
Abstract
Background:
We recently isolated vasohibin-1 (VASH1), a novel angiogenic molecule that is specifically expressed in activated vascular endothelial cells (ECs), and the status of VASH1 expression has been documented in various cancer angiogenesis. The aim of this study was to assess the prognostic value of VASH1 expression in prostate cancer (PCa).
Methods:
In this study, we retrospectively analysed the clinical records and evaluated the VASH1 expression of tumour microvessels in 167 patients with PCa who underwent radical prostatectomy. We immunohistochemically examined the microvessels positive for anti-CD34 as microvessel density (MVD) and the microvessels with activated ECs positive for VASH1 density.
Results:
We found that the VASH1 expression was restricted to ECs in the tumour stroma. VASH1 density was significantly associated with pathological T stage, Gleason score and MVD. The 5-year PSA recurrence-free survival rate was 58.8% in patients with higher VASH1 density (≧12 per mm2) and 89.1% in patients with lower VASH1 density (<12 per mm2), respectively (P<0.001). Microvessel density was not an independent predictor of PSA recurrence. Multivariate analysis revealed that high VASH1 density was an independent prognostic indicator of PSA recurrence (P=0.007, HR=2.950).
Conclusion:
VASH1 density represents a clinically relevant predictor of patient prognosis and can be a new biomarker that would provide additional prognostic information in PCa.
Similar content being viewed by others

Main
Prostate cancer (PCa) is one of the most commonly diagnosed malignant tumours in men and the second leading cause of cancer-related deaths in the United States (Jemal et al, 2010). Nowadays, there are still few effective therapeutic options for advanced PCa (Scher and Sawyers, 2005; Chen et al, 2008). One of the most troublesome aspects of PCa is that androgen-dependent PCa inevitably progresses to highly aggressive and life-threatening castration-resistant prostate cancer after androgen ablation therapy. The key molecular events associated with PCa progression remains to be elucidated.
Angiogenesis, which is the formation of new blood vessel networks, not only plays a role in human normal development but also in pathophysiological conditions such as inflammation and cancer (Folkman, 1971; Sato, 2003). The development and establishment of blood supply has an important role in the development and growth of cancer cells by providing oxygen, nutrients and growth factors. In addition to its traditional role, angiogenesis is one of the potential pathways that contribute to solid tumour progression and metastasis by allowing cancer cells direct access to vessels. In general, angiogenesis is regulated by a balance between stimulatory and inhibitory factors (Sato and Sonoda, 2007, Sato, 2012). Molecules such as CD34, von Willebrand factor and vascular endothelial-cadherin, which are specifically expressed in vascular endothelial cells (ECs), could serve as biomarkers of angiogenesis (Weidner et al, 1991). One of the parameters of angiogenesis in neoplasms is microvessel density (MVD). In PCa, several studies indicated that MVD served as a predictor of poorly differentiated tumours and biochemical failure after treatment (Weidner et al, 1993; Bettencourt et al, 1998; Borre et al, 1998; Rubin et al, 1999; Krupski et al, 2000; Josefsson et al, 2005; Concato et al, 2007, 2009; Kosaka et al, 2007). However, to date the prognostic role of MVD in PCa has not been fully characterised. This is because those angiogenic molecules are expressed in quiescent ECs as well as in activated ECs, and thus cannot reflect ‘angiogenic activity’ alone.
We recently isolated vasohibin-1 (VASH1), a novel angiogenic molecule, that is specifically expressed in ECs and upregulated by vascular endothelial growth factor (VEGF) and fibroblast growth factor 2 (FGF-2) (Watanabe et al, 2004; Kimura et al, 2009). Previous studies found that the expression of VASH1 was restricted to ECs of blood vessels in the tumour stroma and correlated with the expression of VEGF and FGF-2 in tumour cells (Hosaka et al, 2009). No one has ever characterised the expression of VASH1 in relation to tumour angiogenesis in PCa. In this study, we will evaluate whether the expression of VASH1 can serve as a more accurate biomarker of tumour angiogenesis compared with MVD.
We will examine the expression of VASH1 and MVD in PCa specimens acquired by primary surgery and investigate whether VASH1 expression reflects angiogenic activity in PCa and if this is related to the clinical outcome.
Materials and methods
Patients selection
Samples of archival paraffin-embedded tissue sections and clinicopathological features were obtained from 167 patients with PCa diagnosed and operated on at Keio University hospital. One hundred and sixty-seven patients underwent curative surgery that included radical prostatectomy for localised PCa between January 2000 and December 2003. None of the patients had received hormonal treatment before the operation. The characteristics of these patients are shown in Table 1. After radical prostatectomy, patients were followed by serum PSA level and imaging studies. Prostate-specific antigen relapse was defined by an elevation of serum PSA level at three consecutive measurements. Histology of the specimens was evaluated by two independent pathologists using haematoxylin- and eosin-stained tissue preparations.
Tissue samples and immunohistochemistry
All the tissue samples were fixed in 10% formalin, embedded in paraffin and cut into 4-μm-thick sections. All pathological specimens were reviewed again by genitourinary pathologists to unify the reproducibility of the diagnosis. As for the pathologic stage, all neoplasms were classified according to the 2006 TNM staging system. All study participants provided their informed consent, and the study design was approved by the ethics review board of Keio University. We carried out immunohistochemical staining for VASH1 and CD34 (as markers of vascular ECs). Tissue sections were deparaffinised in xylene, and hydrated by immersion in graded alcohols and finally in distilled water. After antigen retrieval was performed, endogenous peroxidase activity was blocked by incubation in 0.3% hydrogen peroxidase for 20 min at room temperature. The tissue sections were then incubated with a blocking solution of 5% dry milk in PBS. They were stained for 60 min at room temperature with primary antibodies, followed by staining for 30 min at room temperature with secondary antibodies. The primary antibodies were all mouse monoclonal antibodies (mAbs): anti-human VASH1 mAb diluted at 1:400 and anti-CD34 (Nichirei Biosciences, Tokyo, Japan) diluted at 1:200. We previously described a mouse mAb against a synthetic peptide corresponding to the 286–299 amino-acid sequence of VASH1 (Watanabe et al, 2004). The specificity of this antibody, which detects VASH1, has been documented in our previous studies (Watanabe et al, 2004; Yoshinaga et al, 2008, 2011; Hosaka et al, 2009; Kimura et al, 2009; Tamaki et al, 2009, 2010; Miyashita et al, 2012; Miyazaki et al, 2012). After washing with PBS, the tissue sections were incubated with secondary antibodies (Histofine Simple Stain MAX PO (M); Nichirei Biosciences). Colour was developed with 3, 3′-diaminobenzamine tetrahydrochloride in 50 mM Tris-HCl (pH 7.5) containing 0.005% hydrogen peroxide. The sections were counterstained with haematoxylin. The positive control slide CD34 antigen was prepared from paraffin-fixed bladder cancer tissue with high MVD. The appropriate negative controls slides for CD34 antigen and VASH1 were prepared by substituting the primary antibody with the immune globulin fraction of nonimmune mouse serum at the same concentration in each staining run.
Evaluation of immunostaining
Two authors independently evaluated immunoreactivity. They were blinded to the clinical course of the patients and the average of the numbers counted by the two investigators was used for subsequent analyses. Olympus IX71 (Olympus, Tokyo, Japan) was used for the analysis. The microvessels within the tumour were counted. Microvessels were identified based on their architecture, lumen lined by ECs and complemented by positivity of the ECs for anti-CD34 after scanning the immunostained section at low magnification ( × 40 and × 100). The areas with the highest number of distinctly highlighted microvessels were selected, and these were counted at high magnification ( × 200). We evaluated at least six areas in high-power fields and selected one area with the highest number of vessels. Any immunostained EC or cluster separated from adjacent vessels was counted as a single microvessel, even in the absence of vessel lumen. Each single count was defined as the highest number of microvessels identified at the ‘hot spot’ as shown previously (Mikami et al, 2006; Kosaka et al, 2007; Shirotake et al, 2011; Yoshinaga et al, 2011). The highest number of microvessels in the hot spot was counted for MVD. Vasohibin-1-positive signals were counted in the ‘hot spot’ in which the highest number of vessels positive for anti-CD34 was identified. We regarded the number of VASH1-positive signals per mm2 as ‘VASH1 density’ (Tamaki et al, 2009, 2010; Yoshinaga et al, 2011). The median values of MVD and VASH1 density were 119.5 and 9.9 per mm2, respectively. We used a median MVD of ≧120 per mm2 and a VASH1 density of ≧12 per mm2 as the cutoff levels.
Statistical analysis
The associations between each clinicopathological parameter and VASH1 density of the tumour were analysed. These associations were validated using χ2 test or Mann–Whitney U-test. Biochemical recurrence-free survival was estimated using the Kaplan–Meier method and was compared by using the log-rank test. Multivariate analysis was performed using the Cox proportional hazard model. Differences among groups were regarded as significant when P<0.05. These analyses were performed with the SPSS version 18.0 statistical software package (IBM corporation, New York, NY, USA).
Results
Patient characteristics and VASH1 expression in PCa
Table 1 shows the clinicopathological characteristics of the patients and their association with MVD or VASH1 density in our study population. The median age of the patients was 66.6 years (range 46–75 years). Pathological T (pT) stage was ≦pT2 in 113 cases (67.7%) and ≧pT3 in 54 cases (32.3%). Gleason score (GS) was ≦ 6 in 69 cases (41.3%) and ≧7 in 98 cases (58.7%). During a median follow-up of 4.9 years, 48 patients (28.7%) experienced PSA recurrence. To elucidate the biological significance of VASH1 in PCa, we examined the expression of VASH1 by immunohistochemical staining (Figure 1). Although CD34 staining of vascular ECs in benign prostatic tissue adjacent to cancerous tissue was positive as shown previously (Figure 1A), VASH1 staining of vascular ECs was negative or negligible (Figure 1B). Vasohibin-1 staining of vascular ECs was negative or negligible in low pT stage and low GS PCa (Figure 1D). On the other hand, in high pT stage PCa, strong VASH1 staining of vascular ECs was detected in many cases (Figure 1F). Strong VASH1 staining was observed in ECs of microvessels in the tumour lesion of high pT stage and high GS specimens. VASH1 staining of vascular ECs was negative or negligible in large-size vessels of the tumour detected by CD34.

Immunostaining for CD34 ( A, C and E ) and VASH1 ( B, D and F ) in PCa. CD34 staining (A) and VASH1 staining (B) of vascular ECs in benign prostatic tissue adjacent to cancerous tissue. VASH1 staining of vascular ECs was negative or negligible. Low pT stage and PCa with low VASH1 density (C and D) or high pT stage with high VASH1 density (E and F). Bar=0.1 mm.
The average MVD and VASH1 density (counts per mm2) were 123±51.6 and 9.9±7.3 in 167 patients, respectively (Table 1). Patients with high GS tumours (P<0.001) or ≧pT3 (P<0.001) had significantly higher levels of both MVD and VASH1 density. As it has been reported that VASH1 associates with CD34, we also investigated the relationship between VASH1 and CD34 expression. Using Spearman’s correlation coefficient test, we detected a significant positive correlation between MVD and VASH1 density in microvessels in the tumour (ρ=0.504, P<0.001).
Prognostic significance of VASH1 expression in PCa patients
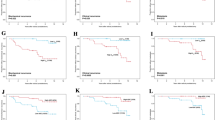
We performed univariate and multivariate analysis to determine the indicators for subsequent PSA recurrence following surgery (Table 2). Univariate analysis revealed that high PSA concentration (P<0.001), high pT stage (P<0.001), high MVD (P<0.001) and high VASH1 density (≧12 per mm2) (P<0.001) were significant predictors of tumour recurrence. Multivariate analysis showed that high pT stage (P<0.001, HR=4.667) and high VASH1 density (P=0.007, HR=2.950) were also independent predictors of PSA recurrence. A high level of MVD was not an independent predictor of PSA recurrence. Table 3 shows the association between the level of VASH1 density and clinic–pathological characteristics in 167 patients. High VASH1 density was significantly associated with GS (P<0.001), pT stage (P=0.005) and MVD (P<0.001). The 5-year Kaplan–Meier PSA recurrence-free survival rate was 58.8% in patients with high VASH1 density compared with 89.1% (P<0.001) in their counterparts (Figure 2A).

Kaplan–Meier curves of PSA recurrence-free survival of the patients after surgery for PCa according to VASH1 density ( A ) or MVD ( B). Kaplan–Meier curves of PSA recurrence-free survival (C) of the patients after surgery for PCa according to pT stage and VASH1 density stratified according to three risk groups. Low-risk group consisted of patients with ≤pT2 and low VASH1 density. High-risk group consisted of those with ≥pT3 and high VASH1 density. All others were included in the intermediate-risk group.
Risk stratification for PCa according to pT stage and VASH1 density
We distributed the patients into three different groups according to pT stage and VASH1 density, which were the two statistically significant variables found by the multivariate Cox regression analysis (Figure 2C). The relative risk of death was calculated with the formula, exp (1.540 × pT stage+1.082 × VASH1 density) for PSA recurrence-free survival. In this equation, the pT stage equaled 1 if the pT stage was pT3 or more, and it equaled 0 if the pT stage was pT2 or less. VASH1 density equaled 1 if VASH1 density was ≧12 per mm2 and 0 if <12 per mm2. On the basis of the relative risk of death, patients with PCa were divided into three risk groups: low (relative risk of PSA recurrence=1), intermediate (8.02–12.7 for PSA recurrence-free survival) and high (13.8 for PSA recurrence-free survival). According to the risk stratification for PCa based on prognostic factors, 65 patients (38.9%) were in the low-risk group (low pT stage and low VASH1 density), 66 patients (39.5%) were in the high-risk group (high pT stage and high VASH1 density) and 36 patients (21.6%) were in the intermediate-risk group (all others). The 5-year PSA recurrence-free survival was 98.1% in the low-risk group, 69.7% in the intermediate-risk group and 33.7% in the high-risk group, respectively. The differences among the groups were significant (P<0.001 in PSA recurrence-free survival and for low- vs intermediate-risk group, P<0.001 for low- vs high-risk group and P<0.001 for intermediate- vs high-risk group in PSA recurrence-free survival).
Microvessel density could be divided into two subclasses for PSA recurrence according to VASH1 density in PCa patients
Univariate analysis revealed that high MVD was one of the significant predictors of PSA recurrence (Figure 2B), while multivariate analysis showed that high MVD was not an independent predictor of PSA recurrence. Then, we re-evaluated univariate analysis of MVD according to high or low VASH1 density (Figure 3). In the low MVD group, 21 patients (25.3%) had high VASH1 density and 62 patients (74.7%) had low VASH1 density (Figure 3A). The 5-year PSA recurrence-free survival rate in the low MVD group was 79.9% for those with high VASH1 density and 94.9% for those with low VASH1 density. The difference between the groups was statistically significant (P<0.001). In the high MVD group, 63 patients (75.0%) had high VASH1 density and 21 patients (25.0%) had low VASH1 density (Figure 3B). The 5-year PSA recurrence-free survival rate in the high MVD group was 43.1% for those with high VASH1 density and 80.1% for those with low VASH1 density. The differences were significant (P<0.001). These results indicated that MVD in PCa could be subdivided into two subclasses for PSA recurrence according to VASH1 density.

Kaplan–Meier curves of PSA recurrence-free survival of the patients among low ( A ) or high ( B ) MVD groups according to VASH1 density. The patients with high MVD and high VASH1 density had a significantly poorer prognosis than the counterpart group (P<0.001).
Discussion
In this study, we retrospectively evaluated the impact of VASH1 expression by immunohistochemical staining in a series of patients with PCa treated in a single centre. Our results suggested that VASH1 expression was a prognostic indicator in addition to other standard factors such as pT stage. High VASH1 density was related to shorter patient PSA recurrence-free survival. To the best of our knowledge, this is the first study evaluating the prognostic value of VASH1 expression in patients with prostate cancer.
Angiogenesis has a critical role in tumour growth and metastasis (Folkman, 1971; Chung et al, 2010). Recent studies revealed significant roles for angiogenesis in the prediction of survival in patients with different malignancies (Sato, 2003, 2012; Chung et al, 2010). One of the biomarkers that could reflect angiogenic aggressiveness was MVD (Weidner et al, 1991; Bochner et al, 1995; Kosaka et al, 2007; Shirotake et al, 2011). Several studies on PCa indicated that the status of MVD was associated with clinical features, such as GS and pathological stage, and could be an independent prognostic factor of patient survival (Weidner et al, 1993; Bettencourt et al, 1998; Borre et al, 1998; Rubin et al, 1999; Krupski et al, 2000; Josefsson et al, 2005; Concato et al, 2007, 2009; Kosaka et al, 2007). However, to date evidence of the prognostic role of MVD in PCa is contradictory, suggesting that the prognostic impact of MVD might be controversial. In this study, univariate analysis reveled that there was significant association between MVD and PSA recurrence. However, multivariate analysis including VASH1 density showed that MVD did not have a prognostic significance in PCa progression. One of the reasons might be because MVD corresponds to the number of accomplished vessels and includes vessels without the potential of neovascularisation in PCa. Our previous reports showed that VASH1 has been isolated from VEGF-inducible genes in ECs present in newly formed blood vessels behind the sprouting front where angiogenesis terminates (Watanabe et al, 2004; Sato and Sonoda, 2007; Hosaka et al, 2009). Recently, we have reported that histologic evidence of VASH1 expression has been found in samples from patients with endometrial carcinoma (Yoshinaga et al, 2008), breast cancer (Tamaki et al, 2009, 2010) and cervical carcinoma (Yoshinaga et al, 2011). Our reports indicated that VASH1 expression was associated with tumour grade and histological type of carcinomas. Moreover, it was reported that VASH1 expression tended to be concordant with MVD, although partial dissociation was observed in some patients with breast carcinoma. VASH1 expression was significantly higher in invasive breast carcinoma, although no significant difference was observed in the level of MVD between patients with invasive disease or not (Tamaki et al, 2010). These studies suggested that an evaluation of the number of VASH1-positive vessels may become one of the prognostic biomarkers for metastasis and prognosis. These results indicate that VASH1 could become a new molecular biomarker of the angiogenic heterogeneity of tumours. In this study, we demonstrated that the prognostic value of MVD depends on the level of VASH1 density.
Our study demonstrated that PCa with a higher number of VASH1-positive vessels tended to have a poor prognosis. We found a significant correlation among VASH1 density, GS and pT stage. Multivariate analysis showed that high VASH1 density was an independent prognostic factor, suggesting that the status of VASH1 density could serve as a biomarker of the malignant potential of tumour angiogenesis. These results suggest that the level of VASH1 expression may influence the clinical course of prostate cancer progression. Moreover, VASH1 may become a molecular target in PCa patients.
Using VASH1 density and other independent indicators, we established a prognostic risk stratification for PCa. Patients were stratified into three groups according to statistical modelling based on the relative risk associated with the prognostic indicators derived from multivariate analysis. As shown in Figure 2C among patients with PCa, the prognosis of patients with higher pT stage and high VASH1 density was worse than that of the other groups (P<0.001). This stratification made it possible to predict PSA recurrence more accurately, suggesting more appropriate follow-up including PSA follow-up interval.
In conclusion, these results indicated that VASH1 can serve as a new biomarker for predicting PCa progression and could become a molecular target in PCa, especially for targeting tumour angiogenesis.
Change history
28 May 2013
This paper was modified 12 months after initial publication to switch to Creative Commons licence terms, as noted at publication
References
Bettencourt MC, Bauer JJ, Sesterhenn IA, Connelly RR, Moul JW (1998) CD34 immunohistochemical assessment of angiogenesis as a prognostic marker for prostate cancer recurrence after radical prostatectomy. J Urol 160: 459–465
Bochner BH, Cote RJ, Weidner N, Groshen S, Chen SC, Skinner DG, Nichols PW (1995) Angiogenesis in bladder cancer: relationship between microvessel density and tumor prognosis. J Natl Cancer Inst 87: 1603–1612
Borre M, Offersen BV, Nerstrom B, Overgaard J (1998) Microvessel density predicts survival in prostate cancer patients subjected to watchful waiting. Br J Cancer 78: 940–944
Chen Y, Sawyers CL, Scher HI (2008) Targeting the androgen receptor pathway in prostate cancer. Curr Opin Pharmacol 8: 440–448
Chung AS, Lee J, Ferrara N (2010) Targeting the tumour vasculature: insights from physiological angiogenesis. Nat Rev Cancer 10: 505–514
Concato J, Jain D, Li WW, Risch HA, Uchio EM, Wells CK (2007) Molecular markers and mortality in prostate cancer. BJU Int 100: 1259–1263
Concato J, Jain D, Uchio E, Risch H, Li WW, Wells CK (2009) Molecular markers and death from prostate cancer. Ann Intern Med 150: 595–603
Folkman J (1971) Tumor angiogenesis: therapeutic implications. N Engl J Med 285: 1182–1186
Hosaka T, Kimura H, Heishi T, Suzuki Y, Miyashita H, Ohta H, Sonoda H, Moriya T, Suzuki S, Kondo T, Sato Y (2009) Vasohibin-1 expression in endothelium of tumor blood vessels regulates angiogenesis. Am J Pathol 175: 430–439
Jemal A, Siegel R, Xu J, Ward E (2010) Cancer statistics, 2010. CA Cancer J Clin 60: 277–300
Josefsson A, Wikstrom P, Granfors T, Egevad L, Karlberg L, Stattin P, Bergh A (2005) Tumor size, vascular density and proliferation as prognostic markers in GS 6 and GS 7 prostate tumors in patients with long follow-up and non-curative treatment. Eur Urol 48: 577–583
Kimura H, Miyashita H, Suzuki Y, Kobayashi M, Watanabe K, Sonoda H, Ohta H, Fujiwara T, Shimosegawa T, Sato Y (2009) Distinctive localization and opposed roles of vasohibin-1 and vasohibin-2 in the regulation of angiogenesis. Blood 113: 4810–4818
Kosaka T, Miyajima A, Takayama E, Kikuchi E, Nakashima J, Ohigashi T, Asano T, Sakamoto M, Okita H, Murai M, Hayakawa M (2007) Angiotensin II type 1 receptor antagonist as an angiogenic inhibitor in prostate cancer. Prostate 67: 41–49
Krupski T, Petroni GR, Frierson HF Jr., Theodorescu JU (2000) Microvessel density, p53, retinoblastoma, and chromogranin A immunohistochemistry as predictors of disease-specific survival following radical prostatectomy for carcinoma of the prostate. Urology 55: 743–749
Mikami S, Oya M, Mizuno R, Murai M, Mukai M, Okada Y (2006) Expression of Ets-1 in human clear cell renal cell carcinomas: implications for angiogenesis. Cancer Sci 97: 875–882
Miyashita H, Watanabe T, Hayashi H, Suzuki Y, Nakamura T, Ito S, Ono M, Hoshikawa Y, Okada Y, Kondo T, Sato Y (2012) Angiogenesis inhibitor vasohibin-1 enhances stress resistance of endothelial cells via induction of SOD2 and SIRT1. PLoS One 7: e46459
Miyazaki Y, Kosaka T, Mikami S, Kikuchi E, Tanaka N, Maeda T, Ishida M, Miyajima A, Nakagawa K, Okada Y, Sato Y, Oya M (2012) The prognostic significance of vasohibin-1 expression in patients with upper urinary tract urothelial carcinoma. Clin Cancer Res 18: 4145–4153
Rubin MA, Buyyounouski M, Bagiella E, Sharir S, Neugut A, Benson M, de la Taille A, Katz AE, Olsson CA, Ennis RD (1999) Microvessel density in prostate cancer: lack of correlation with tumor grade, pathologic stage, and clinical outcome. Urology 53: 542–547
Sato Y (2003) Molecular diagnosis of tumor angiogenesis and anti-angiogenic cancer therapy. Int J Clin Oncol 8: 200–206
Sato Y, Sonoda H (2007) The vasohibin family: a negative regulatory system of angiogenesis genetically programmed in endothelial cells. Arterioscler Thromb Vasc Biol 27: 37–41
Sato Y (2012) The vasohibin family: Novel regulators of angiogenesis. Vascul Pharmacol 56: 262–266
Scher HI, Sawyers CL (2005) Biology of progressive, castration-resistant prostate cancer: directed therapies targeting the androgen-receptor signaling axis. J Clin Oncol 23: 8253–8261
Shirotake S, Miyajima A, Kosaka T, Tanaka N, Maeda T, Kikuchi E, Oya M (2011) Angiotensin II type 1 receptor expression and microvessel density in human bladder cancer. Urology 77, 1009, e19–e25
Tamaki K, Moriya T, Sato Y, Ishida T, Maruo Y, Yoshinaga K, Ohuchi N, Sasano H (2009) Vasohibin-1 in human breast carcinoma: a potential negative feedback regulator of angiogenesis. Cancer Sci 100: 88–94
Tamaki K, Sasano H, Maruo Y, Takahashi Y, Miyashita M, Moriya T, Sato Y, Hirakawa H, Tamaki N, Watanabe M, Ishida T, Ohuchi N (2010) Vasohibin-1 as a potential predictor of aggressive behavior of ductal carcinoma in situ of the breast. Cancer Sci 101: 1051–1058
Watanabe K, Hasegawa Y, Yamashita H, Shimizu K, Ding Y, Abe M, Ohta H, Imagawa K, Hojo K, Maki H, Sonoda H, Sato Y (2004) Vasohibin as an endothelium-derived negative feedback regulator of angiogenesis. J Clin Invest 114: 898–907
Weidner N, Semple JP, Welch WR, Folkman J (1991) Tumor angiogenesis and metastasis – correlation in invasive breast carcinoma. N Engl J Med 324: 1–8
Weidner N, Carroll PR, Flax J, Blumenfeld W, Folkman J (1993) Tumor angiogenesis correlates with metastasis in invasive prostate carcinoma. Am J Pathol 143: 401–409
Yoshinaga K, Ito K, Moriya T, Nagase S, Takano T, Niikura H, Sasano H, Yaegashi N, Sato Y (2011) Roles of intrinsic angiogenesis inhibitor, vasohibin, in cervical carcinomas. Cancer Sci 102: 446–451
Yoshinaga K, Ito K, Moriya T, Nagase S, Takano T, Niikura H, Yaegashi N, Sato Y (2008) Expression of vasohibin as a novel endothelium-derived angiogenesis inhibitor in endometrial cancer. Cancer Sci 99: 914–919
Acknowledgements
We thank colleagues from the Department of Vascular Biology, Institute of Development, Aging and Cancer, Tohoku University for their excellent technical assistance in purifying anti-human VASH1 mAb. This work was supported in part by grants-in-aid for Scientific Research from the Ministry of Education, Culture, Sports, Science, and Technology of Japan, by the Prostate Research Fund in Japan, the Japan Urological Association (5th Young Research Grant 2011 to TK) and the Cooperative Research Project Program 2011, 2012 of Joint Usage/Research Center at the Institute of Development, Aging and Cancer, Tohoku University.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Additional information
This work is published under the standard license to publish agreement. After 12 months the work will become freely available and the license terms will switch to a Creative Commons Attribution-NonCommercial-Share Alike 3.0 Unported License.
Rights and permissions
From twelve months after its original publication, this work is licensed under the Creative Commons Attribution-NonCommercial-Share Alike 3.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-sa/3.0/
About this article
Cite this article
Kosaka, T., Miyazaki, Y., Miyajima, A. et al. The prognostic significance of vasohibin-1 expression in patients with prostate cancer. Br J Cancer 108, 2123–2129 (2013). https://doi.org/10.1038/bjc.2013.169
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/bjc.2013.169
Keywords
This article is cited by
-
m6A methylation-mediated regulation of LncRNA MEG3 suppresses ovarian cancer progression through miR-885-5p and the VASH1 pathway
Journal of Translational Medicine (2024)
-
Vasohibin-1 rescues erectile function through up-regulation of angiogenic factors in the diabetic mice
Scientific Reports (2021)
-
RETRACTED ARTICLE: Long noncoding RNA RBMS3-AS3 acts as a microRNA-4534 sponge to inhibit the progression of prostate cancer by upregulating VASH1
Gene Therapy (2020)
-
Prognostic significance of vasohibin-1 and vasohibin-2 immunohistochemical expression in gastric cancer
Surgery Today (2020)
-
Increased vasohibin-1 expression is associated with metastasis and poor prognosis of renal cell carcinoma patients
Laboratory Investigation (2017)
