
Abstract
There are limited clinical trials examining the efficacy of antihypertensive drug combinations aimed at preventing cardiovascular events. Therefore, we designed a randomized controlled trial using amlodipine as the base drug of a multi-drug regimen, the Optimal Combination of Effective ANtihypertensives (OCEAN) Study, to determine the drug combination that is most efficacious in the prevention of cardiovascular events, such as stroke. The OCEAN Study is a collaborative study between Japan and China, enrolling 20 000 patients and following them for 3 to 4 years. A pilot study was conducted before the full-scale study to confirm the feasibility of the protocol and that the study groups and infrastructures could function properly. A total of 279 Japanese patients were enrolled from 57 participating medical institutions between June and December 2004. Two hundred and sixty-six patients (mean age: 65.9 years) were treated with amlodipine alone. One hundred and fifty-four of these patients (57.9%) did not reach the treatment targets (<140/90 mm Hg for the elderly and patients with cerebrovascular disease, <130/80 mm Hg for those with diabetes mellitus, chronic kidney disease or prior myocardial infarction) and a second agent was added. They were randomly allocated into three different treatment groups using a diuretic, a β-blocker or an angiotensin-converting enzyme inhibitor/angiotensin II receptor antagonist. The pilot study showed that the protocol was appropriate, and the inclusion of patients with slightly higher blood pressures was necessary to increase the randomization rate. It also confirmed that we organized properly functioning study groups and infrastructures.
Similar content being viewed by others


Introduction
Hypertension is the most common lifestyle-related disease and a major risk factor for cardiovascular diseases. The current guidelines for the treatment of hypertension set lower goals for optimal blood pressure (BP) than previous guidelines.1, 2, 3 The recommended BP target is <130/85 mm Hg for young and middle-aged people, <140/90 mm Hg for the elderly and patients with cerebrovascular disease, and <130/80 mm Hg for those with diabetes mellitus, chronic kidney disease or prior myocardial infarction.1 To attain these BP targets, two or more antihypertensive drugs are often necessary.4
A number of clinical trials have been conducted to compare different classes of antihypertensive drugs to determine the class that is most efficacious for the prevention of cardiovascular diseases. In these trials, a number of subjects were treated with two or more classes of drugs to attain the goal of normal blood pressure.5, 6, 7 However, clinical trials examining the efficacy of possible combinations of drugs to prevent cardiovascular events are quite limited.8, 9
Therefore, we planned a randomized controlled trial, the Optimal Combination of Effective ANtihypertensives (OCEAN) Study, to determine the drug combination that is most efficacious in the prevention of cardiovascular events, such as stroke, using amlodipine as the base drug. The OCEAN Study is a collaborative study between Japan and China, enrolling 20 000 patients and following them over a period of three to four years. A pilot study enrolled two hundred patients in Japan and was conducted prior to a full-scale study to confirm the feasibility of the protocol. It also tried to confirm that the study groups and infrastructures we organized do work indeed properly.
Rationale
Reduction of hypertensive cardiovascular complications with antihypertensive therapy has been shown to be attributed to the lowering of BP itself rather than to the characteristics of antihypertensive drugs in clinical trials and meta-analyses.10, 11 As the treatment guidelines tighten recommended target BP values, two or more antihypertensive drugs are frequently required to attain target BP.
Currently, in Japan, the frequency of prescribing calcium-channel blockers is the highest in the world; these drugs are administered to 60–70% of hypertensive patients.12 Hypertension is the most common lifestyle-related disease. However, there is an ethnic difference in the type of cardiovascular complications; whereas heart disease is more prevalent in Europe and the United States, cerebral stroke is more prevalent in Japan and China.13, 14, 15 Recently, there has been a shift toward using composite end points as a primary end point rather than single end points. This is partly because too large of a sample size was needed when a single end point was adopted. Whereas interpretation of results is clear for a single end point, interpretation of the results of a composite end point could be ambiguous depending on the results obtained, particularly when the composite end point is composed of events of different clinical significance. Therefore, in the present study, we chose a single end point, stroke, as a primary end point.
The purpose of the OCEAN Study is to test the effectiveness of the different combinations of antihypertensive agents on the incidence of stroke and other cardiovascular events in a real-world setting. As amlodipine, a calcium-channel blocker, is the most commonly used antihypertensive drug in Japan, the present study is designed to identify another drug as a possible add-on to amlodipine to produce a more efficacious therapy for the prevention of cardiovascular events.
Methods
Study design and protocol
The OCEAN Study is an investigator-initiated, prospective, randomized, open-label, parallel group trial. The study adopts the prospective randomized open-label, blinded endpoint (PROBE) design,16 in which members in the endpoint committee are blinded to drug assignments. The patients entering the study were first treated with amlodipine. If the target BP was not achieved by amlodipine monotherapy, a second agent was added. The patients were randomized to a second agent from the following list: a diuretic, a β-blocker including an αβ-blocker, an angiotensin-converting enzyme (ACE) inhibitor or an angiotensin II receptor antagonist (ARB). The target BP of this study was <140/90 mm Hg; in the case of patients who had diabetes mellitus, the target BP was <130/80 mm Hg. The patients were monitored based on a routine follow-up schedule. The outcomes of the ACE inhibitor/ARB, or the β (αβ)-blocker arms were compared against the diuretics arm.
Patient enrollment
Investigators screened and enrolled eligible outpatients who fulfilled the inclusion criteria in Table 1, aiming for a total of two hundred patients who would complete an initial pilot study. Table 2 shows the exclusion criteria for this study. It was estimated that the full-scale study would require approximately 20 000 patients to complete 3- to 4-year follow-up.
Randomization
The patients who were not achieving BP targets with amlodipine monotherapy were randomized to an add-on therapy at the time of transferring from Step 1 to Step 2. The randomization was applied according to a minimization method to ensure a balance of patient characteristics such as age, sex, diabetes and a history of stroke.17 The randomization was conducted at a data center via the University Hospital Medical Information Network (UMIN) system.
Study medication
Figure 1 shows the study design by which eligible patients were assigned to a treatment regimen at the time of enrollment. Patients who had completed the screening evaluations and fulfilled the inclusion/exclusion criteria began amlodipine at 2.5 or 5.0 mg for Step 1. Those who had been treated with amlodipine before enrollment continued amlodipine for Step 1, and antihypertensive agents other than amlodipine were stopped. The daily dosage of amlodipine should not exceed 5.0 mg. If the patients’ BP achieved the recommended target level, the appropriate dose of amlodipine was maintained and the patients were kept on monotherapy. The patients who had not achieved the target BP after treatment with amlodipine were randomized to amlodipine plus diuretics (Group I), amlodipine plus β (αβ)-blockers (Group II) or amlodipine plus ACE Inhibitor/ARB (Group III) for Step 2 at 4 to 8 weeks (Figure 1).

Study design and treatment protocols. *1: Patient's blood pressure reached the target blood pressure with amlodipine monotherapy after the end of the 16th week. *2: α1 blockers, hydralazine, clonidine, α methyldopa and reserpine were selected by investigators as add-on therapy. *3: Randomization was possible until the 16th week.
When the patients achieved target BP, they were maintained on the regimen until the completion of the study. However, patients who did not respond to the two agents prescribed in Step 2 after 4 to 8 weeks were moved to Step 3. Augmentation treatment agents for Step 3 were α1 blockers, hydralazine, clonidine, α methyldopa and reserpine. When patients did not achieve the target BP in step 3, they were moved to Step 4. In Step 4, patients were treated with amlodipine and other antihypertensive agents including those of the other arms designated in Step 2.
Blood pressure targets
The BP target is the goal recommended by international and local treatment guidelines.1, 2, 3 Systolic blood pressure (SBP) should be <140 mm Hg and diastolic blood pressure (DBP) <90 mm Hg. Patients who have diabetes, however, should have SBP <130 mm Hg and DBP <80 mm Hg. It is recommended that the investigators achieve these target blood pressure measurements by active titration and the addition of medications.
Endpoint assessment
The primary and secondary end points are summarized in Table 3, and an independent endpoint committee evaluated all events without the knowledge of the assigned treatment groups.
Patient follow-up
The patients were evaluated at periodic intervals to assess continued response to treatment and lack of treatment tolerance development, and to determine whether an end point had been reached. Visits occurred at regular intervals to reflect the standard of practice. At the time of enrollment, patient interviews were conducted to determine background information such as sex, age and medical history. At each clinic visit, body weight, resting BP and pulse rates in the sitting position were measured. Laboratory tests, including serum total cholesterol, HDL-cholesterol, triglyceride, plasma glucose, creatinine and a standard 12-lead ECG, were conducted every 6 months.
Ethics committee review and informed consent
This study was conducted in accordance with the Declaration of Helsinki, the ethical guidelines for clinical studies from the Ministry of Health, Labour, and Welfare and the protocol described in this study. This study was approved by either the ethics committee of the Public Health Research Foundation or the local ethics committees of the participating medical institutions. Written informed consent was obtained from each patient before the study.
Statistical considerations and analyses
The sample size was estimated from the examples of the following preceding clinical studies that were conducted in Japan and China: NICS-EH,18 STONE14 and the Syst-China study.15 We assumed the incidence of stroke to be between fifteen and twenty events per thousand patients per year in group I (amlodipine plus diuretics). The null hypothesis was that group I is inferior to group II (amlodipine plus β (αβ)-blockers) and group III (amlodipine plus ACE Inhibitor/ARB) by more than 25%. On the basis of this condition, 57 000–76 000 patient-years are required with an α level at 2.5 and at 90% power. Thus, the estimated sample size was 20 000 patients over the 3- to 4- year follow-up period.
Statistical analyses were performed by unpaired t-test for continuous variables and by chi-square test for dichotomous data. Statistical significance was set at P<0.05.
Study monitoring and data collection
Coordinating Center representatives or visiting clinical research coordinators communicated with the investigators to assess the progress of the study and the adherence to the protocol. The investigators maintained source documents, including laboratory reports, complete histories and physical examinations for review by the monitor. Data were collected electronically in preparation for the full-scale study, in which a large amount of data has to be processed.
Results
This pilot study was conducted to confirm that the full-scale OCEAN study would draw a valid conclusion reflecting real-world clinical practice. The registration period for the pilot study was from June to December 2004, and the registered patients were followed for 12 months.
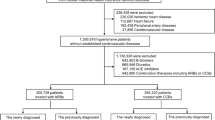
A total of 279 Japanese patients were enrolled from 57 participating medical institutions between June 2004 and December 2004. Thirteen patients were excluded because of the screening failure. Two hundred and sixty-six patients were treated with amlodipine alone, of which 154 patients (57.9%) did not reach the treatment goals (BP <140/90 mm Hg for patients without diabetes, <130/80 mm Hg for patients with diabetes) and were randomly allocated to one of the three treatment groups (Figure 2). Fifty-two patients were allocated to group I, the diuretic group. Fifty patients were allocated to group II, the β (αβ)-blocker group, and 52 patients were allocated to group III, the ACEI or ARB group.

Trial profile.
Several differences were observed in the baseline characteristics between the randomized and non-randomized groups (Table 4). SBP and serum creatinine were higher in the randomized group than in the non-randomized group (P<0.05). Prevalence of diabetes mellitus, smoking, use of ACEI/ARB, decreased eGFR and proteinuria was higher in the randomized group than in the non-randomized group (P<0.001), and the prevalence of stroke was decreased in the randomized group (P<0.001).
The three treatment groups were similar in terms of demographic characteristics, cardiovascular risk factors for stroke and diabetes, rate of current smoking and previous antihypertensive treatment. The numbers and percentages of patients in each group who had already been treated with an antihypertensive agent were 49 (94.2%) for group I, 47 (94%) for group II and 50 (96.2%) for group III. The mean BP and pulse rate of each treatment group are shown in Table 5. SBP was reduced in each treatment group in a similar way, but the amlodipine/β-blocker combined regimen tended to have caused a greater reduction of DBP and pulse rate.
Achievement rates of the target SBP either at 3 months, 6 months or 12 months after randomization were 31% for diabetics and 50% for non-diabetics in group I, 34 and 63% in group II, and 35 and 67% in group III, respectively. Achievement rates of the target DBP either at 3 months, 6 months or 12 months after randomization were 63% for diabetics and 72% for non-diabetics in group I, 81 and 84% in group II, and 68 and 94% in group III, respectively.
All events that were reported during the study were evaluated by the endpoint committee. There was a total of two confirmed cases of stroke: one in group II and one in group III. Two cases of acute myocardial infarction were confirmed in the amlodipine monotherapy group. One death was confirmed in group II. All of these events were determined based on data obtained by the endpoint committee whose members were blinded to the assigned treatment. The patients in all of the treatment groups tolerated treatment well. There were no serious adverse events reported.
Discussion
Two hundred and seventy-nine patients were enrolled in the pilot study, and thirteen patients were excluded by screening failure. Two hundred and sixty-six patients received amlodipine alone; from this group, 154 patients were randomized to either of the three treatment groups. The rest of the enrolled patients attained the target BP of <140/90 mm Hg, or the attending physicians did not randomize patients at their discretion because BPs almost reached the target level. All three groups experienced lower BP to a similar extent, and no severe adverse reactions were reported. In the full-scale study, 5000 patients are required for randomization in Japan. To randomize 5000 patients, approximately 8000 to 9000 patients must be enrolled according to the current protocol. This will be a costly burden for investigators, which may result in low feasibility.
A measurement to improve the feasibility of the study is to change the inclusion criteria. In the current protocol, before the enrollment of patients treated with amlodipine monotherapy, patient SBP should be controlled in the range of 140–159 mm Hg and/or DBP should be in the range of 90–99 mm Hg. However, in other trials, patients already on antihypertensive treatment for higher BP were included. Patients receiving efonidipine with DBP <120 mm Hg were included in the JATOS Study.19 Patients already on antihypertensive treatment with SBP <210 mm Hg and DBP <115 mm Hg were included in the VALUE Study.20 Therefore, by including patients with slightly higher BPs on monotherapy with amlodipine, the randomization rate will be increased without endangering patients or decreasing the number of patients enrolled, and the feasibility of the study would increase.
Achievement rate of the target SBP was relatively low in the diabetic subjects throughout the three treatment groups. This seemed to be due to the lower target SBP in diabetic subjects than in non-diabetic subjects. On the other hand, achievement rates of DBP were relatively high across the 3 treatment groups. This was likely due to the fact that DBP is usually low in elderly people, and many elderly subjects whose mean age was around 70 years were enrolled in the present study.
Hypertension was often complicated by diabetes, and more than 60% of enrolled patients in the present study were diabetics. As a major cardiovascular risk factor, such as diabetes mellitus or past history of stroke, was required to enroll patients, investigators seemed to have regarded patients with diabetes as appropriate and thus enrolled more patients with diabetes than those with past history of stroke.
In the present study, the PROBE design was adopted and end points were confined to hard end points alone. The primary end point was stroke, and the secondary end points were combined end point of myocardial infarction and death, etc. Angina and transient ischemic attacks were regarded as soft end points; therefore, to avoid investigator bias, these were not included either in the primary or secondary end points.
In the present study, clinical study coordinators who were sent from site management organizations were introduced. The coordinators confirmed that informed consent was obtained in writing, verified reported events by documentation, and contributed to the quality assurance of an open-label clinical trial. Even if the PROBE design was adopted, data verification by a third party, such as clinical research coordinators, was necessary to ensure the quality of the study. Electronic data capture was introduced, and we confirmed that this system can process large amounts of data for collection in the full-scale study.
In conclusion, the pilot study confirmed that the study group and infrastructures that we organized worked properly. In addition, the inclusion criteria of patients who were already on antihypertensive treatments should be modified to include patients with higher BPs. This would increase the randomization rate and decrease unnecessary enrollment without endangering patients, thus resulting in higher feasibility of the full-scale OCEAN Study.
References
Ogihara T, Kikuchi K, Matsuoka H, Fujita T, Higaki J, Horiuchi M, Imai Y, Imaizumi T, Ito S, Iwao H, Kario K, Kawano Y, Kim-Mitsuyama S, Kimura G, Matsubara H, Matsuura H, Naruse M, Saito I, Shimada K, Shimamoto K, Suzuki H, Takishita S, Tanahashi N, Tsuchihashi T, Uchiyama M, Ueda S, Ueshima H, Umemura S, Ishimitsu T, Rakugi H, on behalf of the Japanese Society of Hypertension Committee for Guidelines for the Management of Hypertension. The Japanese Society of Hypertension Guidelines for the Management of Hypertension (JSH 2009). Hypertens Res 2009; 32: 3–107.
Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA, Izzo Jr JL, Jones DW, Materson BJ, Oparil S, Wright Jr JT, Roccella EJ, The National High Blood Pressure Education Program Coordinating Committee. Seventh report of the joint national committee on prevention, detection, evaluation, and treatment of high blood pressure. Hypertension 2003; 42: 1206–1252.
World Health Organization, International Society of Hypertension Writing Group;. 2003 World Health Organization (WHO)/International Society of Hypertension (ISH) statement on management of hypertension. J Hypertens 2003; 21: 1983–1992.
Kamijima Y, Ooba N, Yagame M, Samizo K, Shimodozono Y, Kageyama S, Horiguchi S, Nagai R, Kusunoki T, Kubota K . Hypertension management in diabetic patients: prescribing trends from 1999–2005 in three Japanese university hospitals. Pharmacoepidemiol Drug Saf 2008; 17: 904–911.
Dahlöf B, Devereux RB, Kjeldsen SE, Julius S, Beevers G, de Faire U, Fyhrquist F, Ibsen H, Kristiansson K, Lederballe-Pedersen O, Lindholm LH, Nieminen MS, Omvik P, Oparil S, Wedel H, LIFE Study Group. Cardiovascular morbidity and mortality in the Losartan Intervention For Endpoint reduction in hypertension study (LIFE): a randomised trial against atenolol. Lancet 2002; 359: 995–1003.
Julius S, Kjeldsen SE, Weber M, Brunner HR, Ekman S, Hansson L, Hua T, Laragh J, McInnes GT, Mitchell L, Plat F, Schork A, Smith B, Zanchetti A, VALUE trial group. Outcomes in hypertensive patients at high cardiovascular risk treated with regimens based on valsartan or amlodipine: the VALUE randomised trial. Lancet 2004; 363: 2022–2031.
Dahlöf B, Sever PS, Poulter NR, Wedel H, Beevers DG, Caulfield M, Collins R, Kjeldsen SE, Kristinsson A, McInnes GT, Mehlsen J, Nieminen M, O’Brien E, Ostergren J, ASCOT Investigators. Prevention of cardiovascular events with an antihypertensive regimen of amlodipine adding perindopril as required versus atenolol adding bendroflumethiazide as required, in the Anglo-Scandinavian Cardiac Outcomes Trial-Blood Pressure Lowering Arm (ASCOT-BPLA): a multicentre randomised controlled trial. Lancet 2005; 366: 895–906.
Jamerson K, Weber MA, Bakris GL, Dahlöf B, Pitt B, Shi V, Hester A, Gupte J, Gatlin M, Velazquez EJ, for the Accomplish Trial Investigators. Benazepril plus amlodipine or hydrochlorothiazide for hypertension in high-risk patients. N Engl J Med 2008; 359: 2417–2428.
Bakris GL, Toto RD, McCullough PA, Rocha R, Purkayastha D, Davis P, On behalf of the GUARD (Gauging Albuminuria Reduction With Lotrel in Diabetic Patients With Hypertension) Study Investigators. Effects of different ACE inhibitor combinations on albuminuria: results of the GUARD study. Kidney Int 2008; 73: 1303–1309.
The ALLHAT Officers and Coordinators for the ALLHAT Collaborative Research Group.. Major outcomes in high-risk hypertensive patients randomized to angiotensin-converting enzyme inhibitor or calcium channel blocker vs diuretic. The Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT). JAMA 2002; 288: 2981–2997.
Staessen JA, Wang J-G, Thijs L . Cardiovascular protection and blood pressure reduction: a meta-analysis. Lancet 2001; 358: 1305–1315.
Saito I, Kawabe H, Tsujioka M, Hirose H, Shibata H . Trends in pharmacologic management of hypertension in Japan one year after the publication of the JSH 2000 guidelines. Hypertens Res 2002; 25: 175–178.
Kubo M, Kiyohara Y, Kato I, Tanizaki Y, Arima H, Tanaka K, Nakamura H, Okubo K, Iida M . Trends in the incidence, mortality, and survival rate of cardiovascular disease in a Japanese community. The Hisayama Study. Stroke 2003; 34: 2349–2354.
Gong L, Zhang W, Zhu Y, Zhu J, collaborating centres in the Shanghai area, Kong D, Page V, Ghadirian P, LeLorier J, Hamet P . Shanghai trial of nifedipine in the elderly (STONE). J Hypertens 1996; 14: 1237–1245.
Liu L, Wang JG, Gong L, Liu G, Staessen JA, for the Systolic Hypertension in China (Syst-China) Collaborative Group. Comparison of active treatment and placebo in older Chinese patients with isolated systolic hypertension. J Hypertens 1998; 16: 1823–1829.
Hansson L, Hedner T, Dahlöf B, Prospective randomized open blinded end-point (PROBE) study. A novel design for intervention trials. Prospective Randomized Open Blinded End-Point. Blood Press 1992; 1: 113–119.
Taves DR . Minimization, a new method of assigning patients to treatment and control groups. Clin Pharmacol Ther 1974; 15: 443–453.
Kuwajima I, Kuramoto K, Ogihara T, Iimura O, Abe K, Saruta T, Ishii M, Hiwada K, Fujishima M, Fukiyama K, National Intervention Cooperative Study in Elderly Hypertensives (NICS-EH) Study Group. Tolerability and safety of a calcium channel blocker in comparison with a diuretic in the treatment of elderly patients with hypertension: secondary analysis of the NICS-EH. Hypertens Res 2001; 24: 475–480.
JATOS Study Group:. The Japanese Trial to Assess Optimal Systolic Blood Pressure in Elderly Hypertensive Patients (JATOS): protocol, patient characteristics, and blood pressure during the first 12 months. Hypertens Res 2005; 28: 513–520.
Mann J, Julius S, for the VALUE Trial Group: The Valsartan Antihypertensive Long-term Use Evaluation (VALUE) Trial of Cardiovascular Events in Hypertension. Rationale and design. Blood Press 1998; 7: 176–183.
Acknowledgements
This study was funded by the Comprehensive Support Project for Clinical Research of Lifestyle-Related Disease (CSP-LD) from the Public Health Research Foundation.
Author information
Authors and Affiliations
Consortia
Corresponding author
Ethics declarations
Competing interests
SK has served as a consultant and received fees from Astellas, Mochida and Daiichi-Sankyo. YO has served as a monitoring committee member in a post-marketing trial sponsored by Pfizer. IS has received lecture fees from Daiichi-Sankyo, Pfizer, Novartis, MSD, Astellas and Kyowa-Kirin. The other authors declare no conflict of interest.
Appendix
Appendix
OCEAN study organization
Steering Committee: Shigeru Kageyama (Chair, The Jikei Univ.), Shinichiro Ueda (Vice-Chair, Ryukyu Univ.), Kouichi Mochizuki (Vice Chair, Mochizuki Clinic), Masaaki Miyakawa (Miyakawa Clinic), Masahiro Sugawara (Sugawara Clinic), Michio Nakayama (Nakayama Clinic),
Advisors
Takao Saruta (Keio Univ.), Toshiro Fujita (Tokyo Univ.)
Protocol committee
Shigeru Kageyama (Chair, The Jikei Univ.), Shinichiro Ueda (Vice-Chair, Ryukyu Univ.), Kouichi Mochizuki (Vice Chair, Mochizuki Clinic), Masaaki Miyakawa(Miyakawa Clinic), Masahiro Sugawara (Sugawara Clinic), Michio Nakayama (Nakayama Clinic), Yasuo Ohashi (Tokyo Univ.), Toshio Kushiro (Nihon Univ.), Yoshio Uehara (Tokyo Univ.)
Trial promotion committee
Masaaki Miyakawa(Miyakawa Clinic), Ikuro Matsuba (Matsuba Clinic), Masanori Tateishi (Takeishi Clinic), Ken-ichi Ishibashi (Ishibashi Clinic)
Endpoint committee
Ikuo Saito (Chair, Keio Univ.), Makoto Takagi (Saiseikai Hospital), Yasutomo Okajima (Kyorin Univ.), Ikuo Taniguchi (The Jikei Univ.), Satoshi Kuriyama (Saiseikai Hospital), Hideaki Kurata (Jikei Univ.)
Independent data monitoring and safety committee
Hiroshi Watanabe (Hamamatsu Univ,), Akihiro Onishi (Jikei Univ.), Tsutomu Yamasaki (Tokyo Univ.)
Statistical analysis
Yasuo Ohashi (Tokyo Univ.)
OCEAN investigators
Koichi Hirao (HEC Science Clinic), Seiichi Ichikawa (Shonai Amarume Hospital), Kenichi Ishibashi (Ishibashi Clinic), Kazuo Aihara (Tokyu Hospital), Masanori Takeishi (Takeishi Clinic), Tohru Takagishi (Tsurui Clinic), Takeshi Kurihara (Kurihara Clinic), Hirotaka Masabayashi (Masabayashi Clinic), Masahisa Oori (Oori Clinic), Toshiyuki Mizuo (Mizuo Clinic), Koichi Mochizuki (Mochizuki Clinic), Kageki Ito (Ito Internal and Pediatric Clinic), Takehiko Mikawa (Mikawa Clinic), Kimiyuki Tokuyasu (Tokuyasu Clinic), Kazuo Suzuki (Suzuki Clinic), Kazunori Soejima (Suwa Central Hospital), Kunihiko Furuya (Furuya Clinic), Hiroshi Shimomura (Musashino Clinic), Masahiro Sugawara (Sugawara Clinic), Kiyoshi Kamisato (Kamisato Medical Clinic), Keiko Arai (Iiyama Clinic), Takashi Iizuka (Asahi Medical Clinic), Kazuo Sato (Sato Clinic), Hitomi Natomi (Tokyo Life Clinic), Yoshiro Yamashita (Minano Hospital), Tsuguyoshi Asano (Asano Kanamachi Clinic), Munechika Noguchi (Shinagawa East One Medical Clinic), Akiharu Ohkuma (Ohkuma Medical Clinic), Fumitoshi Omura (Koenji Clinic), Sachiko Yoshida (Ayase Clinic), Yoshihisa Abo (Kita Aoyama D Clinic), Mikio Fujioka (Fujioka Clinic), Takehisa Nojima (Kobe Tokushukai Hospital), Haruki Ito (The Cardiovascular Institute Hospital), Kazuko Takada (Shibuya Mark City Takada Clinic), Tomonori Tamura (Sannou Medical Clinic), Shin Kaneda (Kaneda Clinic), Masaaki Miyakawa (Miyakawa Medical & Pediatric Clinic), Hideki Nozaki (Nozaki Clinic), Hitoshi Hirano (Hirano Clinic), Masanari Omata (Oimachi Orthopedic & Surgery Clinic), Naoyuki Kobayashi (Sobudai Nieren Clinic), Takehiko Mizuno (Seijo Mizuno Clinic), Masamichi Niizuma (Niizuma Clinic), Akio Iino (Numata Clinic), Kazuhisa Okamoto (Shinozaki Ekimae Clinic), Hideki Sato (Sato Periatric & Medical Clinic), Issei Koga (Koga Clinic), Makoto Kato (Keiwa Clinic), Yasushi Ogihara (Ogihara Clinic), Akiyoshi Yamamura (Iguchi Hospital), Yuuki Hayashi (Yuuki Clinic), Haruaki Yamamoto (Yamamoto Clinic), Yoshinori Takahashi (Plaza 30F Clinic), Shigetaka Takamizawa (Takamizawa Clinic), Katsuhiko Motokawa (Shinonome Medical Clinic), Emiko Osuga (Kugayama Hospital).
Rights and permissions
About this article
Cite this article
Kageyama, S., Ueda, S., Mochizuki, K. et al. Optimal Combination of Effective ANtihypertensives (OCEAN) study: a prospective, randomized, open-label, blinded endpoint trial—rationale, design and results of a pilot study in Japan. Hypertens Res 35, 221–227 (2012). https://doi.org/10.1038/hr.2011.178
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/hr.2011.178
