
Abstract
Objective:
Infant growth trajectories, in terms of size, tempo and velocity, may programme lifelong obesity risk. Timing of breastfeeding cessation and weaning are both implicated in rapid infant growth; we examined the association of both simultaneously with a range of growth parameters.
Design:
Longitudinal population-based twin birth cohort.
Subjects:
The Gemini cohort provided data on 4680 UK infants with a median of 10 (interquartile range=8–15) weight measurements between birth and a median of 6.5 months. Age at breastfeeding cessation and weaning were reported by parents at mean age 8.2 months (s.d.=2.2, range=4–20). Growth trajectories were modelled using SuperImposition by Translation And Rotation (SITAR) to generate three descriptors of individual growth relative to the average trajectory: size (grams), tempo (weeks, indicating the timing of the peak growth rate) and velocity (% difference from average, reflecting mean growth rate). Complex-samples general linear models adjusting for family clustering and confounders examined associations between infant feeding and SITAR parameters.
Results:
Longer breastfeeding (>4 months vs never) was independently associated with lower growth velocity by 6.8% (s.e.=1.3%) and delayed growth tempo by 1.0 (s.e.=0.2 weeks), but not with smaller size. Later weaning (⩾6 months vs <4 months) was independently associated with lower growth velocity by 4.9% (s.e.=1.1%) and smaller size by 102 g (s.e.=25 g).
Conclusions:
Infants breastfed for longer grew slower for longer after birth (later peak growth rate) but were no different in size, while infants weaned later grew slower overall and were smaller but the timing of peak growth did not differ. Slower trajectories with a delayed peak in growth may have beneficial implications for programming later obesity risk. Replication in cohorts with longer follow-up, alternative confounding structures or randomised controlled trials are required to confirm the long-term effects and directionality, and to rule out residual confounding.
Similar content being viewed by others
Introduction
Faster infant growth is an established risk factor for later obesity.1 Twin analyses indicate less genetic influence on infancy weight gain than later in childhood, which points towards a critical period when growth is more easily modified by environmental factors.2,3 Infant feeding practices are often targeted as modifiable environmental factors for obesity prevention.4, 5, 6 However, although systematic reviews of prospective cohorts support a small protective effect of breastfeeding on later obesity,7,8 most studies of the age at weaning and subsequent obesity have reported no evidence of association.9 Mixed findings from cohort studies are supported by results from randomised controlled trials (RCTs) like PROBIT, a large long-term RCT of breastfeeding exclusivity and duration, which found no differences in obesity prevalence at age 6.5 or 11.5 years.10,11 Three shorter-term RCTs of weaning at 6 vs 4 months found no differences in anthropometric outcomes between 6 and 12 months.12, 13, 14 There is a suggestion from two US and Danish Cohorts that early weaning (before 4 months) is only associated with later weight gain if breastfeeding also ceased by 4 months,15,16 indicating that it may be important to account for both feeding practices concurrently.
Furthermore, single measures of obesity or weight gain between just two time points may not be sufficient to capture the complexity of differences in growth trajectories exhibited by infants in relation to later health risk. For example, it has been reported that breastfeeding is associated with slower growth between 3 and 6 months but faster growth later on,17,18 and emerging evidence suggests that the timing of rapid growth (tempo) itself may have an independent role in modifying the risk of later disease.19 Similar indicators of developmental timing like adiposity rebound, puberty onset and peak height velocity are associated with a higher risk of adult disease,20, 21, 22, 23 suggesting that an accelerated tempo of infant growth may be detrimental to obesity risk.
SuperImposition by Translation And Rotation (SITAR) is a novel method of modelling growth in terms of the size, velocity and tempo of infant weight trajectories.24 Two existing studies that have analysed associations between infant feeding and SITAR have reported conflicting results. In 5949 infants from Hong Kong,25 longer breastfeeding was associated with a 3% increased growth velocity from birth to 1 year. Conversely, in 602 Australian infants, longer breastfeeding was associated with smaller size and reduced growth velocity from birth to 1 year.26 Although infant growth in a rapidly developing economy like Hong Kong, with a different social gradient in infant feeding practices, may genuinely differ from developed economies like Australia, the less detailed measurement of infant feeding in the Hong Kong study may also impact the findings. Neither of these studies has reported the effects of infant feeding on growth tempo or accounted for age at weaning in the same analyses. Furthermore, we are not aware of any investigation of associations between weaning and SITAR parameters, which may shed new light on the role of infant feeding, growth and risk of obesity. Therefore, we aimed to explore the independent associations between infant feeding and the size, tempo and velocity of growth trajectories modelled with SITAR in a large UK twin birth cohort.
Materials and methods
Data came from Gemini,27 a twin birth cohort initiated in 2007 based in England and Wales involving 2402 families (4804 infants) who returned a baseline questionnaire (70% of those contacted and 36% of all eligible families). Parents provided informed written consent and ethical approval was granted by the University College London Committee for the Ethics of non-National Health Service Human Research. All aspects of the data collection and storage were in accordance with the standards stipulated by this body.
Infant feeding practices were assessed in questionnaires completed by the parents at baseline and first follow-up, at mean child ages of, respectively, 8.2 months (s.d.=2.2, range=4–20) and 15.8 months (s.d.=1.1, range=14–27). Duration of breastfeeding (weeks) was calculated as age at cessation minus age at initiation. Three broad levels (none, birth to 4 months, >4 months) and seven detailed levels (none, birth to 1 week, 1 week to 1 month, >1–2 months, >2–3 months, >3–4 months, >4 months) were defined. Age at weaning (first introduction of solid food) was categorised into three broad levels (birth to 4 months, 5 months, 6+ months) and five detailed levels (birth to 3 months, 4 months, 5 months, 6 months, 7+ months).
Infants in England and Wales are measured regularly by health professionals, and weights are recorded in a personal child health record. Gemini parents copied the weights and dates into the questionnaires. A median of 10 (interquartile range (IQR)=8–15) weight measurements per child were reported from birth to median age 6.6 (IQR=5.2–8.3) months. Weights at particular ages: birth (n=4639), 3 months (n=4214) and 6 months (n=3424) were identified for descriptive purposes as those measured closest to, but within 1 month of, that particular age (exact age was recorded). Weight standard deviation scores were calculated adjusted for age, sex and gestational age based on the British 1990 growth reference.28,29
Weight trajectories were analysed using the SITAR method 24 as detailed elsewhere,3 the model including all infants who had at least one weight (124 infants had no weight recorded). Briefly, SITAR is a shape invariant model with random effects26 that estimates an average growth curve for the sample, plus a set of three parameters for each individual that together transform the average growth curve to match each individual’s growth (for examples of growth curves see Figure 1). Size is expressed in grams with higher values representing larger mean size than average (an upward translation of the weight curve); tempo, the age at peak weight velocity, is expressed in weeks with higher values representing delayed tempo compared with the average tempo (a rightward shift or translation of the weight velocity curve); velocity is expressed as a percentage deviation from mean velocity30 with higher values representing faster growth than average (an anticlockwise rotation of the weight curve and an upward translation of the weight velocity curve). The random effects have mean zero and standard deviations estimated from the data. The SITAR analysis was done using a dedicated library written by TJC and based on the nlme library31 in the statistical package R,32 and the model included fixed effects adjusting for gestation and sex.

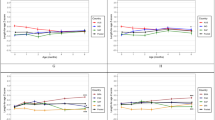
Average weight and weight gain velocity curves for extreme groups of (a) breastfed and (b) weaned infants. Mean size, tempo and velocity of each group ((a) never (black) or >4 months (grey) breastfed; (b) 0–4 months (black) or 6+ months (grey) at weaning) were used to plot the average weight (solid lines) and weight gain velocity (dashed lines) curves. Dotted vertical lines represent post-menstrual age in weeks equivalent to categories of breastfeeding duration and age at weaning (that is, age 4 months since birth is 17 weeks + 36 weeks mean gestation=53 weeks post-menstruation).
Sex, birth order, gestational age, maternal smoking status during pregnancy, maternal education and parental occupation, and dates of birth for children and mothers were reported in the baseline questionnaire. A validated questionnaire33 established zygosity. Mothers reported their height and weight at baseline from which body mass index (BMI) was calculated. Socioeconomic status (SES) was indicated by high, medium and low categories of maternal education and parental occupation classified using the National Statistics Socioeconomic Class index.34 Parity was represented by the number of other children living with the twins sharing a biological mother.
Analyses were performed in SPSS v17 (SPSS Inc, Chicago, IL, USA). Descriptive analyses are presented for all subjects with data available on infant feeding, using mean and standard deviation (s.d.; continuous and normal), median and IQR (continuous and skewed), or frequencies and percentages (categorical). Complex-samples general linear model assessed associations between growth and infant feeding practices adjusting for family clustering and confounders. Separate models were specified for size, tempo or velocity as the outcome, with independent variables included in a staged approach: (1) either breastfeeding or weaning only, (2) adding twin birth order, sex, zygosity, gestational age, age at baseline (child and mother), parental occupation, maternal education, parity, pregnancy smoking and maternal BMI and (3) adding the other feeding behaviour (that is, breastfeeding and weaning), to identify independent effects. Potential confounders were included if they were associated with both infant feeding and SITAR variables. The reference groups were ‘never breastfed’ and ‘weaned ⩽4 months’.
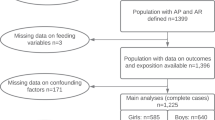
Linearity of infant feeding associations across categories was explored by replacing each category value with the ‘event age’ (the median age for each weaning or breastfeeding cessation group), and then testing for a linear trend in event age. For this comparison, the detailed breastfeeding and weaning categories were used and regression coefficients represented effects on size, tempo or velocity per week of breastfeeding or month of weaning. Shape plots of size, tempo or velocity vs event age were obtained for breastfeeding and weaning by separately plotting the category means for each growth parameter, adjusted via model 3, against the corresponding event ages. All models were for 4251 infants with complete data on infant feeding, covariates and growth parameters (Supplementary Figure 1).
Results
Almost a quarter of infants (n=1097) were never breastfed; of those breastfed (n=3675), 32% were breastfed for more than 4 months (Table 1) but the median duration of breastfeeding was 8 (IQR=4–23) weeks. Exclusive breastfeeding for 1 day or more occurred in 59% of breastfed infants, but the median duration of exclusive breastfeeding was just 4 (IQR=2–21) days. Only 111 infants were exclusively breastfed for more than 4 months (3% of those breastfed, 2% overall). Subsequent analyses are based on exclusive and partial breastfeeding combined.
Age of weaning was 4 months or earlier in 37% and 6 months or later in 28% of the sample (Table 2). Mean age at weaning was 4.6 (s.d.=1.0) months among infants never breastfed, 4.9 (s.d.=1.1) months among those breastfed to 4 months and 5.2 (s.d.=1.0) for those breastfed for more than 4 months (P<0.0001). Median age at breastfeeding cessation was 6 (IQR=3–12) weeks among infants weaned between 0 and 4 months, 8 (IQR=3–16) weeks among those weaned at 5 months and 12 (IQR=6–28) weeks for those weaned at 6 months or later (P<0.0001). Shorter breastfeeding was associated with being male, monozygotic, younger at baseline and having older siblings, a shorter gestation, and a mother of lower SES, younger, with a higher BMI and smoking in pregnancy (all P<0.05, Table 1). Similar associations were observed for earlier weaning except that zygosity was unrelated, and longer gestation was associated with earlier weaning (Table 2).
Earlier weaning was associated with a higher weight standard deviation score at birth, 3 and 6 months (Table 2), whereas shorter breastfeeding was associated with a higher weight standard deviation score at 3 and 6 months only (Table 1). Figure 1 illustrates SITAR model-1-based mean weight and weight velocity curves for extreme groups of breastfed and weaned infants, illustrating the clear peak in velocity soon after 40 post-menstrual weeks. The groups were similar at birth, but clear differences emerged by 90 post-menstrual weeks (approximately 12 months since birth), suggesting that both never breastfeeding and earlier weaning (solid black lines) are associated with larger size compared with breastfeeding for 4 months or more and weaning at 6 months or later. For never breastfed infants, the age at peak weight velocity is earlier (Figure 1a, dashed black line), signifying an advanced growth tempo compared with infants breastfed for longer (Figure 1a, dashed grey line). Both never breastfed infants and those weaned earlier (black dashed lines) displayed higher peaks in weight velocity indicating a faster growth trajectory than infants breastfed for longer or weaned later (dashed grey lines).
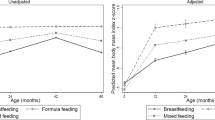
In adjusted models with the SITAR parameter size as the outcome, later weaning, but not longer breastfeeding, was independently associated with smaller size; infants weaned at or after 6 months were 102 g (s.e.=25 g) smaller than those weaned by 4 months (Supplementary table 1, model 3). The relationship was linear, with size decreasing by 46 g (s.e.=11 g) for each extra month that weaning was postponed (Figure 2).

Size by age at weaning or cessation of breastfeeding group mean (95% confidence interval (CI)) plotted against the group median event age (age at weaning or cessation of breastfeeding). Means derived from complex-samples general linear model with size as the outcome; independent variables median age at cessation of breastfeeding (seven groups: (i) 0 weeks; (ii) 1 week; (iii) 3 weeks; (iv) 6 weeks; (v)12 weeks; (vi) 16 weeks; (vii) 28 weeks) and median age at weaning (five groups: (i) 3 months; (ii) 4 months; (iii) 5 months; (iv) 6 months; (v) 7months) adjusting for clustering of twins within families and twin order, sex, zygosity, gestational age, age at baseline (child and mother), parental occupation, maternal education, parity, pregnancy smoking, BMI. Tests for linear trend were performed by comparing models with the feeding practice variable categories coded either as median event age or level.
In adjusted models with the SITAR parameter tempo as the outcome, longer breastfeeding was independently associated with delayed growth tempo; growth rates of infants breastfed for more than 4 months peaked 1.0 (s.e.=0.2 weeks) later than those never breastfed (Supplementary Table1, model 3). The relationship was linear, with tempo delayed by 0.03 (s.e.=0.01 weeks) per extra week of breastfeeding (Figure 3). A weak association between age at weaning and tempo in the unadjusted model (infants weaned at or after 6 months peaked 0.3 (s.e.=0.1) weeks later than those weaned by 4 months, P=0.04) was attenuated after the inclusion of covariates (Supplementary Table 1, models 2 and 3) and there was no linear trend (Figure 3).

Tempo by age at weaning or cessation of breastfeeding. Group mean (95% confidence interval (CI)) plotted against the group median event age (age at weaning or cessation of breastfeeding). Means derived from complex-samples general linear model with tempo as the outcome; independent variables median age at cessation of breastfeeding (seven groups: (i) 0 weeks; (ii)1 week; (iii) 3 weeks; (iv) 6 weeks; (v)12 weeks; (vi) 16 weeks; (vii) 28 weeks) and median age at weaning (five groups: (i) 3 months; (ii) 4 months; (iii) 5 months; (iv) 6 months; (v) 7months) adjusting for clustering of twins within families and twin order, sex, zygosity, gestational age, age at baseline (child and mother), parental occupation, maternal education, parity, pregnancy smoking, BMI. Tests for linear trend were performed by comparing models with the feeding practice variable categories coded either as median event age or level.
In adjusted models with the SITAR parameter velocity as the outcome, both later weaning and longer breastfeeding were independently associated with lower growth velocity; infants weaned at or after 6 months grew 4.9% (s.e.=1.1%) slower than infants weaned by 4 months, and infants breastfed for more than 4 months grew 6.8% (s.e.=1.3%) slower than those never breastfed (Supplementary Table 1, model 3). Both relationships were linear (Figure 4), with growth velocity 2.2% (s.e.=0.5%) slower per extra month that weaning was postponed and 0.3% (s.e.=0.04%) slower per extra week of breastfeeding.

Velocity by age at weaning or cessation of breastfeeding. Group mean (95% confidence interval (CI)) plotted against the group median event age (age at weaning or cessation of breastfeeding). Means derived from complex-samples general linear model with velocity as the outcome; independent variables median age at cessation of breastfeeding (seven groups: (i) 0 weeks; (ii) 1 week; (iii) 3 weeks; (iv) 6 weeks; (v) 12 weeks; (vi) 16 weeks; (vii) 28 weeks) and median age at weaning (five groups: (i) 3 months; (ii) 4 months; (iii) 5 months; (iv) 6 months; (v) 7months) adjusting for clustering of twins within families and twin order, sex, zygosity, gestational age, age at baseline (child and mother), parental occupation, maternal education, parity, pregnancy smoking, BMI. Tests for linear trend were performed by comparing models with the feeding practice variable categories coded either as median event age or level.
Sensitivity analyses were performed to check if the results were altered by mutual adjustment for SITAR parameters, or by the reduction in sample size caused by the inclusion of covariates, but the pattern of results remained the same (Supplementary Table 1, models 4 and 5). All models were repeated in a restricted sample of twins born at term (gestational age ⩾37 weeks) and the pattern of results was unaltered (data not shown).
Discussion
In this study of infant feeding and growth trajectories, longer breastfeeding and later weaning were both associated with lower growth velocity, and additionally with delayed tempo and smaller size, respectively.
Growth velocity was 6.8% greater in those never breastfed vs those breastfed for more than 4 months, which is a slightly smaller effect than observed in an Australian study26 and contrasts with results from the Hong Kong cohort that found slower growth among less breastfed infants.25 Both of those studies modelled growth using SITAR, but the Hong Kong study characterised breastfeeding using a single cutoff of 1 month for exclusive breastfeeding, which may have lacked sensitivity. In Gemini and the Australian study, breastfeeding duration was recorded in more detail and specifically separated infants never breastfed from those breastfed for any duration. The SES patterning of weight/feeding differs in Hong Kong such that differences in associations might be explained by residual confounding by social class, which cannot be completely adjusted for in Gemini.35 However, infant feeding could plausibly be a mediator rather than a confounder of the relationship between SES and growth. We have demonstrated in earlier analyses of Gemini that the SES effect on weight change from birth to 3 months is attenuated primarily by adjustment for breast feeding rather than other SES-related factors like maternal smoking in pregnancy or parental BMI.36
In previous studies using SITAR, the effect of feeding on tempo was not reported (potentially because the importance of the timing of changes in growth was not recognised at that time) making it impossible to directly compare our results. Growth tempo, which is effectively the age when infant weight velocity peaks, is similar to subsequent developmental indicators such as the timing of adiposity rebound or the onset of puberty, which have evidence of an important role in programming later obesity and chronic disease risk.19, 20, 21, 22, 23 Previous research has shown that prolonged breastfeeding in Filipino girls was associated with delayed age at menarche, with the likelihood of early menarche falling by 6% per extra month of exclusive breastfeeding.37 In addition, breastfeeding for more than 4 months was associated with a 10-month delay in the age at adiposity rebound in children from an Australian cohort.38 These associations of longer breastfeeding with delayed development match results from Gemini and suggest that infant growth tempo could be an early indicator of developmental timing.
Infant feeding and growth were both measured longitudinally, but because they were modelled concurrently the direction of effect cannot be inferred, which is a limitation of our study. Feeding and growth are likely to be related in both directions, with transitions to formula or solid food potentially occurring in response to earlier growth rates39 as well as impacting on subsequent growth.18 Mothers may struggle to maintain breastfeeding when the infant’s rate of weight gain (and energy requirement and demand for food) is near its peak. Therefore, an advanced tempo might encourage earlier breastfeeding cessation because mothers conclude that breast milk alone is not enough to satisfy her infant’s appetite. Larger size and birth weight were related to earlier weaning, which raises the possibility of reverse causation in the weaning–growth association, that is, that babies who are born large grow faster and tend to be weaned earlier, because the larger size at birth precedes the exposure to early weaning. In contrast, breastfeeding initiation or duration is not associated with birth weight, indicating that the breastfeeding exposure is non-differential by size and occurs before the observed delay in tempo and slower growth trajectory. However, the causal nature of these associations should be explored using alternative study designs such as randomised controlled trials.
Although many potential confounders were controlled for, residual confounding remains a possibility. Sib-pair analyses are a good strategy to reduce the residual confounding effects of common maternal factors, for example, SES,40 but discordant feeding practice within twin pairs was rare in Gemini, and the informative sample size was insufficient to detect within-family associations. Arguably, within-pair differences in feeding may reflect individual infant factors, such as poor appetite or illness, or other problems related to growth that precede feeding method choices, which may limit the ability of a sib-pair design to completely address such queries. Ultimately, experimental studies involving randomisation of breastfeeding duration or weaning age, such as PROBIT10 and a recent Icelandic study,14 are needed to clarify remaining questions around the nature of causality in the associations observed in the current study.
The main limitation of the study is the use of a twin sample. Twins tend to be born smaller than singletons and subsequently grow faster.41 However, within twins the environmental causes of differences in growth should be similar, and associations between growth and feeding practices have not been noted to be different among twins vs singletons. Long-term health does not differ among twins compared with singletons, suggesting that the systematic difference in growth does not lead to fundamentally different health risks42 and that variation in growth rates within a twin sample are subject to the same causes and consequences as in singletons. The demands of breastfeeding are greater for mothers of twins, which may result in earlier cessation, but similar levels of variation in breastfeeding were observed in Gemini as in a national survey. The proportion of ever breastfed infants in Gemini (born in 2007) was 77% compared with 69% and 81% for multiple and singleton infants, respectively, in the UK 2010 Infant Feeding Survey.43 It was not possible to analyse associations with exclusive breastfeeding, because only 2% of Gemini infants were exclusively breastfed beyond 4 months, which restricted the power for estimating differences in growth trajectories. This issue is not limited to twin studies, however, as a comparable proportion of UK singletons (3–8%) are exclusively breastfed for 4 months.44 Another drawback, which exists in other cohort studies,45,46 is that higher SES families are over-represented in Gemini, thus the representative nature of the findings is limited to similar populations. This limitation is compounded by missing covariate data in 12% of the baseline sample, which excluded twins from lower SES families from the final analysis and with a shorter gestation (Supplementary Tables 2 and 3). Given that SES differences in infant feeding and weight gain have been observed in this sample,36 selection bias may have caused the associations between infant feeding and growth to be underestimated. However, unadjusted associations in those with available data on infant feeding and growth (n=4680) were similar to those in the sample with complete data (models 1 and 5, Supplementary Table 1).
The study is strengthened by having multiple weight measures, which increases the accuracy of growth trajectory estimates over measures from just one or two time points. SITAR accounts for the nonlinear shape of infant growth and has the advantage of efficiently estimating growth trajectories and using all the available data irrespective of measurement timing or frequency. Weight was measured by health professionals and extracted from child records, a process that compares well with clinic-based measures.47 The collection of infant feeding data during infancy is a strength because the potential for recall bias was reduced compared with studies that collected data after infancy.48 Maternal reporting of breastfeeding can be affected by social desirability and many other influences, which may result in both under- and over-reporting of breastfeeding duration.48 Random error reduces the study’s power to detect effects of a given size, suggesting that our results may underestimate the true association between infant feeding and growth. Finally, the application of SITAR to infant growth data is still relatively new. It is unclear whether the growth trajectory associated with longer breastfeeding and later weaning is optimal in terms of later health, although previous work characterising similar concepts like rapid infant growth and timing of adiposity rebound or puberty19, 20, 21, 22, 23 suggest that lower velocity and delayed tempo of growth would be beneficial to health. Future work should investigate how SITAR parameters relate to growth, body composition and health beyond infancy.
Conclusion
Longer breastfeeding and later weaning were both associated with lower growth velocity. Longer breastfeeding was also associated with delayed tempo, and later weaning with smaller size. These results support the hypothesis that longer breastfeeding and later weaning are associated with slower growth, but further research is needed to establish whether these associations are causal and if they could be modified to lower subsequent obesity risk.
References
Ong KK, Loos RJF . Rapid infancy weight gain and subsequent obesity: Systematic reviews and hopeful suggestions. Acta Paediatrica 2006; 95: 904–908.
Touwslager RN, Gielen M, Mulder AL, Gerver WJ, Zimmermann LJ, Fowler T et al. Changes in genetic and environmental effects on growth during infancy. Am J Clin Nut 2011; 94: 1568–1574.
Johnson L, Llewellyn CH, van Jaarsveld CHM, Cole TJ, Wardle J . Genetic and Environmental Influences on Infant Growth: Prospective Analysis of the Gemini Twin Birth Cohort. PLoS One 2011; 6: e19918.
US Department of Human Health Services. The Surgeon General's Vision for a Healthy and Fit Nation2010. Available from http://www.surgeongeneral.gov/initiatives/healthy-fit-nation/obesityvision2010.pdf.
Department of Health Social Services and Public Safety. Framework for Preventing and Addressing Overweight and Obesity in Northern Ireland 2012-2022: A Fitter Future for All2012. Available from http://www.dhsspsni.gov.uk/framework-preventing-addressing-overweight-obesity-ni-2012-2022.pdf.
Cross-Governmental Obesity Unit Department of Health Department for Children Schools and Families. Healthy Weight, Healthy Lives: a cross-government strategy for England2008. Available from http://webarchive.nationalarchives.gov.uk/20100407220245/http://www.dh.gov.uk/prod_consum_dh/groups/dh_digitalassets/documents/digitalasset/dh_084024.pdf.
Harder T, Bergmann R, Kallischnigg G, Plagemann A . Duration of Breastfeeding and Risk of Overweight: A Meta-Analysis. Am J Epidemiol 2005; 162: 397–403.
Arenz S, Ruckerl R, Koletzko B, von Kries R . Breast-feeding and childhood obesity–a systematic review. Int J Obes 2004; 28: 1247–1256.
Pearce J, Taylor MA, Langley-Evans SC . Timing of the introduction of complementary feeding and risk of childhood obesity: a systematic review. Int J Obes 2013; 37: 1295–1306.
Kramer MS, Matush L, Vanilovich I, Platt RW, Bogdanovich N, Sevkovskaya Z et al. Effects of prolonged and exclusive breastfeeding on child height, weight, adiposity, and blood pressure at age 6.5 y: evidence from a large randomized trial. Am J Clin Nut 2007; 86: 1717–1721.
Martin RM, Patel R, Kramer MS, Guthrie L, Vilchuck K, Bogdanovich N et al. Effects of promoting longer-term and exclusive breastfeeding on adiposity and insulin-like growth factor-I at age 11.5 years: a randomized trial. JAMA 2013; 309: 1005–1013.
Cohen RJ, Brown KH, Canahuati J, Rivera LL, Dewey KG . Effects of age of introduction of complementary foods on infant breast milk intake, total energy intake, and growth: a randomised intervention study in Honduras. Lancet 1994; 344: 288–293.
Dewey KG, Cohen RJ, Brown KH, Rivera LL . Age of introduction of complementary foods and growth of term, low-birth-weight, breast-fed infants: a randomized intervention study in Honduras. Am J Clin Nutr 1999; 69: 679–686.
Wells JC, Jonsdottir OH, Hibberd PL, Fewtrell MS, Thorsdottir I, Eaton S et al. Randomized controlled trial of 4 compared with 6 mo of exclusive breastfeeding in Iceland: differences in breast-milk intake by stable-isotope probe. Am J Clin Nut 2012; 96: 73–79.
Huh SY, Rifas-Shiman SL, Taveras EM, Oken E, Gillman MW . Timing of solid food introduction and risk of obesity in preschool-aged children. Pediatrics 2011; 127: e544–e551.
Baker JL, Michaelsen KF, Rasmussen KM, Sorensen TIA . Maternal prepregnant body mass index, duration of breastfeeding, and timing of complementary food introduction are associated with infant weight gain. Am J Clin Nut 2004; 80: 1579–1588.
Butte NF, Wong WW, Hopkinson JM, Smith EOB, Ellis KJ . Infant feeding mode affects early growth and body composition. Pediatrics 2000; 106: 1355–1366.
Rzehak P, Sausenthaler S, Koletzko S, Bauer CP, Schaaf B, von Berg A et al. Period-specific growth, overweight and modification by breastfeeding in the GINI and LISA birth cohorts up to age 6 years. Eur J Epidemiol 2009; 24: 449–467.
Leunissen RWJ, Kerkhof GF, Stijnen T, Hokken-Koelega A . Timing and tempo of first-year rapid growth in relation to cardiovascular and metabolic risk profile in early adulthood. JAMA 2009; 301: 2234–2242.
Williams SM, Goulding A . Patterns of growth associated with the timing of adiposity rebound. Obesity 2008; 17: 335–341.
Pierce MB, Leon DA . Age at menarche and adult BMI in the Aberdeen Children of the 1950s Cohort Study. Am J Clin Nut 2005; 82: 733–739.
Sandhu J, Ben-Shlomo Y, Cole TJ, Holly J, Davey Smith G . The impact of childhood body mass index on timing of puberty, adult stature and obesity: a follow-up study based on adolescent anthropometry recorded at Christ's Hospital (1936-1964). Int J Obes 2006; 30: 14–22.
Tzoulaki I, Sovio U, Pillas D, Hartikainen A-L, Pouta A, Laitinen J et al. Relation of immediate postnatal growth with obesity and related metabolic risk factors in adulthood: the Northern Finland Birth Cohort 1966 Study. Am J Epidemiol 2010; 171: 989–998.
Cole TJ, Donaldson MDC, Ben-Shlomo Y . SITAR–a useful instrument for growth curve analysis. Int J Epidemiol 2010; 39: 1558–1566.
Hui LL, Leung GM, Cowling BJ, Lam TH, Schooling CM . Determinants of infant growth: evidence from Hong Kong's ‘Children of 1997’ Birth Cohort. Ann Epidemiol 2010; 20: 827–835.
Beath KJ . Infant growth modelling using a shape invariant model with random effects. Stat Med 2007; 26: 2547–2564.
van Jaarsveld CHM, Johnson L, Llewellyn C, Wardle J . Gemini: a UK twin birth cohort with a focus on early childhood weight trajectories, appetite and the family environment. Twin Res Hum Genet 2010; 13: 72–78.
Freeman JV, Cole TJ, Chinn S, Jones PR, White EM, Preece MA . Cross sectional stature and weight reference curves for the UK, 1990. Arch Dis Childhood 1995; 73: 17–24.
Cole TJ Software for LMS method: LMSGrowth 24/04/2014. Available from http://www.healthforallchildren.com/?product=lmsgrowth.
Cole TJ . Sympercents: symmetric percentage differences on the 100 loge scale simplify the presentation of log transformed data. Stat Med 2000; 19: 3109–3125.
Pinheiro J, Bates D, DebRoy S, Sarkar D, team RC nlme: linear and nonlinear mixed effects models. R package version 3.1-92 ed, 2009.
R-Development-Core-Team. R: A Language and Environment For Statistical Computing. R Foundation for Statistical Computing: Vienna, 2009.
Price TS, Freeman B, Craig I, Petrill SA, Ebersole L, Plomin R . Infant zygosity can be assigned by parental report questionnaire data. Twin Res 2000; 3: 129–133.
Office for National Statistics O. National Statistics Socio-economic Classification: User Manual. Newport, UK, 2005.
Brion M-JA, Lawlor DA, Matijasevich A, Horta B, Anselmi L, Araújo CL et al. What are the causal effects of breastfeeding on IQ, obesity and blood pressure? Evidence from comparing high-income with middle-income cohorts. Int J Epidemiol 2011; 40: 670–680.
Wijlaars LP, Johnson L, van Jaarsveld CH, Wardle J . Socioeconomic status and weight gain in early infancy. International journal of obesity (2005) 2011; 35: 963–970.
Al-Sahab B, Adair L, Hamadeh MJ, Ardern CI, Tamim H . Impact of Breastfeeding Duration on Age at Menarche. Am J Epidemiol 2011; 173: 971–977.
Chivers P, Hands B, Parker H, Bulsara M, Beilin LJ, Kendall GE et al. Body mass index, adiposity rebound and early feeding in a longitudinal cohort (Raine Study). Int J Obes 2010; 34: 1169–1176.
Kramer MS, Moodie EEM, Dahhou M, Platt RW . Breastfeeding and Infant Size: Evidence of Reverse Causality. Am J Epidemiol 2011; 173: 978–983.
Ness AR, Griffiths AE, Howe LD, Leary SD . Drawing causal inferences in epidemiologic studies of early life influences. Am J Clin Nut 2011; 94: 1959S–1963S.
van Dommelen P, de Gunst MC, van der Vaart AW, van Buuren S, Boomsma D . Growth references for height, weight and body mass index of twins aged 0 to 2.5 years. Acta Paediatr 2008; 97: 1099–1104.
Öberg S, Cnattingius S, Sandin S, Lichtenstein P, Morley R, Iliadou AN . Twinship influence on morbidity and mortality across the lifespan. Int J Epidemiol 2012; 41: 1002–1009.
Department of Health DOH The Health and Social Care Information Centre HSIC. Infant Feeding Survey 2010: Early Results2011; (2012/10/01/). Available from http://www.ic.nhs.uk/catalogue/PUB00648/infa-seed-serv-2010-earl-resu-rep.pdf.
Kelly YJ, Watt RG . Breast-feeding initiation and exclusive duration at 6 months by social class? results from the Millennium Cohort Study. Public Health Nutr 2005; 8: 417–421.
Plewis I . Non-response in a birth cohort study: The Case of the Millennium Cohort Study. Int J Soc Res Methodol 2007; 10: 325–334.
ALSPAC. Representativeness of the ALSPAC cohort, 11/02/2010. Available from http://www.bristol.ac.uk/alspac/sci-com/resource/represent/, 2010.
Howe LD, Tilling K, Lawlor DA . Accuracy of height and weight data from child health records. Arch Dis Childhood 2009; 94: 950–954.
Li R, Scanlon KS, Serdula MK . The validity and reliability of maternal recall of breastfeeding practice. Nutr Rev 2005; 63: 103–110.
Acknowledgements
We thank the Gemini families who are participating in the study and the Office of National Statistics for their help in recruiting them. Gemini is funded by a Grant from Cancer Research UK (C1418/A7974 to JW). TJC is funded by MRC Grant MR/J004839/1.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
J Wardle and L Johnson have received funding for consultancy work from Danone Baby Nutrition. The remaining authors declare no conflict of interest.
Additional information
Supplementary Information accompanies this paper on International Journal of Obesity website
Rights and permissions
This work is licensed under a Creative Commons Attribution 3.0 Unported License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by/3.0/
About this article
Cite this article
Johnson, L., van Jaarsveld, C., Llewellyn, C. et al. Associations between infant feeding and the size, tempo and velocity of infant weight gain: SITAR analysis of the Gemini twin birth cohort. Int J Obes 38, 980–987 (2014). https://doi.org/10.1038/ijo.2014.61
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/ijo.2014.61
Keywords
This article is cited by
-
Prenatal exposures to mixtures of endocrine disrupting chemicals and children’s weight trajectory up to age 5.5 in the SELMA study
Scientific Reports (2021)
-
Breastfeeding and growth trajectory from birth to 5 years among children exposed and unexposed to gestational diabetes mellitus in utero
Journal of Perinatology (2021)
-
The effect of non-organophosphate household pesticides exposure during pregnancy on infants birth sizes and growth rate: a cohort study
BMC Pregnancy and Childbirth (2020)
