
Abstract
Abdominal obesity (AO) is strongly associated with increased cardiovascular risk in hypertensives. Visceral adipose tissue has an important part in water retention, the sympathetic nervous system and renin–angiotensin–aldosterone system activation, which may influence central and systemic hemodynamics. The aim of this study was to estimate the relationship between AO and the hemodynamic profile of patients with arterial hypertension (AH). The clinical evaluation of 144 hypertensives included the following: (1) echocardiographic assessment of the left ventricular ejection fraction (LVEF), the global longitudinal systolic strain (GLSS) and diastolic function (E/A—phase ratio of mitral flow early (E) and late (A) and E/e′—ratio of early mitral flow and mitral septal annulus early diastolic velocity (e′)); (2) the applanation tonometry including the central pulse pressure (CPP) and augmentation index (AI); and (3) the impedance cardiography, acceleration index (ACI), velocity index (VI), systemic vascular resistance index (SVRI) and total artery compliance (TAC). Obese hypertensives in comparison with non-obese ones were characterized with the following values: (1) lower echocardiographic (GLSS: −17.2±2.5% vs. −19.0±2.8%, P=0.0002) and impedance indices of left ventricular performance (VI: 44.8±12.4 vs. 51.6±14.2 × 1000*Ω* s−1, P=0.006; ACI: 66.7±27.8 vs. 79.1±31.2 100*Ω* s−2, P=0.003) and (2) worse diastolic function (e′: 9.08±2.69 vs. 10.39±2.34 cm*s−1, P=0.003; E/e′: 7.54±1.81 vs. 6.74±1.40, P=0.007; E/A: 1.02±0.34 vs. 1.15±0.33, P=0.008). No relevant differences for gender, age, blood pressure, heart rate, LVEF, SVRI, TAC, CPP and AI were identified. AH and AO have overlapping effects on cardiovascular hemodynamics. At the early asymptomatic stage, this overlap is exhibited in the impaired cardiac function.
Similar content being viewed by others


Introduction
Abdominal obesity (AO) is an independent and modifiable cardiovascular risk factor related to a higher occurrence of coronary artery disease, left ventricular (LV) dysfunction and heart failure.1, 2, 3 Obesity and arterial hypertension (AH) are closely related and their coexistence results in the harmful impairment of cardiovascular structure and function.1, 4, 5 However, previous studies suggest that overall obesity may result in different hemodynamic alterations than AH per se.5, 6 Normotensive obese subjects were shown to have higher volume load, higher cardiac output and lower systemic vascular resistance.6, 7 However, non-obese hypertensives present with vasoconstriction as the main mechanism of increased blood pressure (BP).5 These cardiovascular alterations in obese hypertensives can overlap, resulting in various hemodynamic constellations.5, 6, 7, 8 This multifaceted interplay becomes even more complicated in view of the findings that patients with AO may present different hemodynamic patterns than those with overall obesity.8 AO correlates with higher metabolic activity strongly related to the increased activity of the sympathetic nervous system and the renin–angiotensin–aldosterone system, as well as altered endothelial dysfunction and hyperinsulinemia.8, 9, 10, 11 As a consequence, hypertensives with android obesity present higher arterial stiffness and impaired LV performance.11, 12, 13 It is suggested that AO should be included in the models assessing cardiovascular risk as an independent variable.14, 15
These hemodynamic differences between the types of obesity and AH provoke vivid scientific discussions. There is still a need for research on these complex mechanisms to gain a better understanding of the pathophysiological background of the obesity-related AH, which is essential for development of successful treatment strategies. Although the use of noninvasive techniques sensitive enough to detect subclinical cardiovascular disturbances is still limited, some promising methods appear to be on the horizon. Global longitudinal systolic strain (GLSS), a modern, well-validated, echocardiographic method of assessment of LV contractile deformation,16, 17, 18 was shown to be an independent predictor of outcome in patients with AH, heart failure and myocardial infarct.19, 20 Other noninvasive diagnostic techniques, such as impedance cardiography (ICG) and applanation tonometry (AT), provide additional data on arterial stiffness, central BP, fluid load and LV performance.21, 22 When used together, these methods provide detailed insight into the sex-specific patterns of aging23 and the pathophysiological background of subclinical LV dysfunction.24
Based on these assumptions, we hypothesize that at the early stage of hypertensive disease related to AO, the complex ventricular–vascular interplay may be successfully assessed by the combination of the above methods. Thus, the purpose of this study was to investigate the relationship between AO and hemodynamics that was evaluated with the use of echocardiography, AT and ICG in young and middle-aged hypertensives.
Methods
Study population
The group selected for this analysis comprised patients with at least a 3-month history of AH defined according to the European Society of Cardiology guidelines1 and who were included in the prospective clinical study. We excluded patients with the following criteria: (1) confirmed secondary AH, (2) AH treated with three or more medicines before recruitment, (3) heart failure, (4) cardiomyopathy, (5) significant heart rhythm disorders, (6) significant valvular disease, (7) kidney failure (glomerular filtration rate below 60 ml*min−1 per 1.73 m2), (8) chronic obstructive pulmonary disease, (9) diabetes, (10) polyneuropathy, (11) peripheral vascular disease or (12) an age <18 years. The subjects treated with hypotensive drugs were recommended to discontinue them at least 7 days before the examination. The study was conducted according to the Good Clinical Practice guidelines and the Declaration of Helsinki, with the approval of the local ethics committee. Each patient provided written informed consent to participate in the study.
The clinical examination included analysis of cardiovascular risk factors, symptoms indicating secondary cause of AH and laboratory tests (creatinine, glomerular filtration rate, total cholesterol, low-density lipoprotein cholesterol, high-density lipoprotein cholesterol, triglycerides and fasting glucose). Body mass index was derived from height and weight. Patients with metabolic syndrome were defined according to the IDF (International Diabetes Federation) criteria25 and AO according to the European Society of Cardiology guidelines as waist circumference (WC) in men ⩾102 cm and in women ⩾88 cm.1
Office blood pressure measurement
The office blood pressure measurement (OBPM) was performed in the morning (Omron M4 Plus, Omron Healthcare Co. Ltd., Kyoto, Japan) by a technique compliant with the European Society of Cardiology guidelines.1 Automated systolic BP (SBP) and diastolic BP (DBP) measurement was supervised by a trained physician or nurse, after a minimum 5 min of rest in a sitting position. The study only included the patients with AH confirmed in ABPM.
Echocardiography
Two-dimensional echocardiography was performed using standard parasternal, apical and subcostal views (2.5 MHz transducer; VIVID S6 GE Medical System, Wauwatosa, WI, USA). The dimension of the left atrium (LA), left ventricular end-diastolic diameter (LVEDD) and interventricular septum diameter were measured in the parasternal long-axis view in late diastole of the LA and left ventricle (LV), respectively. Left ventricular enlargement was defined as LVEDD indexed to the body surface area >3.2 cm m−2 for men and >3.1 cm*m−2 for women, and LA enlargement as LA >4.0 cm for men and >3.8 cm for women. Left ventricular ejection fraction was calculated according to Simpson’s formula using a two-dimensional image of the LV chamber during systole and diastole in the 4- and 2-chamber apical views. The left ventricular hypertrophy (LVH) was diagnosed according to the ASE-recommended formula for estimation of the left ventricular mass index (LVMI) from two-dimensional linear LV measurements and indexed to the body surface area (cutoff values for men LVMI >115 g*m−2 and for women >95 g*m−2).
Mitral valve inflow was recorded in the apical 4-chamber view with pulsed wave Doppler gate positioned in the LV on the level of the mitral valve edges. The following parameters were measured: mitral inflow early (E) and late (A) phase ratio (E/A), and early phase deceleration time. The apical 5-chamber view enabled simultaneous registration of the inflow pattern through aortic and mitral valves and isovolumic diastolic time calculation. Tissue Doppler imaging was performed in the apical views to acquire mitral annular velocity. The sample volume was positioned within 1 cm of the septal insertion sites of the mitral leaflets and adjusted as necessary (usually 5–10 mm) to cover the longitudinal excursion of the mitral annulus in diastole. Additionally, mitral septal annulus early diastolic velocity (e′) was measured and the E/e′ ratio was calculated. The diagnosis of left ventricular diastolic dysfunction (LVDD) was based on the current guidelines.26 The study group only included patients with normal LVD function and LVD dysfunction stage I (impaired relaxation diastolic filling pattern, which is related to the reduced left ventricular filling in early diastole). The following values were considered abnormal: e′ <8 cm*s−1; LA >40 mm for men and >38 mm for women; E/A <0.8; early phase deceleration time >200 ms; isovolumic relaxation time ⩾100 ms; and E/e′ ratio >8.
For the assessment of GLSS, the dedicated automated function imaging protocol was used. Digital images acquired in the apical long-axis, apical 2-chamber and apical 4-chamber and loop recorded with ECG gating were analyzed. As required, high temporal resolution of >50 frames per second was obtained to enable acoustic myocardial marker tracing. The detection of the tracked area was carried out semiautomatically after selection of two basal points at the level of mitral annulus and the third point in the apex, with manual correction when needed. In each of the apical views, LV walls were divided into six segments. The value of strain and quality of tracing were then assessed for each LV segment. The mean longitudinal peak systolic strain value was calculated for each of the three views. The value of the GLSS was calculated as the arithmetical mean of these values.
Impedance cardiography
All ICG measurements were performed using a Niccomo device (Medis, Ilmenau, Germany) after 10 min of rest in a supine position. The data were recorded during a 10-min assessment and exported to the dedicated software (Niccomo Software, Medis). The final analysis included mean values of hemodynamic parameters characterizing (1) cardiac performance: stroke volume (SV) and its index to body surface area (SI), cardiac output (CO) and its index (CI), acceleration index (ACI), velocity index (VI) and Heather index (HI); (2) afterload: systemic vascular resistance (SVR) and its index, and total arterial compliance (TAC); and (3) preload: thoracic fluid content (TFC) and its index (TFCI). The calculation formulas were presented in our previous publication.27
Applanation tonometry
The assessments of the central BP (CBP) and augmentation index (AI) were performed noninvasively using the SphygmoCor system (AtCor Medical, Sydney, NSW, Australia). Radial artery pressure waveforms were recorded at the left wrist using AT with a high-fidelity micromanometer (Millar Instruments, Houston, TX, USA). The arterial pulse waves were processed with SphygmoCor software (version 9.0; AtCor Medical Inc. Pty Ltd, Sydney, Australia), and the corresponding aortic pressure waveform was generated from the radial artery waveform using a validated transfer function with the identification of an inflection point resulting from the wave reflection and the incisura resulting from the aortic valve closure.28 As a result, central systolic BP (CSBP), central diastolic BP (CDBP) and central pulse pressure (CPP) were derived. Augmentation pressure (AP) was calculated by the maximum systolic pressure minus the pressure at the inflection point and augmentation index (AI as AI=AP × 100/CPP). Only high-quality recordings (quality index >80%) were included in the analysis. The measurements were performed in the supine position just after examination by ICG. The radial pulse and transferred aortic blood pulse were calibrated against the last measurement of brachial SBP and DBP by the oscillometric module of the Niccomo device.
Statistical analysis
The statistical analysis was performed using Statistica 7.0 software (StatSoft Inc.,Tulsa, OK, USA). The distribution and normality of the data were assessed by visual inspection and the Kolmogoro–Smirnov test. Continuous variables were presented as the means±s.d., and categorical variables were presented as absolute and relative frequencies (percentages). To analyze the differences between subgroups of patients with and without AO, Student’s t-test was used for data with normal distribution, and the Mann–Whitney U-test was used if the data were not normally distributed. For categorical variables, the χ2 test and the Fisher's exact test were used. The associations between clinical features, indices of the cardiovascular function and structure with WC were analyzed with Pearson’s correlation coefficients. A P-value <0.05 indicates statistical significance.
Results
Basic characteristics
We identified AO in more than half of the patients (n=79, 54.9%, Table 1). AO was associated with slightly higher office BP, but age, HR, GFR and gender distribution were similar between patients with and without AO (Table 2).
Echocardiographic assessment
AO correlated with larger left chambers and aortic dimensions (LVEDD, LA, AoA), lower absolute value of GLSS and higher prevalence of LVDD (Table 2). No significant differences for left ventricular ejection fraction, LVMI and the prevalence of LVH were observed.
ICG and AT assessment
The most prominent differences in ICG assessment were observed for indices of LV performance and thoracic fluid load. Obese subjects presented with lower values of LV contractility (VI, ACI, HI) but normal SI and CI (Table 3). Moreover, obesity was associated with lower TFC, especially if indexed to the body surface area. No significant differences for afterload parameters (TAC, systemic vascular resistance index, CPP and AI) were observed. However, the consistent trend toward higher central arterial stiffness (lower TAC, higher CPP and AI) seems to be clinically relevant.
Correlation analysis
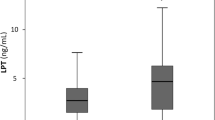
In the analysis of the association between AO and other analyzed variables, the most prominent correlations were noted for WC, LVEDD, LA, AoA, GLSS, E/A, VI, ACI, HI and TFCI (Tables 2 and 3; Figure 1). Statistically borderline relationships, not revealed in intergroup comparison, were noted for WC with SBP, DBP, LVMI and RVEDD.

The correlation plots of waist circumference with: left heart dimensions (a, left ventricular end-diastolic diameter (LVEDD); b, left atrium diameter (LA)); indices of the left ventricular performance (c, global longitudinal systolic strain (GLSS); e, velocity index (VI); f, Heather index (HI)) and mitral inflow pattern (d, mitral inflow early and late phase ratio (E/A)).
Discussion
The results of our study confirmed the relationship between AO and cardiovascular function. The use of complementary diagnostic methods revealed that the excessive accumulation of abdominal fat even in young and middle-aged hypertensives is related to complex hemodynamic alterations. Our results confirmed previous findings in this area and revealed new insights into the pathogenesis of obese-related AH. We showed that asymptomatic impairment of cardiac performance could be the earliest detectable clinical feature of the impaired cardiovascular function related to AO. Both LV diastolic and systolic disturbances were more prominent than alterations in volume load and afterload. Our results substantiate aggressive diagnostic and therapeutic strategies in obese hypertensive patients and indicate the use of easy diagnostic tools, which are promising in preliminary evaluation and the monitoring of the intervention.
AO and left ventricular diastolic function
Our results confirmed a significant association between AO and the impaired LV diastolic function. We observed that the presence of AO favored LVDD, which was exhibited in the impaired LA–LV interaction (lower E/A), prolonged LV relaxation (longer isovolumic relaxation time) and increased LV filling pressure (lower e′ and higher E/e′). The accelerated impairment of LVDD in obese hypertensives was reported by Miyoshi et al.29 These findings also agree with several previous observations30, 31 reporting that an expanded blood volume, LV dilation30 and LVH30, 31 may contribute to LVDD. However, in our study, the prevalence of LVH was very low and there was no case of LV enlargement. In this context, the other factors should be considered as responsible for early-stage LVDD. Parrinello et al.32 illustrate the crucial role of metabolic and neurohormonal abnormalities that are especially prominent in AO. Left ventricular stiffening and hypertrophy are probably two parallel processes induced by one or more of the following: activated sympathetic nervous system, renin–angiotensin–aldosterone system, oxidative stress, insulin resistance, hyperleptinemia, myocardial fibrosis and intramyocellular triglyceride deposition.11, 31
AO and left ventricular systolic function
The mean GLSS (−17.2%) observed in obese hypertensives was higher (lower absolute value) compared with that in the normotensives (−21.1%,17 −20.2%18). The harmful effect of obesity on LV contractility was previously reported. Wong et al.30 found significant differences in myocardial contractility between obese and lean patients. They also showed that the degree of LV dysfunction correlates with body mass index. Obesity in diabetic patients was related to the impaired LV systolic function and deformation in three-dimensional speckle tracking echocardiography. Moreover, the coexistence of overall obesity and AO resulted in the most impaired myocardial systolic performance.33 Obert et al.34 examined asymptomatic, severely obese adolescents and observed significantly altered longitudinal systolic and early diastolic strain rate in the presence of preserved circumferential deformation. This particular sensitivity of GLSS is associated with specificity of myocardial fibers, which are responsible for longitudinal deformation. The fibers are placed subendocardially and therefore are more exposed to ischemia, fibrosis and impaired microcirculation.11
The coexistence of lower GLSS with a higher prevalence of LVDD in obese patients suggests a strong association of these disturbances. These interrelations were previously reported in patients with AH.35, 36 Galderisi et al.17 observed that GLSS was an independent contributor to E/e′ ratio (P<0.0001) separate from age, heart rate, meridional end-systolic stress, LV mass index and left atrial volume index. Additionally, Ballo et al.37 proved that GLSS was superior to circumferential strain in predicting LVDD and increased LV diastolic pressure (E/e′ ⩾13).
The novelty of our approach lies in the hemodynamic assessment of LV performance by ICG and AT. Similar to previous reports,8, 38 we observed higher SV and CO in obese subjects, but after normalization to body dimensions, the values of SI and CI were comparable between obese and non-obese subjects. The significantly depressed parameters, which characterize LV performance as a blood pump (ACI, VI, HI), were found to be useful markers of the obesity-related hemodynamic alterations. The impaired dynamics of LV outflow may reflect reduced LV contractility as with impaired capacity of the aorta to counterbalance forward (blood ejection) and backward (afterload) load forces. These findings provide new insight into the pathogenesis of the obese-related exercise intolerance. Impaired LV contractility and blood outflow may result in the insufficiency of circulatory supply in the case of increased body demand during exercise.
AO and left ventricular load
The differences between hemodynamic indices of afterload have not reached statistical significance in our analysis, but the consistency of the evaluation by two independent methods (ICG and AT) suggests clinically credible proof of increased arterial stiffness in the subgroup with AO. Lower TAC, higher CPP and AI indicate functional stiffening of the aorta, with limited impact of peripheral resistance (systemic vascular resistance index).39 We confirmed that hemodynamic alterations overlapped in obese hypertensives. The possibility to assess afterload may be clinically important in view of the discrepancies between studies reporting arterial status in obesity and AH.3, 5, 6, 13, 40 These apparently confusing observations reflect the interplay between hypertension and obesity. Healthy, normotensive, obese patients present with low peripheral vascular resistance,3, 6, 40 but the superposition of even borderline AH moderates this potentially positive effect.5, 6 Kangas et al.13 observed that arterial stiffness (pulse wave velocity, aortic pulse pressure and AP) is more pronounced in patients with metabolic syndrome, particularly with hypertension. In a prospective observation, Safar et al.4 showed that metabolic disorders increase the risk of the accelerated vascular aging. Rizzoni et al.7 explain that both obesity and AH influence artery structure resistance but with different mechanisms; namely, metabolic disturbances promote vascular smooth muscle growth (hypertrophic remodeling), whereas AH has an increased media-to-lumen ratio (eutrophic remodeling). The obesity-related endothelial dysfunction is another potential mechanism of the impaired vasodilation.9 This imbalance between high output and vasoconstriction may contribute significantly to the increased BP. The observations of Fujii et al.41 emphasize the role of inflammation in hemodynamic disturbances related to AO. The authors followed 705 normotensive subjects and reported increased risk of new-onset hypertension related to copresence of AO and a high level of high-sensitivity C-reactive protein. Kim et al.42 demonstrated that AO is associated with early metabolic disturbances and renal impairment showing a significant correlation between visceral adipose tissue (evaluated by computed tomography), insulin resistance and prevalence of microalbuminuria.
Relatively low TFC/TFCI, as we have observed in the AO subgroup, is quite difficult to interpret. One might expect an increased TFC/TFCI as a reflection of obesity-related fluid retention. However, in our opinion, TFC should be regarded as an indicator of the local fluid content but not the overall body fluid balance. Low TFC may suggest that young and middle-aged obese hypertensives, even with slightly impaired LV performance, do not present pulmonary congestion. Presumably, the LV is efficient enough to cope with the volume load at this preliminary stage of dysfunction. Another issue is that AO may contribute to venous stasis in lower body compartments by mechanical compression of the abdominal veins,43 which may partly explain the relatively low accumulation of fluid in the thorax (TFC/TFCI). However, in our opinion, previous results have not provided enough evidence to consider TFC/TFCI as a good marker of preload in AO. Whole-body impedance methods could provide additional value in the assessment of fluid balance and distribution in obese patients.
AO and heart structure
We observed that obese patients were associated with larger dimensions of the left heart chambers. These anatomic differences were previously reported2, 5, 12, 29, 38 and will not be further discussed. We would like simply to comment that higher LVDD, LA and AoA should be interpreted not only as a reflection of overall body dimensions but also of altered LA–LV interaction and central hemodynamics. Left ventricular mass index was slightly higher in hypertensives with AO and correlated with WC. The difference in the prevalence of LVH was not statistically significant but agreed with clinical trends of higher occurrence of myocardial hypertrophy in obese subjects.2, 5, 6, 38
Clinical implications
The combination of AO and AH is a double burden to the heart. We identified LV dysfunction as the prominent marker of the impaired hemodynamics in obese hypertensives. We show that echocardiographic assessment may be supported by noninvasive diagnostic tools (ICG and AT) and that it may be easily used in everyday practice. These methods revealed the complex interplay between obesity-related (volume load) and hypertension-related (arterial stiffness) hemodynamic alterations, which influence LV performance. The identification of individual hemodynamic profiles may support personalized pharmacotherapy and provide an objective evaluation of the response to the therapeutic intervention. Such an approach may result in better treatment outcomes, including reverse myocardial remodeling and preserved cardiac function.
Limitations
We are aware that the small sample size is a limitation of the study. The use of noninvasive techniques is also biased by non-direct hemodynamic measurements that may be altered by the patient’s temporary state (BP, heart rate, preload and afterload). However, alternative techniques are either invasive or more expensive and cannot be widely used. Another limitation is that we did not perform analyses of echocardiographic radial and circumferential deformation. We also did not exclude asymptomatic ischemic heart artery disease (i.e., by performing an exercise test and/or coronarography). However, no signs or symptoms suggesting cardiac ischemia, such as LV wall motion abnormalities, electrocardiogram findings, chest pain and/or dyspnea, were noted. Previous hypotensive treatment should also be considered as a potential limitation, but it concerned <20% of subjects. Moreover, our study comprised mostly young and middle-aged hypertensives and our conclusions should not be extrapolated to the general population. However, the strength of these results is the population specificity for AH and lack of potential bias related to additional cardiovascular alterations.
Conclusions
The impact of AH and AO on cardiovascular hemodynamics overlaps and, at the early stage, is exhibited in impaired cardiac performance. The asymptomatic depression of the left ventricular diastolic and systolic function seems to be the earliest clinical feature of impaired ventricular–vascular interactions. The assessment of the individual hemodynamic profile with the use of modern noninvasive diagnostic methods should be considered in personalized therapy that aims at the prevention of adverse cardiovascular events.
References
Mancia G, Fagard R, Narkiewicz K, Redón J, Zanchetti A, Böhm M, Christiaens T, Cifkova R, De Backer G, Dominiczak A, Galderisi M, Grobbee DE, Jaarsma T, Kirchhof P, Kjeldsen SE, Laurent S, Manolis AJ, Nilsson PM, Ruilope LM, Schmieder RE, Sirnes PA, Sleight P, Viigimaa M, Waeber B, Zannad F,, Task Force Members. 2013 ESH/ESC Guidelines for the management of arterial hypertension: the Task Force for the management of arterial hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). J Hypertens 2013; 31: 1281–1357.
Chinali M, de Simone G, Roman MJ, Lee ET, Best LG, Howard BV, Devereux RB . Impact of obesity on cardiac geometry and function in a population of adolescents: the Strong Heart Study. J Am Coll Cardiol 2006; 47: 2267–2273.
Morse SA, Bravo PE, Morse MC, Reisin E . The heart in obesity-hypertension. Expert Rev Cardiovasc Ther 2005; 3: 647–658.
Safar ME, Thomas F, Blacher J, Nzietchueng R, Bureau JM, Pannier B, Benetos A . Metabolic syndrome and age-related progression of aortic stiffness. J Am Coll Cardiol 2006; 47: 72–75.
Messerli FH, Christie B, DeCarvalho JG, Aristimuno GG, Suarez DH, Dreslinski GR, Frohlich ED . Obesity and essential hypertension. Hemodynamics, intravascular volume, sodium excretion, and plasma renin activity. Arch Intern Med 1981; 14: 81–85.
Weidmann P, de Courten M, Boehlen L, Shaw S . The pathogenesis of hypertension in obese subjects. Drugs 1993; 46 (Suppl 2): 197–209.
Rizzoni D, De Ciuceis C, Porteri E, Semeraro F, Rosei EA . Structural alterations in small resistance arteries in obesity. Basic Clin Pharmacol Toxicol 2012; 110: 56–62.
de Simone G, Devereux RB, Kizer JR, Chinali M, Bella JN, Oberman A, Kitzman DW, Hopkins PN, Rao DC, Arnett DK . Body composition and fat distribution influence systemic hemodynamics in the absence of obesity: the HyperGEN Study. Am J Clin Nutr 2005; 81: 757–761.
Bagi Z . Mechanisms of coronary microvascular adaptation to obesity. Am J Physiol Regul Integr Comp Physiol 2009; 297: R556–R567.
Zoccali C, Postorino M, Marino C, Pizzini P, Cutrupi S, Tripepi G,, CREDIT Working Group. Waist circumference modifies the relationship between the adipose tissue cytokines leptin and adiponectin and all-cause and cardiovascular mortality in haemodialysis patients. J Intern Med 2011; 269: 172–181.
Davy KP, Hall JE . Obesity and hypertension: two epidemics or one? Am J Physiol Regul Integr Comp Physiol 2004; 286: R803–R813.
Koch R, Sharma AM . Obesity and cardiovascular hemodynamic function. Curr Hypertens Rep 1999; 1: 127–130.
Kangas P, Tikkakoski AJ, Tahvanainen AM, Leskinen MH, Viitala JM, Kähönen M, Kööbi T, Niemelä OJ, Mustonen JT, Pörsti IH . Metabolic syndrome may be associated with increased arterial stiffness even in the absence of hypertension: a study in 84 cases and 82 controls. Metabolism 2013; 62: 1114–1122.
Ostchega Y, Hughes JP, Terry A, Fakhouri TH, Miller I . Abdominal obesity, body mass index, and hypertension in US adults: NHANES 2007–2010. Am J Hypertens 2012; 25: 1271–1278.
Chuang SY, Chou P, Hsu PF, Cheng HM, Tsai ST, Lin IF, Chen CH . Presence and progression of abdominal obesity are predictors of future high blood pressure and hypertension. Am J Hypertens 2006; 19: 788–795.
Pavlopoulos H, Grapsa J, Stefanadi E, Philippou E, Dawson D, Nihoyannopoulos P . Is it only diastolic dysfunction? Segmental relaxation patterns and longitudinal systolic deformation in systemic hypertension. Eur J Echocardiogr 2008; 9: 741–747.
Galderisi M, Lomoriello VS, Santoro A, Esposito R, Olibet M, Raia R, Di Minno MN, Guerra G, Mele D, Lombardi G . Differences of myocardial systolic deformation and correlates of diastolic function in competitive rowers and young hypertensives: a speckle-tracking echocardiography study. J Am Soc Echocardiogr 2010; 23: 1190–1198.
Kraigher-Krainer E, Shah AM, Gupta DK, Santos A, Claggett B, Pieske B, Zile MR, Voors AA, Lefkowitz MP, Packer M, McMurray JJ, Solomon SD,, PARAMOUNT Investigators. Impaired systolic function by strain imaging in heart failure with preserved ejection fraction. J Am Coll Cardiol 2014; 63: 447–456.
Kalam K, Otahal P, Marwick TH . Prognostic implications of global LV dysfunction: a systematic review and meta-analysis of global longitudinal strain and ejection fraction. Heart 2014; 100: 1673–1680.
Ersbøll M, Andersen MJ, Valeur N, Mogensen UM, Fahkri Y, Thune JJ, Møller JE, Hassager C, Søgaard P, Køber L . Early diastolic strain rate in relation to systolic and diastolic function and prognosis in acute myocardial infarction: a two-dimensional speckle-tracking study. Eur Heart J 2014; 35: 648–656.
Krzesiński P, Gielerak G, Kowal J . Impedance cardiography—a modern tool for monitoring therapy of cardiovascular diseases. Kardiol Pol 2009; 67: 65–71.
Canepa M, Alghatrif M, Strait JB, Cheng HM, Chuang SY, Chen CH, Brunelli C, Ferrucci L, Lakatta EG . Early contribution of arterial wave reflection to left ventricular relaxation abnormalities in a community-dwelling population of normotensive and untreated hypertensive men and women. J Hum Hypertens 2014; 28: 85–91.
Krzesiński P, Uziębło-Życzkowska B, Gielerak G, Stańczyk A, Kurpaska M, Piotrowicz K . Global longitudinal two-dimensional systolic strain is associated with hemodynamic alterations in arterial hypertension. J Am Soc Hypertens 2015; 9: 680–689.
Krzesiński P, Stańczyk A, Gielerak G, Piotrowicz K . The hemodynamic patterns in hypertensive men and women of different age. J Hum Hypertens (e-pub ahead of print 2 Jul 2015; doi:10.1038/jhh.2015.63).
Alberti KG, Zimmet P, Shaw J,, IDF Epidemiology Task Force Consensus Group. The metabolic syndrome—a new worldwide definition. Lancet 2005; 366: 1059–1062.
Nagueh SF, Appleton CP, Gillebert TC, Marino PN, Oh JK, Smiseth OA, Waggoner AD, Flachskampf FA, Pellikka PA, Evangelisa A . Recommendations for the evaluation of left ventricular diastolic function by echocardiography. Eur J Echocardiogr 2009; 10: 165–193.
Krzesiński P, Stańczyk A, Gielerak G, Uziębło-Życzkowska B, Kurpaska M, Piotrowicz K, Skrobowski A . Sex determines cardiovascular hemodynamics in hypertension. J Hum Hypertens 2015; 29: 610–617.
Pauca AL, O’Rourke MF, Kon ND . Prospective evaluation of a method for estimating ascending aortic pressure from the radial artery pressure waveform. Hypertension 2001; 38: 932–937.
Miyoshi H, Oishi Y, Mizuguchi Y, Iuchi A, Nagase N, Ara N, Oki T . Contribution of obesity to left atrial and left ventricular dysfunction in asymptomatic patients with hypertension: a two-dimensional speckle-tracking echocardiographic study. J Am Soc Hypertens 2014; 8: 54–63.
Wong CY, O'Moore-Sullivan T, Leano R, Byrne N, Beller E, Marwick TH . Alterations of left ventricular myocardial characteristics associated with obesity. Circulation 2004; 110: 3081–3087.
Eschalier R, Rossignol P, Kearney-Schwartz A, Adamopoulos C, Karatzidou K, Fay R, Mandry D, Marie PY, Zannad F . Features of cardiac remodeling, associated with blood pressure and fibrosis biomarkers, are frequent in subjects with abdominal obesity. Hypertension 2014; 63: 740–746.
Parrinello G, Licata A, Colomba D, Di Chiara T, Argano C, Bologna P, Corrao S, Avellone G, Scaglione R, Licata G . Left ventricular filling abnormalities and obesity-associated hypertension: relationship with overproduction of circulating transforming growth factor beta1. J Hum Hypertens 2005; 19: 543–550.
Wang Q, Gao Y, Tan K, Li P . Subclinical impairment of left ventricular function in diabetic patients with or without obesity: A study based on three-dimensional speckle tracking echocardiography. Herz 2014; 40: 260–268.
Obert P, Gueugnon C, Nottin S, Vinet A, Gayrard S, Rupp T, Dumoulin G, Tordi N, Mougin F . Two-dimensional strain and twist by vector velocity imaging in adolescents with severe obesity. Obesity (Silver Spring, MD) 2012; 20: 2397–2405.
Jovin IS, Ebisu K, Liu YH, Finta LA, Oprea AD, Brandt CA, Dziura J, Wackers FJ . Left ventricular ejection fraction and left ventricular end-diastolic volume in patients with diastolic dysfunction. Congest Heart Fail 2013; 19: 130–134.
García EH, Perna ER, Farías EF, Obregón RO, Macin SM, Parras JI, Agüero MA, Moratorio DA, Pitzus AE, Tassano EA, Rodriguez L . Reduced systolic performance by tissue Doppler in patients with preserved and abnormal ejection fraction: new insights in chronic heart failure. Int J Cardiol 2006; 108: 181–188.
Ballo P, Nistri S, Cameli M, Papesso B, Dini FL, Galderisi M, Zuppiroli A, Mondillo S,, Working Group Nucleus on Echocardiography of the Italian Society of Cardiology. Association of left ventricular longitudinal and circumferential systolic dysfunction with diastolic function in hypertension: a nonlinear analysis focused on the interplay with left ventricular geometry. J Card Fail 2014; 20: 110–120.
Abel ED, Litwin SE, Sweeney G . Cardiac remodeling in obesity. Physiol Rev 2008; 88: 389–419.
Kass DA . Ventricular arterial stiffening: integrating the pathophysiology. Hypertension 2005; 46: 185–193.
Jern S, Bergbrant A, Björntorp P, Hansson L . Relation of central hemodynamics to obesity and body fat distribution. Hypertension 1992; 19: 520–527.
Fujii M, Ohnishi H, Saitoh S, Akasaka H, Miura T, Mori M . The combination of abdominal obesity and high-sensitivity C-reactive protein predicts new-onset hypertension in the general Japanese population: the Tanno-Sobetsu study. Hypertens Res 2015; 38: 426–432.
Kim H, Kim HJ, Shin N, Han M, Park H, Kim M, Kwon H, Choi SY, Heo NJ . Visceral obesity is associated with microalbuminuria in nondiabetic Asians. Hypertens Res 2014; 37: 679–684.
Willenberg T, Clemens R, Haegeli LM, Amann-Vesti B, Baumgartner I, Husmann M . The influence of abdominal pressure on lower extremity venous pressure and hemodynamics: a human in vivo model simulating the effect of abdominal obesity. Eur J Vasc Endovasc Surg 2011; 41: 849–855.
Acknowledgements
We thank the medical staff of the Department of Cardiology and Internal Diseases of Military Institute of Medicine for assistance in patient care and data collection. The study was supported by the Ministry of Science and Higher Education/Military Institute of Medicine, Warsaw, Poland (Grant No. 148/WIM).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article

Cite this article
Krzesiński, P., Stańczyk, A., Piotrowicz, K. et al. Abdominal obesity and hypertension: a double burden to the heart. Hypertens Res 39, 349–355 (2016). https://doi.org/10.1038/hr.2015.145
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/hr.2015.145
Keywords
This article is cited by
-
The characteristics of elevated blood pressure in abdominal obesity correspond to primary hypertension: a cross-sectional study
BMC Cardiovascular Disorders (2023)
-
Very low-calorie ketogenic diet (VLCKD): an antihypertensive nutritional approach
Journal of Translational Medicine (2023)
-
Percentage of free fat mass is associated with elevated blood pressure in healthy Chinese children
Hypertension Research (2019)
-
Is leptin protective against heart failure with preserved ejection fraction? A complex interrelationship among leptin, obesity, and left ventricular hypertrophy
Hypertension Research (2019)
-
Association between epicardial adipose tissue thickness and parameters of target organ damage in patients undergoing coronary angiography
Hypertension Research (2019)
