
Abstract
The 2018 iteration of the ASCO-CAP HER2 testing guidelines proposes significant changes with an emphasis on the integration of concurrent immunohistochemistry (IHC) and in situ hybridization (ISH). We wished to evaluate the impact of these changes on clinical practice. Between Jan 2012 to Feb 2017, 2132 consecutive invasive breast carcinomas were evaluated with IHC and ISH for HER2. The sample tested was the breast primary or axillary nodes in all but 57 (2.7%) distant metastases. For 1824 cases with both dual-probe ISH and IHC results, the ISH subgroup was 1: 299 (16.4%), 2: 19 (1.0%), 1.0%, 3: 6 (0.3%), 4: 48 (2.6%) and 5: 1452 (79.6%). Ultimately 21% of group 2 and 4 cases and 80% of group 4 cases were positive. The change in HER2 status between the 2018 vs 2013 was: amplified in 323 (15.2%) vs 15.5%; not amplified in 1804 (84.6%) vs 82.2%; equivocal in 0 vs 2.3% previously. In 22 of 2127 cases (1.03%) the 2013 and 2018 results were discordant, all in groups 2-4. The discrepant cases included 15 of 331 (4.5%) of 2013 amplified cancers, now negative (all in groups 2 or 3) and 7 of 1796 (0.4%) 2013 nonamplified cases, now positive (all in group 4). Because of routine testing with both IHC and ISH, we found 6 of 1147 (0.52%) IHC negative (0 or 1+) cases were amplified by ISH. Further, 19 of 289 (6.6%) of IHC 3+ cases were nonamplified by ISH, circumstances not covered by these guidelines. In summary at the population level, the 2018 ASCO-CAP guidelines have a 99% agreement with the 2013 results. A major advantage is the abolishment of the clinically problematic equivocal category. Routine performance of both IHC and ISH uncovers a small proportion of cancers whose HER2 status is not addressed by these guidelines.
Similar content being viewed by others



Introduction
In contemporary practice, testing the status of the human epidermal growth factor receptor 2 (HER2) is essential for the care of all women with invasive breast cancer, because this information establishes the likelihood of response to HER2 therapies [1,2,3]. The American Society of Clinical Oncology and the College of American Pathologists (ASCO-CAP) have issued three iterations of HER2 testing guidelines for invasive breast cancer, the latest released in June 2018 [4,5,6].
In Australia, access to government-subsidized HER2 therapy is available through the Pharmaceutical Benefits Scheme (PBS), solely on the basis of HER2 amplification. This differs from practice elsewhere, where 3+ protein expression by IHC is accepted as a positive result. The primacy of ISH has shaped Australian HER2 testing practices [7], leading to routine evaluation of ISH status for all invasive cancers, mostly by brightfield methods. The advantages of integration with light microscopy, cost efficiency and ready availability have led to wide scale uptake of bright field ISH platforms, such as silver in situ hybridization (SISH), throughout the country [8]. Fluorescence ISH (FISH) testing is available for challenging cases. In practice, many Australian laboratories perform both IHC and ISH routinely on all cases, as the patterns of protein expression on IHC provide a measure of quality assurance and assists with the identification of rare cases of genetic heterogeneity.
The 2018 iteration of the ASCO-CAP HER2 testing guidelines has addressed some of the controversial aspects of the 2013 guidelines, particularly refining criteria for HER2 positivity in cases with possible chromosome 17 monosomy and for those with co-amplification of HER2 and CEP17 [6]. This has been achieved through an emphasis on the incorporation of HER2 protein expression by IHC, with the HER2 gene status evaluated by ISH, before a final HER2 result is issued. The key changes introduced in these guidelines include:
-
The clarification of the IHC 2+ category, reverting to the original, commonly accepted definition of weak to moderate complete membrane staining in >10% of tumor cells.
-
Discretionary, rather than mandatory repeat HER2 testing of resected tumors with a prior negative HER2 test on the needle core biopsy, as judged necessary by the pathologist.
-
Enumeration of the five clinical scenarios encountered in HER2 ISH evaluation of breast cancers, as shown in Table 1.
Table 1 2018 HER2 dual ISH clinical subgroups and final results determination based on integration with the IHC results. -
Specification of algorithms for resolving the HER2 status of cases in clinical groups 2-4, through the integration of IHC and ISH results, as shown in Fig. 1. In these guidelines there are no circumstances in which cancers with 0 or 1+ IHC are considered HER2 positive. Cases with 3+ IHC are regarded as HER2 positive, by definition.
Fig. 1: The percentage of a consecutive series of breast cancer patients falling within each HER2 biological subgroup. 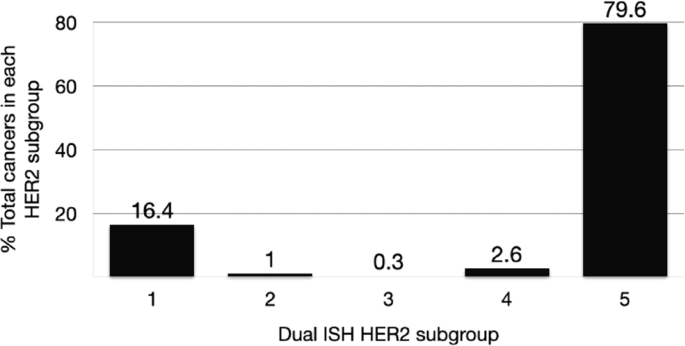
A bimodal distribution is observed with only 3.9% of the cancers are in subgroups 2-4 (monosomic, co-amplified or borderline HER2 dual ISH results).

Our laboratory serves as a reference center for HER2 evaluation. We have maintained an ongoing database of our cancers. We wished to analyze the impact of the changes introduced in the 2018 HER2 Testing Guidelines on clinical care.
Aims
Our primary aim was to (i) determine the impact of the 2018 ASCO-CAP HER2 testing guidelines on HER2 positivity rates in invasive breast cancers in our population. We also wished to: (ii) Assess the biological profiles of the discordant cancers and (iii) evaluate the correlations between HER2 IHC and ISH results, and (iv) assess the clinical profiles of cancers in each of the HER2 subgroups.
Materials and methods
Design
We received approval from the institutional human research ethics committee to access our laboratory data for the purposes of this audit.
We tabulated the raw data for a consecutive series of invasive breast cancers evaluated routinely by both IHC and dual probe ISH at our reference laboratory between Jan 2012 and Feb 2017. We utilized the original test results for this study. We applied both the 2018 and the 2013 HER2 ISH testing criteria to each cancer to determine its HER2 status according to each set of criteria.
The primary endpoint of this study was a comparison of the HER2 status of breast cancers in our population based on the 2018 versus the 2013 testing guidelines.
Other specific outcome measures of interest are:
-
The distribution of invasive breast cancers in each of the 5 dual ISH subgroups,
-
The likelihood of a final positive HER2 result within each ISH subgroup,
-
The proportion of cases with discordant HER2 status based on the 2018 versus the 2013 criteria. The direction of the change and the biologic basis for the discordance,
-
Determination of the clinical profile of cancers in each subgroup, specifically age, grade 3, tumor subtype, ER positivity and HER2 IHC results,
-
Ascertaining the proportion of cases with 0 or 1+ IHC results and HER2 amplification and the proportion with 3+ IHC but nonamplified by ISH.
Results
2132 consecutive invasive cancers were evaluated at our reference laboratory during this timeframe. As summarized in Table 2, the mean patient age was 62.0 (range 24–99). The cancer was the breast primary or axillary nodes in all but 57 cases (2.7%) of distant metastases. The tissue tested comprised needle core biopsies in 32.8%, resections in 68.2% and cell block specimens in 0.03%. The carcinoma was of no special type in 78.2% and a special subtype in 21.3%, the subtype was not stated in 0.4%. None of the discordant cases were among the metastatic samples tested. Overall 84.8% of cancers were ER positive, 15.2% ER negative and this information was missing for 1.2% of cases. Overall 81.0% of cases were PR positive, 19.0% PR negative and this information was missing in 1.5% of cases. HER2 IHC results were 0: 27.5%, 1+: 37.3%, 2+: 20.9%, 3+: 13.8% and not stated in 0.5%.
Both IHC and dual-probe ISH results were available in 1824 patients. For this group, the population distribution of HER2 ISH groupings is given in Table 3 and graphically in Fig. 1.
The clinical profiles of the cancers in each of the 5 ISH subgroups is depicted in Table 4. Patients with classic amplified or co-amplified cancers were significantly younger than those with other subtypes (p < 0.0001). They were also significantly more likely to be grade 3, of no special type and ER negative. Overall, 30.1% of grade 3 cancers were HER2 amplified. Grade 3 cancers comprised 76.2% of groups 1 and 4 cases but were significantly less common in group 2 and 5 cases. The 6 cases showing co-amplification were all grade 3 but the sample size is too small for further conclusions. Special cancer subtypes were over-represented in the nonamplified group. ER positivity rate was 62.2% group 1 cases and 84–100% in the remaining groups. Group 2 cases were negative by IHC in 63.2% of cases, significantly higher than for groups 3 (16.7%) or group 4 cases (33.3%). The highest proportion of IHC 2+ cases was seen in the borderline group 4, amongst which 45.8% showed 2+ protein expression.
Based on the 2018 criteria, the likelihood of a positive final HER2 result in each ISH subgroup is presented in Table 5. While by definition 100% of cases in subgroup 1 are HER2 positive and all cases in subgroup 5 are HER2 negative, the HER2 positive rate was 21.1% for cases in subgroup 2, 83.3% for cases in subgroup 3 and 20.8% in cases in subgroup 4.
Figure 2 displays the correlation in the HER2 status of cancers, between the 2018 and the 2013 HER2 criteria. According to the 2018 criteria, 84.8% of cases were HER2 negative, compared to 82.2% per the 2013 criteria. The HER2 positive rate was 15.2% by 2018 criteria versus 15.5% by 2013 criteria. While 2.3% of cancers were designated as equivocal by 2013 criteria, none had this designation by the 2018 criteria. The HER2 status could not be established in 5 cases (0.2%) due to insufficient/unsuitable tissue.

Note: (i) high overall levels of concordance, (ii) the abolishment of the equivocal group and (iii) a small increase in the proportion of cancers with a negative result.
Focusing on the sources of discordance between the 2018 and the 2013 criteria, Table 6 shows the main change is the abolishment of the equivocal group as the 2018 guidelines resolve all such cases into either positive or negative. The 2013 and 2018 results were concordant in 98.97% of cases. Overall, 22 of 2127 cases (1.03%) had discordant results. All discordant cases were in subgroups 2-4. Of these 15 of 331 (4.5%) were classified as amplified based on the 2013 guidelines but would be negative according to the updated guidelines. All these cases were in subgroups 2 or 3. Conversely, 7 of 1795 (0.4%) of cancers, all are in subgroup 4, were classified as non-amplified in 2013 but now have a positive HER2 status, based on the 2018 criteria.
As detailed in Table 7, the biological basis for a change from a previous positive result to a 2018 negative HER2 classification is monosomy (subgroup 2) or co-amplification (subgroup 3), without 3+ pattern of protein over-expression by IHC. This table also shows that the change of HER2 status from a prior negative result to a current positive result was on the basis of HER2 gene counts in the borderline range, but with evidence of 3 + HER2 protein expression by IHC.
In evaluating the correlation between IHC and 2018 ISH results, complete raw data for IHC and dual ISH were available in 1815 cases. As shown in Table 8, 6 of 1147 (0.52%) IHC negative (0 or 1+) cases were amplified by ISH. Further, 19 of 289 (6.6%) of IHC 3+ cases were non-amplified by ISH. Twelve of these results were based on the testing of resected cancers and 6 based on assessment of core needle biopsy samples and one on a cell block preparation.
Discussion
Targeted therapies for HER2 represent a major advance in the management of breast cancer in our century. These biological therapies are of proven clinical benefit for women whose tumors are HER2 positive [2, 3]. Testing procedures and the classification of HER2 test results have been iterative processes, led by ASCO-CAP [4,5,6]. As most biological variable, the HER2 status of tumors is non-binary, requiring care and judgment in clinical decisions concerning patients who have nonclassical HER2 results. This large, unselected audit of patients evaluated at our laboratory shows that at a population level, when IHC and dual probe ISH are used concurrently and routinely, 96.1% of breast cancers are either classic HER2 amplified (16.4%) or classic non-amplified (79.6%), but 3.9% have more unusual results, including chromosome 17 monosomy, co-amplification of HER2 and CEP 17, or low-level increases in HER2 copy numbers in the borderline range. The distribution of these categories are congruent with a small number of recent studies evaluating the correlation between the 2013 and 2018 guidelines [9,10,11,12,13]. Liu reported their experience with 2233 invasive breast cancers and found an increase in the proportion of HER2 negative cases, mostly through resolution of equivocal cases, but also from re-classification of previously HER2 positive cases into the negative category.
The 2018 HER2 testing criteria aimed to address the problematic area of equivocal HER2 test results, introduced by the 2013 criteria. This has been accomplished through an emphasis on the integration of IHC and ISH results, specifically requiring high levels of protein expression by IHC for patients to be deemed eligible for anti HER2 therapy. In comparing the HER2 test results of a large consecutive series of patients by each of the 2013 and the 2018 criteria, we can confirm that the strategy has successfully eliminated the equivocal test result category. Of the 50 cancers previously classified as equivocal in 2013, all had definitive results by the updated 2018 criteria, 40 were classified as negative and 10 as positive. Hoda et al. recently reported similar resolution of their equivocal cases, mostly reclassified as negative per the 2018 guidelines [10].
In our experience, the level of concordance between the 2013 and 2018 criteria was almost 99%, with only 1.03% of the cancers (22 of 2127 cases), having a change of HER2 status. All these cases were in groups 2-4, The direction of the change was from previously positive to now negative in 15 cases and the reverse in 7 cancers. The latter 7 cases were all among the 47 cancers with initially equivocal- likely negative results in 2013, which are now classified as positive. Among the cases with a change in HER2 status, the 2018 status was determined on the basis of IHC results. A 3+ pattern of IHC in cases with borderline elevated HER2 gene counts without ratios exceeding 2.0, resulting in a positive status, while for cases in subgroups 2 or 3, either 2+ or 3+ IHC resulted in a positive designation.
Overall, we saw a slight reduction in the percentage of cases qualifying as positive in 2018, with a commensurate increase in HER2 negative cases, since most HER2 equivocal cases were ultimately resolved as negative. Indeed, when considering the likelihood of a positive HER2 status by ISH subgroup, we have found that only 21% of cases with monosomy (subgroup 2) or borderline results (subgroup 4) were ultimately positive, while 80% of co-amplified cases (subgroup 3) were classified as positive. Concerning group 2 cases, Zare et al. reported this group to constitute 1.5% of all breast cancers in their series of 1201 cases and none of their cases were HER2 3+ by IHC, suggesting a different biology than classic group 1 HER2 amplified cases [14]. Our assessment of the clinical features among the 5 subgroups confirm significant differences in patient age, ER positivity, likelihood of ER expression and of special subtypes.
Apart from its large size, one of the strengths of our data is the population-based case accrual. The majority of tests were performed on resections rather than cores, reflective of the common patterns of practice during the period of this audit in our setting. We have since transitioned to preferential testing of core biopsies. Since in many centers only cases with 2+ IHC are evaluated by ISH, contemporary population-level data on both IHC and ISH are limited. Our practice of routine prospective evaluation by IHC and ISH in all cases permits assessment of this interesting topic. We have found a good but imperfect level of concordance between the two platforms. Among cancers with 3+ protein expression by IHC, 6.57% (19 of 270) were not amplified by ISH. Conversely, 0.52% (6 of 1141) cancers with 0 or 1+ protein expression by IHC are in fact HER2 amplified. These scenarios are not addressed by the ASCO-CAP guidelines which assumes ISH will only be performed for cases with 2+ IHC. In our setting, government policy permits access to subsidized anti-HER2 therapies to any women with a HER2 amplified cancer regardless of IHC, so technically women with 0 or 1+ IHC expression patterns are eligible and women with 3+ IHC but lacking amplification are ineligible for therapy. Specific outcome data are not available for either of these groups of patients. We are aware that some centers are performing both IHC and ISH for all cases. This has significant clinical, economic and workforce implications but at the very least the observation of a small number of patients with HER2 results outside of the ASCO-CAP framework, mandates strengthening QA processes for both IHC and ISH and continued monitoring of these rare subgroups.
Our data are based on silver ISH, rather than FISH and while the level of concordance between these platforms exceed 95%, they are not identical techniques. Recently, an enhancement of the SISH probe has been launched by the manufacturer with improved HER2 signal detection and reduced rates of technical failures. The impact of these changes in clinical test results is yet to be assessed.
Following the release of the 2018 guidelines where cases with 0 or 1+ IHC expression are classified as negative, the Australian HER2 testing recommendations have been revised and ISH testing is now not advocated for these patients [15]. In this population-based audit, 64.8% of cancers are negative by IHC, having 0 or 1+ protein expression levels. Not requiring ISH for 64.8% of all patients is an efficient use of resources, but the potential tradeoff is the inability to identify the 0.52% patients who, despite 0 or 1+ protein expression levels, are HER2 amplified and technically eligible for HER2 therapy, at least in Australia. Zhang reported that reflex FISH testing of all IHC 1+ cases at their center detected 5% patients with HER2 amplification [16]. Zadare also reported that among cases assigned to the classic amplified subgroup, only 91.5% were 2+ or 3+ by IHC, implying that 8.5% of group 1 cases had other, presumably 0 or 1+, IHC results [13]. It may be argued that since Trastuzumab is an antibody that interacts with the membrane component of its receptor, it requires the over-expression of HER2 protein on the cell surface to exert an effect and thus low IHC protein expression, would predict for a poor clinical response. The NRG trial B-47 (ClinicalTrials.gov identifier: NCT01275677) confirmed the lack of benefit from adjuvant trastuzumab for patients whose tumors lack gene amplification and are 1+ or 2+ by IHC [17]. The above incongruous scenarios of poor protein expression (0 or 1+) but with evidence of gene amplification or the reverse situation of 3+ protein expression without gene amplification are not captured by current clinical outcome data.
Activating mutations of HER2 have been described that potentiate its effects but independently of gene amplification or protein overexpression. The role of these mutations is currently under investigation as possible alternate mechanisms for HER2 targeted therapies.
In conclusion, at the population level, the 2018 ASCO-CAP guidelines have a 99% agreement with the 2013 results and classify over 96% of cancers into classic amplified or nonamplified categories. For cancers in remaining the less common categories, integration of the IHC and HER2 results will lead to definitive and mostly negative HER2 results. These guidelines have successfully eliminated the problematic equivocal category. Given the reliance on both sets of results, continued focus on quality assurance of HER2 ISH and IHC remains important.
References
Perez EA, Dueck AC, McCullough AE, Reinholz MM, Tenner KS, Davidson NE, et al. Predictability of adjuvant trastuzumab benefit in N9831 patients using the ASCO/CAP HER2-positivity criteria. J Natl Cancer Inst. 2012;104:159–62.
Smith I, Procter M, Gelber RD, Guillaume S, Feyereislova A, Dowsett M, et al. 2-year follow-up of trastuzumab after adjuvant chemotherapy in HER2-positive breast cancer: a randomised controlled trial. Lancet. 2007;369:29–36.
Slamon DJ, Leyland-Jones B, Shak S, Fuchs H, Paton V, Bajamonde A, et al. Use of chemotherapy plus a monoclonal antibody against HER2 for metastatic breast cancer that overexpresses HER2. N. Engl J Med. 2001;344:783–92.
Wolff AC, Hammond ME, Hicks DG, Dowsett M, McShane LM, Allison KH, et al. Recommendations for human epidermal growth factor receptor 2 testing in breast cancer: American Society of Clinical Oncology/College of American Pathologists clinical practice guideline update. J Clin Oncol. 2013;31:3997–4013.
Wolff AC, Hammond ME, Schwartz JN, Hagerty KL, Allred DC, Cote RJ, et al. American Society of Clinical Oncology/College of American Pathologists guideline recommendations for human epidermal growth factor receptor 2 testing in breast cancer. J Clin Oncol. 2007;25:118–45.
Wolff AC, Hammond MEH, Allison KH, Harvey BE, Mangu PB, Bartlett JMS, et al. Human epidermal growth factor receptor 2 testing in breast cancer: American Society of Clinical Oncology/College of American Pathologists Clinical Practice Guideline Focused Update. Arch Pathol Lab Med. 2018;142:1364–82.
Farshid G, Armes JE, Bell R, Cummings M, Fox S, Francis G, et al. Establishment of the Australian in situ hybridization program for the assessment of HER2 amplification in breast cancer: a model for the introduction of new biomarkers into clinical practice. Diagn Mol Pathol. 2010;19:187–93.
Morey AL, Brown B, Farshid G, Fox SB, Francis GD, McCue G, et al. Determining HER2 (ERBB2) amplification status in women with breast cancer: final results from the Australian in situ hybridisation program. Pathology. 2016;48:535–42.
Gordian-Arroyo AM, Zynger DL, Tozbikian GH. Impact of the 2018 ASCO/CAP HER2 guideline focused update. Am J Clin Pathol. 2019;152:17–26.
Hoda RS, Brogi E, Xu J, Ventura K, Ross DS, Dang C, et al. Impact of the 2018 American Society of Clinical Oncology/College of American Pathologists HER2 guideline updates on HER2 assessment in breast cancer with equivocal HER2 immunohistochemistry results with focus on cases with HER2/CEP17 ratio <2.0 and average HER2 copy number >/=4.0 and <6.0. Arch Pathol Lab Med. 2019.
Liu ZH, Wang K, Lin DY, Xu J, Chen J, Long XY, et al. Impact of the updated 2018 ASCO/CAP guidelines on HER2 FISH testing in invasive breast cancer: a retrospective study of HER2 fish results of 2233 cases. Breast Cancer Res Treat. 2019;175:51–7.
Xu B, Shen J, Guo W, Zhao W, Zhuang Y, Wang L. Impact of the 2018 ASCO/CAP HER2 guidelines update for HER2 testing by FISH in breast cancer. Pathol Res Pract. 2019;215:251–5.
Zare S, Rong J, Daehne S, Roma A, Hasteh F, Dell’Aquila M, et al. Implementation of the 2018 American Society of Clinical Oncology/College of American Pathologists Guidelines on HER2/neu Assessment by FISH in breast cancers: predicted impact in a single institutional cohort. Mod Pathol. 2019;32:1566–73.
Zare SY, Lin L, Alghamdi AG, Daehne S, Roma AA, Hasteh F, et al. Breast cancers with a HER2/CEP17 ratio of 2.0 or greater and an average HER2 copy number of less than 4.0 per cell: frequency, immunohistochemical correlation, and clinicopathological features. Hum Pathol. 2019;83:7–13.
Farshid G, Bilous M, Morey A, Fox S, Lakhani S, Loi S, et al. ASCO/CAP 2018 breast cancer HER2 testing guidelines: summary of pertinent recommendations for practice in Australia. Pathology. 2019.
Zhang X, Bleiweiss I, Jaffer S, Nayak A. The Impact of 2013 Updated ASCO/CAP HER2 Guidelines on the Diagnosis and Management of Invasive Breast Cancer: A Single-Center Study of 1739 Cases. Clin Breast Cancer. 2017;17:486–92.
Fehrenbacher L, Cecchini RS, Geyer CE, Jr., Rastogi P, Costantino JP, Atkins JN, et al. NSABP B-47/NRG oncology phase III randomized trial comparing adjuvant chemotherapy with or without trastuzumab in high-risk invasive breast cancer negative for HER2 by FISH and With IHC 1+ or 2. J Clin Oncol. 2019:Jco1901455.
Acknowledgements
We acknowledge the patients at our center and the pathologists and treating teams caring for them. We also wish to acknowledge the contributions of the anonymous reviewers whose comments have improved the presentation of our work.
Funding
This study has no external funding.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
GF has been a member of the Roche Australian HER2 Testing Advisory Board. The other authors have declared that they have no conflict of interest.
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Farshid, G., Dhatrak, D., Gilhotra, A. et al. The impact of 2018 ASCO-CAP HER2 testing guidelines on breast cancer HER2 results. An audit of 2132 consecutive cases evaluated by immunohistochemistry and in situ hybridization. Mod Pathol 33, 1783–1790 (2020). https://doi.org/10.1038/s41379-020-0555-7
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41379-020-0555-7
This article is cited by
-
Digital PCR quantification of ultrahigh ERBB2 copy number identifies poor breast cancer survival after trastuzumab
npj Breast Cancer (2024)
-
Comparison of breast cancer HER-2 receptor testing with immunohistochemistry and in situ hybridization
Breast Cancer Research and Treatment (2023)
-
HER2 copy number determination in breast cancer using the highly sensitive droplet digital PCR method
Virchows Archiv (2023)
-
Tumor budding and fibrotic focus—proposed grading system for tumor budding in invasive carcinoma no special type of the breast
Virchows Archiv (2022)
