
Abstract
Macrophages are essential innate immune cells found throughout the body that have protective and pathogenic functions in many diseases. When activated, macrophages can mediate the phagocytosis of dangerous cells or materials and participate in effective tissue regeneration by providing growth factors and anti-inflammatory molecules. Ex vivo-generated macrophages have thus been used in clinical trials as cell-based therapies, and based on their intrinsic characteristics, they outperformed stem cells within specific target diseases. In addition to the old methods of generating naïve or M2 primed macrophages, the recently developed chimeric antigen receptor-macrophages revealed the potential of genetically engineered macrophages for cell therapy. Here, we review the current developmental status of macrophage-based cell therapy. The findings of important clinical and preclinical trials are updated, and patent status is investigated. Additionally, we discuss the limitations and future directions of macrophage-based cell therapy, which will help broaden the potential utility and clinical applications of macrophages.
Similar content being viewed by others


Introduction
History of cell-based therapeutics
Deploying working resources is an exciting and necessary solution when further improvements are not expected from existing pools. Cell therapy conceptually meets this expectation by delivering ‘workable’ cells within the body as medical treatments. The first cell therapy in modern medical history was the intravenous transfusion of whole blood from a donor to a recipient in 19001. Based on the identification of human blood groups, allogeneic blood transfusion became a consolidated medical practice during the First World War and remains a central component of medicine today. Bone marrow transplantation (BMT) facilitated the era of stem cell therapy via the action of long-term self-renewing hematopoietic stem cells transferred from donor to patient2. For decades, cell therapy was predominantly limited to BMT for hematological diseases and epidermis transplantation for large burns3. Recently, however, cell-based therapeutics have experienced exponential growth within the pharmaceutical industry4. A noteworthy clinical application of genetically engineered cells, chimeric antigen receptor T cell (CAR-T) therapy, has emerged and will be an important component of cell therapy in the future5.
Current categories of cell therapy in clinics
With regard to cell origin, the donor and the recipient can be the same (autologous transplantation) or different individuals (allogeneic transplantation)3. Although they do not require cell transplantation, the mobilization of autologous cells is also considered cell therapy. Regarding the differentiation status of cellular sources, stem cells and fully differentiated cells are both applied.
Stem cells are mainly obtained from samples of tissues (skin, cornea, adipose tissue) obtained through biopsy and blood or cord blood samples6,7,8. Embryonic stem cells and induced pluripotent stem cells (iPSCs) will be used more extensively in the future if their utility is proven to outweigh the ethical problems9. Except for blood, bone marrow and adipose tissue-derived stem cells, most patients require ex vivo expansion of cells to obtain appropriate therapeutic efficacy10. For example, in 2014, the first cell therapy product to receive market authorization in Europe was that for cornea transplantation, which requires two interventions: (1) limbal biopsy and (2) in vitro cell expansion to generate the new cornea11.
Directly applying differentiated cells is considered the halfway point between cell and organ transplantation. Islet transplantation is an established therapy for patients with diabetes and has shown limited long-term success rates12. Several clinical trials using differentiated cells have been conducted in patients with heart infarction (cardiomyocytes)13, Parkinson’s disease (dopaminergic neurons)14, and Duchenne muscular dystrophy (myoblasts)15. These trials had inadequate clinical outcomes, and overcoming the barrier of cellular sources remains problematic. Obtaining differentiated cells from genetically modified iPSCs is an intriguing solution but currently requires further development.
CAR-T therapy uses engineered DNA constructs introduced into patient T cells to redirect their cytotoxicity to tumor cells that bear CD19, a B lymphocyte-associated antigen16. This therapy has led to significant advancements in the use of differentiated cells. Engineered alterations in cellular function potentiated the therapeutic use of specific cell types4. Innovations in engineering disciplines are currently being explored, and some of these approaches have been successfully used to generate commercialized products17, although many remain at a preclinical stage.
Macrophage-based cell therapy
Immune cells have specialized characteristics. Their unique ability to move throughout the body enables them to actively search for their target sites and perform their specific roles in the body; this is what we aim for in immune cell-based therapeutics. In this regard, macrophages have great potential as a cell source in cell therapy.
Macrophages are strategically distributed throughout the body as tissue-resident innate immune cells. They perform a vital homeostatic role as prodigious phagocytic cells that clear intruding pathogens and large amounts of endogenous harmful materials, such as apoptotic cells, dying erythrocytes, amyloid beta and surfactants, to maintain normal organ function18. Macrophages are highly heterogeneous cells that can rapidly change their function in response to local microenvironmental signals19. They have an extremely plastic nature in vivo and are involved in many human diseases with both protective and pathogenic functions19. Insights into the development of macrophage-based cell therapies have focused on their notable actions, such as promoting tissue regeneration and clearing cancer cells or pathogens20.
In this review, we update and discuss the current developmental status of macrophage-based cell therapy. In line with the characteristics of macrophages, a wide variety of target diseases are briefly introduced. We also discuss their limitations along with potential future directions.
Clinical trials on macrophage-based therapy
A clinical trial search in ClinicalTrials.gov was conducted with one keyword (Macrophage). In total, 366 search results were found, and it was manually determined whether the trial was relevant to macrophage cell therapy. Only 11 out of the 366 search results were macrophage cell therapy-related clinical trials, and these 11 trials were included in this review (Table 1). Among the 11 selected clinical trials, nine (81.8%) were regarding the adoptive transfer of macrophages and ex vivo polarization with different strategies. Two studies (18.1%) were chimeric antigen receptor-macrophage (CAR-M) trials. Not all clinical trials reported the patient response publicly, either through ClinicalTrials.gov or a paper publication. Interestingly, all studies with publicly reported response data focused on ‘ex vivo polarization and adoptive transfer’.
Most of the clinical trials that used ex vivo polarization and adoptive transfer of macrophages are in phase 2 or 3, and the target diseases are well known, including cardiomyopathy, osteonecrosis, limb ischemia, stroke, arterial disease, and chronic anal fissure, indicating the clinical usefulness of the methodology in regenerative medicine. One of the representative studies was entitled “Treatment of Anal Fissure by Activated Human Macrophages” (registration number: NCT00507364) and was a phase 3 trial consisting of chronic anal fissure treatment21. In this trial, 199 patients were divided into control and macrophage-treated groups. In the macrophage-treated group, a macrophage suspension (0.05 mL/injection) was injected 0.5–1 cm from the edge of the ulcer. Complete recovery was achieved in 27% of the macrophage-treated group, whereas only 6% of the control group showed complete recovery. No adverse effects were noted in the trial. Another trial with publicly reported response data was a phase 1 trial entitled “Safety of Autologous M2 Macrophages in the Treatment of Non-Acute Stroke Patients” (registration number: NCT01845350), which focused on ischemic and hemorrhagic stroke treatment22. Autologous peripheral blood mononuclear cells were obtained from patients with nonacute stroke, polarized to M2 macrophages, and injected intrathecally by a lumbar puncture after premedication with dexasone. Thirteen patients were enrolled and divided into control and treatment groups. Clear improvement in the NIH Stroke Scale/Score (NIHSS) was observed in 75% of the treatment group and 18% of the control group. No adverse effects related to cell therapy were noted throughout the trial. In the phase 2 trial “Use of Ixmyelocel-T (Formerly Catheter-based Cardiac Repair Cell [CRC]) Treatment in Patients with Heart Failure Due to Dilated Cardiomyopathy”, Ixmyelocel-T, including autologous bone marrow-derived activated macrophages, was administered to patients through intramyocardial injection23. Positive effects with improved symptoms were found in patients with ischemic dilated cardiomyopathy but were not found in the nonischemic population. Major adverse cardiovascular events were markedly decreased in the treatment group of ischemic patients, indicating good efficacy of Ixmyelocel-T.
There were no publicly reported response data from any of the studies on CAR-M therapy; it is necessary to note that clinical trials on the technology are in the early stages of development. One representative clinical trial is “CAR-Macrophages for the Treatment of HER2-Overexpressing Solid Tumors”, which is an ongoing phase 1 trial targeting HER2-overexpressing solid tumors. In this clinical trial, CAR-M targeting HER2 was constructed (CT-0508) and intravenously injected into the treatment group. As it is an ongoing trial and the recruitment status is “recruiting”, no response results could be expected as yet. Another important phase 1 clinical trial, “Intraperitoneal MCY-M11 (Mesothelin-targeting CAR) for the Treatment of Advanced Ovarian Cancer and Peritoneal Mesothelioma”, targeted relapsed/refractory ovarian cancers, including peritoneal mesothelioma, fallopian tube adenocarcinoma, adenocarcinoma of the ovary, and primary peritoneal carcinoma. MYC-M11 (mesothelin-targeting CAR) was administered by intraperitoneal infusion to 14 participants; the response data have yet to be publicly reported through ClinicalTrials.gov or a publication of the study findings.
Another important clinical trial should be noted; however, it was conducted in the UK and is not presented in Table 1. Research groups at the University of Edinburgh successfully completed autologous macrophage therapy for liver cirrhosis24. They conducted a phase 1 dose escalation trial of autologous macrophage therapy in nine adults and found that all participants survived and were transplant-free at the one-year follow-up.
Patent status
To identify the international patent status of macrophage-based cell therapy, we conducted a patent analysis and an analysis of market and technology trends. MJL Bio Co. retrieved patent samples with a priority date before 15 June 2021 using a series of search terms, including macrophage, treat, prevent, wound, regeneration, recover, repair, anticancer and inhibit or suppress. In total, 9045 patent documents were initially obtained. From these, we excluded 8833 patents. These were patents for which the aim was the modulation of in vivo resident macrophages by drugs or where macrophages were not used for cell therapy. Ultimately, 212 patent documents were included for further interpretation (Supplementary Table 1).
Looking at the overall application trend by year in the field of macrophage cell therapy, research has been conducted since 2015 (Fig. 1). Recently, considering the existence of undisclosed cases, macrophage cell therapy is on the rise and in the early stages of technological growth worldwide. The top inventors are located in the United States (26%), Europe (20%) and PCT (20%). Among them, the University of Pennsylvania developed CAR-M for the treatment of cancer (Table 2). Duke University has the second-highest number of inventions and primarily focuses on methods for treating cancers and pathogen infections using antigen-presenting cells loaded with RNA. Most patents were related to cancer, but many were related to regenerative medicine. For example, XCELL medical solutions and INSERM applied for patents with regenerative diseases as an indication. XCELL’s patent provides in vitro methods to induce macrophage polarization in an M2 phenotype that overexpresses NGAL and IL-10, which is useful for tissue recovery.

Macrophage cell therapy patent documents by publication year and the top six countries in which assignees applied.
Regarding genetic modification status, 107 patents (55%) were for unmodified macrophages, and 83 (43%) were for modified macrophages. Unmodified macrophages were most frequently applied as activated macrophages and M2 macrophage types. Modified macrophage-related patents were mainly aimed at CAR-M therapy, with 25 studies.
Animal experimental trials
The most widespread example of the experimental success of macrophage cell therapy is in the pulmonary alveolar proteinosis (PAP) disease model25. This disease is prevalent in children who have mutations in CSF2RA or CSF2RB, encoding GM-CSF receptor α or β, respectively, which cause hPAP by impairing GM-CSF-dependent surfactant clearance by alveolar macrophages, resulting in progressive surfactant accumulation in alveoli and hypoxemic respiratory failure26,27. There are currently no pharmacological therapies for hPAP, and surfactants must be removed by whole-lung lavage, an inefficient and invasive procedure to physically remove excess surfactant. Suzuki et al. showed the efficient therapeutic potential of pulmonary macrophage transplantation (PMT) of either wild-type or Csf2rβ gene-corrected macrophages without myeloablation in Csf2rβ mutant mice. PMT was safe and efficient, and only one administration was required to treat lung disease. These exciting results highlighted the need for the development of allogeneic macrophage-based cell therapies based on genetic modifications.
We previously showed the obvious regenerative capacity of wild-type macrophages when transferred into Ptger4 mutant mice with a defect in proper intestinal epithelial regeneration postinflammation28. This study thereby highlighted the need for allogeneic sources of macrophage cell therapy in patients with IBDs who carry genetic mutations at the PTGER4 locus.
Neurodegenerative diseases are another promising target for macrophage cell therapy because stem cell engraftment has clear limitations due to the large size of the human brain; moreover, the need for stereotactic injection complicates the homogeneous distribution of grafted cells even when highly migratory cells such as oligodendrocyte precursors are transplanted29. Transferred bone marrow cell-derived macrophages showed the capacity to efficiently distribute to the brain and clear accumulated glucosylsphingosine in place of malfunctioning microglia in a Parkinson’s disease model30.
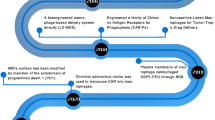
As in vivo studies have been continuously reported in recent years, articles published from 2019 to 2023 were searched using PubMed (https://pubmed.ncbi.nlm.nih.gov/) with the search string ((macrophage[Title/Abstract]) AND (cell therapy[Title/Abstract])). In total, 263 search results were manually determined to be relevant to macrophage cell therapy. With regard to review papers, references were also considered in our search and were reviewed to determine their relevance. Most studies were related to CAR-T therapy using granulocyte-macrophage colony-stimulating factor (GM-CSF) or analyzed the effects of stem cell therapy on macrophages and were excluded from our candidate study list. Studies that included only in vitro experiments were also excluded to limit this review to studies demonstrating clinical possibilities. As a result, 38 papers were included as macrophage cell therapy-related studies and were further classified into five different groups according to methodology as follows: CAR-M, induced pluripotent stem cell (iPSC)-derived macrophages, macrophages loaded with nanoparticles; ex vivo polarization and/or adoptive transfer of macrophages, and surface-anchoring engineering of macrophages (Supplementary Table 2). Among the 38 studies, 12 were considered promising and representative and thereby selected and presented in Table 3 and Fig. 2.

Various attempts to increase the efficiency of macrophage-based cell therapy have been reported. Promising in vivo studies in the previous 5 years (2019–2023) are classified into five different groups. a Direct differentiation of macrophages from iPSCs enables bulk production of macrophages for therapeutic use32. b Utilizing the function of macrophages as efficient transporters, various nanoparticles with therapeutic agents can be loaded onto macrophages and delivered to target lesions33. c Diverse trials changing the target molecules and intracellular signaling domains of the existing CAR-M structure can increase the therapeutic efficacy31. d Macrophages can also be used as delivery cells by anchoring certain materials on the surface of the cell34. e Patient macrophages can be collected and artificially polarized ex vivo for successive adoptive transfer back to the patient35,41. iPSC induced pluripotent stem cell, CpG-ASO unmethylated cytosine-phosphate-guanine motif and anti-P-glycoprotein antisense oligonucleotide, CAR-M chimeric antigen receptor macrophage, MerTK Mer tyrosine kinase, IFN-α interferon alpha, M-CSF macrophage colony-stimulating factor.
Niu et al. (2021) generated CAR-M targeting CCR7 with a cytosolic domain from Mer receptor tyrosine kinase for tumor growth suppression, metastasis prevention, and subsequent prolongation of survival31. The application of anti-CCR7 CAR-M successfully resulted in the suppression of immunosuppressive cell migration from tumor tissue to distal immune organs, showing effective systemic antitumor immunity in vivo.
One issue that requires elucidation in order to use macrophages for therapeutic purposes is how to sufficiently increase the supply quantity. Since the replication capability of macrophages is limited, Pouyanfard et al. (2021) performed a new trial by directly differentiating iPSCs into macrophages to meet the needs on a large scale while still maintaining a homogenous population32. This method effectively induced both M1 and M2 macrophages; in particular, the resulting M2 macrophages were found to reduce fibrogenic gene expression and associated histological markers in liver fibrosis in vivo.
Because of the good penetration efficacy of macrophages into lesions, they can also be used as good transporters of loaded nanoparticles. Wang et al. (2022) used a RAW264.7 cell line polarized to M1 macrophages and loaded with nanospheres composed of the nucleic acid therapeutic and chemotherapeutic drug cisplatin. The loaded cells were injected and targeted A549 human alveolar basal epithelial cell adenocarcinoma; significant antitumor performance without significant adverse effects was observed33.
Shields et al. (2020) reported one of the most innovative approaches to maintaining macrophage subtypes for a longer duration based on the geometric principles of macrophage phagocytosis34. They anchored soft particles called ‘backpacks’ on the surface of the macrophages, which are phagocytosis-resistant owing to their morphology and, at the same time, contain IFNα to help macrophages maintain the M1 subtype for longer. The cells with ‘backpacks’ significantly reduced tumor growth and improved survival without significant toxicity when used in a 4T1 breast cancer cell model in vivo.
Most studies using ex vivo polarization and adoptive transfer generally make use of M2-polarized macrophages, which reduce the inflammatory response and simultaneously increase wound healing. Treatment using this method has been studied in a wide variety of target diseases, including acute kidney injury, autoimmune encephalomyelitis, full-thickness cutaneous wounds, hepatic fibrosis caused by cystic echinococcosis, heart tissue damage, Achilles tendon rupture, spinal cord injury, and myocardial infarction35,36,37,38,39,40,41.
Limitations
For macrophage-based cell therapy to be successful, preclinical study and clinical trial pathways must be carefully navigated, and scientific and manufacturing hurdles must be overcome.
Two of the most common indications are cancer and regenerative diseases, indicating that the most significant characteristic of macrophages is their plasticity. They have the ability to alter their phenotypes in response to their surroundings42; however, because of this ability, they have an important inherent drawback. We expect CAR-M to have phagocytic ability against cancer cells; however, there is the possibility of acquiring M2 phenotypes, leading to a tumor-prone microenvironment when exposed to cancer cells43. It is worth noting that in every trial regarding the adoptive transfer of macrophages for cancer in our preliminary study, eventually, cancer growth was accelerated. In contrast, ex vivo-generated M2 macrophages can be used to promote tissue regeneration; however, there is the risk of their phenotypes reverting to M1 macrophages when they encounter chronic, incurable inflammatory environments. In this regard, macrophage polarization needs to be fully understood with regards to how long the epigenetic mark perpetuates44 and how we can potentiate desired phenotypes via ex vivo priming. One way to overcome the uncertainty of phenotype duration is to create genetically ‘fixed’ macrophages. Because the CRISPR system works easily in primary macrophages45, the TNF gene could be deleted to promote tissue regeneration in concordance with lowering the risk of inducing unnecessary inflammation. The knockout of a critical enzyme or transcription factor may also be useful; for example, Prkacb deletion promotes macrophages into M1 phenotypes even when exposed to the cancer environment46.
Along with the phenotype duration, the period of substantive activity of transferred macrophages in vivo requires further elucidation. In-depth tracking studies of injected macrophages have yet to be performed. In previous reports using murine iPSC-derived macrophages, the population maintained the macrophage phenotype for at least 1 year47. While many immunological studies have shown the persistence of transferred macrophages using valuable mouse models for cell tracing, few studies on therapeutic macrophage transfer have considered the duration of survival with the same function. Preclinical GLP studies should present the distribution data of injected macrophages over time using quantitative PCR following different routes of injections. Intravenously injected macrophages were reported to be trapped in the lungs soon after injection due to entrapment inside the pulmonary capillaries and were rarely observed in tumors; the same result was also observed for MSCs48,49,50. In this regard, intravenously injected macrophages may have beneficial effects even if they are not present in large amounts in the target tissue. These effects are believed to be ascribed to the production of anti-inflammatory cytokines, such as growth factors that ameliorate the damage to organs. However, local injections into the mucosal layer, skin, or a consolidated tissue structure would lead to different biodistributions and pharmacokinetics. For example, gene-corrected macrophages transferred into the lungs of Csf2rb (CD131)-deficient mice were evaluated by transgene-specific PCR tracking25. Over a period of 12 months, the proportion of CD131+ cells among bronchoalveolar lavage cells increased from 0 to 69% due to the proliferation of the transplanted macrophages. Understanding the in-depth kinetics of injected macrophages along with their mechanistic actions will allow the further use and development of macrophage-based cell therapy.
Another challenge is producing macrophages on a scale that will allow the treatment cost to decrease3. Understanding whether and how it will be possible to produce macrophages on a large scale will be an important determinant of whether macrophage cell therapy will transition from a boutique, expensive cottage industry to mass production and take advantage of economies of scale. Manufacturing facilities should provide tightly unified protocols to produce macrophages with stable and consistent phenotypes. At least ~109 M-CSF-derived macrophages should be produced from a patient in one leukapheresis51,52,53, but more importantly, macrophages should be obtained from different sources, including hematopoietic stem cells. Based on the trend that the development of allogeneic therapies has drastically increased in recent years54, stable and unified protocols for genetic modification of different sources of macrophages are needed.
Genetic engineering
As described throughout this review, genetic engineering of macrophages has much therapeutic value. To date, the best way to obtain a specific knockout is mediated by CRISPR/Cas9 complexes. The delivery of ribonucleoprotein into ex vivo-generated macrophages via electroporation is very efficient and safe45 and thus will be used to provide therapeutic macrophage sources from allogeneic as well as autologous donors. The advantage of electroporation is that it does not alter the phenotype of macrophages itself. However, it is more complicated in the case of protein overexpression, such as CAR-M. The current successive approach to introduce exogenous DNA sequences is the use of a viral delivery system, which strongly changes macrophages into the M1 phenotype. This is helpful in treating cancer but might be a negative factor for the treatment of regenerative diseases. Further studies are needed to obtain efficient genetic engineering in primary macrophages in the future.
Future directives
Macrophages have great potential as cellular therapeutic sources (Fig. 3). Their outstanding regenerative capacity could directly aid tissue reconstruction in injured organs, such as the intestines, skin, liver, heart, kidneys, and lungs. Their phagocytic ability could be used to clear cancer cells or neurodegenerative materials as well as infectious agents. As efficient pro-inflammatory regulators, they could be applied to suppress inflammation and deliver active tissue-healing substances. Based on these unique features of macrophages compared to other cell types, more data on safety need to be produced in an effort to make them available for use. In the future, gene editing will be used to obtain purpose-oriented macrophage phenotypes. Although numerous hurdles will need to be addressed, the inherent nature of macrophages will extend their application to new therapeutic frontiers.

The outstanding phagocytic and wound-healing abilities of macrophages will extend the scope of target diseases for macrophage-based cell therapies in the future. a Ex vivo activated PBMC-derived macrophages promote skin wound healing via the secretion of growth factors and anti-inflammatory cytokines21. b Transferred macrophages efficiently clear accumulated neurotoxic materials30. c Genetically engineered CAR-M eradiate cancer cells16. d A specific subtype of macrophages reduces ECM contents around the heart injury site and promotes regeneration23,41. e Transferred macrophages clear excessive surfactant and resolve the pathology of PAP25. f Macrophages secrete CXCL1 and WNT to coordinate damaged intestinal epithelial cell regeneration28. g Regenerative macrophages can resolve fibrosis and promote hepatocyte regeneration24,32. PBMCs peripheral blood mononuclear cells, ECM extracellular matrix, PAP pulmonary alveolar proteinosis, IBD inflammatory bowel disease, CAR-M chimeric antigen receptor macrophages, VEGFA vascular endothelial growth factor A, EGF epidermal growth factor.
References
Madge, H. M. On transfusion of blood. Br. Med. J. 1, 42–44 (1874).
Thomas, E. D., Lochte, H. L. Jr., Lu, W. C. & Ferrebee, J. W. Intravenous infusion of bone marrow in patients receiving radiation and chemotherapy. N. Engl. J. Med. 257, 491–496 (1957).
Cossu, G. et al. Lancet Commission: stem cells and regenerative medicine. Lancet 391, 883–910 (2018).
Bashor, C. J., Hilton, I. B., Bandukwala, H., Smith, D. M. & Veiseh, O. Engineering the next generation of cell-based therapeutics. Nat. Rev. Drug Discov. 21, 655–675 (2022).
Lyu, L., Feng, Y., Chen, X. & Hu, Y. The global chimeric antigen receptor T (CAR-T) cell therapy patent landscape. Nat. Biotechnol. 38, 1387–1394 (2020).
Green, H. Cultured cells for the treatment of disease. Sci. Am. 265, 96–102 (1991).
Pellegrini, G. et al. Biological parameters determining the clinical outcome of autologous cultures of limbal stem cells. Regen. Med. 8, 553–567 (2013).
Rama, P. et al. Limbal stem-cell therapy and long-term corneal regeneration. N. Engl. J. Med. 363, 147–155 (2010).
Robertson, J. A. Embryo stem cell research: ten years of controversy. J. Law Med. Ethics 38, 191–203 (2010).
Barrandon, Y. & Green, H. Three clonal types of keratinocyte with different capacities for multiplication. Proc. Natl Acad. Sci. USA 84, 2302–2306 (1987).
Europena Medicines Agency (EMA). First stem-cell therapy recommended for approval in EU (2014). https://www.ema.europa.eu/en/news/first-stem-cell-therapy-recommended-approval-eu.
Bruni, A., Gala-Lopez, B., Pepper, A. R., Abualhassan, N. S. & Shapiro, A. J. Islet cell transplantation for the treatment of type 1 diabetes: recent advances and future challenges. Diabetes Metab. Syndr. Obes. 7, 211–223 (2014).
Smalley, E. Neural stem cell trailblazer StemCells folds. Nat. Biotechnol. 34, 677–678 (2016).
Dunnett, S. B., Bjorklund, A. & Lindvall, O. Cell therapy in Parkinson’s disease—stop or go? Nat. Rev. Neurosci. 2, 365–369 (2001).
Mendell, J. R. Immunosuppressive therapy in Duchenne muscular dystrophy: considerations for myoblast transfer studies. Adv. Exp. Med. Biol. 280, 287–295 (1990).
Villanueva, M. T. Macrophages get a CAR. Nat. Rev. Cancer 20, 300 (2020).
Kirouac, D. C. et al. Deconvolution of clinical variance in CAR-T cell pharmacology and response. Nat. Biotechnol. https://doi.org/10.1038/s41587-023-01687-x (2023).
Mosser, D. M. & Edwards, J. P. Exploring the full spectrum of macrophage activation. Nat. Rev. Immunol. 8, 958–969 (2008).
Murray, P. J. & Wynn, T. A. Protective and pathogenic functions of macrophage subsets. Nat. Rev. Immunol. 11, 723–737 (2011).
Lee, S., Kivimae, S., Dolor, A. & Szoka, F. C. Macrophage-based cell therapies: the long and winding road. J. Control Release 240, 527–540 (2016).
Danon, D. et al. Treatment of human ulcers by application of macrophages prepared from a blood unit. Exp. Gerontol. 32, 633–641 (1997).
Chernykh, E. R. et al. Safety and therapeutic potential of M2 macrophages in stroke treatment. Cell Transpl. 25, 1461–1471 (2016).
Henry, T. D. et al. Safety and efficacy of ixmyelocel-T: an expanded, autologous multi-cellular therapy, in dilated cardiomyopathy. Circ. Res. 115, 730–737 (2014).
Moroni, F. et al. Safety profile of autologous macrophage therapy for liver cirrhosis. Nat. Med. 25, 1560–1565 (2019).
Suzuki, T. et al. Pulmonary macrophage transplantation therapy. Nature 514, 450–454 (2014).
Suzuki, T. et al. Familial pulmonary alveolar proteinosis caused by mutations in CSF2RA. J. Exp. Med. 205, 2703–2710 (2008).
Suzuki, T. et al. Hereditary pulmonary alveolar proteinosis: pathogenesis, presentation, diagnosis, and therapy. Am. J. Respir. Crit. Care Med. 182, 1292–1304 (2010).
Na, Y. R. et al. Prostaglandin E(2) receptor PTGER4-expressing macrophages promote intestinal epithelial barrier regeneration upon inflammation. Gut 70, 2249–2260 (2021).
Gupta, N. et al. Neural stem cell engraftment and myelination in the human brain. Sci. Transl. Med. 4, 155ra137 (2012).
Shibuya, Y. et al. Treatment of a genetic brain disease by CNS-wide microglia replacement. Sci. Transl. Med. 14, eabl9945 (2022).
Niu, Z. et al. Chimeric antigen receptor-modified macrophages trigger systemic anti-tumour immunity. J. Pathol. 253, 247–257 (2021).
Pouyanfard, S. et al. Human induced pluripotent stem cell-derived macrophages ameliorate liver fibrosis. Stem Cells 39, 1701–1717 (2021).
Wang, Y. et al. Engineering CpG-ASO-Pt-loaded macrophages (CAP@M) for synergistic chemo-/gene-/immuno-therapy. Adv. Healthc. Mater. 11, e2201178 (2022).
Shields, C. W. T. et al. Cellular backpacks for macrophage immunotherapy. Sci. Adv. 6, eaaz6579 (2020).
Chu, F. et al. Adoptive transfer of immunomodulatory M2 macrophages suppresses experimental autoimmune encephalomyelitis in C57BL/6 mice via blockading NF-kappaB pathway. Clin. Exp. Immunol. 204, 199–211 (2021).
Ebrahimi, L. et al. Transplantation of decellularised human amniotic membranes seeded with mesenchymal stem cell-educated macrophages into animal models. J. Biomed. Mater. Res. B Appl. Biomater. 110, 1637–1650 (2022).
Li, B. et al. Effect of different types of macrophages on hepatic fibrosis in Echinococcus granulosus mice. Biomed. Pharmacother. 117, 109178 (2019).
Vagnozzi, R. J. et al. An acute immune response underlies the benefit of cardiac stem cell therapy. Nature 577, 405–409 (2020).
Chamberlain, C. S. et al. Extracellular vesicle-educated macrophages promote early Achilles tendon healing. Stem Cells 37, 652–662 (2019).
Han, G. H. et al. Transplantation of tauroursodeoxycholic acid-inducing M2-phenotype macrophages promotes an anti-neuroinflammatory effect and functional recovery after spinal cord injury in rats. Cell Prolif. 54, e13050 (2021).
Podaru, M. N. et al. Reparative macrophage transplantation for myocardial repair: a refinement of bone marrow mononuclear cell-based therapy. Basic Res. Cardiol. 114, 34 (2019).
Murray, P. J. Macrophage polarization. Annu. Rev. Physiol. 79, 541–566 (2017).
Koba, C. et al. Therapeutic effect of human iPS-cell-derived myeloid cells expressing IFN-beta against peritoneally disseminated cancer in xenograft models. PLoS ONE 8, e67567 (2013).
Netea, M. G. & Joosten, L. A. Master and commander: epigenetic regulation of macrophages. Cell Res. 26, 145–146 (2016).
Freund, E. C. et al. Efficient gene knockout in primary human and murine myeloid cells by non-viral delivery of CRISPR-Cas9. J. Exp. Med. 217, e20191692 (2020).
Na, Y. R. et al. Protein kinase A catalytic subunit is a molecular switch that promotes the pro-tumoral function of macrophages. Cell Rep. 31, 107643 (2020).
Racanelli, A. C. & Ding, B. S. Manmade macrophage offers a new therapy for pulmonary alveolar proteinosis. Am. J. Respir. Crit. Care Med. 198, 297–298 (2018).
Lee, R. H. et al. Intravenous hMSCs improve myocardial infarction in mice because cells embolized in lung are activated to secrete the anti-inflammatory protein TSG-6. Cell Stem Cell 5, 54–63 (2009).
Eggenhofer, E. et al. Mesenchymal stem cells are short-lived and do not migrate beyond the lungs after intravenous infusion. Front. Immunol. 3, 297 (2012).
Karp, J. M. & Leng Teo, G. S. Mesenchymal stem cell homing: the devil is in the details. Cell Stem Cell 4, 206–216 (2009).
Faradji, A. et al. Large scale isolation of human blood monocytes by continuous flow centrifugation leukapheresis and counterflow centrifugation elutriation for adoptive cellular immunotherapy in cancer patients. J. Immunol. Methods 174, 297–309 (1994).
Andreesen, R. et al. Adoptive transfer of tumor cytotoxic macrophages generated in vitro from circulating blood monocytes: a new approach to cancer immunotherapy. Cancer Res. 50, 7450–7456 (1990).
Andreesen, R., Hennemann, B. & Krause, S. W. Adoptive immunotherapy of cancer using monocyte-derived macrophages: rationale, current status, and perspectives. J. Leukoc. Biol. 64, 419–426 (1998).
Saez-Ibanez, A. R. et al. Landscape of cancer cell therapies: trends and real-world data. Nat. Rev. Drug Discov. 21, 631–632 (2022).
Mao, R. et al. Peritoneal M2 macrophage transplantation as a potential cell therapy for enhancing renal repair in acute kidney injury. J. Cell Mol. Med. 24, 3314–3327 (2020).
Funding
S.S. was supported by funding from the Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Science & ICT (2022M3E5F2018261, 2020R1A2C2010202), and the Korea Drug Development Fund funded by the Ministry of Science and ICT, Ministry of Trade, Industry, and Energy, and Ministry of Health and Welfare (HN22C0644). Y.N. was supported by NRF (2021R1A2C2010219), and SNUH Research Fund (0320223010, 0320210190). S.K. was supported by NRF grant funded by the Korea government (MSIT) (2022R1C1C2010114).
Author information
Authors and Affiliations
Contributions
Y.R.N. and S.H.S. conceptualized the study. Y.R.N. and S.W.K. analyzed the data. Y.R.N., S.W.K., and S.H.S. wrote the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Na, Y.R., Kim, S.W. & Seok, S.H. A new era of macrophage-based cell therapy. Exp Mol Med 55, 1945–1954 (2023). https://doi.org/10.1038/s12276-023-01068-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s12276-023-01068-z
This article is cited by
-
Macrophage-based therapeutic approaches for cardiovascular diseases
Basic Research in Cardiology (2024)
