
Abstract
This longitudinal prospective study aimed to investigate the relationship between pituitary-adrenal responses and severity of retinopathy of prematurity (ROP) in 92 preterm, very low birth weight infants ≤ 30 wk gestation. The human corticotropin releasing hormone stimulation test was performed on these infants at D 7 and 14 of postnatal life. Univariate analysis revealed significant associations between severity of ROP and gestational age (r = −0.53, p < 0.0001), birth weight (r = −0.56, p < 0.0001), Apgar score at 1 min (r = −0.27, p < 0.05), Clinical Risk Index for Babies score (r = 0.48, p < 0.0001), duration of mechanical ventilation (r = 0.48, p < 0.0001), oxygen dependency (r = 0.48, p < 0.0001), and length of hospitalization (r = 0.49, p < 0.0001). The stage of ROP was also significantly associated with the basal and peak plasma ACTH (r > −0.22, p < 0.05) and peak serum cortisol (r = −0.21, p = 0.05) at d 7. Multivariate analysis using the classification and regression trees indicated that the two most influential risk factors affecting the development of advanced stages of ROP (≥ stage 3) were i) birth weight and ii) oxygen dependency at 28 d of life or at 36 wk postconceptional age. Our findings suggest that early endogenous or stimulated pituitary-adrenal responses are not independent risk factors associated with the development of severe ROP. Low birth weight and prolonged oxygen exposure are likely to be important factors that influence the degree of damage inflicted on the retina.
Similar content being viewed by others

Main
Recent advances in neonatal management, including the use of antenatal corticosteroids, surfactant replacement, and new forms of assisted ventilation, have paved the way for improvement in morbidity and mortality of preterm, VLBW (<1500 g) infants (1–3). ROP, however, remains a devastating disease and a significant cause of blindness and visual impairment that contributes to long-term neurologic sequelae of these vulnerable infants (4, 5). Thus far, no definitive prevention, other than judicious use of supplemental oxygen, is available for minimizing the incidence and severity of this serious condition (6, 7). As ROP is considered by some investigators to be an oxygen free radical disease (8) and occurs mainly in the most immature infants (9), treatments that can minimize the use of oxygen or enhance the maturity of body organ systems may potentially be beneficial for the management or prevention of this condition. Recent studies suggested that preterm infants, suffering from TAP, with low circulating cortisol levels, had an increased risk of developing systemic hypotension, patent ductus arteriosus, and oxygen free radical–related disease such as CLD (10–15). Corticosteroids have been shown to suppress preretinal and subretinal neovascularization in animal models (16–18), to up-regulate the expression of antioxidants such as superoxide dismutase (19, 20), and to stabilize or modulate the inflammatory response of capillary endothelium (21, 22). Hence, this group of drugs may be used to reduce the susceptibility of developing retinal vessels to oxidative injury, and assists in accelerating the maturation of retinal vasculature. In addition, recent reports suggest that the use of antenatal dexamethasone or a prolonged course of postnatal corticosteroids might decrease the severity of ROP (22, 23). This prospective study, therefore, aimed to investigate the relationship between endogenous or stimulated pituitary-adrenal responses and severity of ROP. Such a relationship would set the stage for clinical trials of physiologic doses of corticosteroids in the early postnatal period to prevent this disease.
The hCRH test was chosen to assess the pituitary-adrenal function of VLBW infants because we have previously demonstrated that the test is safe, reproducible, and capable of eliciting a consistent response similar to those of older children and adults (24). The hCRH test is also preferable to other hypothalamic-pituitary-adrenal (HPA) axis stimulation tests such as the insulin stress test, the metyrapone test, and the low-dose short-synacthen test, because these latter investigations are either unsuitable for use in preterm infants because of their potential side effects, not as sensitive as the hCRH test in demonstrating a mild degree of adrenal insufficiency, or do not assess the pituitary function of the axis (24, 25).
PATIENTS AND METHODS
Ophthalmologic examination for preterm infants.
Indirect ophthalmoscopy was performed for all preterm infants in the Neonatal Intensive Care Unit at the Prince of Wales Hospital, Hong Kong, who met the screening criteria for ROP: i) infants <32 wk gestation or <1500 g at birth, and ii) preterm infants (<37 wk gestation) receiving supplemental oxygen for >2 wk. Gestation assessment was by mother's last menstrual period, early ultrasound dating, and new Ballard score assessment after birth. The infants were first examined by ophthalmologists (A.K.H.K., B.S.M.T.) at 4 wk of postnatal age. All studied infants received 0.5% tropicamide and 1.25% phenylephrine for pupil dilatation. One drop of 4% amethocaine was instilled before opening the eye with a Cook's infant speculum. The zones and stages of vascularization were recorded for each eye. The stages of ROP were classified according to the International Classification of Retinopathy of Prematurity (26). The eyes were closely monitored every 2 wk, or more frequently if indicated, until discharge or death or until retinal vascularization was complete. Indirect laser retinopexy using diode or argon laser was performed if threshold disease was present.
Management of patients.
VLBW infants were looked after in a low-illumination environment with the incubators partially shaded by cloth. Eye shields were routinely used in infants receiving phototherapy. Infants requiring supplemental oxygen were continuously monitored by pulse oximetry. The target blood oxygen saturation levels were between 90% and 94%. Such levels of pulse oximetry target did not change with the identification of ROP. All studied infants received two doses of surfactant (Survanta, Abbott Laboratories, North Chicago, IL, U.S.A.) if they required mechanical ventilation but none received vitamin E supplementation.
hCRH test for preterm infants.
This prospective study was performed as part of a large study for assessing the relation between pituitary-adrenal responses and systemic hypotension or CLD (10, 27). The selection criteria of preterm infants for the hCRH test have been standardized as follows: i) gestational age <32 wk, ii) birth weight <1500 g, iii) no postnatal systemic or inhaled corticosteroids treatment before the hCRH test, and iv) possession of an indwelling arterial cannulae at d 7 of life. A second hCRH test was also performed if the arterial cannulae remained in situ at d 14. Infants were excluded if they had concurrent hypoglycemia, systemic infection, necrotizing enterocolitis, or major surgery in the preceding week.
We chose to perform the hCRH tests on d 7 and 14 of life. The reasons for selecting this time sequence have been explained previously (24). All tests were performed between 0800 h and 1000 h. The method of performing the hCRH test in preterm infants and the laboratory hormone assays have been standardized and described in detail in our previous studies (24, 28). In brief, synthetic hCRH (Ferring Pharmaceuticals Ltd., Arzneimittal, Wittland, Germany), 1 μg/kg, was given by bolus i.v. injection. Blood samples (0.5 mL) were obtained, immediately before hCRH administration (0 min), and at 15, 30, and 60 min after the injection. The plasma ACTH and serum cortisol concentrations were measured by double-antibody RIA and solid-phase RIA, respectively (24). Plasma ACTH concentration in picomoles per liter can be converted to picograms per milliliter by multiplying by a factor of 4.5; likewise, the conversion of serum cortisol concentration from nanomoles per liter to micrograms per deciliter can be achieved by dividing by 27.6.
Statistical analysis.
The descriptive statistics on demographic data were expressed as median and interquartile range. Spearman's correlation was used to assess the relationship between stages of ROP and i) clinical characteristics of the studied infants, and ii) circulating and stimulated hormone concentrations. In addition, Mann Whitney U test and χ2 tests were used to compare the clinical characteristics of infants with stage 0–2 ROP (Group 1) and those with threshold disease or stage 3 or higher ROP (Group 2—the severe ROP group). As the absolute plasma ACTH and serum cortisol levels, and the incremental rise in hormone concentrations between the basal and peak levels [i.e. the difference in plasma ACTH concentration between 0 and 15 min (ΔACTH0–15), and the difference in serum cortisol concentration between 0 and 30 min (ΔCortisol0–30)] are important in evaluating the adequacy of pituitary-adrenal responsiveness, Mann Whitney U test was also used to assess the circulating hormone concentrations at the corresponding time points between the two groups of patients. Univariate significant results (p < 0.05) were further subjected to multivariate analysis using the CART method (29). CART is a nonparametric, binary recursive-partitioning algorithm developed through a two-stage process. A complex tree is initially constructed through a sequence of optimal binary splits of a set of covariates. These covariates are then partitioned recursively into two subgroups that are most different with respect to the outcome. The partitioning continues until the dependent variable is separated into homogeneous subgroups. The second stage prunes the resulting complex tree to an optimal subtree that minimizes the overall classification error. This error rate is then estimated by a cross-validation method and is implemented by a pruning algorithm. The statistical tests were performed by SPSS for Windows (Release 11, SPSS Inc., Chicago, IL, U.S.A.) and S-Plus 2000 (Release 3, MathSoft Inc., Seattle, WA, U.S.A.), and the statistical analysis was performed on raw and logarithmically (Ln) transformed data where appropriate to correct the skewness of the results.
Ethical approval.
Ethical approval of the study was obtained from the research ethics committee of the Chinese University of Hong Kong. Informed parental consent was obtained for each case before commencement of the test.
RESULTS
Two hundred and twenty-six hCRH tests were performed on 137 VLBW infants at d 7 and 14 of postnatal age. The preliminary ACTH and cortisol results of this cohort have been compiled to provide a reference range for the hCRH test in VLBW infants (28). The findings indicated that peak plasma ACTH and serum cortisol occurred at 15 and 30 min, respectively (24, 28). The data concerning the relationship between hormones of the HPA axis and ROP have not been reported previously.
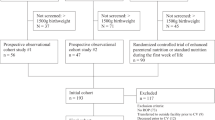
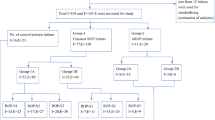
This study was carried out in the mid- and late 1990s (August 1994 to December 1996 and April 1998 to December 1999). The interruption was due to lack of funding of the program. As no patient above 30 wk gestation developed threshold disease and stage 3 or higher ROP, the analysis of data was, thus, confined to infants below this gestation and those who survived to term (i.e. allowing adequate time for complete ophthalmologic examination). One hundred and eighty-three VLBW infants, ≤ 30 wk gestation were born within the study periods. Of these infants, 25 died within the first 72 h of life, 21 were recruited to the early inhaled corticosteroid study (30), and 45 did not possess an arterial line or their parents were unwilling to take part in the study. Hence, a total of 92 infants were enrolled in the ROP study. None of the infants received postnatal corticosteroid therapy before the hCRH test. Sixty-nine and 23 infants belonged to Group 1 (stage 0–2) and Group 2 (≥ stage 3), respectively. Among infants in Group 2, 11 of 23 (48%) underwent laser treatment.
Eight infants missed the first hCRH test, of whom five belonged to Group 1 and three belonged to Group 2. Twenty-seven infants were not tested on d 14. Twenty-two and five belonged to Group 1 and Group 2, respectively. The reasons for missing the hCRH test were due to systemic infection, necrotizing enterocolitis, or lack of an indwelling arterial line when due for the investigation. Six of the 27 infants not tested on d 14 were commenced on early dexamethasone because of severe lung disease. Two infants belonged to Group 1 and four belonged to Group 2. The clinical characteristics of the infants are summarized in Table 1. As expected, Group 2 infants were significantly more immature and sicker than infants of Group 1 (Table 1). There were, however, no significant differences in plasma ACTH and serum cortisol at either time point or in incremental ACTH (ΔACTH0–15) and cortisol (ΔCortisol0–30) between the two groups (Table 2).
Univariate analysis using Spearman's correlation revealed significant associations between stages of ROP and gestational age (r = −0.53, p < 0.0001), birth weight (r = −0.56, p < 0.0001), Apgar score at 1 min (r = −0.27, p < 0.05), CRIB score (r = 0.48, p < 0.0001), duration of mechanical ventilation (r = 0.48, p < 0.0001), oxygen dependency (r = 0.40, p < 0.0001) and length of hospitalization (r = 0.49, p < 0.0001). The severity of ROP was also significantly associated with the basal and peak plasma ACTH (r > −0.22, p < 0.05) and the peak serum cortisol (r = −0.21, p = 0.05) at d 7. In contrast, none of the hormone levels at d 14 or ΔACTH0–15 and ΔCortisol0–30 correlated significantly with the severity of the condition. There was also no significant correlation between the severity of ROP and acute respiratory indices, including OI and AaDO2, recorded within the first 14 d of life.
Univariate significant factors, including gestational age, birth weight, Apgar score at 1 min, CRIB score, duration of mechanical ventilation, oxygen dependency at 28 d of life and at 36 wk postconceptional age, use of postnatal dexamethasone, basal and peak plasma ACTH, and peak serum cortisol at d 7, were further subjected to multivariate CART analysis. Statistical significance between stages of ROP and ACTH or cortisol was lost after the analysis. The two most influential factors affecting the severity of ROP were i) birth weight and ii) oxygen dependency at 28 d of life or at 36 wk postconceptional age. The CART model accurately predicted 83% of infants (10/12 patients) <780 g for developing severe ROP (≥stage 3), whereas the accuracy for infants >918 g having a milder disease (stage 0–2) was 91% (60/66 patients). In addition, the model correctly predicted 80% of infants (4/5 patients) with birth weight ranged between 780 and 918 g who did not require oxygen supplementation at 28 d or 36 wk for having the mild stages. Conversely, the accuracy for the same group of infants who required prolonged oxygen supplementation for developing the severe stages was 67% (6/9 patients). The overall sensitivity, specificity, and positive and negative predictive values of these two factors for predicting advance stages of ROP were 70%, 93%, 76%, and 90%, respectively.
DISCUSSION
To our knowledge, this is the largest study using the hCRH stimulation test to assess the HPA axis response in preterm infants, and the first report to investigate the relationship between endogenous or stimulated pituitary-adrenal hormone responses and ROP. The 61% incidence of ROP in the current study is similar to those reported in previous trials (23, 31). Our results suggest that there is a negative but weak association between advanced stages of ROP and peak plasma ACTH or serum cortisol concentrations. However, it has also been shown that a correlation exists between gestational age and serum cortisol due to progressive maturation of the HPA axis (32). Multivariate CART analysis was, therefore, used to identify the relative importance of different potential risk factors. The findings indicated that other factors such as gestational age, birth weight, CRIB score, and CLD (oxygen dependency >28 d of life or >36 wk of postconceptional age) are more influential than endogenous or stimulated pituitary-adrenal hormonal responses in correlating with the evolution of ROP. In fact, the two most important risk factors predisposing to the development of stage 3 or higher ROP are birth weight and prolonged requirement for oxygen supplementation. These results closely correspond to the findings observed by Hussain et al.(9), which demonstrate that gestational age and days on supplemental oxygen therapy are strongly associated with the development of ROP. The latter study also indicates that infants <28 wk gestation or with birth weight <1000 g are at increased risk of requiring retinal surgical intervention (9). VEGF, an oxygen-regulated factor, and IGF-I, a somatic growth factor, are important mediators associated with the pathogenesis of ROP (33). Preterm infants with low birth weight tend to have low circulating IGF-I level (34). VEGF, in the absence of IGF-I, is unable to stimulate normal retinal vascular development, and thereby increases the likelihood of developing clinical ROP (35). In addition, there was no significant difference in hormone concentrations at any corresponding time points or incremental rise in hormone concentrations between Group 1 and Group 2 infants. There were also no significant differences in plasma ACTH and serum cortisol even when the above comparisons were limited to infants <27 wk gestation [i.e. when there was no statistical difference in gestational age between the two groups; median peak plasma ACTH were 10.3 and 8.6 pmol/L, and median peak serum cortisol were 425 and 414 nmol/L for Groups 1 (n = 18) and 2 (n = 15), respectively]. Thus, the overall results suggest that the endocrine factor per se probably plays a minor or secondary role in predisposition to severe ROP.
It is known that the etiology of ROP is likely to be complex and multifactorial, and many etiologic factors are interrelated. However, the influence of corticosteroid treatment on ROP is controversial. A recent animal study suggests that rodent pups exposed to dexamethasone and oxygen have significantly lower retinopathy scores compared with pups exposed to oxygen alone (36). The use of corticosteroid therapy in preterm infants has been reported to have protective (22, 23), harmful (37–40), and no effect (41–43) on ROP. Similarly, early (<96 h), moderately early (7–14 d), and delayed postnatal corticosteroid treatment (>3 wk), has been associated with a reduction, no effect, and an increased risk of developing severe ROP, respectively (2, 44, 45). We postulate that the inconsistency and conflicting observations may be related to i) the retrospective nature (22, 37–43), ii) the relatively small sample size (46, 47), iii) the timing of corticosteroids administration (46–50), iv) a weak association between HPA axis hormones and ROP, and v) an interdependent relationship between various risk factors. Suppression of VEGF expression by hyperoxia and low IGF-1 level in premature low birth weight infants can prevent normal vascularization of the retina in the early postnatal period (phase 1 of ROP). Conversely, inhibition of these factors during the neovascular phase (phase 2 of ROP) may minimize the destructive retinal neovascularization process (33). Hence, the timing of therapeutic interventions, such as the use of corticosteroids or replacement of IGF-I, may be critical in affecting the disease process (35). Although this study series failed to show a direct association between TAP and CLD or prolonged oxygen requirement (27), other investigators have suggested a connection between these factors (11–13). Thus, a plausible integrated mechanism could be that premature and extremely low birth weight infants with a higher incidence of TAP are more prone to require prolonged oxygen supplementation (11–13), which ultimately increases the risk of oxidative damage to the premature retina. Our findings suggest that low birth weight (closely associated with prematurity) and prolonged oxygen exposure are likely to be the primary and essential risk factors involved in the development of severe ROP, and low circulating serum cortisol may probably act as a secondary link for progression to chronic lung damage.
The results also indicate that the severity of respiratory distress syndrome per se, as reflected by OI and AaDO2 gradients, does not contribute significantly to the development of advanced stages of retinal disease. These findings suggest that an acute or transient increase in mechanical ventilation or oxygen requirement is probably not the major risk factor predisposing to severe ROP. In contrast, chronic oxygen exposure appears to be more damaging to the retina, as cessation of normal retinal vascular growth and subsequent retinal neovascularization are dynamic but slow processes that would not be completed within the first few weeks of postnatal life.
Similar to previous studies investigating the pathogenesis and etiologic factors of ROP, the current exercise also suffers from its own intrinsic limitations. First, although the current series represents one of the largest studies of pituitary and adrenal responses in preterm infants, the moderate sample size may still not have sufficient statistical power to detect a small difference in the risk factors between the two groups. Subgroup analysis, such as excluding infants who received antenatal or postnatal corticosteroids, is not feasible as the number of untreated infants would be too few to be considered for a meaningful analysis. Second, the multifactorial etiology of the disease and the interdependent relationship between various risks factors further complicates the issue. We have, however, tried to minimize some of the important confounders by standardizing the time schedule of performing the hCRH tests and using a sophisticated mathematical model (CART) to identify the relative importance of individual factors. Third, despite evaluating a comprehensive list of risk factors, some less recognized or unidentified factors might not have been included in the statistical model. Other factors such as perinatal and postnatal sepsis, systemic fungal infection, and use of bronchodilators and diuretics have not been studied. Nonetheless, the inclusion of such factors would not have altered the findings of the multivariate analysis, as we did not find a significant association between early serum cortisol level and ROP. The importance of these risk factors, in particular sepsis, in causing ROP could not be assessed by the current study. Fourth, it is arguable that the studied infants might represent a sicker category of patients, as all required arterial line monitoring soon after birth. The relatively liberal use of indwelling arterial lines (10) and the balanced distribution of normotensive and hypotensive infants in our cohort (10), suggest that a wide spectrum of VLBW infants with different severity of TAP and disease conditions have been studied in this series.
CONCLUSIONS
In summary, circulating plasma ACTH and serum cortisol levels show only a weak correlation with the severity of ROP, suggesting at best a minor contributory but not a substantive effect. Multivariate CART analysis identifies birth weight and CLD to be the two most important risk factors associate with advanced stages of ROP. Further, the severity of the initial lung disease, as reflected by OI and AaDO2 gradients within the first 14 d of life, does not appear to play a major role in the pathogenic process, whereas prolonged oxygen exposure greater than 28 d or more than 36 wk postconceptional age is associated with significant damage to the retina. Although, at first glance, our results suggest that corticosteroids replacement in the early postnatal period may not be particularly useful for prophylaxis of ROP, there is some preliminary evidence to suggest their beneficial role in prevention of CLD (2, 51). Whether physiologic doses of corticosteroids administered in the early postnatal period would translate into a reduced requirement for supplemental oxygen and a subsequent decrease in the incidence of ROP will require a large, multi-center, randomized control study to determine their effects. Our present data suggest that endogenous or stimulated pituitary-adrenal responses are not independent risk factors associated with the development of severe ROP.
Abbreviations
- AaDO2:
-
alveolar-arterial oxygen gradients
- CART:
-
classification and regression trees
- CLD:
-
chronic lung disease
- CRIB:
-
Clinical Risk Index for Babies
- hCRH:
-
human corticotropin releasing hormone
- HPA:
-
hypothalamic-pituitary-adrenal
- OI:
-
oxygenation index
- ROP:
-
retinopathy of prematurity
- TAP:
-
transient adrenocortical insufficiency of prematurity
- VEGF:
-
vascular endothelial growth factor
- VLBW:
-
very low birth weight
References
Crowley P 2002 Prophylactic corticosteroids for preterm birth (Cochrane Review). In: The Cochrane Library, Issue 4. Update Software, Oxford, UK
Halliday HL, Ehrenkranz RA 2003 Early postnatal (< 96 hours) corticosteroids for preventing chronic lung disease in preterm infants (Cochrane Review). In: The Cochrane Library, Issue 1. Update Software, Oxford, UK
Courtney SE, Durand DJ, Asselin JM, Hudak ML, Aschner JL, Shoemaker CT, Neonatal Ventilation Study Group 2002 High-frequency oscillatory ventilation versus conventional mechanical ventilation for very-low-birth-weight infants. N Engl J Med 347: 643–652
The STOP-ROP Multicenter Study Group 2000 Supplemental therapeutic oxygen for prethreshold retinopathy of prematurity (STOP-ROP), a randomized, controlled trial. I: primary outcomes. Pediatrics 105: 295–310
Phelps DL 2001 Retinopathy of prematurity: clinical trials. Neoreviews 2: e167–e172
Bancalari E, Flynn J, Goldberg RN, Bawol R, Cassady J, Schiffman J, Feuer W, Roberts J, Gillings D, Sim E 1987 Influence of transcutaneous oxygen monitoring on the incidence of retinopathy of prematurity. Pediatrics 79: 663–669
Gaynon MW, Stevenson DK, Sunshine P, Fleischer BE, Landers MD 1997 Supplemental oxygen may decrease progression of prethreshold disease to threshold retinopathy of prematurity. J Perinatol 17: 434–438
Saugstad OD 1990 Oxygen toxicity in the neonatal period. Acta Paediatr Scand 79: 881–892
Hussain N, Clive J, Bhandari V 1999 Current incidence of retinopathy of prematurity, 1989–1997. Pediatrics 104: e26
Ng PC, Lee CH, Lam CWK, Ma KC, Fok TF, Chan IHS, Wong E 2004 Transient adrenocortical insufficiency of prematurity (TAP) and systemic hypotension in very low birth weight infants. Arch Dis Child ( in press)
Watterberg KL, Gerdes JS, Cook KL 2001 Impaired glucocorticoid synthesis in premature infants developing chronic lung disease. Pediatr Res 50: 190–195
Watterberg KL, Scott SM, Backstrom C, Gifford KL, Cook KL 2000 Links between early adrenal function and respiratory outcome in preterm infants: airway inflammation and patent ductus arteriosus. Pediatrics 105: 320–324
Huysman MWA, Hokken-Koelega ACS, De Ridder MAJ, Sauer PJJ 2000 Adrenal function in sick very preterm infants. Pediatr Res 48: 629–633
Helbock HJ, Insoft RM, Conte FA 1993 Glucocorticoid responsive hypotension in extremely low birth weight newborns. Pediatrics 92: 715–717
Ng PC, Lam CWK, Fok TF, Lee CH, Ma KC, Chan IHS, Wong E 2001 Refractory hypotension in preterm infants with adrenocortical insufficiency. Arch Dis Child 84: F122–F124
Danis RP, Bingaman DP, Yang Y, Ladd B 1996 Inhibition of preretinal and optic nerve head neovascularization in pigs by intravitreal triamcinolone acetonide. Ophthalmology 103: 2099–2104
Ishibashi T, Miki K, Sorgenti N, Patterson R, Ryan SJ 1985 Effects of steroids on experimental subretinal neovascularization in the subhuman primate. Arch Ophthalmol 3: 708–711
Lawas-Alejo PA, Slivka S, Hernandez H, Bry K, Hallman M 1999 Hyperoxia and glucocorticoid modify retinal vessel growth and interleukin-1 receptor antagonist in newborn rabbits. Pediatr Res 45: 313–317
Randhawa P, Hass M, Frank L, Massaro D 1986 Dexamethasone increases superoxide dismutase activity in serum-free rat fetal lung organ cultures. Pediatr Res 20: 895–898
Frank L, Lewis PL, Sosenko IR 1985 Dexamethasone stimulation of fetal rat lung antioxidant enzyme activity in parallel with surfactant stimulation. Pediatrics 75: 569–574
Cronstein BN, Kimmel SC, Levin RI, Martiniuk F, Weissmann G 1992 A mechanism for the antiinflammatory effects of corticosteroids: the glucocorticoid receptor regulates leukocyte adhesion to endothelial cells and expression of endothelial-leukocyte adhesion molecule 1 and intercellular adhesion molecules 1. Proc Natl Acad Sci USA 89: 9991–9995
Sobel DB, Philip AGS 1992 Prolonged dexamethasone therapy reduces the incidence of cryotherapy for retinopathy of prematurity in infants of less than 1 kilogram birth weight with bronchopulmonary dysplasia. Pediatrics 90: 529–533
Higgins RD, Mendelsohn AL, DeFeo MJ, Ucsel R, Hendricks-Munoz KD 1998 Antenatal dexamethasone and decreased severity of retinopathy of prematurity. Arch Ophthalmol 116: 601–605
Ng PC, Wong GWK, Lam CWK, Lee CH, Wong MY, Fok TF, Wong W, Chan DC 1997 The pituitary-adrenal responses to exogenous human corticotrophin releasing hormone in preterm, very low birth weight infants. J Clin Endocrinol Metab 82: 797–799
Karlsson R, Kallio J, Irjala K, Ekblad S, Toppari J, Kero P 2000 Adrenocorticotropin and releasing-releasing hormone tests in preterm infants. J Clin Endocrinol Metab 85: 4592–4595
The Committee for the Classification of Retinopathy of Prematurity 1984 An international classification of retinopathy of prematurity. Arch Ophthalmol 102: 1130–1134
Ng PC, Lee CH, Lam CWK, Ma KC, Chan IHS, Wong E, Fok TF 2004 Early pituitary-adrenal response and respiratory outcomes in preterm infants. Arch Dis Child ( in press)
Ng PC, Lam CWK, Lee CH, Ma KC, Fok TF, Chan IHS, Wong E 2002 Reference ranges and factors affecting the human corticotropin releasing hormone test in preterm, very low birth weight infants. J Clin Endocrinol Metab 87: 4621–4628
Brieman I, Friedman JH, Olshen RA, Stone CJ 1993 Classification and regression trees. Chapman and Hall, New York, pp 18–55.
Fok TF, Lam K, Dolovich M, Ng PC, Wong W, Cheung KL, So KW 1999 Randomised controlled study of early use of inhaled corticosteroid in preterm infants with respiratory distress syndrome. Arch Dis Child 80: F203–F208
Charles JB, Ganthier R, Appiah AP 1991 Incidence and characteristics of retinopathy of prematurity in a low-income inner-city population. Ophthalmology 98: 14–17
Ng PC, Wong GWK, Lam CWK, Lee CH, Wong MY, Fok TF, Wong W, Chan DC 1997 Pituitary-adrenal response in preterm very low birth weight infants after treatment with antenatal corticosteroids. J Clin Endocrinol Metab 82: 3548–3552
Smith LEH 2002 Pathogenesis of retinopathy of prematurity. Acta Paediatr 437( Suppl): 26–28
Giudice LC, de Zegher F, Gargosky SE, Dsupin BA, de las Fuentes L, Crystal RA, Hintz RL, Rosenfeld RG 1995 Insulin-like growth factors and their binding proteins in the term and preterm human fetus and neonate with normal and extremes of intrauterine growth. J Clin Endocrinol Metab 80: 1548–1555
Hellstrom A, Perruzzi C, Ju M, Engström E, Hard AL, Liu JL, Albertsson-Wikland K, Carlsson B, Niklasson A, Sjodell L, LeRoith D, Senger DR, Smith LEH 2001 Low IGF-1 suppresses VEGF-survival signaling in retinal endothelial cells: direct correlation with clinical retinopathy of prematurity. Proc Natl Acad Sci USA 98: 5804–5808
Rotschild T, Nandgaonkar BN, Yu K, Higgins RD 1999 Dexamethasone reduces oxygen induced retinopathy in a mouse model. Pediatr Res 46: 94–100
Haroon Parupia MF, Dhanireddy R 2001 Association of postnatal dexamethasone use and fungal sepsis in the development of severe retinopathy of prematurity and progression to laser therapy in extremely low-birth-weight infants. J Perinatol 21: 242–247
Ramanathan R, Siassi B, deLemos RA 1995 Severe retinopathy of prematurity in extremely low birth weight infants after short-term dexamethasone therapy. J Perinatol 15: 178–182
Termote J, Schali-Delfos NE, Donders AR, Cats BP 2000 Do postnatal glucocorticoids and retinopathy of prematurity relate?. Am J Perinatol 17: 291–298
Batton DG, Roberts C, Trese M, Maisels MJ 1992 Severe retinopathy of prematurity and steroid exposure. Pediatrics 90: 534–536
Cuculich PS, DeLozier KA, Mellen BG, Shenai JP 2001 Postnatal dexamethasone treatment and retinopathy of prematurity in very-low-birth-weight neonates. Biol Neonate 79: 9–14
Jacobs MA, Blanco CE 1998 The incidence of retinopathy of prematurity and steroid therapy for broncho-pulmonary dysplasia. J Perinat Med 26: 13–16
Wright K, Wright SP 1994 Lack of association of glucocorticoid therapy and retinopathy of prematurity. Arch Pediatr Adolesc Med 148: 848–852
Halliday HL, Ehrenkranz RA, Doyle LW 2003 Moderately early (7–14 days) postnatal corticosteroids for preventing chronic lung disease in preterm infants (Cochrane Review). In: The Cochrane Library, Issue 1. Update Software, Oxford, UK
Halliday HL, Ehrenkranz RA, Doyle LW 2003 Delayed (> 3 weeks) postnatal corticosteroids for chronic lung disease in preterm infants (Cochrane Review). In: The Cochrane Library, Issue 1. Update Software, Oxford, UK
Vincer MJ, Allen AC 1998 Double blind randomized controlled trial of 6-day pulse of dexamethasone for very low birth weight infants (VLBW < 1500 grams) who are ventilator dependent at 4 weeks of age. Pediatr Res 43: 201A( abstr)
Suske G, Oestreich K, Varnholt V, Lasch P, Kachel W 1996 Influence of early postnatal dexamethasone therapy on ventilator dependency in surfactant-substituted preterm infants. Acta Paediatr 85: 713–718
Brozanski BS, Jones JG, Gilmore CH, Balsan MJ, Vazquez RL, Israel BA, Newman B, Mimouni FB, Guthrie RD 1995 Effect of pulse dexamethasone therapy on the incidence and severity of chronic lung disease in the very low birthweight infant. J Pediatr 126: 769–776
Durand M, Sardesai S, McEvoy C 1995 Effect of early dexamethasone therapy on pulmonary mechanics and chronic lung disease in very low birth weight infants: a randomised controlled trial. Pediatrics 95: 584–590
Kothadia JM, O'Shea TM, Roberts D, Auringer ST, Weaver RG, Dillard RG 1999 Randomized placebo-controlled trial of a 42-day tapering course of dexamethasone to reduce the duration of ventilator dependency in very low birthweight infants. Pediatrics 104: 22–27
Watterberg KL, Gerdes JS, Gifford KL, Lin HM 1999 Prophylaxis against early adrenal insufficiency to prevent chronic lung disease in premature infants. Pediatrics 104: 1258–1263
Author information
Authors and Affiliations
Additional information
Funded by the Department of Pediatrics, The Chinese University of Hong Kong.
Rights and permissions
About this article
Cite this article
Ng, P., Kwok, A., Lee, C. et al. Early Pituitary-Adrenal Responses and Retinopathy of Prematurity in Very Low Birth Weight Infants. Pediatr Res 55, 114–119 (2004). https://doi.org/10.1203/01.PDR.0000100464.09953.C9
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1203/01.PDR.0000100464.09953.C9
This article is cited by
-
Medical morbidities and DNA methylation of NR3C1 in preterm infants
Pediatric Research (2017)
