
Abstract
Adult peak bone mass is related to birth weight, suggesting it could be affected by fetal growth pattern. Small-for-gestational-age (SGA) newborns have lower bone mineral content (BMC), but what about adapted-for-gestational-age (AGA) newborns with fetal growth restriction? The purpose of the study was to determine the respective role of birth weight and fetal growth pattern on BMC. Full-term newborns from SGA high-risk pregnancies were included (n = 185). Estimated fetal weight percentiles were measured monthly from mid-gestation to birth, and restricted fetal growth (FGR) was defined as a loss by more than 20 percentiles. BMC was measured at birth, using dual x-ray absorptiometry. Newborns were SGA (n = 56) or AGA (n = 129). Newborns with FGR (n = 111) were AGA (n = 71) or SGA (n = 41). BMC was significantly lower in SGA than AGA (1.48 ± 0.02 vs. 1.87 ± 0.04 g/cm) and lower when FGR irrespective of birth weight (1.66 g/cm ± 0.03 vs. 1.89 g ± 0.05). In multivariate analysis, FGR and SGA were significant and independent predictors of low BMC. In conclusion, fetal growth pattern affects BMC not only in SGA infants but also when birth weight is maintained in the normal range.
Similar content being viewed by others

Main
The peak bone mass of an individual depends upon growth and mineralization during the first two decades of life. However, a proportion of the variance of bone mineral content (BMC) found in the general population cannot be explained by genetic factors or childhood environment (1,2). Epidemiologic studies have suggested that part of this residual variation might be explained by the growth pattern in infancy (3) and probably during fetal development. Linear fetal growth is high during the last two trimesters of pregnancy, and fetal bone mineralization increases toward the end of pregnancy (4). Previous studies on a small number of newborns have shown that being born small for gestational age (SGA) was for a strong determinant of bone metabolism. BMC is lower in SGA infants at birth and is associated with a decrease in osteocalcin plasma level, suggesting that fetal mineralization is affected by fetal growth pattern (5,6). Moreover, prospective data in adult subjects indicate that bone mass and BMC are associated with birth weight after adjustment for environmental factors and body size at the time of investigation (7). However, birth weight results from fetal growth in utero. In addition, to gestational age and gender, other pregnancy characteristics, such as maternal height and weight before pregnancy, parity and ethnicity account for a large part of variation in fetal growth velocity and weight at birth. On the one hand, small babies who are small simply as a result of adaptation to maternal size can be separated from those who have suffered from restricted fetal growth (FGR). On the other hand, infants with appropriate for gestational age (AGA) birth weight can fail to reach their genetic potential of growth because of a real FGR. Birth weight by itself is not sufficient to identify FGR then. It has recently been shown that customized fetal growth estimation, adjusting for maternal and fetal characteristics, allows precise evaluation of fetal growth restriction by identifying newborns who have failed to reach their genetic potential of growth (8–10) and newborns at high risk of adverse perinatal outcome. The purpose of this study was to determine the respective roles of birth weight and FGR on BMC at birth, using the method of customized fetal growth. We hypothesized that not only birth weight per se but also FGR would affect BMC at birth.
METHODS
Subjects.
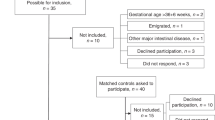
The study population consists of 185 newborns included between May 2004 and May 2007 in the CASyMIR cohort, a French prospective cohort exploring the metabolic consequences of being born SGA in early infancy. The infants were born from white women recruited during their first or second trimester of pregnancy in the maternity of the Robert Debré Hospital in Paris and considered as high risk of SGA pregnancies. The inclusion criteria were preexisting hypertension, smoking more than five cigarettes per day, a history of SGA in a previous pregnancy or among both parents, a history of pregnancy-induced hypertensive disorder, maternal height less than 152 cm corresponding to 2 SD for French women, uterine malformations, abnormal uterine or umbilical uterine arteries Doppler, and small fetal size at second trimester ultrasound examination. The date of conception was determined from the ultrasound examination performed at 12 wk of gestation.1
Birth weight of newborns was recorded within 10 g by midwives, using an electronic scale. Birth length was measured on a standard infants' measuring board within millimeter. Dual x-ray absorptiometry scan was performed in all newborns on the third day of life. The study protocol was approved by the ethical committee of Paris—Saint Louis Medical School (Paris 7 University), and all parents gave written informed consent.
Assessment of fetal growth.
Fetal growth was assessed every 4 wk by ultrasound from 22 to 36 wk of gestation. All four ultrasound scans were performed by the same observer for each woman under a standardized protocol according to the guidelines of College des Echographistes de France (Rapport du comité technique de l'echographie de diagnostic prenatal, collège français d'échographie fetale, Avril 2005, http://www.cfef.og). Estimated fetal weight (EFW) was calculated using the second Hadlock formula, which includes abdominal, head circumferences, and femur length measurements (11). The customized fetal and birth weight percentiles were calculated for each case with a computer program that adjusts for parity, gender, maternal weight and height, and ethnic group March 2007 (Gestation related optimal weight program. Software version 5.15 and Centile calculator software v5.12.1 March 2007, http://www.gestation.net). Coefficients for these physiologic variables (based on 40,000 ultrasound-dated pregnancies from Nottingham) are contained in the software. Intrauterine growth velocity was calculated as the change in EFW percentiles from 22 wk of gestation until birth (12). Fetal growth restriction was defined as a reduction of EFW by 20 percentiles or more and newborns were divided into three groups: newborns with no reduction of EFW percentile [regular growth (NG)], newborns with a reduction in EFW by less than 20 percentiles [intermediate growth (IG)], and newborns with a reduction in EFW by 20 percentiles or more (FGR). At birth, SGA was defined as birth weight equal or below the 10th and AGA—above the 10th percentile according to the French reference curves (13).
Measurement of body composition.
All BMC measurements were performed by using the same dual x-ray absorptiometry scan (Lunar Prodigy DXP Pro, GE medical Systems, Madison, WI). Scans were analyzed by using a specific software for small body weight (14,15). Radiation dose was 1.8 μGy according to the constructor. Coefficient of variation for BMC measurement is around 1.95% in animal studies (16) and around 2.4% for newborns in vivo, according to literature (17). Daily quality assurance tests were performed prior measurements. Newborns were placed in the supine position and the whole body was scanned, beginning at the top of the head and moving in a rectilinear pattern down the body to the feet. No sedation was used. Measurements were performed having the baby asleep. If significant movement were encountered, the scan was stopped and repeated. Total body mineral content was measured in grams. The total body scan area was divided into two regions of interest selected and analyzed separately: the head or cephalic mineral content (CMC) and the rest of the body (trunk, pelvis, upper and lower limbs) or trunk and limbs mineral content (TLMC). For head segmentation, a horizontal line above the shoulders was adjusted to immediately below the chin. BMC, CMC, and TLMC were measured in grams and are expressed as grams per centimeter of body size to adjust to body size.
Statistical analysis.
All analyses were performed using the JMP software version 5.1 (SAS Inc. Meylan, France). Data are given as mean ± SD. Chi-square test was used to compare proportions between groups. Continuous variables were compared using analysis of variance in univariate models. To further assess the effect of birth weight and fetal growth restriction on BMC, a multivariate linear model was built including gestational age, gender, maternal smoking, and seasonality at birth as covariates.
RESULTS
Mineral content related to birth weight and fetal growth.
The subjects' characteristics are shown in Table 1. One hundred eighty-five full-term newborns have been included in this study (92 boys and 93 girls). In this population, 56 infants were classified as SGA and 129 as AGA. Using our criteria, 73 newborns experienced normal or subnormal growth. By contrast, 112 newborns experienced FGR. Gestational age and gender were not different between the three groups, whereas caesarean sections were more frequent in the FGR group than in the IG and NG groups (28.6% vs. 18.7% and 10.2%, respectively p = 0.0028). FGR was present in most of the SGA newborns (77%) and in 55% of AGA subjects. In both SGA and AGA, the main risk factors of fetal growth restriction were maternal smoking, abnormal Doppler measurements, and history of SGA in previous pregnancies.
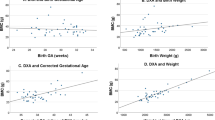
Figure 1 shows BMC according to birth weight. As expected, total BMC was lower in SGA infants than in AGA newborns (1.48 ± 0.02 g/cm vs. 1.87 ± 0.04 g/cm). CMC and TLMC were studied separately, to further analyze which body compartment was affected by fetal growth restriction. CMC and TLMC were both lower in SGA children (CMC: 0.66 g/cm ± 0.01 in SGA vs. 0.84 g/cm ± 0.02 in AGA; TLMC: 0.78 g/cm ± 0.02 in SGA and 1.03 g/cm ± 0.03 in AGA).

Total bone mineral content (total BMC), Cranium mineral content (CMC) and trunk and limbs mineral content (TLMC) in SGA newborns (▪) and AGA newborns (□). *p < 0.05, adjusted for gestational age and gender.
Figure 2A shows total BMC, CMC, and TLMC of the infants with respect to fetal growth irrespective of birth weight. BMC was not significantly different between NG and IG groups. However, it was decreased in case of FGR irrespective of birth weight. Total BMC was lower in FGR group (1.66 g/cm ± 0.03) compared with IG and NG group, (1.86 g ± 0.04 and 1.89 g ± 0.05, respectively). The lower total BMC in newborns with restricted growth was associated with a decrease in BMC of trunk and limbs. TLMC was lower in FGR group (TLMC: 0.89 g/cm ± 0.02 in FGR, 1.04 g/cm ± 0.03 in IG, and 1.06 g/cm ± 0.03 in NG), whereas CMC was not significantly different between the groups. Similar results were found when comparing BMC, CMC, and TMLC in AGA newborns among different patterns of fetal growth (Fig. 2B). BMC and TLMC were lower in the FGR groups (BMC: 1.8 g ± 0.03 in FGR, 2.0 g ± 0.08 in IG, and 1.95 ± 0.05 in NG; TLMC: 0.98 g/cm ± 0.02 in FGR, 1.13 g/cm ± 0.05 in IG, and 1.10 g/cm ± 0.03 in NG). In SGA newborns, BMC and TLMC were lower as well in FGR (Fig. 2C), but this difference did not reach statistical significance because of the small number of SGA babies in IG and NG groups (BMC: 1.42 g/cm ± 0.04 in FGR, 1.59 g/cm ± 0.03 in IG, and 1.62 g/cm ± 0.09 in NG; TLMC: 0.74 g/cm ± 0.03 in FGR, 0.86 g/cm ± 0.08 in IG, and 0.9 g/cm ± 0.07 in NG).

Total bone mineral content (total BMC), Cranium mineral content (CMC) and limbs and trunk mineral content (TLMC) and fetal growth pattern, in the whole cohort (A) and in relation with birth weight: AGA newborns (B) or SGA newborns (C) regular growth (NG, □); intermediate growth (IG,  ); restricted growth (FGR, ▪) (*p < 0.05, adjusted for gestational age and gender).
); restricted growth (FGR, ▪) (*p < 0.05, adjusted for gestational age and gender).
Determinants of mineral content.
Determinants of mineral content at birth were assessed using a multivariate analysis (β coefficients and adjusted p values are shown in Table 2, where BMC was adjusted for neonatal and maternal factors). Fifty-seven percent of the variance of BMC at birth was explained by the significant determinants included in the model: gestational age, being SGA, FGR, and maternal smoking (r2 = 0.57, p < 0.0001). As expected, BMC was strongly correlated to SGA status, but was also associated to fetal growth restriction in both SGA and AGA newborns. SGA was independently and significantly associated with a decreased of BMC by −0.0099 g/cm (p < 0.0001) and FGR with a decreased by −0.006 g/cm (p = 0.001). Moreover, the effect of FGR was further accentuated in SGA newborns (−0.003 g/cm, p < 0.0001) as evidenced by the statistical negative interaction between SGA or AGA and FGR. BMC was also significantly associated to lower gestational age and maternal smoking during pregnancy. BMC, however, was not related to the season of birth or to the way of delivery nor to maternal BMI.
DISCUSSION
Factors associated with BMC were studied in newborns and we report that both birth weight and fetal growth pattern affect BMC. BMC is reduced not only in SGA but also when birth weight is maintained in the normal range after fetal growth restriction. BMC in children and in adults is affected by intrauterine and early postnatal events. In a cohort of adults, it has been reported that birth weight was a significant predictor of BMC some seven decades later (7). This relationship was independent of known adult lifestyle determinant of bone loss such as physical activity, low calcium intake, or cigarette smoking. It also remained significant after adjustment for age, gender, and adult height, suggesting that intrauterine environmental factors that influence the fetal growth pattern could have long-term effects. This lower BMC seems to be present already at birth in subjects born SGA. Indeed, in the present study, BMC at birth was lower in SGA newborns than in AGA newborns. We hypothesized that BMC could be additionally affected by fetal growth restriction, a feature that can be observed not only in SGA infants but also in AGA infants. For the purpose of the study, FGR was defined as the failure to reach the genetic potential of growth using the customized fetal growth method. Fetal growth was monitored in a prospective way in all pregnant women. The EFW and the corresponding percentile were calculated from the data collected during antenatal ultrasound examinations using the method of the customized percentiles. Using this method, we were able to identify fetal growth restriction both in AGA and SGA newborns. FGR was associated with decreased total BMC (both in AGA and SGA newborns), which was related to a reduced mineral content in limbs and trunk, whereas CMC was maintained as previously reported (18). Moreover, fetal growth restriction remained a significant and independent predictor of low BMC irrespective of birth weight. Finally, both reduction in birth weight and in fetal growth affect BMC, the effect of FGR being even amplified in SGA newborns, as attested by the statistical interaction between these two parameters.
It has been previously reported that children born SGA have lower BMC and decreased bone formation marker (osteocalcin) compared with those born AGA even after allowing for seasonal variation (5). Osteocalcin gene is expressed in the late phase of bone formation (differentiation and mineralization period). Cord serum 1,25-(OH)2 vitamin D, the active metabolite of vitamin D that enhances uteroplacental calcium transfer, is lower in SGA than in AGA infants (19). One could think that the lower IGF-1 levels reported in SGA could affect collagen synthesis and bone matrix apposition rates. Indeed, IGF-1 stimulates preosteoblast cell replication and enhances osteoblastic collagen type 1 synthesis by increasing type 1 collagen transcript levels in osteoblasts (20,21). But, serum biochemical indices of collagen synthesis and degradation are similar in SGA and AGA children (22). Taking together, these data emphasize that reduced BMC in SGA infants is predominantly related to low mineral supply rather than defective matrix synthesis. We can speculate that in the present study, BMC is lower in the FGR group for the same reason.
During pregnancy, minerals are actively transported across the placenta to the fetal circulation against a concentration gradient and the fetus is totally dependent on maternal resources to acquire Ca2+, P, and Mg. The rate of maternofetal Ca2+ transfer increases dramatically during the last trimester of pregnancy (from 24 wk to term gestation), with a peak accretion rates between 36 and 38 wk gestation (19). Approximately, two-thirds of total body Ca2+ accumulated in a healthy term human fetus is transported during the last trimester of pregnancy (23). Conditions affecting placenta nutrient transfer at that time are also likely to affect fetal bone mineralization. According to our results, in the FGR group, the main risk factors were uteroplacental vascular abnormalities and maternal smoking. Maternal smoking, reported to influence skeletal growth, acts through different mechanisms. The most widely cited are impaired placental function, reduced uteroplacental blood flow, or effects on fetal oxygen carrying capacity (24,25). Another reported mechanism is a potential toxic effect of the heavy metal cadmium on fetal skeletal growth. Cadmium is present in high concentration as a contaminant in tobacco and has specific effects on trophoblast calcium transport (26).
Determination of factors affecting BMC is important because osteoporosis as a risk factor for fracture is still a public health problem (27). The strong association between birth weight and BMC is pointing to the importance of fetal growth on skeletal development. Here, we have reported for the first time that impaired fetal growth has an impact on BMC irrespective of birth weight. An association between early postnatal growth and BMC was previously reported (28,29). Weight at 1 y has been reported as a significant predictor of BMC in the lumbar spine and femoral neck of women and lumbar spine in men some seven decades later in the Hertfordshire cohort (3). Accelerated growth in the first year has been furthermore associated with greater bone size and strength as assessed by peripheral quantitative computed tomography (30). In a Finnish cohort, childhood growth velocity was a major determinant of hip fracture risk in elderly (31). Taking together, these data support the concept that fetal and early postnatal growth determines BMC, bone growth, and the risk of osteoporosis later in life. Our results suggest that fetal growth could modulate this risk even when birth weight is protected within the normal range. Calcium supplementation in women with adequate dietary calcium intake during the pregnancy has shown to have no effect on BMC in newborn (32). The effect of calcium supplementation during childhood on fracture risk is still debated (33,34). Therefore, appropriate diet and medical assessment of postnatal growth seems to be the best medical practice in this situation.
In conclusion, fetal growth restriction is an important determinant of BMC at birth and can be considered as an independent predictor of fetal bone mineralization even when birth weight is maintained within the normal range. This effect is independent of low birth weight making the SGA babies with fetal growth restriction the more at risk of low BMC.
Abbreviations
- AGA:
-
appropriate for gestational age
- BMC:
-
bone mineral content
- CMC:
-
cephalic mineral content
- EFW:
-
estimated fetal weight
- FGR:
-
restricted fetal growth
- IG:
-
intermediate fetal growth
- NG:
-
regular fetal growth
- SGA:
-
small for gestational age
- TLMC:
-
trunk and link mineral content
References
Cadogan J, Eastell R, Jones N, Barker ME 1997 Milk intake and bone mineral acquisition in adolescent girls: randomised, controlled intervention trial. BMJ 315: 1255–1260
Friedlander AL, Genant HK, Sadowsky S, Byl NN, Gluer CC 1995 A two-year program of aerobics and weight training enhances bone mineral density of young women. J Bone Miner Res 10: 574–585
Cooper C, Cawley M, Bhalla A, Egger P, Ring F, Morton L, Barker D 1995 Childhood growth, physical activity, and peak bone mass in women. J Bone Miner Res 10: 940–947
Widdowson EM, Spray CM 1951 Chemical development in utero. Arch Dis Child 26: 205–214
Namgung R, Tsang RC, Specker BL, Sierra RI, Ho ML 1993 Reduced serum osteocalcin and 1,25-dihydroxyvitamin D concentrations and low bone mineral content in small for gestational age infants: evidence of decreased bone formation rates. J Pediatr 122: 269–275
Akcakus M, Kurtoglu S, Koklu E, Kula M, Koklu S 2007 The relationship between birth weight leptin and bone mineral status in newborn infants. Neonatology 91: 101–106
Gale CR, Martyn CN, Kellingray S, Eastell R, Cooper C 2001 Intrauterine programming of adult body composition. J Clin Endocrinol Metab 86: 267–272
Mongelli M, Gardosi J 1995 Longitudinal study of fetal growth in subgroups of a low-risk population. Ultrasound Obstet Gynecol 6: 340–344
de Jong CL, Gardosi J, Dekker GA, Colenbrander GJ, van Geijn HP 1998 Application of a customised birthweight standard in the assessment of perinatal outcome in a high risk population. Br J Obstet Gynaecol 105: 531–535
Clausson B, Gardosi J, Francis A, Cnattingius S 2001 Perinatal outcome in SGA births defined by customised versus population-based birthweight standards. BJOG 108: 830–834
Hadlock FP, Harrist RB, Sharman RS, Deter RL, Park SK 1985 Estimation of fetal weight with the use of head, body, and femur measurements—a prospective study. Am J Obstet Gynecol 151: 333–337
Stratton JF, Scanaill SN, Stuart B, Turner MJ 1995 Are babies of normal birth weight who fail to reach their growth potential as diagnosed by ultrasound at increased risk?. Ultrasound Obstet Gynecol 5: 114–118
Gardosi J, Chang A, Kalyan B, Sahota D, Symonds EM 1992 Customised antenatal growth charts. Lancet 339: 283–287
Rigo J, Nyamugabo K, Picaud JC, Gerard P, Pieltain C, De Curtis M 1998 Reference values of body composition obtained by dual energy X-ray absorptiometry in preterm and term neonates. J Pediatr Gastroenterol Nutr 27: 184–190
Picaud JC, Duboeuf F, Vey-Marty V, Delams P, Claris O, Salle BL, Rigo J 2003 First all-solid pediatric phantom for dual X-ray absorptiometry measurements in infants. J Clin Densitom 6: 17–23
Picaud JC, Rigo J, Nyamugabo K, Milet J, Senterre J 1996 Evaluation of dual-energy X-ray absorptiometry for body-composition assessment in piglets and term human neonates. Am J Clin Nutr 63: 157–163
Braillon PM, Salle BL, Brunet J, Glorieux FH, Delmas PD, Meunier PJ 1992 Dual energy x-ray absorptiometry measurement of bone mineral content in newborns: validation of the technique. Pediatr Res 32: 77–80
Koo WW, Walters J, Bush AJ, Chesney RW, Carlson SE 1996 Dual-energy X-ray absorptiometry studies of bone mineral status in newborn infants. J Bone Miner Res 11: 997–1002
Namgung R, Tsang RC 2003 Bone in the pregnant mother and newborn at birth. Clin Chim Acta 333: 1–11
Hock JM, Centrella M, Canalis E 1988 Insulin-like growth factor I has independent effects on bone matrix formation and cell replication. Endocrinology 122: 254–260
Ernst M, Froesch ER 1988 Growth hormone dependent stimulation of osteoblast-like cells in serum-free cultures via local synthesis of insulin-like growth factor I. Biochem Biophys Res Commun 151: 142–147
Namgung R, Tsang RC, Sierra RI, Ho ML 1996 Normal serum indices of bone collagen biosynthesis and degradation in small for gestational age infants. J Pediatr Gastroenterol Nutr 23: 224–228
Abrams SA 2003 Normal acquisition and loss of bone mass. Horm Res 60: 71–76
Shiverick KT, Salafia C 1999 Cigarette smoking and pregnancy I: ovarian, uterine and placental effects. Placenta 20: 265–272
Salafia C, Shiverick K 1999 Cigarette smoking and pregnancy II: vascular effects. Placenta 20: 273–279
Lin FJ, Fitzpatrick JW, Iannotti CA, Martin DS, Mariani BD, Tuan RS 1997 Effects of cadmium on trophoblast calcium transport. Placenta 18: 341–356
Cooper C, Melton L 1996 Magnitude and impact of osteoporosis and fractures. Ostoporosis. Academic press, San Diego pp 419–434
Cooper C, Fall C, Egger P, Hobbs R, Eastell R, Barker D 1997 Growth in infancy and bone mass in later life. Ann Rheum Dis 56: 17–21
Laitinen J, Kiukaanniemi K, Heikkinen J, Koiranen M, Nieminen P, Sovio U, Keinanen-Kiukaanniemi S, Jarvelin MR 2005 Body size from birth to adulthood and bone mineral content and density at 31 years of age: results from the northern Finlandbirth cohort study. Osteoporos Int 16: 1417–1424
Oliver H, Jameson KA, Sayer AA, Cooper C, Dennison EM 2007 Growth in early life predicts bone strength in late adulthood: the Hertfordshire Cohort Study. Bone 41: 400–405
Cooper C, Eriksson JG, Forsen T, Osmond C, Tuomilehto J, Barker DJ 2001 Maternal height, childhood growth and risk of hip fracture in later life: a longitudinal study. Osteoporos Int 12: 623–629
Koo WW, Walters JC, Esterlitz J, Levine RJ, Bush AJ, Sibai B 1999 Maternal calcium supplementation and fetal bone mineralization. Obstet Gynecol 94: 577–582
Kalkwarf HJ, Khoury JC, Lanphear BP 2003 Milk intake during childhood and adolescence, adult bone density, and osteoporotic fractures in US women. Am J Clin Nutr 77: 257–265
Winzenberg T, Shaw K, Fryer J, Jones G 2006 Effects of calcium supplementation on bone density in healthy children: meta-analysis of randomised controlled trials. BMJ 333: 775
Acknowledgements
The authors acknowledge the skilful technical assistance of Aurore Foureau.
Author information
Authors and Affiliations
Corresponding author
Additional information
This work was supported by a grant from the “Institut National de la santé et de la recherché médicale (INSERM)”. J.B. was supported by a fellowship from the “Institut Danone” (France, 2006). R.N. and R.V. were supported by a grant from the “Programme Charcot” (France).
Rights and permissions
About this article
Cite this article
Beltrand, J., Alison, M., Nicolescu, R. et al. Bone Mineral Content at Birth Is Determined Both by Birth Weight and Fetal Growth Pattern. Pediatr Res 64, 86–90 (2008). https://doi.org/10.1203/PDR.0b013e318174e6d8
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1203/PDR.0b013e318174e6d8
This article is cited by
-
Fetal femur length and risk of diabetes in adolescence: a prospective cohort study
Tropical Medicine and Health (2024)
-
Drug Treatment of Low Bone Mass and Other Bone Conditions in Pediatric Patients
Pediatric Drugs (2022)
-
There is No Link Between Birth Weight and Developmental Dysplasia of the Hip
Indian Journal of Orthopaedics (2021)
-
Could low birth weight and preterm birth be associated with significant burden of hip osteoarthritis? A systematic review
Arthritis Research & Therapy (2018)
-
Assessment of body composition in Wistar rat offspring by DXA in relation to prenatal and postnatal nutritional manipulation
Pediatric Research (2016)
