
An important challenge in addressing mental-health problems is that trends can be difficult to detect because detection relies heavily on self-disclosure. As such, helplines — telephone services that provide crisis intervention to callers seeking help — might serve as a particularly useful source of anonymized data regarding the mental health of a population. This profiling could be especially useful during the COVID-19 pandemic, given the potential emergence or exacerbation of mental-health problems1. Together, the threat of disease to oneself and others that is associated with a local epidemic2, the restrictiveness of local non-pharmaceutical interventions (such as stay-at-home orders) and the potential associated loss of income could have contributed to a decline in the mental health of a population while at the same time inhibiting or delaying people’s search for help for problems3. Writing in Nature, Brülhart et al.4 present evidence suggesting that helpline-call data can be used to monitor real-time changes in the mental health of a population — including over the course of the COVID-19 pandemic.
Read the paper: Mental health concerns during the COVID-19 pandemic as revealed by helpline calls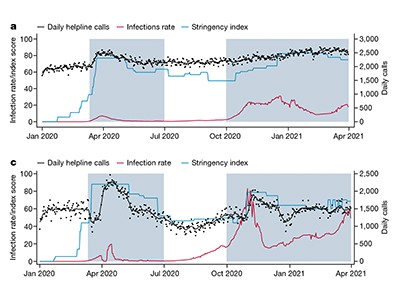
More so than in other areas of medicine, the stigma that can be associated with mental illness often prevents people from fully disclosing their experiences and feelings to those in their social networks, or even to licensed mental-health-care professionals. Furthermore, although mental illness contributes immensely to the global disease burden, primary health-care providers are overburdened, mental-health systems are underfunded and access to evidence-based treatment remains poor5,6. For these reasons, helplines have, since their introduction in the United Kingdom by Samaritans in 1953, played a key part in providing low- or no-cost, anonymous support to people with unmet acute and chronic mental-health needs around the world.
Brülhart and colleagues updated and expanded on their previous work looking at helpline calls in one country7 by assembling data on more than 7 million helpline calls in 19 countries over the course of 2019, 2020 and part of 2021. They found that, within 6 weeks of the start of a country’s initial outbreak (defined as the week in which the cumulative number of reported SARS-CoV-2 infections was higher than 1 in 100,000 inhabitants), call volumes to helplines peaked at 35% higher than pre-pandemic levels (Fig. 1). By examining the changes in the proportion of calls relating to different categories, Brülhart and co-workers attribute these increases to fear, loneliness and concerns about health. The authors also found that suicide-related calls increased in the wake of more-stringent, non-pharmaceutical interventions, but that such calls decreased when income-support policies were introduced. The latter finding is perhaps unsurprising, but is a welcome addition to the evidence base that supports ongoing appeals for financial and other support to mitigate the adverse effects of non-pharmaceutical interventions on uncertainties over employment, income and housing security8.

Figure 1 | A surge in helpline calls after local outbreaks of COVID-19. Helpline data can be used to monitor people’s mental health in near-real time. Brülhart et al.4 used helpline data to track changes in mental health at the population level. They gathered anonymized data from 21 helplines across 19 countries. The authors compared the volume of calls in the weeks before and after the start of local COVID-19 outbreaks (defined as the week in which the cumulative number of infections surpassed 1 in 100,000 inhabitants). The number of calls increased by an average of 35% by 6 weeks from the start of the local outbreak, after which the number gradually decreased.
The study by Brülhart et al. is among the most comprehensive such analyses of helpline data9,10 conducted so far. Other investigators have used data from Internet search-engine queries11 or electronic health records12 to track mental-health trends in a population. Compared with data on mental-health-related queries in search engines (which might represent information-seeking rather than help-seeking), helpline-call data are more likely to reflect the mental-health concerns of individual callers. And they are not subject to the lag times that might impose limitations on the use of electronic health records for tracking the mental health of a population.
Nevertheless, there are limitations to the use of helpline-call data for monitoring people’s mental health. Individuals in emotional distress who choose to call a helpline are unlikely to have a similar mental-health profile to people in emotional distress who do not call helplines or who lack the means to make such a call. Furthermore, for people who do not live alone, stay-at-home restrictions could compromise the privacy that they might need to place a helpline call, particularly in circumstances in which they are at risk of violence from an intimate partner13. These factors, which would probably result in underestimates of population mental-health problems, would be likely to reduce the usefulness of helpline-call data for monitoring.
Text-message nudges encourage COVID vaccination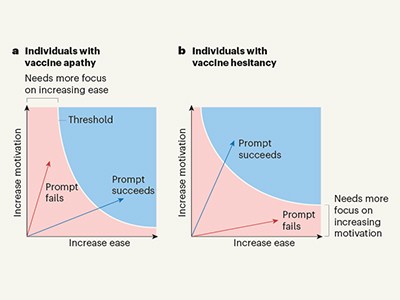
There are also limitations to relying on the identified topics of the calls, because there might be within- and between-country differences in how the calls are interpreted and categorized. Whether an individual call is categorized as being prompted by ‘a relationship issue’ as opposed to ‘loneliness’ or ‘violence’, for example, is likely to be governed by operator- and culture-specific factors. In addition, the identified topic might not reflect the underlying source of concern, but rather be a topic that the caller wants to discuss with the helpline operator. Furthermore, although helplines are an established service, and call data (such as call topic) can be analysed, less is known about the individuals making the calls, and relatively few studies have examined the characteristics of helpline callers14. Anonymized data on the characteristics of helpline callers could be correlated with data on the content of helpline calls to further inform mental-health policy, service delivery and programme implementation. In doing this, we would be able to identify the types of individual who might benefit from these intervention or prevention programmes.
Despite these limitations, Brülhart and colleagues’ study improves our understanding of how experiences of the pandemic around the world have led people to reach out for help. Although, for the reasons described above, help-seeking is not a straightforward indicator of distress, the call volumes over time — which showed an initial peak and then a decline to pre-pandemic levels — have a trajectory that is consistent with that seen in longitudinal studies that have assessed distress over time during the pandemic through other methodologies (such as using surveys)15,16. It seems that the convergence of findings from different methods for monitoring mental health in populations can further inform our understanding of how the pandemic has driven both distress and help-seeking behaviour.
Scrutinizing the defects of digital technology on mental health
The rapid changes in the trajectory of the COVID-19 pandemic and its immediate effects on acute distress have revealed the urgent need for real-time monitoring to enable evidence-based, responsive changes in social policies and health-care systems to be implemented and assessed. Public-health officials have relied on the tracking of the spread of the SARS-CoV-2 virus worldwide to guide interventions to prevent disease; however, similar efforts are also urgently needed to address mental-health problems. Helpline-call data could enable policymakers, mental-health professionals and the general public to determine the best course of action for addressing mental-health concerns and any associated problems. Understanding how policies specifically influence mental health on the basis of location (for example, country) and caller demographic (including age, gender and race) could enable policies to be tailored and optimized.
This study serves as an excellent example of a data resource that it is hoped will spur researchers to assess the promise of applying other data sources (such as Internet applications and text- or Internet-based messaging services) to monitor population mental health in other countries worldwide.
 Read the paper: Mental health concerns during the COVID-19 pandemic as revealed by helpline calls
Read the paper: Mental health concerns during the COVID-19 pandemic as revealed by helpline calls
 Text-message nudges encourage COVID vaccination
Text-message nudges encourage COVID vaccination
 Scrutinizing the defects of digital technology on mental health
Scrutinizing the defects of digital technology on mental health





