
Abstract
Mast cell sarcoma (MCS) is an exceedingly rare form of mastocytosis characterized by invasive malignant mast cell growth and metastatic potential. Diagnosis of MCS is very challenging due to its marked morphologic variations and significant immunophenotypic overlap with other neoplasms. In this study, we undertook an extensive study of 10 cases of MCS from our series, with review of additional 24 cases from the literature, to better clarify the clinicopathologic and molecular features of MCS. From the analyses of our 10 cases, MCS equally involved males and females with a median age of 54.5 years (range 1-63). The bone was the most common site of involvement, as noted in 9/10 of cases. Two patients had prior germ cell tumors (mediastinal germ cell tumor and ovarian dysgerminoma), and concurrent systemic mastocytosis was noted in one of nine patients. Serum tryptase levels were elevated in 6/7 of patients, and 3/9 of patients had mast cell activation symptoms. Morphologically, the tumor cells were typically large and pleomorphic with frequent reactive eosinophils. By immunohistochemical staining, MCS consistently expressed CD43 (8/8), CD117 (10/10), and mast cell tryptase (10/10), as well as CD13 (3/3) and CD33 (10/10), with variable positivity of CD2 (1/9), CD25 (4/9), CD30 (5/8), and CD68 (5/9). Notably, KIT D816V was not detected in nine cases in our study, although two cases had other mutations of KIT gene. Seven out of eight patients received chemotherapy with or without radiotherapy. However, the response was poor, and four out of eight patients died within a median follow-up interval of five months. Taken together, there are no standardized therapeutic regimens available for MCS at this time, and the prognosis is dismal. Therefore, it is critical to further investigate and characterize this rare entity, with the hope of improving diagnostic accuracy and providing more effective, targeted therapies.
Similar content being viewed by others

Introduction
Under the 2016 WHO Classification, mast cell sarcoma (MCS) is defined as an exceedingly rare neoplasm composed of destructive and highly atypical mast cells with poor prognosis.1 Since the first case report of MCS in humans by Horny et al. in 1986,2 only scattered single case reports and small case series have been documented in the English literature. Thus, limited information is available regarding the clinical features, pathologic characteristics, and molecular genetic alterations.
The diagnosis of MCS is particularly challenging due to its scarcity, variability in clinical presentation, absence of typical mast cell morphology, and significant immunophenotypic overlap with other hematologic neoplasms. Therefore, MCS is likely under-recognized. In contrast to systemic mastocytosis (SM), the imatinib resistant canonical KIT D816V mutation is often absent in MCS,3,4 and other molecular genetic features of this entity have not been well-characterized. Currently, there are no effective therapeutic options available; consequently, the overall survival of such patients is usually within months after diagnosis. Here we present 10 cases of MCS in our study, along with a comprehensive review of 24 additional cases from the literature.
Materials and methods
Case Selection
In our study, a total of 10 cases of MCS were collected from multiple institutions. The diagnosis of each case was confirmed with morphologic assessment as well as necessary ancillary studies.
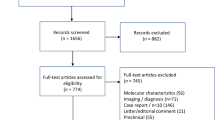
Case #2 to #4 were previously reported,5,6,7,8 and additional clinical history and/or materials were obtained for further studies. An extensive literature search was conducted in PubMed (http://www.ncbi.nlm.nih.gov/pubmed/), resulting in 24 additional cases of MCS retrieved from the English literature that were included in our review.2,3,4,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25 The clinical, radiologic, morphologic, immunophenotypic, and molecular genetic features, as well as treatment regimens and survival data, were collected in available cases and the detailed data are summarized in Supplementary Table 1.
Morphologic assessment
The morphology of the cases from our study and the literature was evaluated based upon the hematoxylin and eosin (H&E) stained slides or the images provided in peer-reviewed articles. The histologic and cytologic features assessed included: cell size [large (larger than the nuclei of histiocytes) or medium (similar size to the nuclei of histiocytes)]; cytologic atypia (degree of pleomorphism); nuclear shapes (round/oval, irregular, lobated, or other); chromatin (fine, coarse, or vesicular); cytoplasmic granules; mitotic figures [active (at least one per high-power-field) or low (less than one per high-power-field)]; presence of spindle cells; and reactive eosinophils.
Immunohistochemistry
The formalin-fixed and paraffin-embedded (FFPE) tissue blocks were sectioned at 4.0 μm for immunohistochemical (IHC) stains. The tissue sections were incubated at 60 °C for 2 h, and then the slides were deparaffinized in xylene twice, followed by 5 min each in 99.5% and 95% ethanol and 5 min in distilled water. After standard antigen retrieval, the tissue sections were stained for antibodies using automated platforms (Benchmark, Ventana Medical Systems Inc., Tucson, AZ, USA, and Bond Polymer Refine Detection system, Leica Biosystems Inc., Buffalo Grove, IL, USA) with an incubation time of 60 minutes. The major antibodies utilized for the 10 cases in our study are summarized in Table 1.
OncomineTM Dx mutational analysis
Mutational analyses were conducted using OncomineTM Comprehensive Assay Version 3 (Thermo Fisher Scientific Inc., Waltham, MA, USA) on our cases #1, #3 and #4. Tumor samples and corresponding normal control tissues were microdissected from FFPE tissue sections. Dual DNA and RNA isolations were performed (Qiagen Inc., Hilden, Germany, Maxwell® RSC by Promega, Madison, WI, USA). Isolated DNA was amplified using a modification of the Ion AmpliSeq™ Oncomine Comprehensive Assay Version 3 multiplex PCR primer sets. The isolated RNA was reverse transcribed into cDNA and subjected to multiplex PCR using the Ion AmpliSeq™ Oncomine Comprehensive Assay Version 3 primer sets for RNA. Amplicon sequencing was performed on an Ion S5™ XL next-generation sequencer (Thermo Fisher Scientific Inc., Waltham, MA, USA). The raw data generated were pre-processed within Torrent Suite (Thermo Fisher Scientific Inc.), with the alignment of sequencing reads performed by the Torrent Mapping (TMAP) algorithm. Variants identified by the Ion Reporter, MuTect2 and Strelka variant callers were passed through Ensembl Variant Effect Predictor to derive annotations from multiple genomic databases. Copy number variant (CNV) detection was performed using IonReporterTM (Thermo Fisher Scientific Inc.) and DNAcopy (Bioconductor). Both algorithms implement read depth-based CNV detection, where variations in read depth between the tumor and normal are used to determine regions of abnormal copy number. The complete list of specific gene variants tested is provided in Supplementary Table 2. The results of next-generation sequencing studies for cases #2, #8, #9, and #10 were provided by outside institutions.
Statistical analysis
A total of 30 cases of MCS with survival data were included in the statistical analysis, including 7 from our study and 23 from the literature. Survival was defined as months from diagnosis to death or last follow-up. Those alive at last follow-up were treated as censored. The Kaplan-Meier method was used to estimate overall distribution. GraphPad Prism software was used for this analysis (GraphPad Software, La Jolla, CA, USA).
Results
Results from our study
Clinical information
The major clinical features of the 10 cases of MCS in our study are summarized in Table 2. There were five males and five females with a median age of 54.5 years, ranging from 1 to 63 years. Patient #1 had a history of Lynch syndrome and uterine carcinoma 14 years prior to the diagnosis of MCS. Interestingly, two patients had prior germ cell tumors, including a mediastinal germ cell tumor 26 years prior to MCS diagnosis (patient #8) and an ovarian dysgerminoma 3 years prior (patient #10). Concurrent SM was noted in 1/9 patient (case #6). Three of nine patients had mast cell activation symptoms (MCAS), including but not limited to flushing, skin rashes, sweating, vomiting, diarrhea, and tachycardia.
The bone was the most common site of involvement, as noted in nine of 10 patients (Fig. 1A), and other locations included soft tissue (2 cases), spleen (2), brain (1), liver (1), lymph node (1), and lung (1). Serum tryptase levels were elevated in six of seven patients, with a median level of 132 ng/ml (range 34.1 to 1.034 ng/ml; normal reference range 0–11.4 ng/ml). The bone marrow was involved by MCS in 3/9 patients and positive for SM in 1/9 patients.

A PET scan shows tumor involvement in L2 and paraspinal soft tissue. Two biopsies from the same location on patient #1 display (B) blastoid cytology with high N/C ratio, medium size, and fine chromatin and (C) sarcomatous features with scattered multinucleated giant tumor cells. D Histiocytoid tumor cells with frequent bi-lobated nuclei. E Large epithelioid cells with abundant cytoplasm and frequent eosinophils in the background. F Plasmacytoid or rhabdoid tumor cells with eccentric nuclei and abundant dense pink cytoplasm. (B–F, H&E, ×400).
Of those with treatment data available, seven of eight patients received chemotherapy, and four patients also received radiotherapy. However, all six patients with documented information had no response to these therapies initially, and four even showed disease progression. None of the seven patients received stem cell transplants. Eight patients had clinical follow-up data; four patients died within a median follow-up interval of five months (range 2–35).
Histomorphology
The results of the histomorphology of our cases are summarized in Table 3. In our study, nine of 10 cases had H&E slides available for morphologic assessment. Interestingly, two biopsies taken three weeks apart from patient #1 on the same site showed different cytomorphologic features, and therefore, they were evaluated separately (Fig. 1B and C).
Eight of 10 biopsies from our nine patients contained large tumor cells, while the remaining two biopsies demonstrated mostly medium-sized cells. The tumor cells in all 10 biopsies displayed overt pleomorphism, including one with high-grade sarcomatous changes (Fig. 1C). The nuclei showed mixed shapes, including irregular (9/10), round/oval (3/10), and lobated (2/10) morphology (Fig. 1D). In addition, epithelioid or plasmacytoid/rhabdoid cytology was noted in two different cases (Fig. 1E and F). The chromatin was fine (4/10), coarse (4/10), or vesicular (2/10). Cytoplasmic granules were mostly absent (8/10), and only two cases had visible granules on H&E sections. Active mitotic figures were noted in 6/9 cases. Small foci of spindle cells were noted in 3/9 biopsies. Particularly, five of nine biopsies contained frequent reactive eosinophils.
As aforementioned, the two biopsies from case #1 in the same location exhibited significantly different morphologic features. The initial biopsy (case #1 A) contained mostly medium-sized tumor cells with a high N/C ratio and fine chromatin, which was misinterpreted as myeloid sarcoma by an outside institution (Fig. 1B). However, a repeat biopsy (case #1B) displayed highly pleomorphic sarcomatous cells with anaplastic nuclei and abundant cytoplasm, mimicking a poorly differentiated soft tissue sarcoma (Fig. 1C).
Immunohistochemistry
The results of immunohistochemistry are summarized in Table 4. In our study, the tumor cells expressed CD43 (8/8) (Fig. 2A), CD117 (10/10) (Fig. 2B), and mast cell tryptase (MCT) (10/10) (Fig. 2C) in all cases tested. In addition, the myeloid markers, CD13 (3/3) and CD33 (10/10) (Fig. 2D), were detected in all three and 10 cases stained, respectively; however, CD34 (0/8) and MPO (0/7) were negative. A subset of cases stained positively for CD45 (5/9), CD2 (1/9), CD25 (4/9), CD4 (2/5), CD56 (2/5), CD68 (5/9) (Fig. 2E), and CD123 (2/3). Furthermore, CD30 was positive in 5/8 cases with variable intensity (Fig. 2F). Other negative markers included CD1a (0/5), CD3 (0/8), CD20 (0/7), and S100 (0/10).

MCS consistently expresses (A) CD43, (B) CD117, (C) mast cell tryptase, and (D) CD33. CD68 is positive in most cases with a cytoplasmic granular staining pattern (E). CD30 is detected in 54% cases of MCS with variable intensity (F). (A–F, ×400).
Molecular genetic findings
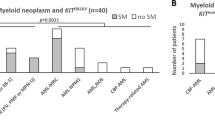
In our study, KIT D816V mutation was not detected in all nine cases studied (0/9), although case #5 had a KIT L799F mutation in exon 17 and case #10 was positive for KIT N822Y mutation. However, additional significant molecular genetic alterations were identified, which included case #1: RB1 R73fs, TP53 H179R, and NF1 R1337W; case #2: TP53 L330R, MLH1 L259S, and NOTCH1 D1185N; case #3: t(4;5)(q21.3;q33), PRKG2/PDGFRB rearrangement; case #5: 7q deletion; case #8: KRAS G12C; case #9: SH2B3 E208Q and ATM Y144H; and case #10: TP53 R273C. A summary of the molecular genetic studies is listed in Table 5, and the detailed data are provided in Supplementary Table 1.
Comprehensive review of the literature
Clinical information
An extensive review of the 34 cases of MCS (Table 2 and Supplementary Table 1), including 10 from our study and 24 from the literature, showed that MCS had a slight male predominance (M: F = 9: 8), with a median age of 39 years (range 1–77). The common sites of involvement included the bone (21/34, 62%), gastrointestinal tract (7/34, 21%), and soft tissue (5/34, 15%). Only 12% (2/17) of patients exhibited B-symptoms at diagnosis. Nearly half of patients (10/22, 45%) showed mast cell activation symptoms. Based on the data from complete blood count (CBC), 53% (10/19) of patients presented with anemia, while most patients had normal white blood cell count (12/18, 67%) and platelet count (12/17, 71%). Bone marrow involvement by MCS was noted in 8/26 (31%) of cases, while 4/26 (15%) were involved by SM. Seventeen of 23 (74%) patients had elevated serum tryptase levels, with a median level of 200 ng/ml (range 18–1034 ng/ml).
Seven of 30 (23%) patients had antecedent (5 cases) or synchronous (2 cases) systemic mastocytosis (SM), including three with neonatal mastocytosis. Transformation into mast cell leukemia was noted in 7/30 (23%) cases. Interestingly, patient #30 had a history of mediastinal yolk sac tumor 10 years prior, which was clonally related to MCS.21 In addition, as aforementioned, two patients in our study also had histories of germ cell tumors, including case #8 with a mediastinal germ cell tumor and case #10 with an ovarian dysgerminoma; however, neither case had sufficient materials to investigate the clonal relationship between the germ cell tumors and MCS. Furthermore, MCS from case #34 was clonally transformed from a T-lymphoblastic lymphoma/leukemia (T-LBL/ALL).25
Twenty-three of 27 (85%) patients received chemotherapy, and 11/26 (42%) received local radiotherapy. Most patients (16/23, 70%) had no response to the therapies, and 74% (17/23) of patients showed disease progression instead. Overall, only three patients had complete resolution of disease following chemotherapy with imatinib, imatinib and interferon-alpha 2b, and fludarabine, busulfan, and ATG-Fresenius (Neovii Biotech) followed by HLA-matched unrelated hematopoietic stem cell transplant (HSCT), respectively. Therefore, the prognosis was poor; during a median follow-up interval of 13 months (range 2–81 months), nearly half of the patients died (16/31, 52%) with a median survival of 24 months (Fig. 3).

Kaplan–Meier curve shows that the patients with MCS had a median survival of 24 months (n = 30).
Histomorphology
The tumor cells of MCS were mostly large (26/29, 90%) and displayed pleomorphic cytology (30/30, 100%) (Table 3), including sarcomatous changes in six cases. Mixed nuclear shapes were often present, mostly showing irregular (22/30, 73%), lobated (13/30, 43%), and round/oval (11/40, 37%) morphology. The chromatin in most cases was either fine (12/26, 46%) or coarse (11/26, 42%). The cytoplasm was mostly moderate to abundant and pale to lightly eosinophilic. In 59% (17/29) of cases, the cytoplasmic granules were absent or inconspicuous on H&E slides, although the basophilic metachromatic granules were more visible with Toluidine blue or Giemsa stain. Mitotic figures were active in 14 of 21 (67%) cases. Only 5 of 28 (18%) cases had focal spindled mast cells. Overall, 14 of 25 (56%) cases contained frequent background eosinophils, whereas 5 of 25 (20%) revealed rare eosinophils.
Immunophenotype
The neoplastic cells in MCS consistently expressed CD43 (14/14, 100%), CD117 (32/32, 100%), MCT (32/32, 100%), CD13 (7/7, 100%), and CD33 (15/15, 100%) (Table 4). They were variably positive for CD2 (8/24, 33%) and CD25 (15/25, 60%). In addition, CD4 (4/8, 50%), CD30 (13/24, 54%), CD45 (13/20, 65%), CD56 (3/8, 38%), CD68 (18/22, 82%), and CD123 (3/6, 50%) were detected in a subset of cases. The Ki67 proliferation indices were highly variable but mostly low with a median level of 10% (range 1–80%, n = 17). Other negative stains included CD1a (0/10), CD3 (0/19), CD20 (0/15), CD34 (0/20), CD163 (0/9), MPO (0/17), and S100 (0/17).
Molecular genetic assays
The canonical KIT D816V mutation was found in only two of 28 cases (7%), while six additional cases (6/28, 21%) had other forms of KIT mutations, including L799F, N822Y, N822K, V560G, D419del, and D579del (Table 5 and Supplementary Table 1). In case #30, both the mediastinal germ cell tumor and the MCS shared the same KIT D579del mutation.
Seven MCS cases were associated with SM. Among these cases, two (cases #19 and #25) shared the same KIT mutations with SM, indicating the clonal transformation of SM to MCS.17,19 In case #23, the KIT D419del mutation was detected in MCS but not reported in the prior SM.3 For the remaining four cases, the clonal relationship between MCS and SM was not proven due to lack of KIT mutations, including our case #6.4,16,18
Very limited molecular studies were performed on the MCS in the literature. In addition to the molecular genetic aberrations mentioned in our cases, only two cases from the literature had NGS data: case #31 was negative for mutations of NRAS, KRAS, CBL, and IDH1/2; and case #34 had multiple mutations, including BRAF G464V, TP53 R282W, ASXL1 Q768*, RUNX1 V164fs, and PHF6 (Table 5).
Discussion
Overview of MCS
Mast cell sarcoma (MCS) is classified as a variant of mastocytosis in the 2016 WHO classification.1 It is described as a destructive neoplasm composed of highly atypical mast cells that are initially localized but may spread and resemble mast cell leukemia by its terminal phase. Currently, there are only 34 cases of this entity reported including the 10 cases from our study.
MCS presents with a broad spectrum of ages and anatomic locations. Our review demonstrated that MCS nearly equally affected males and females with a median age of 39 years (range 1 to 77 years). Bone involvement was the most frequent manifestation, followed by the gastrointestinal tract and soft tissue. Association with systemic mastocytosis (SM) was noted in 23% cases of MCS, and the clonal transformation has been proven in some cases.17,19 Thus, it highlights the need for a long-term follow-up of SM with close monitoring for potential mass presentation and symptom progression. Responses to chemotherapy and radiotherapy were poor, and therefore the prognosis was dismal.
The morphologic features of MCS were typically high-grade with no resemblance to normal mast cells or atypical mast cells in SM. Most cases contained sheets of large pleomorphic cells with irregular nuclei and frequent bi- or multi-lobation. CD117 and MCT were very sensitive in labeling MCS, although tumor cells commonly expressed other myelomonocytic markers, including CD13, CD33 and CD68. Surprisingly, the canonical KIT D816V mutation detected in >90% of SM was only found in 7% of MCS, although mutations in other exons of KIT were noted.
Differential diagnoses of MCS
Diagnosis of MCS is very challenging due to its rarity, unusual clinical presentations with frequent bone involvement, nonspecific high-grade morphology, and overlapping immunophenotypic features with other more common hematologic neoplasms. As summarized in our review, MCS displays a broad spectrum of morphologic features with limited resemblance to normal mast cells. Moreover, significant morphologic variation may be present even in the same case, as noted in our case #1. Thus, MCS has been misinterpreted as lymphoma, Langerhans cell histiocytosis (LCH), myeloid sarcoma, and undifferentiated soft tissue sarcoma. Overall, the major differential diagnoses of MCS include histiocytic sarcoma, LCH, ALK-negative anaplastic large cell lymphoma (ALCL), and myeloid sarcoma (Table 6).
MCS commonly shows histiocytoid cytology with abundant cytoplasm, and therefore it is often confused with histiocytic sarcoma, in conjunction with the frequent expression of CD4 and CD68. However, histiocytic sarcoma is positive for CD163 with occasional expression of S100, but negative for CD117 and MCT.26
The epithelioid and/or histiocytoid cytology and background eosinophilia in MCS may lead to consideration of LCH during initial evaluation.8 Moreover, both LCH and MCS commonly involve the bone and express CD4 and CD68. Nevertheless, the characteristic longitudinal nuclear grooves of LCH are absent in MCS. In addition, none of the reported MCS cases expressed S100, CD1a or langerin, making these markers useful to differentiate LCH from MCS. Conversely, expression of CD117 and MCT is not observed in LCH.
MCS may closely resemble ALK-negative ALCL due to its highly pleomorphic cytology and frequent expression of CD2, CD4, CD25, CD30 and CD43. However, MCS typically shows a variable expression of CD30, in contrast to the diffuse and strong positivity in ALCL. Particularly, the positive staining of MCT and negative expression of other T-cell and cytotoxic markers essentially exclude the diagnosis of ALCL.
Occasionally, MCS may show blastoid cytology, as demonstrated in our case #1 A, which was initially misinterpreted as myeloid sarcoma (MS). Similar misdiagnosis was also reported in the literature.27 It is particularly confusing due to frequent positivity of myelomonocytic markers in MCS, including CD13, CD33, CD43, CD68, and CD117, although CD34 and MPO are consistently negative in MCS. Therefore, MCS has to be separated from MS or acute myeloid leukemia (AML) with monocytic differentiation. Leukemia cells with monocytic differentiation are mostly medium or medium-large in size, which a diffuse and strong expression of monocytic markers, including CD14, CD68 and CD163. On the other hand, the expression of MCT aids in the diagnosis of MCS. Another diagnostic hint is that MCS usually has a much lower Ki67 proliferation rate (median 10%) than that of MS or AML.
The frequent involvement of bone and soft tissue and the presence of high-grade pleomorphic cytology in most cases of MCS also raise the possibility of a poorly differentiated sarcoma of the bone and soft tissue. An accurate diagnosis could be very difficult due to lack of specific lineage markers in the initial IHC panel, including CD3, CD20, S100, cytokeratin, and myogenin. Therefore, it is recommended to include CD43 and/or CD45 in the initial workup of a poorly differentiated neoplasm. Based on our review, co-expression of CD43 and CD117 is sensitive albeit not specific for MCS; the positive stains for these two markers should trigger further workup for MCS after ruling out other more common hematologic neoplasms, particularly in cases with bone involvement. Further immunostains (MCT, CD2, and CD25) and serum tryptase levels are essential in establishing the diagnosis of MCS. He et. al reported a case of MCS with extreme anaplastic morphology, and the diagnosis was rendered as the tumor expressed strong and diffuse CD117 with weak expression of MCT, in addition to elevated serum tryptase level.20
MCS may variably express CD4, CD56 and CD123 (50%), which may raise a suspicion of blastic plasmacytoid dendritic neoplasm (BPDCN) in the cases with blastoid cytology. BPDCN mostly involves the skin and typically reveals a diffuse and strong expression of CD4, CD56 and CD123. However, many cases of BPDCN may have a weak positivity of CD4, CD123, and/or CD56, and additional markers such as TCL1 and TCF4 may aid in the diagnosis of BPDCN. Rare cases of MCS resemble plasma cell neoplasm with bone involvement and plasmacytoid cytology, but CD138 was negative in all nine cases stained (Supplementary Table 1). Other mimickers of MCS include melanoma and poorly differentiated carcinoma, although cytokeratin and S100 were negative in MCS. Interestingly, MITF was positive in two cases stained (cases #23 and #33), while other melanocytic markers were negative, including S100, HMB-45, and Melan-A.
Molecular genetics and pathogenesis
Although most cases of MCS manifest de novo, some are associated with SM, as observed in 23% of cases according to our review, and direct transformation of SM to MCS has been observed.17,19 Remarkably, a MCS was reported to be clonally related to a mediastinal yolk sac tumor (case #30).21 Indeed, two additional patients in our study also had histories of germ cell tumors, including a mediastinal germ cell tumor in case #8 and an ovarian dysgerminoma in case #10, although the relationship with MCS was uncertain due to lack of sufficient materials for further studies. Interestingly, multiple case reports have confirmed the clonal relationship between SM and germ cell tumors with the same underlying KIT mutations, including dysgerminoma (D816A),28 immature teratoma (D816V),29 and mixed germ cell tumors (D816H and D816V).30,31 In addition, the MCS in case #34 was clonally transformed from a T-LBL/ALL, and comprehensive genetic profiling of the MCS revealed an acquired TP53 mutation in addition to many shared somatic mutations with the original T-LBL/ALL.25
Our case #1 had Lynch syndrome with microsatellite instability (MSI), which was not reported in MCS. Of interest, our case #3 had a PDGRFB rearrangement. Rearrangement of PDGFRB is known to be associated with the WHO entity “myeloid/lymphoid neoplasms with eosinophilia and rearrangement of PDGFRA, PDGFRB, or FGFR1, or with PCM1-JAK2”. Indeed, PDGFRA or PDGFRB rearrangements have been reported in a few cases of SM.32,33,34
Mutational status of KIT gene has important diagnostic and therapeutic implications for SM. Particularly, the KIT D816V mutation on exon 17 is present in >90% cases of SM, which confers resistance to imatinib and certain other tyrosine kinase inhibitors (TKIs).35 Surprisingly, the KIT D816V mutation was only detected in 7% cases of MCS. The findings indicate that MCS is molecularly distinct from SM or that MCS more likely arises from the mast cell neoplasm without KIT D816V mutation.
The molecular genomic aberrations of MCS have not been well-defined. Molecular alterations are of interest as prognostic markers and potential therapeutic targets. NGS assays were performed on advanced cases of SM, including aggressive systemic mastocytosis (ASM), mast cell leukemia (MCL), and systemic mastocytosis with associated hematologic neoplasm (SM-AHN).36,37 In these studies, multiple recurrent mutations were detected in TET2 (47%), SRSF2 (43%), ASXL1 (29%), RUNX1 (23%), JAK2 (16%), N/KRAS (14%), CBL (13%), and EZH2 (10%); particularly, mutations in SRSF2, ASXL1, and RUNX1 were associated with adverse prognosis.36 In addition, these mutations have been shown to develop before KIT mutations in nearly all cases.38 In our review, NGS mutational studies were performed on eight cases of MCS, of which three carried TP53 mutations. Additional mutations were detected in MLH1, NOTCH1, RB1, NF1, BRAF, ASXL1, RUNX1, and PHF6. Although limited by the sample size, the genetic alterations and molecular pathogenesis of MCS could be thought of as distinct in comparison to SM.
Management of MCS
Multiple therapies have been tried in controlling MCS, but effective therapeutic regimens haven’t been established. This is likely due to the rarity and aggressiveness of this entity leading to an incomplete understanding of its biology. Therefore, currently the prognosis of MCS remains dismal.
Localized MCS may be managed with surgical excision followed by close monitoring.24 In addition, radiotherapy has been proposed for localized disease. In our review, 11 of 26 (42%) patients received radiotherapy, but the overall efficacy was very limited.
KIT mutations are clinically important predictive markers of response to TKIs. Especially, the KIT D816V mutation, which is frequently detected in SM, confers resistance to majority of TKIs.39 This mutation is only detected in 7% of MCS, which would suggest sensitivity to TKI. Indeed, there was a successful treatment of MCS of the uterus with imatinib.15 However, based on our review, MCS was mostly resistant to TKIs, including imatinib, dasatinib and midostaurin, with either minimal or only short-term responses.
The conventional chemotherapy regimens for lymphoid or myeloid neoplasms did not provide long-term response; these chemotherapies have been reported to show limited activity in MCS with only transient responses.3,10 High dose corticosteroids may induce a reduction in MCS burden and improve clinical symptoms, including MCAS, but the effect was usually transient. In addition, 2-chlorodeoxyadenosine (2-CdA) as a single agent did not appear to be efficacious against MCS.
Only one patient with MCS in the literature received matched unrelated hematopoietic stem cell transplantation (HSCT), who achieved remission.23 Therefore, more clinical trials are necessary to assess the value of HSCT in managing this aggressive neoplasm. Furthermore, new targeted therapeutic approaches should be explored, including experimental therapies using monoclonal antibodies (e.g., brentuximab vedotin, anti-CD30 or gemtuzumab ozogamicin, anti-CD33).
In summary, MCS is a very rare and highly aggressive neoplasm that carries an inferior prognosis with limited therapeutic regimens. MCS mostly manifests de novo, but it can transform from SM. It primarily involves the bone, and the diagnosis can be established with the expression of CD117 and particularly MCT, in conjunction with high serum tryptase levels. However, MCS may be underdiagnosed due to its nonspecific pleomorphic cytology and overlapping immunophenotype with other hematologic neoplasms. Notably, the cardinal KIT D816V mutation present in most cases of SM was uncommon in MCS, indicating overlapping but distinct pathogenesis of these two entities. In summary, it is essential to be aware of this rare entity and to develop a better understanding of its biology to provide accurate diagnosis and optimal management.
References
Swerdlow, S. H. et al. The 2016 revision of the world health organization classification of lymphoid neoplasms. Blood 127, 2375–2390 (2016).
Horny, H. P. et al. Mast cell sarcoma of the larynx. J. Clin. Pathol. 39, 596–602 (1986).
Ryan, R. J. et al. Mast cell sarcoma: a rare and potentially under-recognized diagnostic entity with specific therapeutic implications. Mod. Pathol. 26, 533–543 (2013).
Monnier, J. et al. Mast cell sarcoma: new cases and literature review. Oncotarget 7, 66299–66309 (2016).
Ravanpay, A. C., Fromm, J. R., Edlefsen, K. L., Martin, P. & Chesnut, R. The first report of human primary thoracic spine mast cell sarcoma: a case report. Clin. Neuropathol. 37, 28–35 (2018).
Wang, R. C., Ward, D., Dunn, P. & Chang, C. C. Acute mast cell leukemia associated with t(4;5)(q21;q33). Hum Pathol 67, 198–204 (2017).
Bautista-Quach, M. A. et al. Mast cell sarcoma in an infant: a case report and review of the literature. J Pediatr. Hematol. Oncol. 35, 315–320 (2013).
Kim, Y. S. et al. Pediatric mast cell sarcoma of temporal bone with novel L799F (2395 C > T) KIT mutation, mimicking histiocytic neoplasm. Am. J. Surg. Pathol. 37, 453–458 (2013).
Kojima, M. et al. Mast cell sarcoma with tissue eosinophilia arising in the ascending colon. Mod. Pathol. 12, 739–743 (1999).
Guenther, P. P. et al. Temporary response of localized intracranial mast cell sarcoma to combination chemotherapy. J. Pediatr. Hematol. Oncol. 23, 134–138 (2001).
Chott, A. et al. Morphologic and immunophenotypic properties of neoplastic cells in a case of mast cell sarcoma. Am. J. Surg. Pathol. 27, 1013–1019 (2003).
Brcic, L. et al. Mast-cell sarcoma of the tibia. J. Clin. Pathol. 60, 424–425 (2007).
Krauth, M. T. et al. Aggressive systemic mastocytosis with sarcoma-like growth in the skeleton, leukemic progression, and partial loss of mast cell differentiation antigens. Haematologica 92, e126–e129 (2007).
Bugalia, A., Abraham, A., Balasubramanian, P., Srivastava, A. & Nair, S. Mast cell sarcoma of the small intestine: a case report. J. Clin. Pathol. 64, 1035–1037 (2011).
Ma, H. B. et al. Successful treatment of mast cell sarcoma of the uterus with imatinib. Int. J. Hematol. 94, 491–494 (2011).
Auquit-Auckbur, I. et al. Malignant transformation of mastocytoma developed on skin mastocytosis into cutaneous mast cell sarcoma. Am. J. Surg. Pathol. 36, 779–782 (2012).
Falleti, J. et al. Mast cell sarcoma of the scalp: the first sign of undisclosed systemic mastocytosis? Pathol. Res. Pr. 208, 683–686 (2012).
Georgin-Lavialle, S. et al. Mast cell sarcoma: a rare and aggressive entity-report of two cases and review of the literature. J. Clin. Oncol. 31, e90–e97 (2013).
Schwaab, J. et al. Mast cell sarcoma mimicking metastatic colon carcinoma. Ann. Hematol. 93, 1067–1069 (2014).
He, F. et al. Anaplastic mast cell sarcoma: a unique pathologic entity in mastocytosis. Leuk. Lymphoma 58, 1515–1517 (2017).
Yamashita, A. et al. Mast cell sarcoma of the sternum, clonally related to an antecedent germ cell tumor with a novel D579del KIT mutation. Virchows Arch. 470, 583–588 (2017).
Raymond, L. M. et al. Mast cell sarcoma with concurrent mast cell leukaemia. Br. J. Haematol 189, e160–e164 (2020).
Kubasch, A. S. et al. Allogeneic hematopoietic stem cell transplantation in a rare case of tonsillar mast cell sarcoma. Front. Oncol. 10, 219 (2020).
Wardle, C. L. W. et al. Case report of a clinically indolent but morphologically high-grade cutaneous mast cell tumor in an adult: Atypical cutaneous mastocytoma or mast cell sarcoma? J. Cutan. Pathol. 48, 1404–1409 (2021).
Gao, J. et al. Mast cell sarcoma transdifferentiated from clonally-related T-lymphoblastic leukemia upon acquisition of TP53 mutation and genetic complexity. Leuk. Lymphoma 62, 3304–3307 (2021).
Pan, Z. & Xu, M. L. Histiocytic and dendritic cell neoplasms. Surg. Pathol. Clin. 12, 805–829 (2019).
Galanis, E., Li, C. Y. & Phyliky, R. Mast cell disease mimicking granulocytic sarcoma. Am. J. Hematol. 56, 194–195 (1997).
Tsutsumi, M. et al. An aggressive systemic mastocytosis preceded by ovarian dysgerminoma. BMC Cancer 20, 1162,020-07653-z (2020).
Lee, J. W. et al. Aggressive systemic mastocytosis after germ cell tumor of the ovary: C-KIT mutation documentation in both disease states. J. Pediatr. Hematol. Oncol. 29, 412–415 (2007).
Mitchell, S. G., Bunting, S. T., Saxe, D., Olson, T. & Keller, F. G. A variant c-KIT mutation, D816H, fundamental to the sequential development of an ovarian mixed germ cell tumor and systemic mastocytosis with chronic myelomonocytic leukemia. Pediatr. Blood Cancer 64, 10 (2017).
Xiao, P. et al. Ovarian germ cell tumor/mastocytosis with KIT mutation: A unique clinicopathological entity. Genes Chromosomes Cancer 61, 50–54 (2021).
Brown L. E., et al A 26-year-old female with systemic mastocytosis with associated myeloid neoplasm with eosinophilia and abnormalities of PDGFRB, t(4;5)(q21;q33). Case Rep. Hematol. 4158567 (2016).
Yamada, Y. & Cancelas, J. A. FIP1L1/PDGFR alpha-associated systemic mastocytosis. Int. Arch. Allergy Immunol 152, 101–105 (2010).
Dalal, B. I., Bruyere, H. & Forrest, D. L. Imatinib mesylate responsiveness in aggressive systemic mastocytosis: Novel association with a platelet derived growth factor receptor beta mutation. Am. J. Hematol. 82, 77–79 (2007).
Garcia-Montero, A. C. et al. KIT mutation in mast cells and other bone marrow hematopoietic cell lineages in systemic mast cell disorders: A prospective study of the spanish network on mastocytosis (REMA) in a series of 113 patients. Blood 108, 2366–2372 (2006).
Jawhar, M. et al. Additional mutations in SRSF2, ASXL1 and/or RUNX1 identify a high-risk group of patients with KIT D816V(+) advanced systemic mastocytosis. Leukemia 30, 136–143 (2016).
Li, P. et al. Comprehensive clinicopathologic and molecular analysis of mast cell leukemia with associated hematologic neoplasm: A report and in-depth study of 5 cases. Front Oncol 11, 730503 (2021).
Jawhar, M. et al. Molecular profiling of myeloid progenitor cells in multi-mutated advanced systemic mastocytosis identifies KIT D816V as a distinct and late event. Leukemia 29, 1115–1122 (2015).
Hornick, J. L. & Fletcher, C. D. The role of KIT in the management of patients with gastrointestinal stromal tumors. Hum. Pathol 38, 679–687 (2007).
Author information
Authors and Affiliations
Contributions
Z.P. and N.P.M. performed study design, acquisition of data, analysis and interpretation of data, writing, review and revision of the paper; J.Y. provided acquisition of data, analysis and interpretation of data, and review and revision of the paper; M.L.X. provided study concept and design, and review and revision of the paper; J.W., Q.S., X.C., Y.K., C.W.Z., C.C.C., W.C., D.C., M.C., and M.S. provided acquisition and interpretation of data, and review and revision of the paper; S.D.G. provided statistical analysis, and review and revision of the paper. All authors read and approved the final paper.
Corresponding author
Ethics declarations
Competing interests
M.L.X. has served in the Seattle Genetics lymphoma advisory board and as a consultant for Pure Marrow and Blueprint Medicines. All other authors have no conflicts of interest to disclose.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
About this article

Cite this article
Matsumoto, N.P., Yuan, J., Wang, J. et al. Mast cell sarcoma: clinicopathologic and molecular analysis of 10 new cases and review of literature. Mod Pathol 35, 865–874 (2022). https://doi.org/10.1038/s41379-022-01014-w
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41379-022-01014-w
This article is cited by
-
The international consensus classification of mastocytosis and related entities
Virchows Archiv (2023)
