties of dates in healthy and diabetic subjects. Nutr. J. 10, 59 (2011).
Alkaabi, J., Al-Dabbagh, B., Saadi, H., Gariballa, S. & Yasin, J. Effect of traditional Arabic coffee consumption on the glycemic index of Khalas dates tested in healthy and diabetic subjects. Asia Pac. J. Clin. Nutr. 22, 565–573 (2013).
Al, Dhaheri et al. Glycaemic index and glycaemic load values of commonly consumed foods in the United Arab Emirates. Br. J. Nutr. 117, 1110–1117 (2017).
Jarrar, A. H., Kamal-Eldin, A., Bataineh, Ma & Al Dhaheri, A. S. Glycemic index (GI) and glycemic load (GL) values for dried bisr and tamr dates. Emir. J. Food Agric. (2019).
Ali, A., Al-Hakmani, M., Waly, M. & Essa, M. Glycemic index of commonly consumed snack foods in Oman. Int. J. Nutr. Pharmacol. Neurol. Dis. 10, 50–56 (2020).
Al-Mssallem, M. Q., Hampton, S. M., Frost, G. S. & Brown, J. E. A study of Hassawi rice (Oryza sativa L.) in terms of its carbohydrate hydrolysis (in vitro) and glycaemic and insulinaemic indices (in vivo). Eur. J. Clin. Nutr. 65, 627–634 (2011).
Al-Mssallem, M. Q. & Brown, J. E. Arabic coffee increases the glycemic index but not insulinemic index of dates. Saudi Med. J. 34, 923–928 (2013).
AlGeffari, M. A., Almogbel, E. S., Alhomaidan, H. T., El-Mergawi, R. & Barrimah, I. A. Glycemic indices, glycemic load and glycemic response for seventeen varieties of dates grown in Saudi Arabia. Ann. Saudi Med. 36, 397–403 (2016).
Daher, C., Farhat, A., Moukarzel, S. & El-Said, R. Glycemic index of commonly consumed Lebanese mixed meals and desserts. Asian J Clin. Nutr. 2, 48–57 (2010).
Acknowledgements
We thank A*STAR, International Medical University (IMU) and Wilmar International Limited for supporting this review. We would also like to thank Tan Le Sze (our student Intern) from the National University of Singapore for helping in the data collection. This study was supported by the Biomedical Science Institute Industry Alignment Fund (IAF-PP); Food Structure Engineering for Nutrition and Health (H17/01/a0/A11 and H18/01/a0/B11).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Henry, C.J., Quek, R.Y.C., Kaur, B. et al. A glycaemic index compendium of non-western foods. Nutr. Diabetes 11, 2 (2021). https://doi.org/10.1038/s41387-020-00145-w
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41387-020-00145-w
This article is cited by
-
The salivary microbiome shows a high prevalence of core bacterial members yet variability across human populations
npj Biofilms and Microbiomes (2022)
-
The interaction between glycemic index, glycemic load, and the genetic variant ADIPOQ T45G (rs2241766) in the risk of colorectal cancer: a case–control study in a Korean population
European Journal of Nutrition (2022)
