
Abstract
The prevalence of fluoroquinolone-resistant Streptococcus pneumoniae is increasing worldwide. In the present study, a comparison of drug sensitivity and genotypes of clinically isolated strains of levofloxacin (LVFX)-resistant S. pneumoniae obtained from Hong Kong, Okinawa Island and the Japanese main island (Honshu) was performed. MICs of quinolones (LVFX, tosufloxacin, ciprofloxacin, gatifloxacin and sitafloxacin (STFX)) and other antibiotics (penicillin G, cefcapene, cefditoren, clarithromycin and azithromycin) were determined by a microdilution broth method according to the Clinical and Laboratory Standards Institute Standards. The quinolone-resistance determining regions (QRDRs) of gyrA, gyrB, parC and parE of these strains were analyzed by PCR-based sequencing. All 40 strains tested had more than one amino-acid substitution in the QRDRs of gyrA, gyrB, parC or parE. Although there seemed to be some clonality in strains obtained from Hong Kong, there was no clonality in strains obtained from Okinawa and Japan. Strains obtained from Hong Kong, Okinawa Island and the Japanese main island were genetically different by pulsed-field gel electrophoresis analysis. The range of MIC values of STFX against isolates resistant to LVFX (MIC 4–32 mg l−1) was 0.12–0.5 mg l−1, and MIC80 values of STFX against LVFX-resistant isolates were 0.25 mg l−1. This study suggests that LVFX-resistant S. pneumoniae is similar in all three locations and STFX is potent against LVFX-resistant S. pneumoniae with multiple mutations in QRDRs of gyrase A and topoisomerase IV.
Similar content being viewed by others

Introduction
Streptococcus pneumoniae is a major cause of respiratory tract infections, bacteremia and bacterial meningitis. Although penicillin has been the most effective drug for the treatment of infections caused by S. pneumoniae, the incidence of multiple drug-resistant S. pneumoniae is currently increasing throughout the world.1 In particular, the rapid spread of pneumococcal clones resistant to β-lactams and macrolides has promoted the use of selected fluoroquinolones for the treatment of pneumococcal infections. Therefore, fluoroquinolones with anti-pneumococcal activity, such as levofloxacin (LVFX), tosufloxacin (TSFX), ciprofloxacin (CPFX), sparfloxacin (SPFX), gatifloxacin (GTFX) and sitafloxacin (STFX), may have an important role in the management of pneumococcal disease.2
The reported increase in S. pneumoniae resistance to fluoroquinolones is of great concern. So far, two mechanisms responsible for the reduced susceptibility to fluoroquinolones have been identified in clinical isolates: target alteration and/or reduced drug accumulation due to drug efflux.3 The targets of fluoroquinolones are DNA gyrase and topoisomerase IV, which are encoded by gyrA, gyrB, parC and parE, and fluoroquinolone-resistant strains show amino-acid substitutions in the quinolone-resistance determinant regions (QRDRs) of DNA gyrase and topoisomerase IV. Multiple mutations within the QRDRs of both gyrA and parC result in high-level resistance against LVFX.4 We hypothesized that the increase of fluoroquinolone-resistant S. pneumoniae strains might be related to the selection of resistant clones in restricted areas. Therefore, in the present study, a comparison of the drug sensitivities and genotypes of clinically isolated strains of LVFX-resistant S. pneumoniae obtained from Hong Kong, Okinawa Island and the Japanese main island (Honshu) was performed.
Materials and methods
Bacterial strains
Forty clinical isolates of S. pneumoniae with resistance to LVFX (MIC ⩾4 mg l−1) were used in this study, including 19 from Hong Kong, 9 from Okinawa Island and 12 from the Japanese main island (Honshu). Strains were collected from various specimens submitted to the clinical laboratory. Only one isolate per patient was considered. The isolates were confirmed to be S. pneumoniae by colony morphology, optochin susceptibility and bile solubility, and the presence of the autolysin gene lytA was confirmed by PCR (Wakunaga Pharmaceuticals, Hiroshima, Japan). Bacteria were grown on 5% sheep blood agar (Kyokuto, Tokyo, Japan) at 37 °C in an atmosphere of 5% CO2. LVFX-susceptible clinical strains, S. pneumoniae ATCC 700669 and ATCC 700671, were used as quality control strains for sequence analysis and MIC determination.
Antimicrobial susceptibility testing
The MICs of quinolones (LVFX, TSFX, CPFX, SPFX, GTFX and STFX) and other antibiotics (penicillin G (PCG), cefcapene (CFPN), cefditoren (CDTR), clarithromycin (CAM) and azithromycin (AZM)) were determined by the twofold broth microdilution method according to the guidelines of the Clinical and Laboratory Standards Institute (formerly National Committee for Clinical Laboratory Standards).5 Cation-adjusted Mueller–Hinton broth (Difco Laboratories, Detroit, MI, USA) was supplemented with 3% lysed horse blood. Microdilution trays (final volume, 100 μl per well) were inoculated using an automatic MIC-2000 inoculator (Dynatech Laboratories, Alexandria, VA, USA). Final inocula contained ∼5 × 104 CFU per well. The MIC of each drug was defined as the lowest concentration resulting in the complete inhibition of visible growth after 18 h incubation.
Sequencing and analysis of DNA-related drug sensitivity
Quinolone-resistance gene
Mutations in the QRDRs of the gyrA, gyrB, parC and parE genes of LVFX-resistant strains were investigated by a method involving PCR. The primer sequences used in this study have been previously described.6 Bacterial genomic DNA was prepared from several colonies of S. pneumoniae grown on a blood agar plate by boiling with Chelex-100 (Bio-Rad, Hercules, CA, USA). Subsequently, 5 μl of the extract was added to 50 μl of a PCR solution (1 × PCR buffer, 200 μM of each dNTP, 2.5 U of Taq polymerase (Takara Biomedical, Kyoto, Japan) and 0.5 μM of sense and reverse primers). PCR conditions were as follows: 35 cycles at 94 °C for 30 s, 55 °C for 30 s and 72 °C for 1 min. The PCR products were electrophoresed on an agarose gel to confirm the presence of the product, and were then purified with a PCR purification kit (Qiagen Sciences, Germantown, MD, USA) to prepare the sequencing template. The sequencing reaction was conducted with a Rhodamine Terminator Cycle Sequencing FS Ready Reaction kit (Perkin-Elmer Biosystems, Foster city, CA, USA). The reaction mixtures were placed in a thermal cycler and denatured at 94 °C for 2 min. Reactions were then subjected to 25 cycles (94 °C for 10 s, 50 °C for 5 s and 60 °C for 4 min). The nucleotide sequences were determined using an ABI PRISM3100 DNA sequencer (Applied Biosystems, Carlsbad, CA, USA).
Penicillin-binding protein gene alterations
We evaluated alterations in penicillin-binding protein (PBP) genes of S. pneumoniae by PCR, according to Ubukata et al.,7 with some modifications described by Harimaya et al.8 The system contains primer sets for unaltered PBP genes (pbp1a, pbp2x and pbp2b). Extraction of DNA from a colony on a blood agar plate and PCR was performed according to Ubukata et al.9 The reaction profile used was 30 cycles of 94 °C for 30 s, 53 °C for 30 s and 72 °C for 1 min. PCR products were separated in 3% NuSieve 3:1 agarose (Cambrex, East Rutherford, NJ, USA) and visualized by UV light illumination. The bands of PBP genes were detected on the agarose gel when the PBP genes were not altered, and the bands were not detected when the genes were altered.
Macrolide-resistance gene
Two sets of oligonucleotide primers designed on the basis of our sequence results were as follows: ermB1, 5′-721CGTACCTTGGATATTCACCG740-3′ and ermB2, 5′-944GTAAACAGTTGACGATATTCTCG922-3′ for the ermB gene; and mefA1, 5′-288CTGTATGGAGCTACCTGTCTGG309-3′ and mefA2, 5′-581CCCAGCTTAGGTATACGTAC562-3′ for the mefA gene. The DNA fragments amplified by these primers were 224 bp for the ermB and 294 bp for the mefA gene. A single colony on the blood agar medium was suspended in a microtube containing 30 μl lysis solution.7 The tube was set in a thermal cycler (Gene Amp PCR System 9600-R; Perkin-Elmer, Norwalk, CT, USA), and bacterial cells were lysed by incubation at 60 °C for 10 min followed by 94 °C for 5 min. Next, 2 μl of the lysed bacterial solution was placed in a PCR tube containing 25 μl of a reaction mixture. One milliliter of the reaction mixture consisted of 60 ng of a primer for each of ermB and mefA, 80 μl 25 mM dNTP mixture, 25 U Taq DNA polymerase and 100 μl of 10 × PCR buffer. The PCR conditions were 94 °C for 20 s, 52 °C for 20 s and 72 °C for 15 s, with 30 cycles in total.
Molecular typing
Isolates were characterized by pulsed-field gel electrophoresis (PFGE) by previously described methods.10, 11 Fragments were separated by PFGE in a CHEF-DRIII apparatus (Bio-Rad) as previously described, and were compared using the Fingerprinting software (Bio-Rad). The PFGE profiles were visually examined, and clusters were assigned on the basis of three or fewer band differences,12 corresponding to a similarity index of ∼80%. Therefore, a cluster was defined as three or more isolates sharing ⩾80% similarity on the dendrogram.
Results
A list of LVFX-resistant strains obtained from Hong Kong, Okinawa Island and the Japanese main island and susceptibilities of several antibiotics against these strains are shown in Table 1. The MICs for LVFX, TFLX, CPFX, SPFX, GFLX, STFX, PCG, CFPN, CDTR, CAM and AZM against the control strain, ATCC 700669, were 1, 0.12, 2, 0.25, 0.25, 0.06, 2, 1, 1, <0.06 and <0.06 mg l−1, respectively (Table 1). The MICs for LVFX, TFLX, CPFX, SPFX, GFLX, STFX, PCG, CFPN, CDTR, CAM and AZM against the second control strain, ATCC 700671, were 1, 0.12, 1, 0.25, 0.25, <0.03, 2, 1, 0.5, <0.06 and <0.06 mg l, respectively (Table 1).
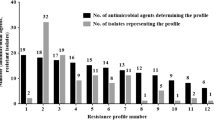
The ranges of MICs for PCG, CFPN, CDTR, CAM and AZM against isolates resistant to LVFX (MIC 4–32 mg l−1) are shown in Figure 1. Strains obtained from Okinawa had relatively high susceptibilities to β-lactams and macrolides (Table 1; Figure 1). In addition, the ranges of MICs for LVFX, TFLX, CPFX, SPFX, GFLX and STFX against isolates resistant to LVFX (MIC 4–32 mg l−1) are shown in Figure 2. STFX demonstrated the lowest MICs against LVFX-resistant strains (Figure 2). The range of MIC for STFX against isolates resistant to LVFX (MIC 4–32 mg l−1) was 0.125–0.5 mg l−1 and the MIC80 for STFX against LVFX-resistant isolates was 0.25 mg l−1 (Table 1; Figure 2).

Susceptibilities for several antibiotics of clinically isolated strains of levofloxacin (LVFX)-resistant S. pneumoniae. Susceptibilities to penicillin G, cefcapene, cefditoren, clarithromycin and azithromycin were evaluated in 19 strains obtained from Hong Kong, 9 strains obtained from Okinawa and 12 strains obtained from the Japanese main island. A full color version of this figure is available at The Journal of Antibiotics journal online.

Susceptibilities of clinically isolated strains of levofloxacin (LVFX)-resistant S. pneumoniae to several fluoroquinolones. Susceptibilities to sitafloxacin (STFX), tosufloxacin (TFLX), levofloxacin (LVFX), ciprofloxacin (CPFX), sparfloxacin (SPFX) and gatifloxacin (GFLX) were evaluated in 19 strains obtained from Hong Kong, 9 strains obtained from Okinawa and 12 strains obtained from the Japanese main island. A full color version of this figure is available at The Journal of Antibiotics journal online.
Nucleotide sequencing of the region encoding the QRDRs of gyrA, gyrB, parC and parE was carried out to investigate the involvement of gene mutations in LVFX-resistant clinical isolates. The results of sequencing analysis were reproducible. Table 2 summarizes the substitutions of deduced amino-acid sequences within QRDRs of gyrA, gyrB, parC and parE of the 42 LVFX-resistant strains. All 40 LVFX-resistant strains had more than one amino-acid substitution in the QRDRs of gyrA, gyrB, parC or parE, which included Ser81Tyr/Phe, Glu85Lys, Ser114Gly and Ala115His in gyrA, Ser79Phe/Ile/Tyr, Asp83Tyr, Asn91Asp, Ser107Phe, Lys137Asn and Ala142Ser in parC and Asp435Asn and Ile460Val in parE. Among these, 34 strains had amino-acid substitutions in both QRDRs of gyrA and parC. Most isolates had Ser81Tyr/Phe in gyrA, and Ile460Val substitutions in parE. Only one strain (#19) had the amino-acid substitution Arg477His in gyrB (Table 2).
PBP gene mutations
Among 42 isolates, 40 had mutations in the PBP genes. Only two strains obtained from Okinawa Island (#27 and #28) had no mutations in PBP genes (Table3). Thirty-one strains had pbp1a+2x+2b, two strains (#22 and #29) had pbp2x+2b, three strains (#24, #32 and #36) had pbp2x, one strain (#25) had pbp2b, and three strains (#31, #40 and #42) had pbp1a+2x (Table 3). In particular, all 19 strains obtained from Hong Kong had pbp1a+2x+2b. In contrast, strains obtained from Okinawa Island and the Japanese main island demonstrated heterogeneous mutation patterns in PBP genes (Table 3).
Expressions of macrolide-resistant genes
Among 42 strains, 18 strains had mefA gene expression and 18 strains had ermB gene expression. Only one strain (#26) expressed both mefA gene and ermB gene.
Patterns of PFGE
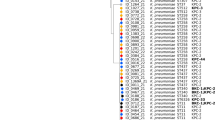
Two ATCC strains (ATCC 700669 and ATCC 70671) and 40 LVFX-resistant strains were classified in 25 different PFGE patterns (Figure 3; Table 3). Two strains obtained from Okinawa Island showed similar PFGE patterns (as shown G1 and G2 in Table 3). In particular, 15 of 19 strains obtained from Hong Kong had a similar PFGE pattern (as shown C in Table 3). In addition, three strains among the remaining four strains obtained from Hong Kong had a similar PFGE pattern (as shown E in Table 3). In contrast, strains obtained from Okinawa Island and the Japanese main island demonstrated heterogeneous patterns by PFGE (Table 3).

Genomic analysis of two ATCC strains and 40 clinically isolated strains of levofloxacin (LVFX)-resistant S. pneumoniae by pulsed-field gel electrophoresis (PFGE).
Discussion
The emergence of quinolone-resistant S. pneumoniae is an important clinical issue. In the PROTEKT study, it has been demonstrated that the frequency of quinolone-resistant S. pneumoniae strains in Asia is ∼3.5%, and the prevalence rate of quinolone-resistant S. pneumoniae has been indicated as high in Hong Kong.13
Given this information, the purpose of the present study was to compare LVFX-resistant strains obtained from Hong Kong, Okinawa Island and the Japanese main island (Honshu) by analyzing the heterogeneity of strains, drug sensitivities, amino-acid substitutions at QRDRs, PBP alterations, expressions of mefA and ermB genes and PFGE patterns. Based on the data of drug sensitivity tests, it was suggested that strains obtained from Okinawa Island have relatively high susceptibilities to β-lactams and macrolides. Interestingly, based on the data of PBP gene mutations, all 19 strains obtained from Hong Kong had pbp1a+2x+2b. In contrast, strains obtained from Okinawa Island and the Japanese main island demonstrated heterogeneous mutation patterns in the PBP genes. Based on the data of PFGE patterns, 15 of 19 strains obtained from Hong Kong had similar migration patterns. In addition, three strains among the remaining four strains obtained from Hong Kong had similar PFGE patterns. In contrast, strains obtained from Okinawa Island and the Japanese main island demonstrated heterogeneous patterns by PFGE. These data suggested that the same or closely related strains of bacteria had been transmitted in Hong Kong, since strains obtained from Hong Kong were derived from the relatively small restricted area. In addition, it is well known that nosocomial, familial or social droplet transmission was possible in S. pneumoniae infection. Therefore, the rate of LVFX resistance was high and PBP as well as PFGE pattern were similar in Hong Kong. In contrast, strains obtained from Okinawa Island as well as Japan were derived from relatively wide geographic areas.
Recently, Hong Kong investigators demonstrated high rates of resistance of S. pneumoniae isolates to various fluoroquinolones and the presence of the Spanish 23F clone that had acquired fluoroquinolone resistance while circulating in Hong Kong.14, 15, 16 Our data confirmed a prevalence of similar strains of LVFX-resistant S. pneumoniae in Hong Kong. Although the overall rate of strains resistant to fluoroquinolones remains low in most Asian countries, the emergence of highly resistant strains to fluoroquinolones will likely be a concern in the future with regard to the treatment of pneumococcal pneumonia. In fact, clinical failures of LVFX for the treatment of pneumococcal pneumonia have already been documented.17 To overcome this problem, STFX, a recently developed quinolone, is potent against Gram-positive cocci as well as Gram-negative rods, and excellent activities of these drugs against S. pneumoniae have been reported.18 In the present study, STFX had significantly lower MICs against S. pneumoniae with resistance to LVFX, compared with other quinolones tested, and these findings support previous reports that show the potency of this drug against LVFX-resistant S. pneumoniae with defined multiple mutations within both the gyrase A and topoisomerase IV genes.19, 20 Interestingly, three (#13, #29 and #30) of five strains (#13, #18, #29, #30 and #35) that showed a higher MIC (0.5 mg l−1) against LVFX-resistant strains possessed Glu85Lys substitutions in gyrA. This suggests that the primary target of STFX may be gyrA, and Glu85Lys substitution in gyrA reflected the higher MIC for STFX.
The reason why STFX was potent compared with other quinolones based on mutations in gyrA should be discussed. In general, quinolones are known to interact with two related but distinct targets: DNA gyrase and topoisomerase IV. The recognition of dual drug target enzymes also has important implications for the development of resistance. For resistance mutations in the primary target enzyme, the increment in resistance may be limited by the level of sensitivity of the unmutated secondary target enzyme, which becomes the more sensitive enzyme when the primary target is resistant.21 This scheme implies that concurrent dual mutations in both target enzymes would be required for any quinolone that had equal potency against DNA gyrase and topoisomerase IV.21 In the present study, as STFX has strong activity against LVFX-resistant S. pneumoniae, it was suggested that STFX might have equal strong inhibitory activity against DNA gyrase as well as topoisomerase IV.
There may be some limitations in interpreting the data from this study. Since pneumococcal isolates were collected from one or two referral centers, mainly in urban areas, and the number of isolates was relatively small, data from this study may not reflect the overall resistance status in these populations.
In summary, LVFX-resistant S. pneumoniae isolated in Hong Kong showed similarities to strains from Okinawa Island and the Japanese main island. In addition, STFX was potent against LVFX-resistant S. pneumoniae with multiple mutations in QRDRs of gyrase A and topoisomerase IV. Further clinical studies are warranted to evaluate the usefulness of STFX against infections caused by LVFX-resistant S. pneumoniae.
References
Appelbaum, P.C. Resistance among Streptococcus pneumoniae: implications for drug selection. Clin. Infect. Dis. 34, 1613–1620 (2002).
File, T.M. Jr. Clinical implications and treatment of multiresistant Streptococcus pneumoniae pneumonia. Clin. Microbiol. Infect. 12 (suppl. 3), 31–41 (2006).
Broskey, J. et al. Efflux and target mutations as quinolones resistance mechanisms in clinical isolates of Streptococcus pneumoniae. J. Antimicrob. Chemother. 45 (suppl. 1), 95–99 (2000).
Richter, S.S. et al. The molecular epidemiology of Streptococcus pneumoniae with quinolone resistance mutations. Clin. Infect. Dis. 40, 225–235 (2005).
National Committee for Clinical Laboratory Standards. Methods for Dilution Antimicrobial Susceptibility Tests for Bacteria That Grow Aerobically. Approved Standard, 6th edn. NCCLS document M7-A6. (NCCLS, Wayne, PA, USA, 2003).
Pestova, E., Beyer, R., Cianciotto, N.P., Noskin, G.A. & Peterson, L.A. Contribution of topoisomerase IV and DNA gyrase mutations in Streptococcus pneumoniae to resistance to novel fluoroquinolones. Antimicrob. Agents Chemother. 43, 2000–2004 (1999).
Ubukata, K., Muraki, T., Igarashi, A., Asahi, Y. & Konno, M. Identification of penicillin and other beta-lactam resistance in Streptococcus pneumoniae by polymerase chain reaction. J. Infect. Chemother. 3, 190–197 (1997).
Harimaya, A. et al. Alterations of pbp1a, pbp2b, and pbp2x in Streptococcus pneumoniae isolates from children with otolaryngological infectious disease in the Sapporo district of Japan. J. Infect. Chemother. 12, 366–371 (2006).
Ubukata, K., Iwata, S. & Sunakawa, K. In vitro activities of new ketolide, telithromycin, and eight other macrolide antibiotics against Streptococcus pneumoniae having mefA and that mediate macrolide resistance ermB genes. J. Infect. Chemother. 9, 221–226 (2003).
Lefevre, J. C., Faucon, G., Sicard, A. M. & Gasc, A. M. DNA fingerprinting of Streptococcus pneumoniae strains by pulsed-field gel electrophoresis. J. Clin. Microbiol. 31, 2724–2728 (1993).
McEllistrem, M. C., Stout, J. E. & Harrison, L. H. Simplified protocol for pulsed-field gel electrophoresis analysis of Streptococcus pneumoniae. J. Clin. Microbiol. 38, 351–353 (2000).
Tenover, F. C. et al. Interpreting chromosomal DNA restriction patterns produced by pulsed-field gel electrophoresis: criteria for bacterial strain typing. J. Clin. Microbiol. 33, 2233–2239 (1995).
Felmingham, D., Reinert, R. R., Hirakata, Y. & Rodloff, A. Increasing prevalence of antimicrobial resistance among isolates of Streptococcus pneumoniae from the PROTEKT surveillance study, and comparative in vitro activity of the ketolide, telithromycin. J. Antimicrob. Chemother. 50 (suppl. S1), 25–37 (2002).
Critchley, I. A. et al. Phenotypic and genotypic analysis of levofloxacin-resistant clinical isolates of Streptococcus pneumoniae collected in 13 countries during 1999-2000. Int. J. Antimicrob. Agents 20, 100–107 (2002).
Canton, R., Morosini, M., Enright, M. C. & Morrissey, I. Worldwide incidence, molecular epidemiology and mutations implicated in fluoroquinolone-resistant Streptococcus pneumoniae: data from the global PROTEKT surveillance programme. J. Antimicrob. Chemother. 52, 944–952 (2003).
Ho, P. L. et al. Fluoroquinolone and other antimicrobial resistance in invasive pneumococci, Hong Kong, 1995-2001. Emerg. Infect. Dis. 10, 1250–1257 (2004).
Fuller, J. D. & Low, D. E. A review of Streptococcus pneumoniae infection treatment failures associated with fluoroquinolone resistance. Clin. Infect. Dis. 41, 118–121 (2005).
Jolley, A., Andrews, J.M., Brenwald, N. & Wise, R. The in-vitro activity of a new highly active quinolone, DU-6859a. J. Antimicrob. Chemother. 32, 757–763 (1993).
Jones, M. E. et al. Prevalence of gyrA, gyrB, parC, and parE mutations in clinical isolates of Streptococcus pneumoniae with decreased susceptibilities to different fluoroquinolones and originating from worldwide surveillance studies during 1997-1998 respiratory season. Antimicrob. Agents Chemother. 44, 462–466 (2000).
Browne, F.A. et al. Antipneumococcal activity of DK-507k, a new quinolone, compared with the activities of 10 other agents. Antimicrob. Agents Chemother. 47, 3815–3824 (2003).
Hooper, D.C. Mechanisms of action of antimicrobials: focus on fluoroquinolones. Clin Infect Dis. 32 (suppl. 1), S9–15 (2001).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
JF has served on speaker’s bureaus for GlaxoSmithKline, Abbott Japan, Boehringer Ingelheim, Pfizer, Astellas, Daiichi Sankyo and Taisho Toyama.
Rights and permissions
About this article
Cite this article
Sunagawa, S., Fujita, J., Higa, F. et al. Comparison of drug sensitivity and genotypes of clinically isolated strains of levofloxacin-resistant Streptococcus pneumoniae obtained from Okinawa Island, the Japanese main island and Hong Kong. J Antibiot 64, 539–545 (2011). https://doi.org/10.1038/ja.2011.46
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/ja.2011.46
Keywords
This article is cited by
-
Development and characterisation of highly antibiotic resistant Bartonella bacilliformis mutants
Scientific Reports (2016)
