
Abstract
In infants with congenital diaphragmatic hernia (CDH), a posterolateral diaphragmatic defect results in herniation of abdominal contents into the chest and compression of the intrathoracic structures. In the most severe cases, hypoplasia of the ipsilateral and contralateral lungs, severe pulmonary hypertension (PH) and left ventricular (LV) hypoplasia/dysfunction all contribute to increased mortality. The management of PH in CDH is complicated by structural and functional changes in the heart, pulmonary vasculature, airways and lung parenchyma; consequently, determining optimal management strategies is challenging. Treatment of PH in patients with CDH changes as the underlying pathophysiology evolves in the days and weeks after birth. During the early transition, the use of pulmonary vasodilators is limited by LV structural and functional abnormalities, and pulmonary vasodilators such as inhaled nitric oxide (iNO) may have a limited role (for example, stabilization for extracorporeal membrane oxygenation (ECMO), treatment of marked preductal desaturation and treatment of PH as LV performance improves). In contrast, subacute treatment of PH in CDH with iNO has an important role in recurrent or persistent PH and potentially improves survival. Chronic PH and vascular abnormalities may persist into childhood in patients with CDH, contributing to late mortality. It is unclear how pulmonary vasodilator therapies, such as iNO, sildenafil and bosentan, will modulate late outcomes in CDH with late/chronic PH.
Similar content being viewed by others

Introduction
Congenital diaphragmatic hernia (CDH) is a severe birth defect characterized by herniation of abdominal contents into the thorax caused by a defect in the diaphragm.1 Recent insight into pathophysiologic processes responsible for CDH suggests an early role for environmental and/or genetic factors before the development of the diaphragm, leading to arrested development of both lungs. In addition, incomplete closure of the diaphragm results in a diaphragm defect, herniation of the abdominal contents into the chest and compression of the intrathoracic structures. Solid organ herniation exacerbates the degree of lung hypoplasia and the most severe cases are associated with hypoplasia of the ipsilateral and contralateral lung (low lung-to-head ratio, LHR).2 Along with degree of lung hypoplasia, the severity of pulmonary hypertension (PH) and the presence of left ventricular (LV) hypoplasia all contribute to the severity of the defect and adverse outcomes.3, 4 Overall survival of infants with CDH has improved in experienced centers, but mortality and morbidity remain high.
Several individual prenatal prognostic factors have been identified in CDH that can predict the clinical course after birth as well as long-term outcomes. These include liver position, severity of lung hypoplasia (as assessed by fetal lung volume on magnetic resonance imaging: percent predicted lung volume and total lung volume; LHR and observed to expected LHR by ultrasound), LV hypoplasia (right ventricle (RV): left ventricle disproportion on fetal echocardiogram (ECHO)) and development and reactivity of the pulmonary vasculature (for example, McGoon index, in utero hyperoxia test). In addition, the presence of congenital heart disease or a genetic syndrome5 markedly impact outcomes. The reliability of each individual parameter to predict survival and long-term outcome is low, and combining multiple parameters improves reliability. The CDH congenital prognostic index (CDH-CPI) is a useful tool that amalgamates 10 prenatal parameters representing genetic, cardiac, hernia and lung factors to comprehensively capture the range of severity and associated anomalies influencing prognosis.5 The CDH-CPI score is correlated with survival and extracorporeal membrane oxygenation (ECMO) support, with significantly lower survival at scores below 8.5
PH in CDH
The classical histological findings of CDH show pulmonary vascular remodeling superimposed on hypoplasia or pruning of the pulmonary vascular bed.1 These changes in the pulmonary vasculature are responsible for increased vascular tone and altered vasoreactivity after birth.1 Management of PH in the newborn with CDH is complicated by the structural and functional changes in the heart, pulmonary circulation, airways and lung parenchyma. Moreover, the role and selection of pulmonary vasodilator therapies for treatment of PH changes as the underlying pathophysiology evolves in the days and weeks after birth. In response, management strategies need to adjust as pulmonary vascular abnormalities progress from the acute to subacute (late) and finally chronic stages.
Acute PH in CDH
After birth, infants with CDH typically present with severe hypoxemic respiratory failure and shock. The etiology of hypoxemia is multifactorial and occurs secondary to intrapulmonary shunt as well as extrapulmonary right-to-left shunting across fetal conduits (ductus arteriosus (DA) and foramen ovale). Newborns with severe CDH often present with left-to-right shunting at the atrial septum and right-to-left shunting at the DA.6 Differential shunting across these fetal conduits is responsible for postductal desaturation and differences in pre- and postductal arterial blood gas parameters.6 The direction of atrial level shunt is determined by the relative right and left ventricular end diastolic pressures. Left-to-right shunting at the atrial septum occurs when LV end diastolic pressure exceeds right ventricular end diastolic pressures with impaired LV filling and elevated left atrial pressure.
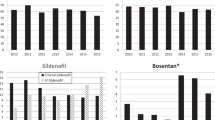
Structural and functional LV abnormalities are responsible for impaired LV filling and contribute to the development of pulmonary venous hypertension. Baumgart et al.7 showed that ECMO-treated CDH infants (survivors) had significantly smaller LV mass (P<0.002) than infants requiring ECMO for other diagnoses and healthy term infants. Moreover, ECMO-treated CDH neonates who died had significantly smaller LV size than other groups (P<0.0005) including ECMO-treated CDH survivors (in addition to CDH and non-CDH ECMO-treated infants and well infants).7 Byrne et al.8 reported that fetuses with severe left CDH were more likely to have smaller mitral valve (P<0.001) and aortic valve sizes (P<0.001), and LV end diastolic volume (P=0.006) Z-scores than those with mild left CDH (Figure 1). In addition to the structural changes in the LV, their percentage LV output was also lower. Those with severe left CDH trended toward higher risk of neonatal death compared with those with mild left CDH. Although mitral and aortic valve dimensions in fetuses with right CDH were larger than in left CDH, LV outputs were similarly diminished.

Left heart hypoplasia stratified by congenital diaphragmatic hernia (CDH) side and severity at fetal assessment. Left CDH: mild (n=42), liver down; moderate (n=41), lung-to-head ratio (LHR) 1 to 1.4; severe (n=88), LHR ⩽1; Right CDH: mild (n=2), LHR >1; severe (n=15), LHR ⩽1. For left heart measurements (mitral and aortic values, left ventricular volume) severity of hypoplasia increased with increasing severity of hernia, while the effect in the fetus with right CDH was less pronounced. Adapted with permission from Byrne et al.8 L, left; R, right.
The etiology of LV hypoplasia in CDH is almost certainly multifactorial reflecting mechanical compression by intra-abdominal contents as well as alteration in LV filling hemodynamics during fetal development due to changes in orientation of the inferior vena cava and venous return from the placenta. Left heart underfilling and subsequent underdevelopment may result from abnormal hemodynamics due to leftward distortion of the ductus venosus or reduced pulmonary blood flow return to the left heart.8 In addition, after birth, compression of the LV by the RV in the presence of elevated RV pressure also impairs LV filling. The common pathway for these mechanisms is decreased filling of the left ventricle. Altered hemodynamics and compression of the heart by herniated abdominal viscera together can create strikingly abnormal LV structure and function with anomalous relaxation and small chamber size, even with normal or near-normal systolic performance. Overall, altered fetal hemodynamics leading to decreased LV output can occur in both right and left CDH, but an additional compressive effect on the left heart is seen in left-sided CDH.8
Echocardiographic findings may be valuable in guiding the selective use of pulmonary vasodilators in management of early PH with CDH. For example, ECHO findings in the presence of severe PH may show right-to-left shunting (caused by suprasystemic pulmonary vascular resistance) at the atrial level and DA. This constellation of echocardiographic findings suggests a favorable response to pulmonary vasodilation. However, in the presence of LV dysfunction, right-to-left DA shunting is seen along with mitral insufficiency with left-to-right atrial shunting at the foramen ovale.9 This constellation of findings is again consistent with suprasystemic right ventricular systolic pressure (RVSP), but left-to-right atrial shunting suggests the presence of pulmonary venous hypertension and a poor response to pulmonary vasodilator therapy. Diastolic dysfunction is difficult to assess, but can be interpreted from a high LV end diastolic pressure and manifests as left-to-right shunt at the atrial level. Pulmonary vasodilator therapy in the setting of left-to-right shunting at the atrial septum has the potential to exacerbate left arterial and pulmonary venous hypertension and contribute to pulmonary hemorrhage. In addition, as preductal saturations are maintained in this setting, pulmonary vasodilator therapy is unlikely to improve preductal saturations and may result in only a modest increase in postductal saturations. Reserving inhaled nitric oxide (iNO) therapy for infants with right-to-left atrial shunting and preductal desaturation is recommended early in the clinical course and has the potential to prevent pulmonary hemorrhage in CDH. In addition, as right-to-left shunting across the DA causes veno-arterial admixture, it is common to see significant differences in pre- and postductal arterial blood gas measurements.6 Determining the need for ECMO, degree of respiratory support and fraction of inspired oxygen (FiO2) should be based on measurement of preductal arterial gases in these infants.6
Overall, acute treatment of PH in CDH with pulmonary vasodilators is limited by the severity of LV hypoplasia, degree of impairment of LV filling and LV systolic dysfunction. Because infants with severe CDH and acute PH are poor responders, iNO should not be routinely administered in this setting. However, careful ECHO assessment can help identify limited clinical situations that may benefit from PH therapies, including iNO, and guide the course of treatment.9, 10 In the acute management of CDH, iNO may have a selective role in stabilization for ECMO and treatment of marked preductal desaturation secondary to right-to-left atrial level shunt. Furthermore, the use of iNO for treatment of PH may be considered as LV performance improves. LV hypoplasia, and related LV output, also have a role in the poor response to pulmonary vasodilators as diminished LV performance results in RV-dependent systemic circulation.10 Initiating pulmonary vasodilator therapy in the presence of an RV-dependent systemic circulation may adversely affect systemic hemodynamics.
The Neonatal Inhaled Nitric Oxide Study (NINOS) Group conducted the largest trial of iNO in infants with CDH (N=53) who were randomized to 20 p.p.m. iNO or 100% oxygen (control).11 The oxygenation index was approximately 45 in both groups, indicating more severe disease. NINOS showed no difference in the combined endpoint ‘death/ECMO utilization’ between iNO-treated patients and controls. However, ECMO utilization was higher in the iNO-treated group (80% vs 54% control, P=0.043), pointing to an adverse effect of iNO early in the course of CDH. These results lend support to the hypothesis that LV systolic and diastolic dysfunction contribute to morbidity in severe CDH and limit the efficacy of aggressive pharmacologic pulmonary vasodilator therapy early in the course of CDH and severe PH.
Indeed, a poor response to pulmonary vasodilation is not unexpected given the structural and functional abnormalities that characterize acute CDH. Although speculative, the lack of response to pulmonary vasodilators is more likely due to left atrial/pulmonary vein hypertension than functional changes in the pulmonary arterial vasculature.
Subacute (Late) PH in CDH
In addition to complicating the early course of neonates with CDH, severe PH can be protracted—persisting weeks to months after improvement in respiratory failure and cardiac performance—leading to prolonged mechanical ventilation.10 In a multicenter prospective ECHO study of neonates with CDH (N=220), mortality at discharge in newborns with severe PH (RVSP/systolic blood pressure (SBP) >2/3) was 56.1% compared with 1.4% in infants with mild PH (RVSP/SBP <1/2) and 7.4% in those with moderate PH (RVSP/SBP 1/2 to 2/3).4 Recently, Lusk et al.12 reviewed ECHO results for 140 newborns with CDH and found that although the majority of infants had resolution of PH between 1 and 3 weeks of age, at 2 weeks the severity of PH by echocardiogram predicted mortality and need for prolonged ventilation.12
Treatment strategies for infants with late PH have not been carefully studied. iNO is usually the first-line therapy for treatment of PH in CDH. In a subset of newborns with CDH, improvement in parenchymal lung disease may allow for the use of non-invasive iNO by continuous positive airway pressure or nasal cannula.13 There is limited experience with other pharmacologic pulmonary vasodilators (for example, prostacyclin, endothelin antagonists and phosphodiesterase inhibitors) in infants with CDH and late PH. Olson et al.14 recently described two infants with CDH and severe PH at 6 weeks of age who responded favorably to treatment with trepostinil. Clearly, further investigation is needed to define an approach to the management of late PH in this population.
Chronic PH in CDH
Chronic PH may persist in CDH over months and years, and enduring structural and functional abnormalities of pulmonary circulation in the ipsilateral and contralateral lung can complicate the course of the disease. Cardiac catheterization of seven patients with CDH who survived the neonatal period with protracted or recurrent PH revealed a range of pulmonary vascular abnormalities.10 These patients (age range, 3 months to 12 years) had a history of severe hypoxemic respiratory failure and PH as newborns. At catheterization, therapies included supplemental oxygen (n=7), iNO (n=2), prostacyclin (n=2) and bosentan (n=1). Three of the seven patients had significant pulmonary vascular abnormalities in the lung contralateral to the initial diaphragmatic defect. Major findings at cardiac catheterization included left pulmonary artery hypoplasia or stenosis in three patients and pulmonary vein stenosis or delayed venous return in six patients. Two patients with right-sided diaphragmatic defect had striking left-sided pulmonary venous abnormalities. One patient with right-sided CDH was discharged home, but died at age 5 months with marked pulmonary vascular changes on autopsy consistent with severe PH. After a median follow-up of 12 months from catheterization, five patients were alive and discharged from hospital. The two patients with the most severe PH died from related complications at ages 8 and 19 months.
In some patients with CDH, significant PH, which may be subclinical, clearly continues beyond the neonatal period, contributing to morbidity and mortality. Understanding the pathophysiology underlying these long-term effects will require a more sophisticated view of CDH than that originating solely from in utero cardiopulmonary compression. It is possible that the injury associated with management of hypoxemic respiratory failure in newborns with CDH may cause previously unrecognized long-term effects in susceptible individuals, and/or the pulmonary circulation in patients with severe CDH may be fundamentally altered in utero, leading to abnormal responses to injury that last far beyond the newborn period.10
Improving outcomes in CDH
Treatment strategies for CDH continue to evolve with increasing clinical experience and greater insight into the underlying nature of the condition. These strategies include simultaneous postductal and preductal samples to measure blood gases (adjusting ventilator support accordingly) (Appendix A). Early ECHO is essential to define pulmonary artery pressure and assess LV size and function. It is reasonable to delay the use of pulmonary vasodilator therapy until there is ECHO evidence of adequate LV performance. Reducing LV afterload pharmacologically may have an important role (for example, milrinone), as well as maintaining ductal patency with prostaglandin E1 if RV-dependent systemic circulation is demonstrated by ECHO. Adrenal insufficiency also complicates the course of newborns with severe CDH and decreases catecholamine drug responsiveness.15
Despite refinement of postnatal interventions, limitations persist and treatment of CDH and PH remains suboptimal. Consequently, new therapeutic options such as prenatal intervention or cell-based therapy are the subject of current investigation. The effects of LV dysfunction/hypoplasia on the neonatal course in severe CDH provide a compelling reason to study fetal intervention. The efficacy of prenatal intervention with percutaneous fetoscopic endoluminal tracheal occlusion therapy in CDH has been described in case series and controlled studies.16, 17 The potential role of fetoscopic endoluminal tracheal occlusion is being investigated in CDH in an European and North American collaboration called the TOTAL (Tracheal Occlusion To Accelerate Lung Growth) Trial.18
Mesenchymal stem cells also represent an emerging therapeutic approach in CDH. Several experimental studies in animal models have shown that treatment with mesenchymal stem cells can reduce pulmonary injury and PH.19, 20 A recent study in a rat model of experimental CDH found that mesenchymal stem cell transplantation promotes alveolar and pulmonary artery development, reducing the severity of pulmonary hypoplasia.21
Conclusion
In summary, the early course of CDH is characterized by severe PH, and cardiac, lung parenchymal and airway abnormalities. Acute treatment of PH in CDH with pulmonary vasodilator therapy is limited by structural and functional changes of the left ventricle. In a significant subset of newborns with severe CDH, late or protracted PH occurs and may persist weeks to months following improvement in respiratory failure and cardiac performance. In contrast to early CDH, pulmonary vasodilator therapy has a critical role in management of late PH in CDH, and potentially improves survival.
Despite progress in CDH management, advances have been limited by the lack of randomized controlled trials to properly test new treatments. Major differences in clinical practice regarding the ascertainment and treatment of PH make it difficult to determine the most effective strategies to manage late PH in CDH infants. Moreover, institutional practices that lead to ‘improved’ outcomes are slowly adopted and local changes are often guided only by experience and conviction. To overcome these barriers, centers with the best outcomes for isolated CDH should be identified from current databases and their practices disseminated to the wider community. Improving outcomes in patients with CDH will require continued vigilance, multidisciplinary collaboration and widespread adoption of best practices.
References
Pierro M, Thebaud B . Understanding and treating pulmonary hypertension in congenital diaphragmatic hernia. Semin Fetal Neonatal Med 2014; 19: 357–363.
Lipshutz GS, Albanese CT, Feldstein VA, Jennings RW, Housley HT, Beech R et al. Prospective analysis of lung-to-head ratio predicts survival for patients with prenatally diagnosed congenital diaphragmatic hernia. J Pediatr Surg 1997; 32: 1634–1636.
Taira Y, Yamataka T, Miyazaki E, Puri P . Comparison of the pulmonary vasculature in newborns and stillborns with congenital diaphragmatic hernia. Pediatr Surg Int 1998; 14: 30–35.
Wynn J, Krishnan U, Aspelund G, Zhang Y, Duong J, Stolar CJ et al. Outcomes of congenital diaphragmatic hernia in the modern era of management. J Pediatr 2013; 163: 114–119.
Le LD, Keswani SG, Biesiada J, Lim FY, Kingma PS, Haberman BE et al. The congenital diaphragmatic hernia composite prognostic index correlates with survival in left-sided congenital diaphragmatic hernia. J Pediatr Surg 2012; 47: 57–62.
Gien J, Kinsella JP . Differences in preductal and postductal arterial blood gas measurements in infants with severe congenital diaphragmatic hernia. Arch Dis Child Fetal Neonatal Ed 2015 (epub ahead of print).
Baumgart S, Paul JJ, Huhta JC, Katz AL, Paul KE, Spettell C et al. Cardiac malposition, redistribution of fetal cardiac output, and left heart hypoplasia reduce survival in neonates with congenital diaphragmatic hernia requiring extracorporeal membrane oxygenation. J Pediatr 1998; 133: 5762.
Byrne FA, Keller RL, Meadows J, Miniati D, Brook MM, Silverman NH et al. Severe left diaphragmatic hernia limits size of fetal left heart more than right diaphragmatic hernia. ltrasound Obstet Gynecol 2015; 46: 688–694.
Kinsella JP, Abman SH . Clinical approach to inhaled nitric oxide therapy in the newborn with hypoxemia. J Pediatr 2000; 136: 717–726.
Kinsella JP, Ivy DD, Abman SH . Pulmonary vasodilator therapy in congenital diaphragmatic hernia: acute, late, and chronic pulmonary hypertension. Semin Perinatol 2005; 29: 123–128.
Inhaled nitric oxide and hypoxic respiratory failure in infants with congenital diaphragmatic hernia. The Neonatal Inhaled Nitric Oxide Study Group (NINOS). Pediatrics 1997; 99: 838–845.
Lusk LA, Wai KC, Moon-Grady AJ, Steurer MA, Keller RL . Persistence of pulmonary hypertension by echocardiography predicts short-term outcomes in congenital diaphragmatic hernia. J Pediatr 2015; 166: 251–256.
Kinsella JP, Parker TA, Ivy DD, Abman SH . Noninvasive delivery of inhaled nitric oxide therapy for late pulmonary hypertension in newborn infants with congenital diaphragmatic hernia. J Pediatr 2003; 142: 397–401.
Olson E, Lusk LA, Fineman JR, Robertson L, Keller RL . Short-term treprostinil use in infants with congenital diaphragmatic hernia following repair. J Pediatr 2015; 167: 762–764.
Kamath BD, Fashaw L, Kinsella JP . Adrenal insufficiency in newborns with congenital diaphragmatic hernia. J Pediatr 2010; 156: 495–497.
Jani J, Valencia C, Cannie M, Vuckovic A, Sellars M, Nicolaides KH . Tracheal diameter at birth in severe congenital diaphragmatic hernia treated by fetal endoscopic tracheal occlusion. Prenat Diagn 2011; 31: 699–704.
Ruano R, Yoshisaki CT, da Silva MM, Ceccon ME, Grasi MS, Tannuri U et al. A randomized controlled trial of fetal endoscopic tracheal occlusion versus postnatal management of severe isolated congenital diaphragmatic hernia. Ultrasound Obstet Gynecol 2012; 39: 20–27.
Deprest J, De CP . Antenatal management of isolated congenital diaphragmatic hernia today and tomorrow: ongoing collaborative research and development. Journal of Pediatric Surgery Lecture. J Pediatr Surg 2012; 47: 282–290.
Hoffman AM, Paxson JA, Mazan MR, Davis AM, Tyagi S, Murthy S et al. Lung-derived mesenchymal stromal cell post-transplantation survival, persistence, paracrine expression, and repair of elastase-injured lung. Stem Cells Dev 2011; 20: 1779–1792.
Aslam M, Baveja R, Liang OD, Fernandez-Gonzalez A, Lee C, Mitsialis SA et al. Bone marrow stromal cells attenuate lung injury in a murine model of neonatal chronic lung disease. Am J Respir Crit Care Med 2009; 180: 1122–1130.
Yuniartha R, Alatas FS, Nagata K, Kuda M, Yanagi Y, Esumi G et al. Therapeutic potential of mesenchymal stem cell transplantation in a nitrofen-induced congenital diaphragmatic hernia rat model. Pediatr Surg Int 2014; 30: 907–914.
Acknowledgements
This article is based on discussions at a roundtable meeting supported by a grant from Mallinckrodt Pharmaceuticals, formerly Ikaria. Presentations and discussions were developed solely by the participants, without grantor input. The meeting chair Robin Steinhorn, MD, determined the agenda and attendees. JG and JPK developed the presentations and led the discussions upon which this article is based, provided critical review and revisions to the outline and manuscript drafts, provided final approval of the version to be published, and are accountable for the integrity of the content and for addressing questions. We gratefully acknowledge the contributions of the following individuals who participated in discussion that shaped the content of this article: Namasivayam Ambalavanan, MD; Judy L Aschner, MD; Ganesh Konduri, MD; Satyan Lakshminrusimha, MD; Ola Didrik Saugstad, MD, PhD, FRCPE; and Robin Steinhorn, MD. Writing and editorial assistance was provided by John Kross, and Sharon Suntag and Julie Gerke of Quintiles.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
JG and JPK received honoraria for their participation in a roundtable meeting supported by a grant from Mallinckrodt Pharmaceuticals, formerly Ikaria.
Appendix
Appendix
Current approach to optimize management of CDH and related PH at Children’s Hospital Colorado
Rights and permissions
About this article

Cite this article
Gien, J., Kinsella, J. Management of pulmonary hypertension in infants with congenital diaphragmatic hernia. J Perinatol 36 (Suppl 2), S28–S31 (2016). https://doi.org/10.1038/jp.2016.46
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/jp.2016.46
This article is cited by
-
Pulmonary hypertension
Nature Reviews Disease Primers (2024)
-
Early nitric oxide is not associated with improved outcomes in congenital diaphragmatic hernia
Pediatric Research (2023)
-
The Utility of Serial Echocardiography Parameters in Management of Newborns with Congenital Diaphragmatic Hernia (CDH) and Predictors of Mortality
Pediatric Cardiology (2023)
-
Congenital diaphragmatic hernia: phosphodiesterase-5 and Arginase inhibitors prevent pulmonary vascular hypoplasia in rat lungs
Pediatric Research (2022)
-
Treatment of pulmonary hypertension during initial hospitalization in a multicenter cohort of infants with congenital diaphragmatic hernia (CDH)
Journal of Perinatology (2021)
