
Abstract
Purpose
To report the 7-year incidence of uncorrected refractive error in a metropolitan Chinese elderly population.
Methods
The Shihpai Eye Study 2006 included 460/824 (55.8%) subjects (age range 72–94 years old) of 1361 participants in the 1999 baseline survey for a follow-up eye examination. Visual acuity was assessed using a Snellen chart, uncorrected refractive error was defined as presenting visual acuity (naked eye if without spectacles and with distance spectacles if worn) in the better eye of <6/12 that improved to no impairment (≥6/12) after refractive correction.
Results
The 7-year incidence of uncorrected refractive error was 10.5% (95% confidence interval (CI): 7.6–13.4%). 92.7% of participants with uncorrection and 77.8% with undercorrection were able to improve at least two lines of visual acuity by refractive correction. In multivariate analysis controlling for covariates, uncorrected refractive error was significantly related to myopia (relative risk (RR): 3.15; 95% CI: 1.31–7.58) and living alone (RR: 2.94; 95% CI 1.14–7.53), whereas distance spectacles worn during examination was protective (RR: 0.35; 95% CI: 0.14–0.88).
Conclusion
Our study indicated that the incidence of uncorrected refractive error was high (10.5%) in this elderly Chinese population. Living alone and myopia are predisposing factors, whereas wearing distance spectacles at examination is protective.
Similar content being viewed by others

Introduction
The prevalence of correctable visual impairment is known to increase with age1 and has become a public health concern. Less than 1% of people aged 40–49 years have visual impairment due to uncorrected refractive error, but this percentage increases to >13% among those aged 80 years and older.1 The World Health Organization estimated that uncorrected refractive error accounts for 153 million cases of visual impairment globally, thus making it the major cause of mild to moderate levels of visual impairment worldwide.2 Uncorrected refractive error has been targeted as one of the priorities of the VISION 2020: The Right to Sight program. Visual impairment limits people’s ability to perform daily tasks3, 4 and affects their quality of life.5, 6, 7 Whereas most population-based studies have emphasized the importance of noncorrectable visual impairment, uncorrected refractive error has also been shown to affect the elderly, though to a lesser extent.2, 4, 5, 6, 7
Many cross-sectional studies have highlighted that the vision of a significant proportion of the elderly can be improved by wearing eyeglasses or changing the patient’s existing glasses.1, 8, 9, 10, 11, 12, 13 However, few longitudinal studies11, 14, 15 have assessed the incidence of uncorrected refractive error, and such studies have been primarily limited to the Blue Mountains Eye Study11, 14 and the Melbourne Visual Impairment Project.15 These two studies concluded that even after people have been informed of the potential for refractive improvement, correctable visual impairment may still persist over time.14
Currently, there is no longitudinal information about uncorrected refractive error in the Asian population. The purpose of the present study was to investigate the incidence of uncorrected refractive error in a metropolitan Chinese elderly cohort and the risk factors for this condition with a 7-year follow-up.
Materials and methods
The Shihpai Eye Study13, 16 was a community-based, cross-sectional survey of vision and eye diseases among noninstitutionalized subjects 65 years of age and older in Shihpai, Taipei, Taiwan. Residents 65 years of age and older were identified using the household registration system. This system officially registers personal information, such as the date of birth, sex, home address and family members and relations. According to the official household registration in 1999, the total number of residents aged 65 years and older in Shihpai was 4750; of them, 3746 persons were eligible, and 2045 were randomly selected to be invited to participate in the study. Of the 2045 subjects, 1361 (66.6%) participated in both the questionnaire and eye examination. The baseline examinations were conducted between 1 July 1999 and 31 December 2000. The follow-up examinations of the eye conditions of the fixed cohort were conducted beginning on 25 March 2006 and ended on 31 December 2007. We planned to invite the 1361 subjects who had participated in the baseline examinations for the follow-up study. A structured questionnaire similar to the baseline survey16 was administered by intensively trained interviewers. The questionnaire obtained information about demographics (ie, age, gender, education, and marital status), body height, body weight (ie, the body mass index=body weight (kg)/body height2 (m2)), and lifestyle (ie, smoking and alcohol intake). The personal medical histories were assessed with a checklist. The participants were asked whether a physician had diagnosed them with a chronic disease, such as diabetes (yes/no), hypertension (yes/no), cardiovascular disease (yes/no), or stroke (yes/no). The participants were also asked whether they lived alone or with a spouse, children, relatives, or friends and whether they required supportive services (definitely need supportive services, need supportive services sometimes, or do not need supportive services at all). The subjects were also asked to rate their health statuses over the past half-year (excellent, very good, good, fair, or poor), and whether they had received contact eye service before (yes/no). The subjects who were interviewed were invited to participate in comprehensive ophthalmic examinations that were conducted in the Taipei Veterans General Hospital. These examinations included the presenting and best-corrected visual acuities, slit-lamp biomicroscopy, tonometry, and fundus photography. Ophthalmologists conducted the examinations according to a standardized protocol. Informed consent was obtained from each subject after explaining the purpose and procedure of the study. The survey followed the tenets of the Declaration of Helsinki.
This study was approved by the Institutional Review Board of the Taipei Veterans General Hospital.
Procedures
Visual acuity was assessed using a Snellen tumbling ‘E’ chart at a distance of 6 m and was recorded separately for each eye. The presenting visual acuity was measured initially with the subject’s spectacles (if worn). Visual acuity was measured without spectacles when the subjects did not have spectacles with them at the time of the ophthalmic examination (ie, for the adults who did not wear spectacles and the adults who had spectacles but did not wear them habitually).
If the presenting visual acuity was <6/6, the examination was repeated with subjective refraction. If a refraction measurement could not be appropriately obtained, a pinhole-corrected acuity test was performed. Visual acuity was determined as the smallest line for which most of the E’s were positioned correctly, that is, correct for 4 of the 4 Es at a given level of acuity or correct for at least 5 of the 6 Es at a given level.
Definitions
Uncorrected refractive error was defined as the presenting visual acuity (with the naked eye if the participant was without spectacles and with distance spectacles when worn by the participant) in the better eye of <6/12 that improved to no impairment (≥6/12) after refractive correction according to the methods described in our previous prevalence study.13
Refractive status was assessed using the spherical equivalent (sphere+1/2 cylinder), which was calculated from the best refractive correction. Spherical equivalents between −1.0 and +1.0 D were defined as emmetropia, spherical equivalents below −1.0 were defined as myopia, and spherical equivalents >+1.0 were defined as hyperopia.
Statistical analysis
The analyses were performed by comparing the subjects who had uncorrected refractive error with those who had no visual impairment. The tested independent variables were age, gender, education, marital status, refractive status, nuclear sclerosis, self-assessed need for supportive service, living status, self-rated health status in the recent half-year, whether distance spectacles were worn during the examination, and history of contact eye service. Univariate analyses were performed to test for associations of each independent variable with the dependent variable using chi-square analyses. A multivariate logistic regression analysis was used to fit the best model for the independent variables. Gender, age, and the independent variables with P-values of 0.2 or less in the univariate analyses were analyzed in the multivariate models. A P-value below 0.05 was considered to be statistically significant in the multivariate model. The statistical analyses were performed with the Statistical Analysis System (SAS 6.12; SAS Institute, Cary, NC, USA) software.
Results
Of the 1361 participants who attended the baseline examination in the 1999 study, 205 (15.1%) were dead before the follow-up study began, 301 (22.1%) had moved away, and 31 (2.3%) were institutionalized. In total, 824 (60.5%) subjects were thus eligible for the study, and 725 (87.4%) agreed to be interviewed for the questionnaire. Among those interviewed, 460 (55.8% of those eligible or 39.8% of the survivors) participated in the ophthalmic examination (Supplementary Figure). Comparisons of the demographics and some of the variables between the subjects who did and did not undergo the eye examination are shown in Table 1. The participants were younger (78.1±4.1 years vs 80.4±5.4 years, P<0.001), more likely to be male (P<0.01), married and living with a spouse (P=0.03), and were more highly educated (P<0.001). The participants were less likely to have a history of stroke (P=0.03) and more likely to be current smokers (P=0.03).
There were six participants who declined or were unable to cooperate with the visual acuity examination; hence, information about visual acuity was obtained for 454 participants. Of the 127 participants who were identified as having uncorrected refractive error in the baseline examination, 27 participated in the follow-up study, and these participants were excluded from the estimation of the incidence of correctable visual impairment.
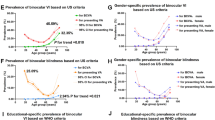
Table 2 illustrates the distribution of the visual acuity statuses of the participants. Forty-four subjects (7-year incidence: 10.5%; 95% CI: 7.6–13.4%) were noted to have newly developed uncorrected refractive error in this cohort. Of the participants (n=27) with uncorrected refractive error in the baseline study, 15 (55.6%) participants were no longer visually impaired (with their naked eyes or their presenting glasses), 6 (22.2%) continued to have uncorrected refractive errors, and 6 (22.2%) had deteriorated to noncorrectable impairment (best-corrected visual acuity below in the 6/12 in the better eye).
Our results reveal that of the 50 participants with uncorrected or undercorrected refractive errors, 92.7% with uncorrected errors and 77.8% with undercorrected errors improved by least 2 lines of visual acuity due to refractive correction, and 46.3% of the uncorrected and 44.4% of the undercorrected subjects improved by 4 lines or more (Supplementary Table). The participants with uncorrected refractive errors exhibited similar potential for improvement in visual acuity as those with undercorrected refractive error (P>0.05).
The univariate analyses revealed that uncorrected refractive error was significantly related to myopia (P=0.01), the use of distance eyeglasses during the examination (P=0.03) and living alone (P=0.01; Table 3).
The multivariate analysis that controlled for covariates revealed that uncorrected refractive error was significantly related to myopia (relative risk (RR): 3.15; 95% CI: 1.31–7.58) and living alone (RR: 2.94; 95% CI 1.14–7.53), whereas the use of distance eyeglasses during the examination was protective against correctable visual impairment (RR: 0.35; 95% CI: 0.14–0.88; Table 4).
Discussion
In the 7-year follow-up, the incidence of uncorrected refractive error was 10.5%, whereas this incidence was 9.6% in our prevalence analysis.13
Since Tielsch17 and Schwab18 brought attention to the importance of correctable visual impairment, there has been wide recognition of uncorrected refractive errors. Prevalence studies have indicated that correctable visual impairment is a major cause of reduced vision in both developing19, 20 and developed countries.21, 22 When comparing the results of different studies, it should be noted that various definition of correctable visual impairment are used. For example, some studies have defined uncorrected refractive error as an improvement in visual acuity of at least two lines or more in the better eye with the best possible refractive correction.8, 10 In the present study, visual impairment was defined as a presenting visual acuity of <6/12 in the participant’s better eye that improved to no impairment (≥6/12) after refractive correction because this measure reflects the visual acuity a person experiences in everyday living, is more representative of the visual demands of modern life,23, 24, 25 such as driving, and accords with the greatest number of population-based studies.11, 13, 14, 26, 27
The Melbourne Visual Impairment Project15 noted that undercorrected refractive error was the most frequent cause of the prevalence (53%) and the incidence (59%) of bilateral impairment. The incidence and severity of visual impairment due to undercorrected refractive error have been noted to increase with age. The incidence of undercorrected refractive error in participants older than 80 (7.2%) years observed in this study is consistent with our findings.
In addition, in accordance with the findings of the Blue Mountains Eye Study,14 our study further confirmed that despite the suggestion of spectacle correction, correctable visual impairments may still persist over time. At a 5-year follow-up, the authors of the Blue Mountains Eye Study found that 34 (27.2%) participants had persistent correctable impairments compared with the 22.2% observed in our study. The predictive factors identified in these two studies were similar and included increasing age, being female, living alone, using community support services and having a history of heart disease.
After education to increase the awareness of ophthalmic health and clinical examinations that was provided at baseline, the awareness of the elderly of eye care and vision improvement was expected to be higher. Surprisingly, the proportion of the elderly with uncorrected refractive errors remained high after 7 years.
In the literature, barriers to eliminating correctable visual impairment have been suggested to exist at three levels,28 that is, the individual level, within the service or treatment context and the societal level. After the implementation of the National Health Insurance Scheme in 1994, the accessibility to ophthalmic medical care services increased, and economic burden became less of a barrier to the public. These trends can be observed in our study in the finding that in our baseline study, 66.9% of the participants who had received cataract surgeries did so under the National Health Program16 after 1994, when this surgery became available free of charge. The prescription of spectacles is offered at a low charge under the National Health Insurance system. However, spectacle frames and lenses have to be paid for by the public at full price. It has been speculated that among generally old and retired populations, the cost of spectacle frames and corrective lenses alone might still be an obstacle to the use of eyeglasses. If the costs of spectacle frames and lenses were also covered by the National Health Insurance, then the proportion of people with correctable visual impairments would be expected to be lower.
Another possible reason is that some elderly may not have strong demands for distance vision or that their daily activities seldom involve distance vision. Hence, distance refractive correction may be deemed unnecessary. This possibility agrees with the fact that myopic subjects are more inclined to have correctable visual impairments than hyperopes. Combined with the fact that the participants who were living alone were more likely to have correctable visual impairments, the barriers were mostly likely at the individual and societal levels in our elderly population.
Moreover, the ideas that the loss of vision in senior life is a natural aging process29 and that there is no method to prevent or to improve this condition has been widely cultivated since youth in this population and was likely not easily changed, even with the provision of ophthalmic education and eye care.
There are some limitations to our study. The response rate was relatively low (55.8% of those eligible). Obtaining population-based prevalence estimates of eye disease among elderly persons is challenging because this group of individuals is less likely to participate in research studies.30 The inclusion rate in the Rotterdam Study31 ranged from 59% in the 75- to 84-year group to 28% in the group that was 85 years old and older. Similarly, in the Baltimore Study,32 the inclusion rates were 48% in the 70- to 79-year group and 21% in the group that was 80 years old and older. Another potential reason for the low participation rate is that the lack of the utilization of ophthalmologic care, prevention, and treatment has created the impression that the loss of vision is expected in senior life and the idea that nothing can be done to improve the situation among elderly people, particularly among less-educated elderly people.16 Many elderly were not aware of the importance of regular physical checkups or that many diseases are asymptomatic in the early stages. This reason could be observed in the findings that more than 90% of participants had received previous contact eye service, whereas only 8% of the nonparticipants had previously attended similar services. We further confirmed this speculation by asking the nonparticipants (684 at the baseline examination) about their reasons for declining the ophthalmic examination: 63% felt that they were fine and did not need any examination; 10% of the elderly stated that they already had regular ophthalmic clinical follow-ups; and the third reason was that they had already previously participated in a similar survey (8%).
The unexamined subjects remain a potential source of bias. Our study population was composed of noninstitutionalized survivors and excluded those who were inpatients or had paralysis or disability, which likely removed a disproportionate number of potential participants with functional or physical impairments and/or declining health-related quality of life and thus might have biased the results of the study. Hence, the incidence of correctable visual impairment may have been underestimated.
Second, the assessments of comorbidities via dichotomized classifications were simplistic. Third, the possibilities of chance findings cannot be completely excluded. Moreover, it should be noted that there were insufficient data for certain variables, such as ever having received eye service, the need for supportive service and the self-rated health in the recent half-year, which prevented meaningful statistical comparisons.
In conclusion, our study indicated that the incidence of correctable visual impairment is high. Living alone and myopia were found to be predisposing factors, whereas the use of distance spectacles at the examination was found to be protective. Further studies should be directed at the underlying reasons for not undergoing refractive error correction and the effects of this lack of correction on the quality of life of the elderly. Public education should be implemented to heighten the awareness of the elderly about eye care and the importance of having their refractive errors checked regularly and to promote the idea that it is possible to improve visual acuity by wearing spectacles.

References
Weih LM, VanNewkirk MR, McCarty CA, Taylor HR . Age-specific causes of bilateral visual impairment. Arch Ophthalmol 2000; 118: 264–269.
Resnikoff S, Pascolini D, Mariotti SP, Pokharel GP . Global magnitude of visual impairment caused by uncorrected refractive errors in 2004. Bull World Health Org 2008; 86 (1): 63–70.
Rubin GS, Roche KB, Prasada-Rao P, Fried LP . Visual impairment and disability in older adults. Optom Vis Sci 1994; 71: 750–760.
Lee PP, Spritzer K, Hays RD . The impact of blurred vision on functioning and well-being. Ophthalmology 1997; 104: 390–396.
Stelmack J . Quality of life of low-vision patients and out-comes of low-vision rehabilitation. Optom Vis Sci 2001; 78: 335–342.
Keeffe JE, Lam D, Cheung A, Dinh T, McCarty CA . Impact of vision impairment on functioning. Aust N Z J Ophthalmol 1998; 26 (Suppl 1): S16–S18.
Carabellese C, Appollonio I, Rozzini R, Bianchetti A, Frisoni GB, Frattola L et al. Sensory impairment and quality of life in a community elderly population. J Am Geriatr Soc 1993; 41: 401–407.
Saw SM, Foster PJ, Gazzard G, Friedman D, Hee J, Seah S . Undercorrected refractive error in Singaporean Chinese adults: the Tanjong Pagar survey. Ophthalmology 2004; 111: 2168–2174.
Varma R, Wang MY, Lai MY, Donofrio J, Azen SP ; Los Angeles Latino Eye Study Group. The prevalence and risk indicators of uncorrected refractive error and unmet refractive need in Latinos: The Los Angeles Latino Eye Study. Invest Ophthalmol Vis Sci 2008; 49: 5264–5273.
Rosman M, Wong TY, Tay WT, Tong L, Saw SM . Prevalence and risk factors of undercorrected refractive errors among Singapore Malay Adults: The Singapore Malay Eye Study. Invest Ophthalmol Vis Sci 2009; 50: 3621–3628.
Foran S, Rose K, Wang JJ, Mitchell P . Correctable visual impairment in an older population: the Blue Mountains Eye Study. Am J Ophthalmol 2002; 134: 712–719.
Bourne RR, Dineen BP, Noorul Huq DM, Ali SM, Johnson GJ . Correction of Refractive Error in the Adult Population of Bangladesh: Meeting the Unmet Need. Invest Ophthalmol Vis Sci 2004; 45: 410–417.
Kuang TM, Tsai SY, Hsu WM, Cheng CY, Liu JH, Chou P . Correctable Visual Impairment in an Elderly Chinese Population in Taiwan: The Shihpai Eye Study. Invest Ophthalmol Vis Sci 2007; 48: 1032–1037.
Foran S, Rose K, Wang JJ, Thiagalingam S, Mitchell P . Five-year outcome of correctable visual impairment: the Blue Mountains Eye Study. Clin Experiment Ophthalmol 2002; 30 (3): 155–158.
Dimitrov PN, Mukesh BN, McCarty CA, Taylor HR . Five-year incidence of bilateral cause-specific visual impairment in the Melbourne Visual Impairment Project. Invest Ophthalmol Vis Sci 2003; 44 (12): 5075–5081.
Tsai SY, Hsu WM, Cheng CY, Liu JH, Chou P . Epidemiologic study of age-related cataracts among an elderly Chinese population in Shih-Pai, Taiwan. Ophthalmology 2003; 110: 1089–1095.
Tielsch JM, Sommer A, Witt K, Katz J, Royall RM . Blindness and visual impairment in an American urban population. The Baltimore Eye Survey. Arch Ophthalmol 1990; 108 (2): 286–290.
Schwab L, Steinkuller PG . Visual disability and blindness secondary to refractive errors in Africa. Soc Sci Med 1983; 17 (22): 1751–1754.
Dineen BP, Bourne RR, Ali SM, Huq DM, Johnson GJ . Prevalence and causes of blindness and visual impairment in Bangladeshi adults: results of the National Blindness and Low Vision Survey of Bangladesh. Br J Ophthalmol 2003; 87 (7): 820–828.
Ramke J, Palagyi A, Naduvilath T, du Toit R, Brian G . Prevalence and causes of blindness and low vision in Timor-Leste. Br J Ophthalmol 2007; 91 (9): 1117–1121.
Vitale S, Cotch MF, Sperduto RD . Prevalence of visual impairment in the United States. JAMA 2006; 295 (18): 2158–2163.
van der Pols JC, Bates CJ, McGraw PV, Thompson JR, Reacher M, Prentice A et al. Visual acuity measurements in a national sample of British elderly people. Br J Ophthalmol 2000; 84 (2): 165–170.
Peli E . Low vision driving in the USA: who, where, when and why. CE Optometry 2002; 5: 54–58.
Daien V, Peres K, Villain M, Colvez A, Carriere I, Delcourt C . Visual acuity thresholds associated with activity limitations in the elderly. The Pathologies Oculaires Liées à l'Age study. Acta Ophthalmol 2014; 92 (7): e500–e506.
Rahi JS, Cumberland PM, Peckham CS . Visual function in working-age adults: early life influences and associations with health and social outcomes. Ophthalmology 2009; 116: 1866–1871.
Klein R, Klein BE, Linton KL, De Mets DL . The Beaver Dam Eye Study: visual acuity. Ophthalmology 1991; 98: 1310–1315.
West SK, Munoz B, Rubin GS, Schein OD, Bandeen-Roche K, Zeger S et al. Function and visual impairment in a population-based study of older adults. The SEE Project. Invest Ophthalmol Vis Sci 1997; 38: 72–82.
Schneider J, Leeder SR, Gopinath B, Wang JJ, Mitchell P . Frequency, course, and impact of correctable visual impairment (Uncorrected refractive error). Surv Ophthalmol 55: 539–560.
Livingston PM, Taylor HRT . Reducing vision loss in the community: a public health priority. Aust J Public Health 1994; 18: 7–8.
Friedman DS, Jampel HD, Muñoz B, West SK . The prevalence of open-angle glaucoma among blacks and whites 73 years and older. The Salisbury Eye Evaluation Glaucoma Study. Arch Ophthalmol 2006; 124: 1625–1630.
Ramrattan RS, Wolfs RCW, Jonas JB, Hofman A, de Jong PT . Determinants of optic disc characteristics in a general population: the Rotterdam Study. Ophthalmology 1994; 106 (8): 1588–1596.
Varma R, Tielsch JM, Quigley HA, Hilton SC, Katz J, Spaeth GL et al. Race-, age-, gender-, and refractive error-related differences in the normal disc. Arch Ophthalmol 1994; 112 (8): 1068–1078.
Acknowledgements
This study was supported by a grant from Taipei Veterans General Hospital, Taipei, Taiwan (V95S3-001).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Additional information
Supplementary Information accompanies this paper on Eye website
Supplementary information
Rights and permissions
About this article

Cite this article
Kuang, TM., Tsai, SY., Liu, CL. et al. Seven-year incidence of uncorrected refractive error among an elderly Chinese population in Shihpai, Taiwan: The Shihpai Eye Study. Eye 30, 570–576 (2016). https://doi.org/10.1038/eye.2015.276
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/eye.2015.276
This article is cited by
-
Prevalence and risk factors of refractive error in Qinghai, China: a cross-sectional study in Han and Tibetan adults in Xining and surrounding areas
BMC Ophthalmology (2021)
-
Relationship between peripapillary atrophy and myopia progression in the eyes of young school children
Eye (2021)
-
Association between dry eye and depressive symptoms in an elderly Chinese population in Taiwan: the Shihpai Eye Study
Eye (2021)
